PTSD english

of 44
-
Upload
ganpat-vankar -
Category
Documents
-
view
242 -
download
0
Transcript of PTSD english
-
7/28/2019 PTSD english
1/44
Trauma and PTSD
-
7/28/2019 PTSD english
2/44
,
-
7/28/2019 PTSD english
3/44
PTSD DSM-IV Criteria
Exposure to traumatic event with
Actual or threatened death or serious
injuryand
Response involving intense fear,
helplessness, or horror
American Psychiatric Association. DSM-IV. 1994.
-
7/28/2019 PTSD english
4/44
Symptom Clusters
Re-experiencing: intrusive recollections,
recurrent dreams, dissociative flashbacks
Avoidance and numbness: avoidance ofcognitions/activities related to trauma,
decreased interest, feeling detached
Hyperarousal: hypervigilance, insomnia,
exaggerated startle response
-
7/28/2019 PTSD english
5/44
PTSD DSM-IV Criteria
Re-experiencing the traumatic event
Persistent avoidance of stimuli associated with event
Numbing of general responsiveness Symptoms of increased arousal
At least 1 months duration (otherwise can diagnose
Acute Stress Disorder)
Significant distress or impairment in social,occupational, or other functioning
American Psychiatric Association. DSM-IV. 1994.
-
7/28/2019 PTSD english
6/44
PTSDAssociated Features
Alcohol/drug problems
Aggression/violence
Suicidal ideation, intent, attempts
Dissociation Distancing
Problems at work
Marital problems
Homelessness
-
7/28/2019 PTSD english
7/44
Epidemiology of PTSD
National Comorbidity Study 7.8% of adults in the U.S. (lifetime)
Type of trauma most often the basis for
PTSD: rape in women (46% risk)
combat in men (39% risk)
1/3 of cases have duration of many years 88% of cases have psychiatric comorbidity
Kessler RC, et al. Arch Gen Psychiatry. 1995;52:1048-60.
-
7/28/2019 PTSD english
8/44
Combat-Related PTSD:
Epidemiology
Lifetime Prevalence:
30% in Vietnam veterans
5-10% of Gulf War I deployed veterans 10-20% in Operation Enduring Freedom
and Operation Iraqi Freedom
VIETNAM: Kulka RA, et al. Trauma and the Vietnam war generation: Report of the findings from the National Vietnam Veterans
Readjustment Study. 1990, New York: Brunner/Mazel.
GULF WAR: Stretch RH et al. Military Medicine. 1996;161:407-410.IRAQ WAR: Hoge, C.W., et al. R.L. N Engl J Med. 2004;351:13-22.
-
7/28/2019 PTSD english
9/44
0
1020
30
4050
60
70
80
Numbe
rof
Individ
uals
McFarlane, et al. Ann N Y Acad Sci. 1997;821:437-441
Responses to Trauma Are Heterogeneous
Primary Psychiatric Disorder
6 Months Following Trauma
-
7/28/2019 PTSD english
10/44
Kessler RC, et al. Arch Gen Psychiatry. 1995;52:1048-60.
3mW 9m Years
94%
47%
42%
30%?
Longitudinal Course of PTSD
Symptoms
-
7/28/2019 PTSD english
11/44
Risk Factors for PTSD
Severity of trauma (ie, threat, duration, injury, loss)
Prior traumatization
Gender
Ethnicity Prior mood and/or anxiety disorders
Family history of mood or anxiety disorders
Education
-
7/28/2019 PTSD english
12/44
Screening Questions for
PTSDWhats the worst thing that ever happened toyou?
How did you react when it happened?
Do memories of _______ still bother you? Didyou get over it?
Do you avoid situations that might remind you of
____? Have your relationships suffered because of____?
Have you become more nervous since ___? Is ithard for you to relax because of ____?
-
7/28/2019 PTSD english
13/44
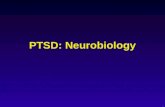
Functional Neuroanatomy of Traumatic Stress
Amygdala
Hippocampus
Locus Coeruleus
Pituitary
Hypothalamus
OrbitofrontalCortex
Cerebral Cortex
Adrenal
CRF
ACTH NE
Extinction to fearthrough amygdala
inhibition
Long-term storage oftraumatic memories
Conditioned fear
Cortisol
Output tocardiovascularsystem
Prefrontal
Cortex
Parietal Cortex Stress
Attention and vigilance - fear behaviorDose response effect on metabolism
Glutamate
-
7/28/2019 PTSD english
14/44
PTSD Treatment Options
Psychotherapy
Pharmacotherapy
Complementary Alternative
Interventions
Yoga
Exercise
Meditation
Multimodal treatment
-
7/28/2019 PTSD english
15/44
Early Post-Trauma Interventions Crisis InterventionsShort cognitive behavioral therapy (CBT):
Psychological Debriefingequivocal or harmful
Cognitive Behavioral Prevention Programs: Prolonged Exposure (PE) Prolonged Exposure + Stress Inoculation Training (PE/SIT)
Psychotherapy Brief dynamic psychotherapy for traumatic grief Supportive counseling Spiritual counseling
Pharmacotherapy Propranolol
Foa EB, et al. J Clin Psychiatry. 1999;60(suppl 16):1-34.
Mitchell JT. JEMS. 1983;8:36-9.
-
7/28/2019 PTSD english
16/44
Psychological Treatments for
Chronic PTSD
Psychotherapy
Exposure therapy
Cognitive processing therapy
Anxiety managementAdditional treatments
Eye Movement Desensitization andReprocessing (EMDR)
Hypnotherapy
Psychodynamic therapy
Expressive therapies
-
7/28/2019 PTSD english
17/44
Treatment
Psychotherapy is the treatment of choice
Meds are not the primary treatment but should
target specific symptoms as they arise
Restoring a sense of control over emotions
-
7/28/2019 PTSD english
18/44
Issues with pharmacological treatment
Efficacy across symptom clusters
Comorbidity/Associated sxs
depression and substance abuse common
guilt, shame, distrust significant marital, occupational, financial, health problems
Discontinuation of meds original symptoms returning
Response to meds not guaranteed
Changes not necessarily large
-
7/28/2019 PTSD english
19/44
Medication
Selective Serotonin Reuptake Inhibitors Benzodiazepines Tricyclic Antidepressants (TCAs)
-
7/28/2019 PTSD english
20/44
TCAs
1st antidepressants used
Prevent reuptake of monoamines (serotonin ornorepinephrine) by the presynaptic neurons in the CNS,thus prolonging the effects of these NTs
Numerous side effects: blurred vision, dry mouth, constipation,weight gain, dizziness when changing position, increased sweating,difficulty urinating, changes in sexual desire, decrease in sexualability, muscle twitches, fatigue and weakness
Overdose delirium, hypotension, cardiac arrhythmiasand death.
-
7/28/2019 PTSD english
21/44
SSRIs
1st line of treatment
Antidepressants that block reuptake of serotonin at
presynaptic neurons in the brain
Side effects: nausea, sweating, fatigue, sleepiness, andsexual side effects.
Generally safer than TCAs if overdose is taken
-
7/28/2019 PTSD english
22/44
Benzodiazepines
Relatively fast-acting
Use has declined
concerns over dependence and abuse
Lower anxiety by vigilance, eliminating muscle tension,
and causing sedation
act on the g-aminobutyric acid (GABA)/benzodiazepine (BZ)
receptor complex
Side effects: concentration problems, a mild form of amnesia,drowsiness and a loss of coordination; fatigue and mental slowing or
confusion
dangerous to drive or operate heavy machinery
-
7/28/2019 PTSD english
23/44
Cognitive behavioral therapy
(CBT) interventions designed to change the way
people think about and understand
situations and behaviors. This reduces the
frequency of distressing negative reactionsand emotions.
-
7/28/2019 PTSD english
24/44
PTSD Thinking Distortions
Two erroneous beliefs
the world is dangerous and the individual with PTSD is incompetent.
CBT is used to change these beliefs, and
successful CBT will result in the patient no
longer believing that the world is
dangerous or that they are incompetent
-
7/28/2019 PTSD english
25/44
CBT normally lasts from 9-12 individual
sessions, lasting about 60-90 minutes,
administered once or twice weekly.
Patients are normally also assignedhomework to practice specific
interventions on their own between
sessions.
-
7/28/2019 PTSD english
26/44
The most often used
interventions include exposure therapy stress inoculation training (SIT) cognitive restructuring These therapies may be used on their own
or they may be combined. Another type of
CBT is eye movement desensitization and
reprocessing (EMDR).
-
7/28/2019 PTSD english
27/44
Exposure Therapy
Exposure therapy is a treatment designed to
help you confront safe but feared
thoughts, situations, objects, people,
places, or activities. These thingselicit anxiety in the PTSD sufferer and are
avoided, which takes a negative toll on
everyday life.
http://www.epigee.org/mental_health/anxietyvspanic.htmlhttp://www.epigee.org/mental_health/anxietyvspanic.html -
7/28/2019 PTSD english
28/44
The goal of exposure therapy
help the individual
confront and process traumatic memories and
correct erroneous thoughts about the world
and the self that derive from them.
-
7/28/2019 PTSD english
29/44
PTSD patients are also exposed to real life
situations and objects that trigger anxiety andavoidance.
Each person, place, situation and activity thattriggers anxiety and avoidance is identified and
evaluated for safety and relevance to thepatient's normal functioning.
Then these things are repeatedly confronted
until anxiety and avoidance centered on them
goes away. Therapy starts small and works its
way to more feared and challenging situations
-
7/28/2019 PTSD english
30/44
Exposure therapy designed for PTSD involvesimaginative exposure to the trauma memory.
The patient is instructed to close her eyes and
remember the traumatic event by imagining thatit's currently happening.
They will provide detailed descriptions of all
thoughts, physical sensations, and emotional
reactions to the memory. This is repeated
several times over the course of therapy and it is
taped to be listened to later as homework.
-
7/28/2019 PTSD english
31/44
Stress Inoculation Training
Teaching the PTSD sufferer how to manage their
anxiety reactions to situations, memories, etc.They normally fear and avoid.
For the physical manifestations : controlledbreathing and progressive muscle relaxation.
For intrusive thoughts and worrying: how to
interrupt their thought patterns and think of
positive imagery.
-
7/28/2019 PTSD english
32/44
Cognitive Restructuring
helps patients identify and challenge theirerroneous beliefs and interpretations.
It is based on the idea that it is not actual
events that cause negative emotional
reaction but the interpretation of thoseevents.
-
7/28/2019 PTSD english
33/44
Cognitive restructuring seeks to replace worry
and anxiety with more positive and productiveemotions through the way a patient thinks.
People undergoing this therapy are taught tolook at their negative beliefs and evaluate the
pros and cons of maintaining them. They
carefully consider the likelihood of their fears
and the cost of those outcomes and look forpossible alternative explanations and ways of
thinking.
-
7/28/2019 PTSD english
34/44
34
Approach to Trauma Treatment
Evaluation and Assessment
Type of trauma & Type of trauma client
Safety
Risk assessment
Mental status & co-morbid disorders
Medical History
Family and occupational functioning
Medication
-
7/28/2019 PTSD english
35/44
35
Approach to Trauma Treatment
Psychoeducation about trauma
Coordination of care with medical providers
Affect management skills
Safe place exercise, grounding Container method
Calming the body down
Meditation, breathing
Yoga, chanting
Integration of Traumatic Memories via EMDR
-
7/28/2019 PTSD english
36/44
36
What is Eye-Movement Desensitization
and Reprocessing (EMDR)?
A type of psychotherapy for treating
emotional difficulties that are caused by
disturbing life experiences, ranging
from traumatic events such as combat
stress, assaults to upsetting events.
EMDR is also being used to alleviate
performance anxiety, generalized
anxiety, sleep disturbances, phobias,
grief, relapse prevention, andperformance enhancement.
Francine Shapiro
Adaptive Information Processing: A
-
7/28/2019 PTSD english
37/44
37
Adaptive Information Processing: A
Theoretical Model(Parnell, 2007; Shapiro, 1995)
We all have an information processing system
through which new experiences and information
are processed to an adaptive state.
Trauma or disturbing experiences becometrapped in the nervous system.
In EMDR, we ask the patient to focus on a target
memory.
-
7/28/2019 PTSD english
38/44
38
Adaptive Information Processing
Continued
When information stored in memory networks
related to a distressing or traumatic
experience is not fully processed it gives rise
to dysfunctional reactions. Eye movements or BLS stimulates
accelerated information processing.
The goal is to reach adaptive resolution -reduce vivid imagery and related affect & shift
negative beliefs about oneself.
-
7/28/2019 PTSD english
39/44
39
The Eight Phases of EMDR Treatment
The 8 phases of the EMDR protocol
represent a comprehensive treatment
approach.
1. Client History and Treatment Planning
2. Client Preparation
3. Assessment
-
7/28/2019 PTSD english
40/44
HOW WAS EMDR DEVELOPED?
Discovered and Developed by Francine Shapiro1987
She noticed that :
Disturbing Anxious Thoughts
Changed with spontaneous eye movements to:
LESS DISTURBING THOUGHTS LEADING
TO ADAPTIVE RESOLUTION
(ie. The negative charge was greatly
reduced)
-
7/28/2019 PTSD english
41/44
1987
EMDR : Eye Movement Desensitization
1990EMDR :
Eye Movement
Desensitization & Reprocessing
( Processed Traumatic Memories Into
Something More Adaptive And Functional)
-
7/28/2019 PTSD english
42/44
WHAT HAPPENS DURING EMDR?
TRAUMATIC MEMORY MEMORYEMDR
State-specific Form
In Implicit Memory
(Right Hemisphere)
Less disturbing Image, a
Positive Cognition,Appropriate Affect without
disturbing Physical
Sensations
Functional Form In
Explicit Memory
(Left Hemisphere)
Associated with disturbing
Image, Cognitions,Affect, Physical
Sensations
(fragmented, not integrated)
Re-experiencingTimeless RememberingSense of time
-
7/28/2019 PTSD english
43/44
HOW DOES EMDR WORK?
Not entirely clear! EMDR induces changes in regional brain
activation similar to REM sleep
EMDR increases prefrontal lobe activationleading to more appropriate responses totriggers
The Eye Movements or other dual
attention stimuli elicit an OrientingResponse which disrupts the traumaticmemory network, interrupting previouslinks to negative emotions and allows
integration of new information
-
7/28/2019 PTSD english
44/44
HOW DOES EMDR WORK?
EMDR has evolved into a synthesis oftraditional orientations:
Aspects of CBT
Brief /Interrupted exposure Free Association :
Directed and Non-directed
Focus on physical sensations
Dual attention stimulation