Efficacy of Psychotherapy for Borderline Personality Disorder

1
Psychotherapy in MS Patients with Dementia and Personality Changes
Ralph HB Benedict, PhD
Professor of Neurology
University at Buffalo, State University of New York
Research Support from the NIH, National MS Society, and Industry
Acknowledgements:
Bianca Weinstock‐Guttman MD
Robert Zivadinov MD
Murali Ramanathan PhD
Channa Kolb MD, David Hojnacki MD, Meg Bucello NP
Jonathan Rodgers PhD, Audrey Smerbeck PhD, Adam Booth MA, Seth Frndek BS, Carrie Fisher BA, Allison Drake BA, Victoria Kordovski BA, Claire Modica BS, Maria Pollack, Kelly Couglin, Joy Parrish PhD
Disclosures:Accorda, Bayer, Biogen Idec, EMD Serono, Genzyme, Genentech, Novartis, Questor
2
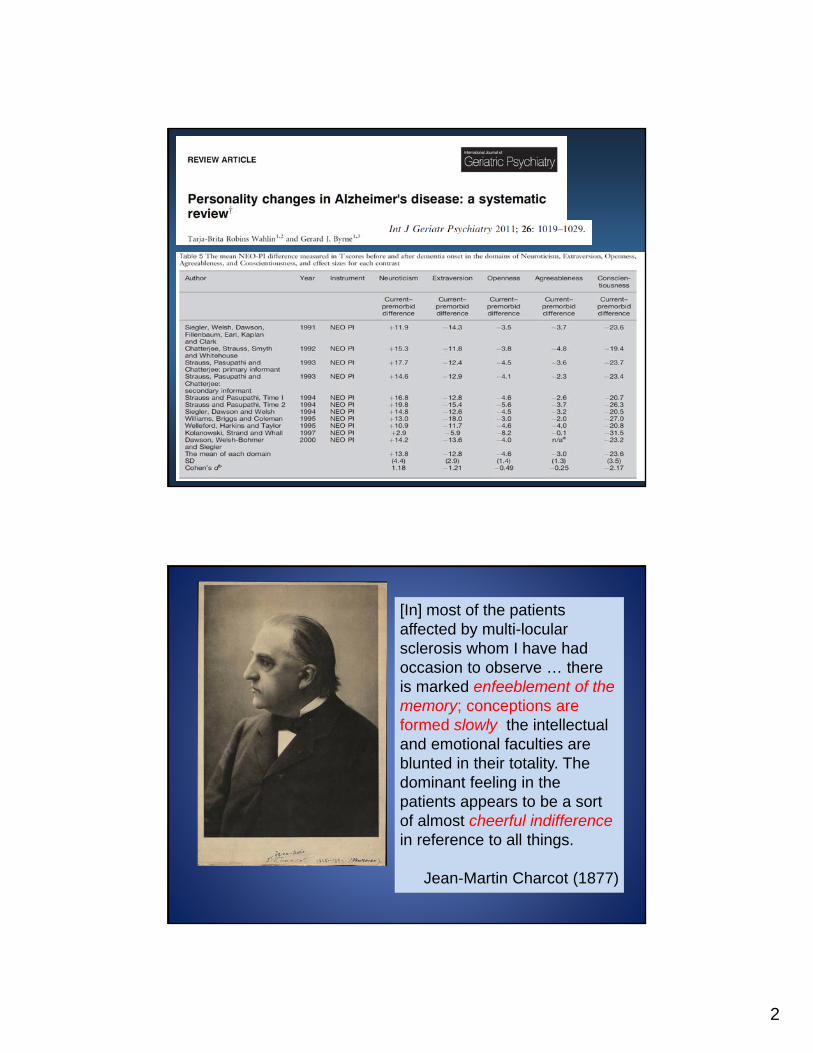
[In] most of the patients affected by multi-locularsclerosis whom I have had occasion to observe … there is marked enfeeblement of the memory; conceptions are formed slowly; the intellectual and emotional faculties are blunted in their totality. The dominant feeling in the patients appears to be a sort of almost cheerful indifferencein reference to all things.
Jean-Martin Charcot (1877)
3
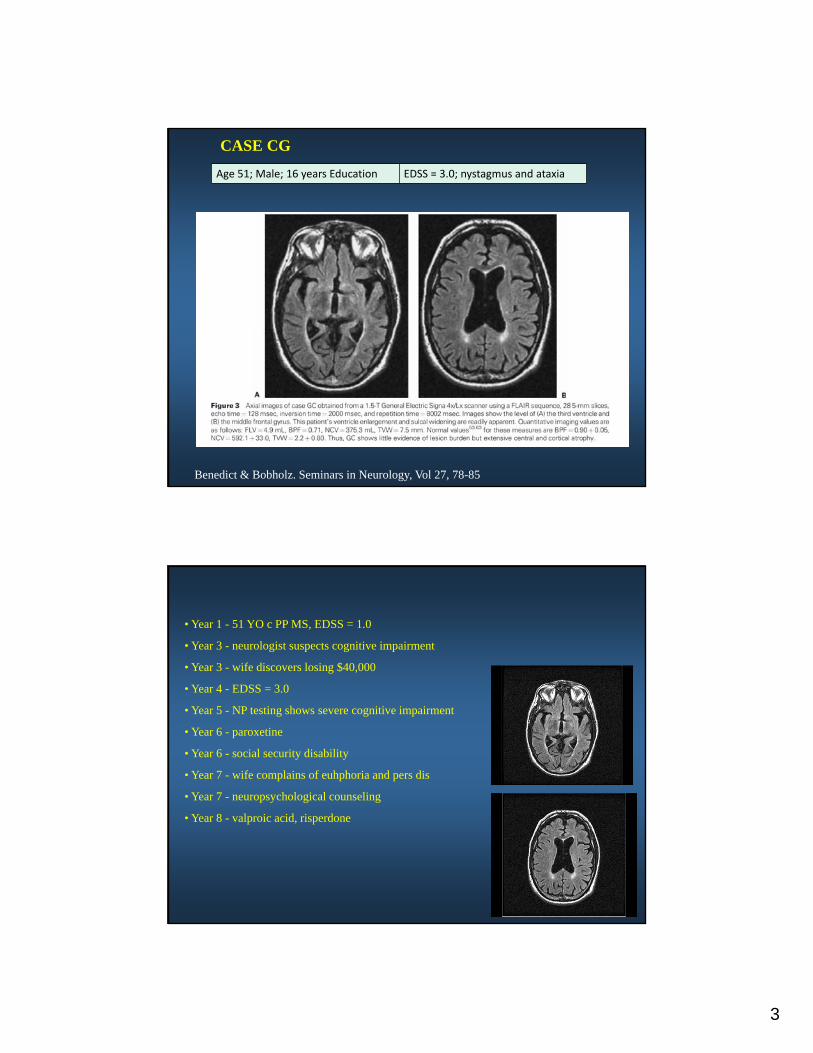
Benedict & Bobholz. Seminars in Neurology, Vol 27, 78-85
Age 51; Male; 16 years Education EDSS = 3.0; nystagmus and ataxia
CASE CG
• Year 1 - 51 YO c PP MS, EDSS = 1.0
• Year 3 - neurologist suspects cognitive impairment
• Year 3 - wife discovers losing $40,000
• Year 4 - EDSS = 3.0
• Year 5 - NP testing shows severe cognitive impairment
• Year 6 - paroxetine
• Year 6 - social security disability
• Year 7 - wife complains of euhphoria and pers dis
• Year 7 - neuropsychological counseling
• Year 8 - valproic acid, risperdone
4
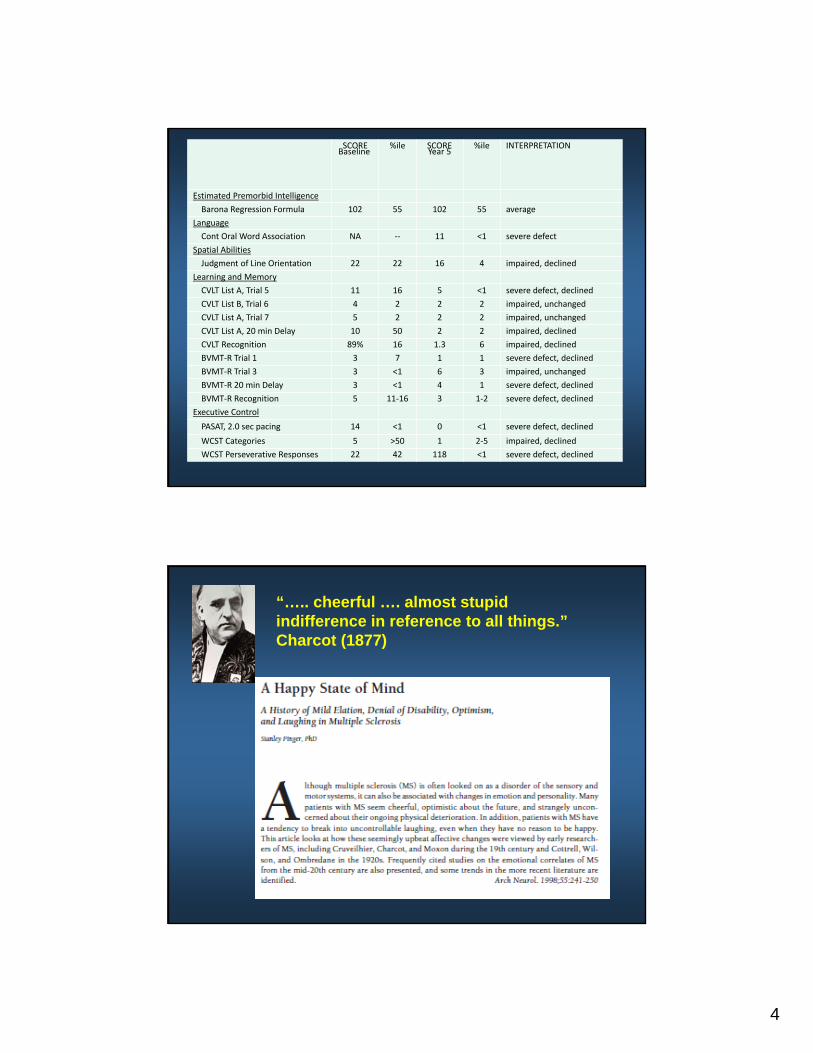
SCOREBaseline
%ile SCORE Year 5
%ile INTERPRETATION
Estimated Premorbid Intelligence
Barona Regression Formula 102 55 102 55 average
Language
Cont Oral Word Association NA ‐‐ 11 <1 severe defect
Spatial Abilities
Judgment of Line Orientation 22 22 16 4 impaired, declined
Learning and Memory
CVLT List A, Trial 5 11 16 5 <1 severe defect, declined
CVLT List B, Trial 6 4 2 2 2 impaired, unchanged
CVLT List A, Trial 7 5 2 2 2 impaired, unchanged
CVLT List A, 20 min Delay 10 50 2 2 impaired, declined
CVLT Recognition 89% 16 1.3 6 impaired, declined
BVMT‐R Trial 1 3 7 1 1 severe defect, declined
BVMT‐R Trial 3 3 <1 6 3 impaired, unchanged
BVMT‐R 20 min Delay 3 <1 4 1 severe defect, declined
BVMT‐R Recognition 5 11‐16 3 1‐2 severe defect, declined
Executive Control
PASAT, 2.0 sec pacing 14 <1 0 <1 severe defect, declined
WCST Categories 5 >50 1 2‐5 impaired, declined
WCST Perseverative Responses 22 42 118 <1 severe defect, declined
“….. cheerful …. almost stupid indifference in reference to all things.”Charcot (1877)
5
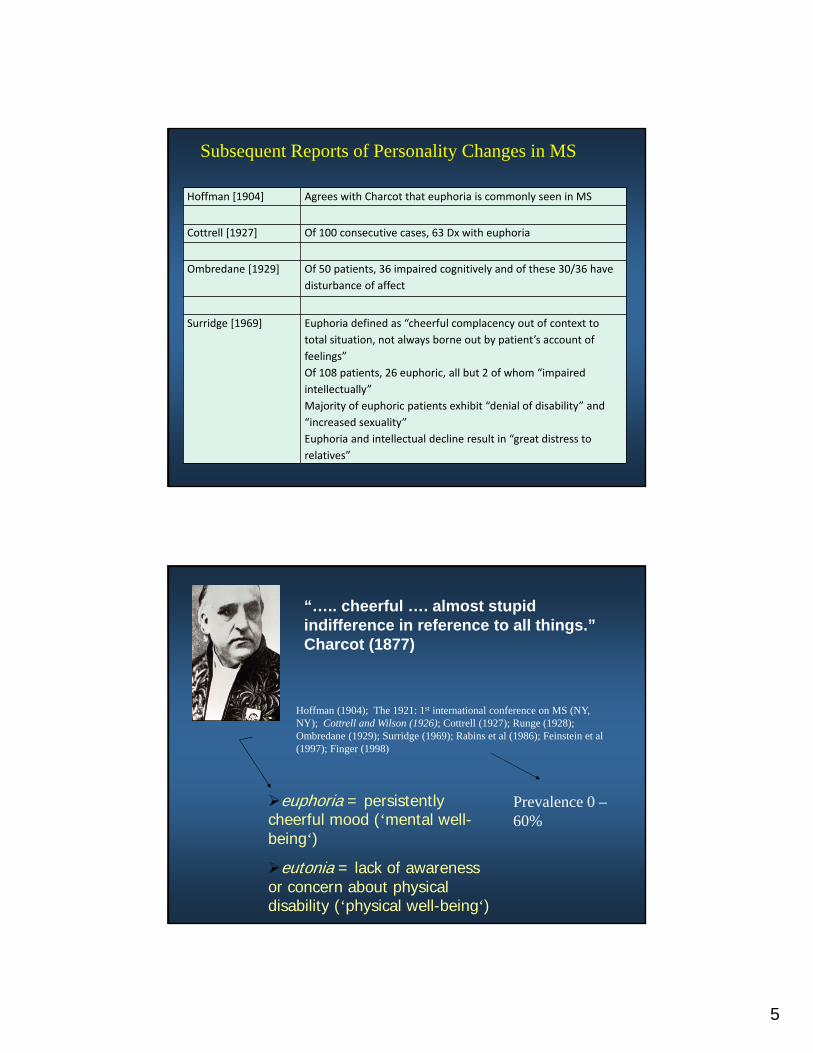
Hoffman [1904] Agrees with Charcot that euphoria is commonly seen in MS
Cottrell [1927] Of 100 consecutive cases, 63 Dx with euphoria
Ombredane [1929] Of 50 patients, 36 impaired cognitively and of these 30/36 have
disturbance of affect
Surridge [1969] Euphoria defined as “cheerful complacency out of context to
total situation, not always borne out by patient’s account of
feelings”
Of 108 patients, 26 euphoric, all but 2 of whom “impaired
intellectually”
Majority of euphoric patients exhibit “denial of disability” and
“increased sexuality”
Euphoria and intellectual decline result in “great distress to
relatives”
Subsequent Reports of Personality Changes in MS
“….. cheerful …. almost stupid indifference in reference to all things.”Charcot (1877)
Hoffman (1904); The 1921: 1st international conference on MS (NY, NY); Cottrell and Wilson (1926); Cottrell (1927); Runge (1928); Ombredane (1929); Surridge (1969); Rabins et al (1986); Feinstein et al (1997); Finger (1998)
euphoria = persistently cheerful mood (‘mental well-being‘)
eutonia = lack of awareness or concern about physical disability (‘physical well-being‘)
Prevalence 0 –60%
6
NeuroticExtrovert
OpenAgreeable
ConsciEmpathic
MS
30
35
40
45
50
55
60
65
MS Normal
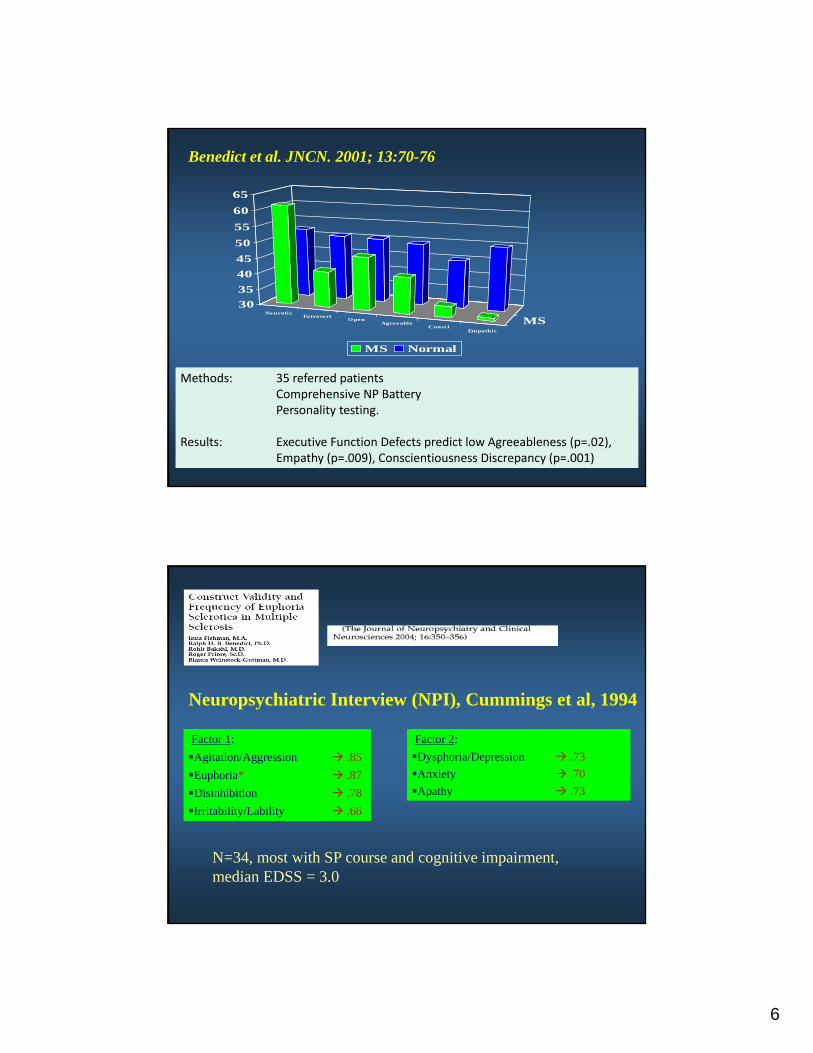
Methods: 35 referred patientsComprehensive NP BatteryPersonality testing.
Results: Executive Function Defects predict low Agreeableness (p=.02), Empathy (p=.009), Conscientiousness Discrepancy (p=.001)
Benedict et al. JNCN. 2001; 13:70-76
Neuropsychiatric Interview (NPI), Cummings et al, 1994
Factor 1:
Agitation/Aggression .85
Euphoria* .87
Disinhibition .78
Irritability/Lability .66
Factor 2:
Dysphoria/Depression .73
Anxiety .70
Apathy .73
N=34, most with SP course and cognitive impairment, median EDSS = 3.0
7
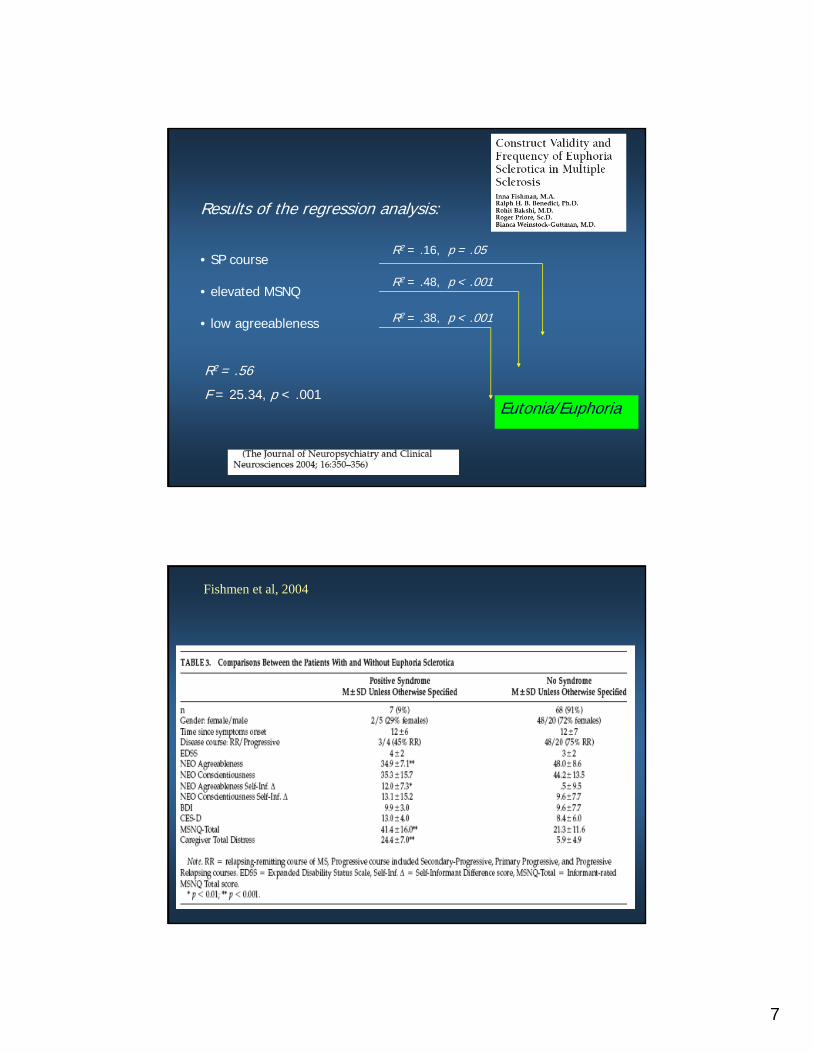
Results of the regression analysis:
• SP course
• elevated MSNQ
• low agreeableness
Eutonia/Euphoria
R2 = .56
F = 25.34, p < .001
R2 = .16, p = .05
R2 = .48, p < .001
R2 = .38, p < .001
Fishmen et al, 2004
8
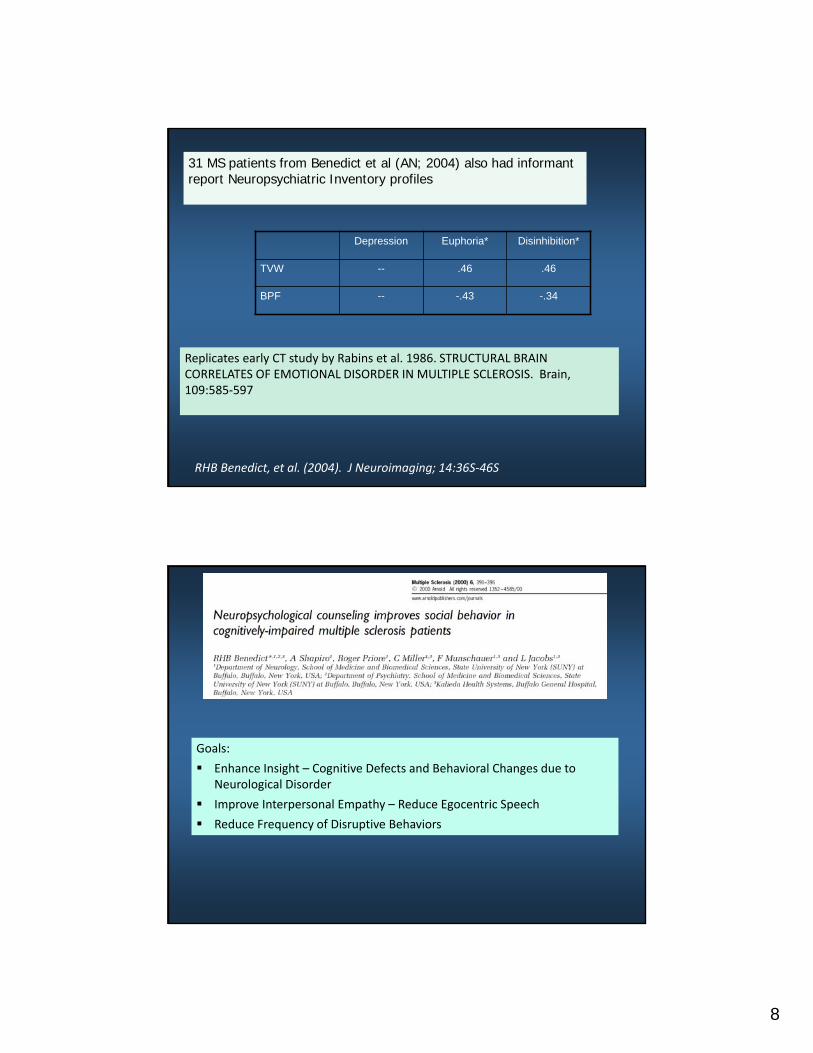
RHB Benedict, et al. (2004). J Neuroimaging; 14:36S‐46S
31 MS patients from Benedict et al (AN; 2004) also had informant report Neuropsychiatric Inventory profiles
Depression Euphoria* Disinhibition*
TVW -- .46 .46
BPF -- -.43 -.34
Replicates early CT study by Rabins et al. 1986. STRUCTURAL BRAIN CORRELATES OF EMOTIONAL DISORDER IN MULTIPLE SCLEROSIS. Brain, 109:585‐597
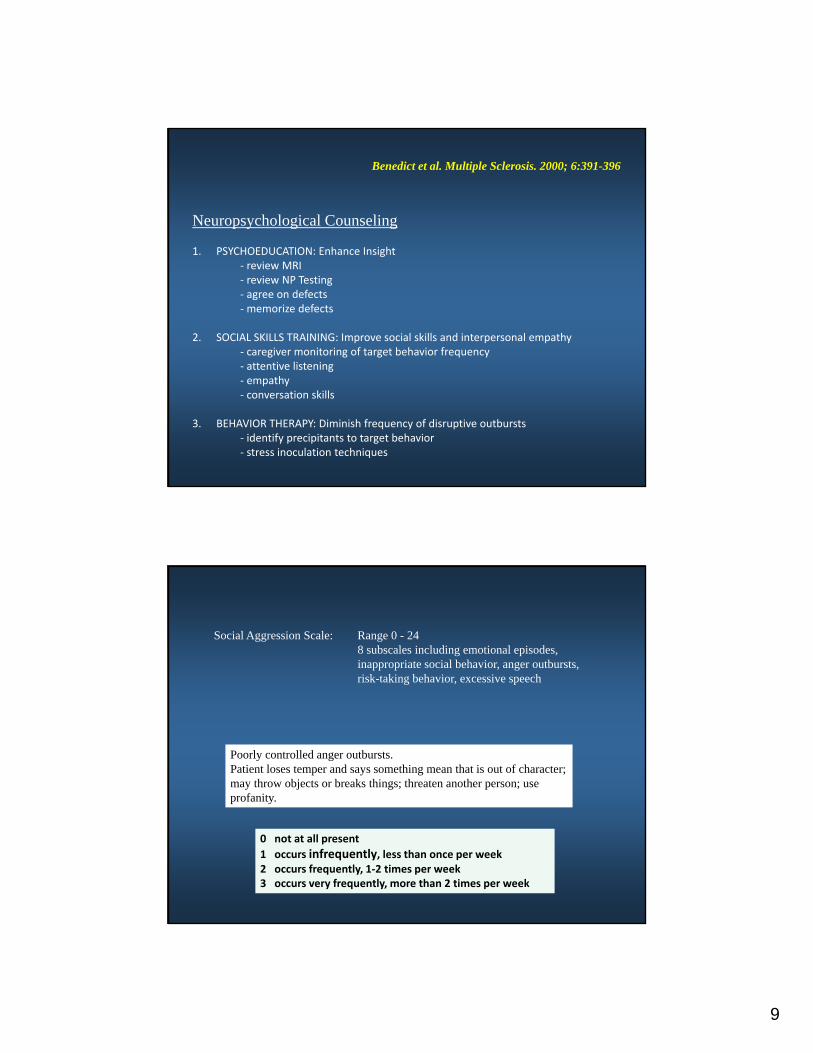
Neuropsychological Counseling
Goals:
Enhance Insight – Cognitive Defects and Behavioral Changes due to Neurological Disorder
Improve Interpersonal Empathy – Reduce Egocentric Speech
Reduce Frequency of Disruptive Behaviors
9
Neuropsychological Counseling
1. PSYCHOEDUCATION: Enhance Insight‐ review MRI‐ review NP Testing‐ agree on defects‐memorize defects
2. SOCIAL SKILLS TRAINING: Improve social skills and interpersonal empathy‐ caregiver monitoring of target behavior frequency‐ attentive listening‐ empathy‐ conversation skills
3. BEHAVIOR THERAPY: Diminish frequency of disruptive outbursts‐ identify precipitants to target behavior‐ stress inoculation techniques
Benedict et al. Multiple Sclerosis. 2000; 6:391-396
Social Aggression Scale: Range 0 - 248 subscales including emotional episodes, inappropriate social behavior, anger outbursts, risk-taking behavior, excessive speech
0 not at all present
1 occurs infrequently, less than once per week2 occurs frequently, 1‐2 times per week3 occurs very frequently, more than 2 times per week
Poorly controlled anger outbursts. Patient loses temper and says something mean that is out of character; may throw objects or breaks things; threaten another person; use profanity.
10
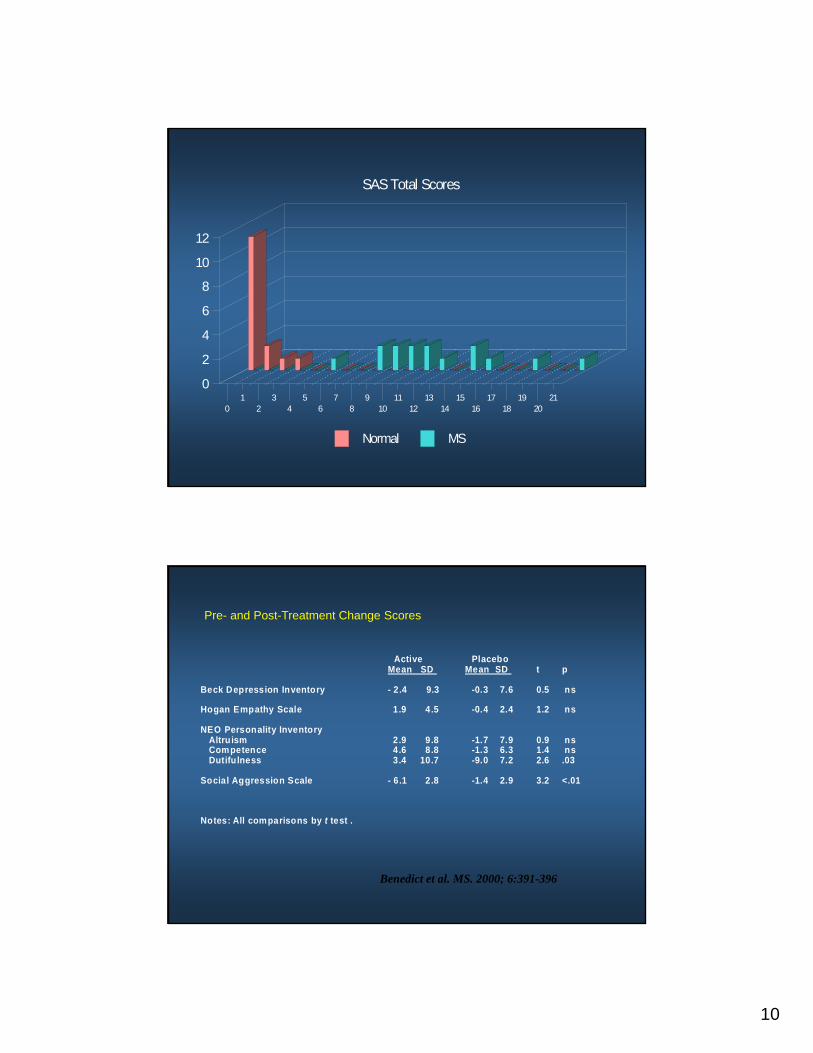
SAS Total Scores
Normal MS
01
23
45
67
89
1011
1213
1415
1617
1819
2021
0
2
4
6
8
10
12
Active PlaceboMean SD Mean SD t p
Beck Depression Inventory - 2.4 9.3 -0.3 7.6 0.5 ns
Hogan Empathy Scale 1.9 4.5 -0.4 2.4 1.2 ns
NEO Personality Inventory Altruism 2.9 9.8 -1.7 7.9 0.9 ns Competence 4.6 8.8 -1.3 6.3 1.4 ns Dutifulness 3.4 10.7 -9.0 7.2 2.6 .03
Social Aggression Scale - 6.1 2.8 -1.4 2.9 3.2 <.01
Notes: All comparisons by t test .
Pre- and Post-Treatment Change Scores
Benedict et al. MS. 2000; 6:391-396
11
0
2
4
6
8
10
12
14
16
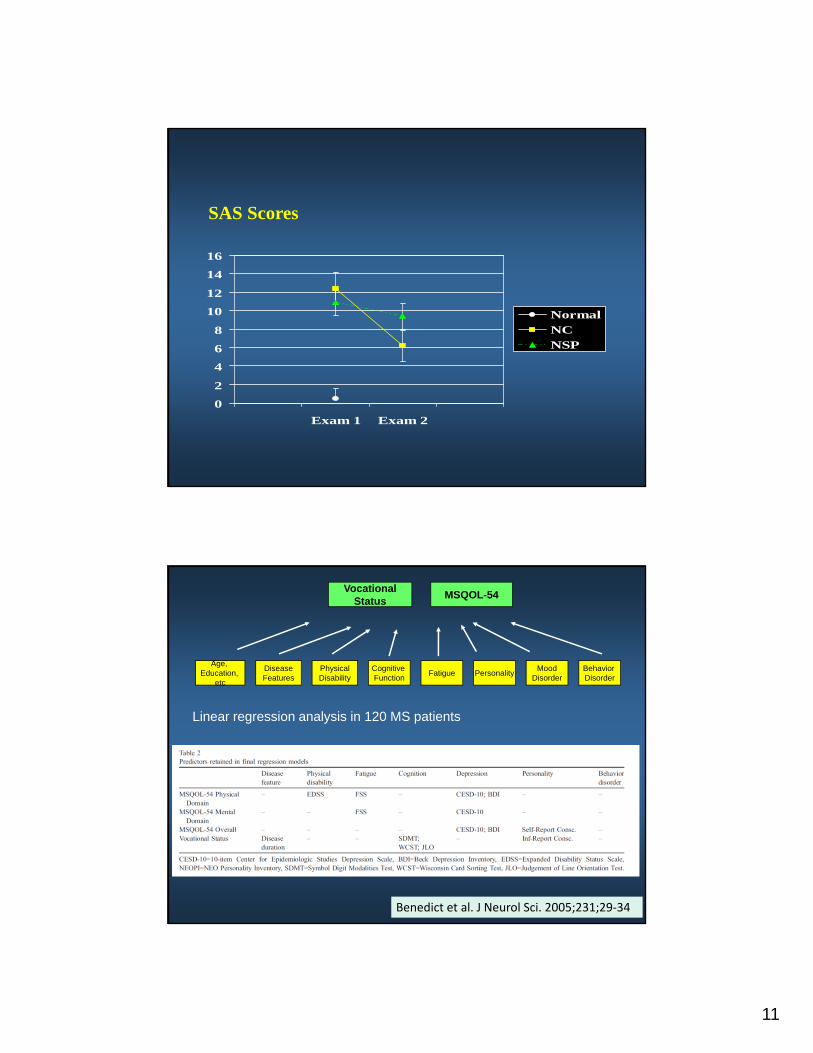
Exam 1 Exam 2
NormalNCNSP
SAS Scores
VocationalStatus
FatigueAge,
Education, etc
DiseaseFeatures
PhysicalDisability
Cognitive Function
MoodDisorder
PersonalityBehavior Disorder
MSQOL-54
Benedict et al. J Neurol Sci. 2005;231;29‐34
Linear regression analysis in 120 MS patients
12
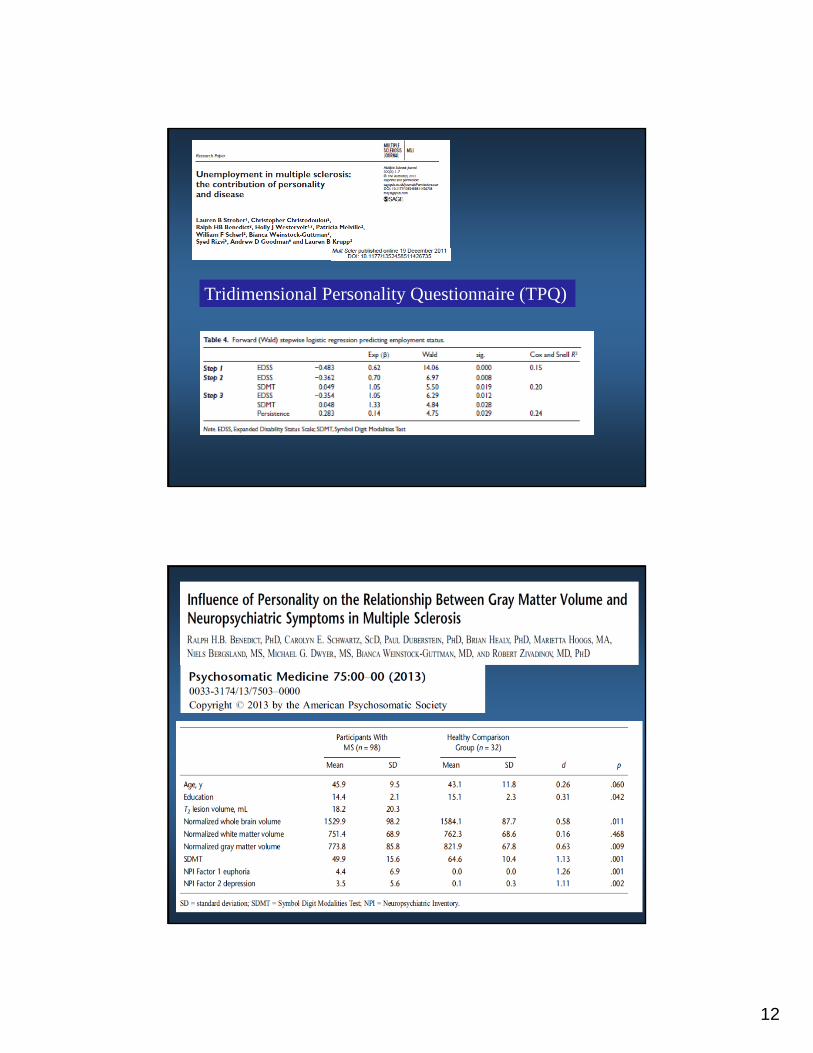
Tridimensional Personality Questionnaire (TPQ)
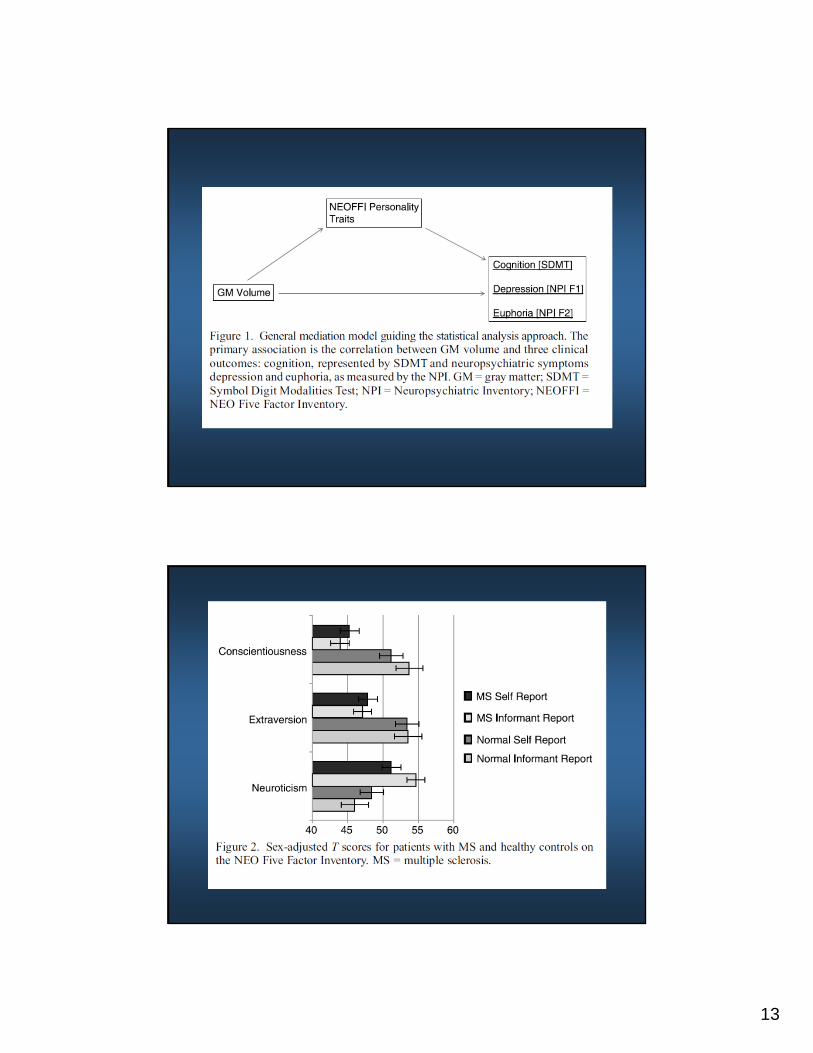
13
14
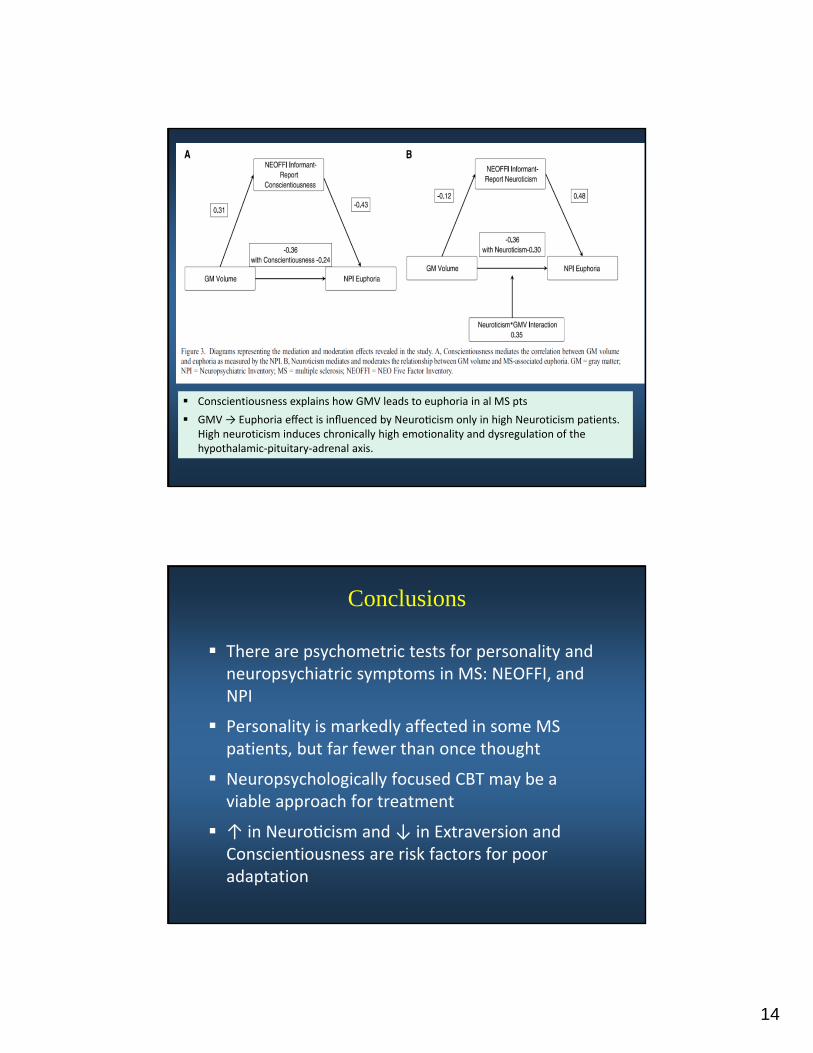
Conscientiousness explains how GMV leads to euphoria in al MS pts
GMV → Euphoria effect is influenced by Neuro cism only in high Neuroticism patients. High neuroticism induces chronically high emotionality and dysregulation of the hypothalamic‐pituitary‐adrenal axis.
Conclusions
There are psychometric tests for personality and neuropsychiatric symptoms in MS: NEOFFI, and NPI
Personality is markedly affected in some MS patients, but far fewer than once thought
Neuropsychologically focused CBT may be a viable approach for treatment
↑ in Neuro cism and ↓ in Extraversion and Conscientiousness are risk factors for poor adaptation
15
Thank You
Bianca Weinstock-Guttman MD
Robert Zivadinov MD; Murali Ramanathan PhD
David Hojnacki MD; Channa Kolb MD
Margaret Bucello NP; Audrey Smerbeck PhD
Jonathan Rodgers PhD, Natalie Emmert BA