Psoriasis - Iowa Nurse Practitioner Society - Home · Clinical Pearls for Diagnosis ... diagnosing...
20
1 Learning Objectives Upon completion of this educational activity, participants should be able to: • Summarize the epidemiology and pathophysiology of psoriasis and PsA. • Describe the diagnosis, disease classification, and assessment associated with psoriasis and PsA. • Incorporate patient preferences and shared decision making into tailored treatment plans for patients with psoriasis and PsA. • Evaluate the efficacy and safety of recently available therapies for the management of psoriasis and PsA. Psoriasis
Transcript of Psoriasis - Iowa Nurse Practitioner Society - Home · Clinical Pearls for Diagnosis ... diagnosing...
1
Learning ObjectivesUpon completion of this educational activity, participants should be able to:• Summarize the epidemiology and pathophysiology
of psoriasis and PsA.• Describe the diagnosis, disease classification, and
assessment associated with psoriasis and PsA.• Incorporate patient preferences and shared
decision making into tailored treatment plans for patients with psoriasis and PsA.
• Evaluate the efficacy and safety of recently available therapies for the management of psoriasis and PsA.
Psoriasis
2
Psoriasis
• Chronic, immune-mediated skin disease– Most common autoimmune disease– Correlation between skin and systemic
inflammation
• High comorbidity burden
• Affects almost 8 million Americans
Rachakonda TD, et al. J Am Acad Dermatol. 2014;70(3):512-516; Eder L, et al. Arthritis Rheumatol. 2016;68(4):915-923; Helmick CG, et al. Am J Prev Med. 2014;47(1):37-45; Nestle FO, et al. N Engl J Med. 2009;361(5):496-509.
Psoriasis
Tollefson MM, et al. J Am Acad Dermatol. 2010;62(6):979-987; Icen M, et al. J Am Acad Dermatol. 2009;60(3):394-401; Rachakonda TD, et al. J Am Acad Dermatol. 2014;70(3):512-516; Helmick CG, et al. Am J Prev Med. 2014;47(1):37-45.
050
100150200250300
18-29 30-39 40-49 50-59 60-69 70-79 >80
# o
f P
ati
en
ts w
ith
P
so
ria
sis
Age in Years
Men
Women
Psoriasis in Adults (n=2564)
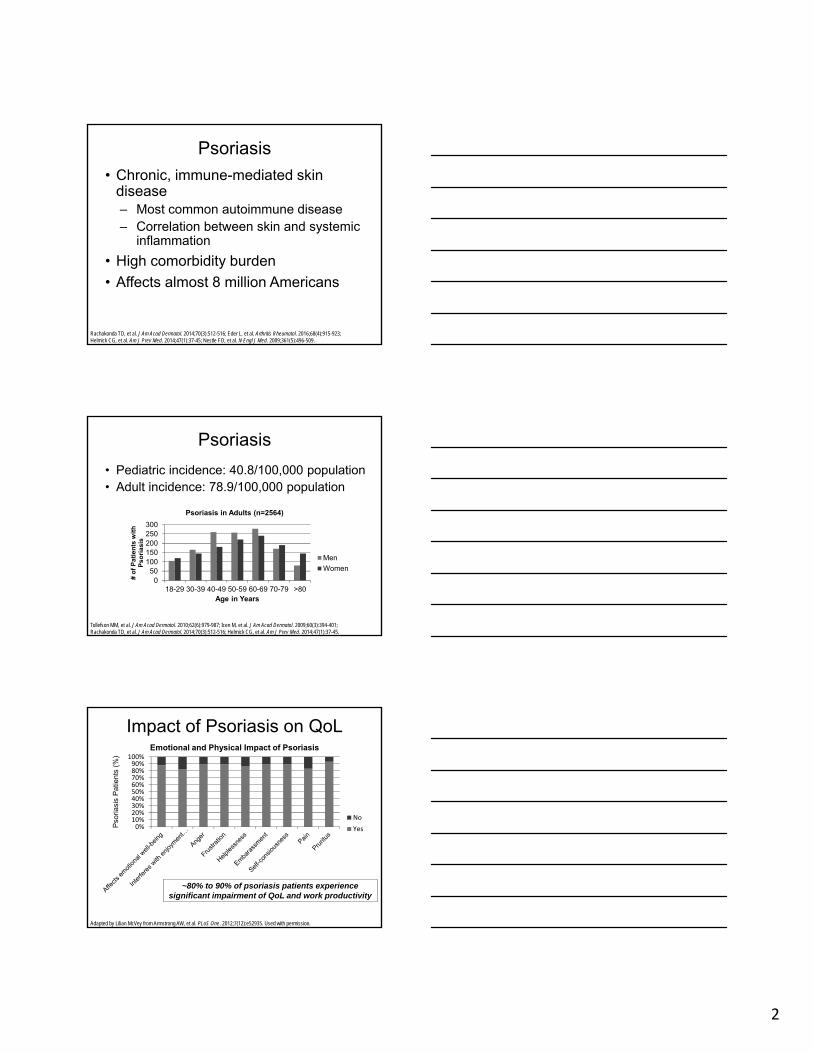
• Pediatric incidence: 40.8/100,000 population• Adult incidence: 78.9/100,000 population
0%10%20%30%40%50%60%70%80%90%
100%
No
Yes
Impact of Psoriasis on QoLEmotional and Physical Impact of Psoriasis
Pso
riasi
s P
atie
nts
(%)
Adapted by Lilian McVey from Armstrong AW, et al. PLoS One. 2012;7(12):e52935. Used with permission.
~80% to 90% of psoriasis patients experience significant impairment of QoL and work productivity
3
Pathogenesis
Ainsworth C. Nature. 2012;492(7429):S52-S54. Used with permission.
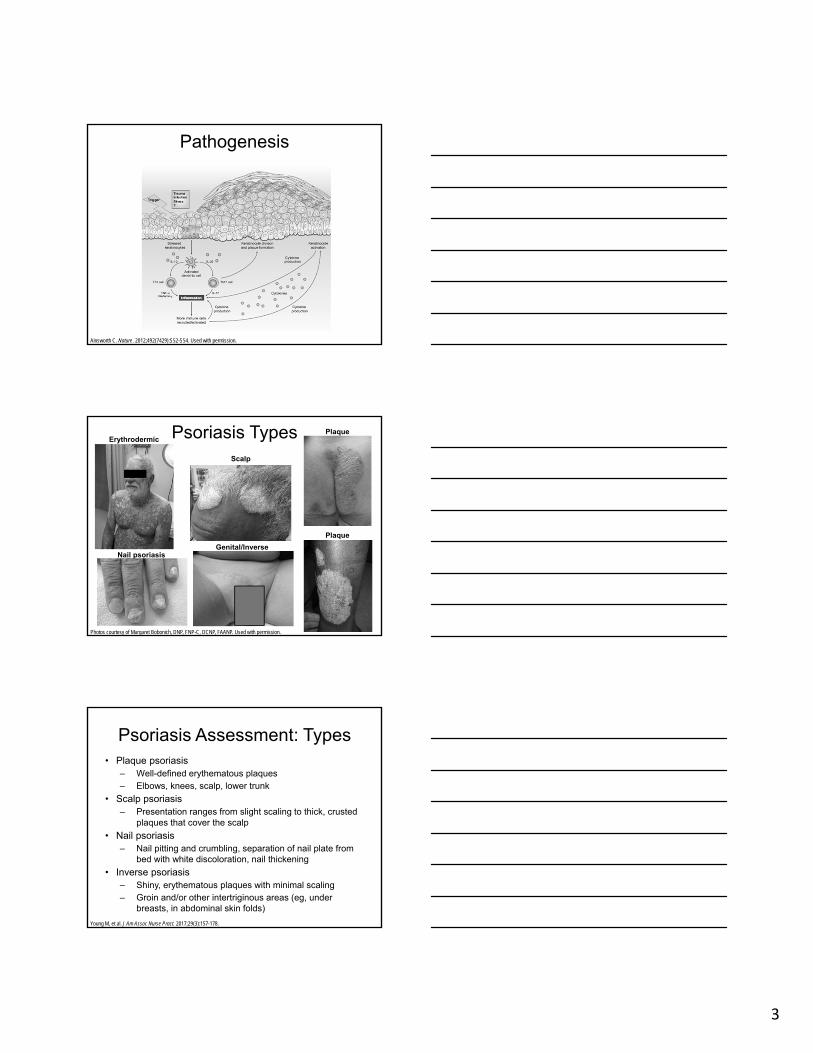
Psoriasis Types
Photos courtesy of Margaret Bobonich, DNP, FNP-C, DCNP, FAANP. Used with permission.
Erythrodermic
Nail psoriasis
Scalp
Genital/Inverse
Plaque
Plaque
Psoriasis Assessment: Types• Plaque psoriasis
– Well-defined erythematous plaques– Elbows, knees, scalp, lower trunk
• Scalp psoriasis– Presentation ranges from slight scaling to thick, crusted
plaques that cover the scalp
• Nail psoriasis– Nail pitting and crumbling, separation of nail plate from
bed with white discoloration, nail thickening
• Inverse psoriasis– Shiny, erythematous plaques with minimal scaling– Groin and/or other intertriginous areas (eg, under
breasts, in abdominal skin folds)
Young M, et al. J Am Assoc Nurse Pract. 2017;29(3):157-178.
4
Psoriasis Assessment: Types (cont’d)• Pustular psoriasis
– Eruption of sterile pustules– Generalized and extensive or localized to existing plaques
• Palmoplantar pustular psoriasis– Yellow-brown sterile pustules on hands and feet– May include scaling and severe pruritis
• Erythrodermic psoriasis– Generalized exfoliative dermatitis, often with hair loss
and nail dystrophy– Affects large body surface area (BSA); ≥80%
• Guttate psoriasis– Small, scattered, pink, oval-shaped papules
w/silvery scaling– Affects trunk and extremities
Young M, et al. J Am Assoc Nurse Pract. 2017;29(3):157-178.
Psoriasis Assessment• Comprehensive exam• Medication history• Assess for comorbidity
– Psoriatic arthritis (PsA) and other arthropathies
– Diabetes– Hyperlipidemia– Obesity– Cardiovascular disease– Malignancy– Depression
• Differential diagnoses– Eczema– Contact dermatitis– Seborrheic dermatitis– Drug eruption– Tinea infections– Pityriasis rosea– Lichen planus– Candidal intertrigo– Onychomycosis
Psoriasis can be difficult to diagnose…When in doubt, REFER!
Young M, et al. J Am Assoc Nurse Pract. 2017;29(3):157-178.
Clinical Pearls for Diagnosis
• Distribution– Eczema common on flexors– Psoriasis common on extensors
• Auspitz sign• Well-defined
– vs eczema with diffuse border
• Consider treatment secondary infection– Inverse psoriasis vs candidiasis vs intertrigo
• Skin biopsy if unsure (punch biopsy)
5
Psoriasis Assessment: Severity
• Scoring tools:– PASI: Psoriasis Area and Severity Index
– BSA: Body Surface Area
– DLQI: Dermatology Life Quality Index
• Remember:– Severity ≠ amount of area affected
– Consider Area(s) of involvement
Palms, genitals, soles, scalp, nails
Interference with QoL
US Perspectives: MAPP Survey
• Multinational Assessment of Psoriasis and Psoriatic Arthritis (MAPP) survey– N=1,005 patients, 101 dermatologists, and
100 rheumatologists
• Key findings– Both psoriasis and PsA remain undertreated
in patients with moderate-to-severe disease– Gaps in care include screening, assessing,
diagnosing and treating psoriasis patients with symptoms of PsA
Lebwohl MG, et al. Am J Clin Dermatol. 2016;17(1):87-97.
US Perspectives: MAPP Survey
• Key findings (cont’d)– Widespread dissatisfaction with current
treatment options Lack of efficacy
Long-term safety unknown
Administration challenges
Cost
– Difference in perceptions of severity, treatment impact in patients vs clinicians
Lebwohl MG, et al. Am J Clin Dermatol. 2016;17(1):87-97.
6
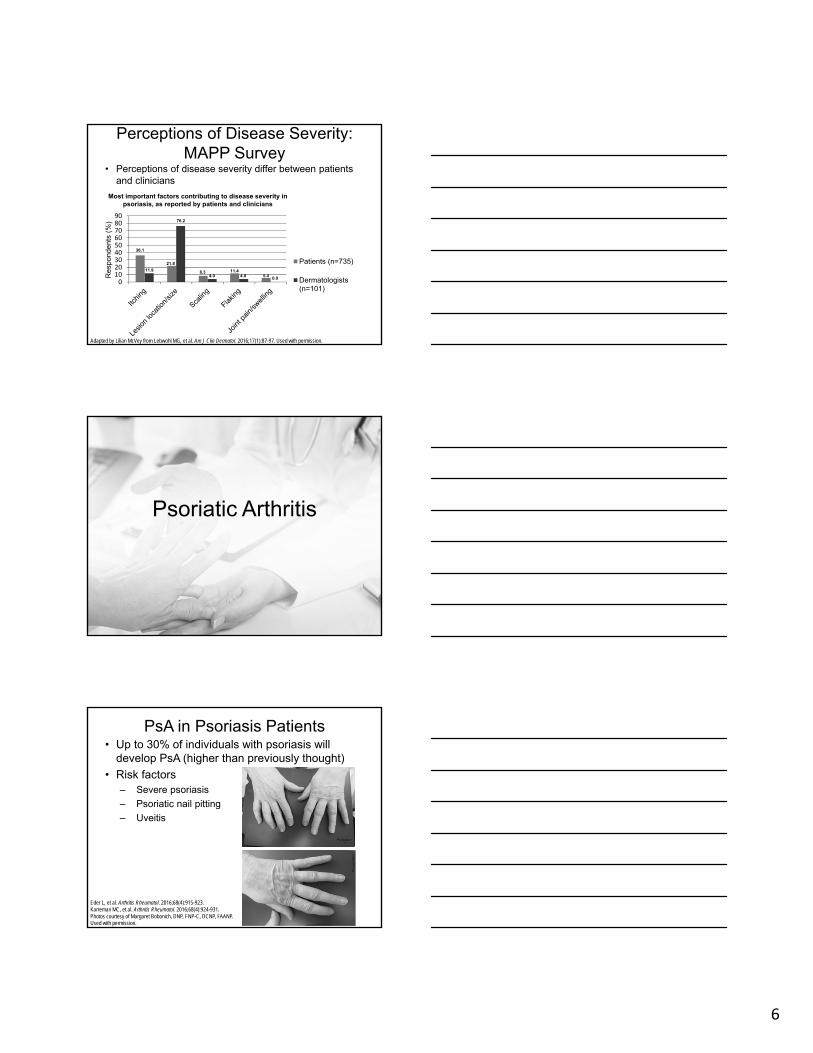
Perceptions of Disease Severity: MAPP Survey
• Perceptions of disease severity differ between patients and clinicians
Adapted by Lilian McVey from Lebwohl MG, et al. Am J Clin Dermatol. 2016;17(1):87-97. Used with permission.
0102030405060708090
Patients (n=735)
Dermatologists(n=101)
Res
pond
ents
(%
)
36.1
11.9
21.8
76.2
8.34.0
11.44.0 5.4 0.0
Most important factors contributing to disease severity in psoriasis, as reported by patients and clinicians
Psoriatic Arthritis
PsA in Psoriasis Patients• Up to 30% of individuals with psoriasis will
develop PsA (higher than previously thought)
• Risk factors– Severe psoriasis
– Psoriatic nail pitting
– Uveitis
Eder L, et al. Arthritis Rheumatol. 2016;68(4):915-923.Karreman MC, et al. Arthritis Rheumatol. 2016;68(4):924-931.Photos courtesy of Margaret Bobonich, DNP, FNP-C, DCNP, FAANP.Used with permission.
7
PsA• Inflammatory arthritis
– Skin disease typically precedes joint disease
• Variable disease course– Flares and remission
• Severe disease is associated with:– Progressive joint damage– Increased mortality– Increase in cardiovascular
risk
Eder L, et al. Arthritis Rheumatol. 2016;68(4):915-923.Gladman DD. Clin Exp Rheumatol. 2008;26(5 Suppl 51):S62-S65.Arumugam R, McHugh NJ. J Rheumatol Suppl. 2012;89:32-35.Photo courtesy of Margaret Bobonich, DNP, FNP-C, DCNP, FAANP. Used with permission.
80%
20%
Diagnosis of PsA• High prevalence of undiagnosed PsA (~10%-15%)• Patients with PsA report a mean interval of 12.4
years between onset of skin symptoms and onset of joint symptoms
• Arthritis symptoms precede skin involvement in 13% to 17% of patients
• 15% of patients have undiagnosed or unrecognized psoriasis
1. Villani A, et al. J Am Acad Dermatol. 2015;73(2):242-248.2. Karreman MC, et al. Arthritis Rheumatol. 2016;68(4):924-931.3. Gottlieb A, et al. J Am Acad Dermatol. 2008;58(5):851-864.
Joint symptoms represent DESTRUCTIVE, IRREVERSIBLE DISEASE.
Early diagnosis is critical for preventing progression.
Diagnosis of PsA
• Common signs and symptoms‒ Musculoskeletal (32.1%) Joint symptoms (88.2%)
Tendon symptoms (50.4%)Dactylitis
Low back pain (73.9%)
Peripheral arthritis
‒ Psoriatic nail dystrophy (15.5%)
‒ Enthesitis (4.6%-7.0%)
‒ Uveitis
‒ Plaque psoriasisKarreman MC, et al. Arthritis Rheumatol. 2016;68(4):924-931.
8
Diagnosis of PsA• 2 primary patterns
‒ Peripheral joint disease (~95% of PsApatients)
‒ Axial involvement only (~5% of PsApatients)
• Diagnosis is typically made in a patient with psoriasis and inflammatory arthritis in a PsA-type pattern– Patients with psoriasis may have other
types of arthritis including RA, OA, gout, reactive arthritis, and arthritis of IBD
Gottlieb A, et al. J Am Acad Dermatol. 2008;58(5):851-864.
Diagnosis Is Made Clinically• History
– Skin disease– Joints involved– Enthesitis, dactylitis, eye
disease, inflammatory back pain (age <40, worse at night with AM stiffness, better with activity)
– Family history• Physical exam• Laboratory testing
– CBC– BUN, creatinine, uric acid, and
UA– ESR and CRP (elevated in 40%
of patients)– RF (2%-10%), anti-CCP (8%-
16%) and ANA (low titer 50%)– HLAB27 (50%)
• Arthrocentesis– To rule out septic arthritis, gout
and CPPD• Imaging
– Plain film, ultrasound, MRI– Co-existence of erosive
changes and new bone formation, which may occur in same joint or within same digit
Menter A, et al. J Am Acad Dermatol. 2011;65(1):137-174; Alenius GM, et al. Ann Rheum Dis. 2006;65(3):398-400; Johnson SR, et al. Ann Rheum Dis. 2005;64(5):770-772; Eder L, et al. Ann Rheum Dis. 2012;71(1):50-55.
Diagnosis can be challenging:
REFER
ClASsification Criteria for Psoriatic ARthritis (CASPAR)
• Valuable in clinical trials, can be used for diagnosis– Limited to peripheral arthritis, axial disease, and
enthesitis
• Specificity of 98.7% and sensitivity of 91.4%
• Advantages over Moll and Wright Criteria*– High specificity and sensitivity– Includes family history of psoriasis– Includes inflammatory articular disease– Includes RF status
*To meet the Moll and Wright 1973 classification criteria for psoriatic arthritis, a patient with psoriasis and inflammatory arthritis who is seronegative for RA must present with 1 of 5 clinical subtypes: polyarticular, symmetric arthritis; pligoarticular (less than 5 joints), asymmetric arthritis; distal interphalangeal joint predominant; spondylitis predominant; or arthritis mutilans.Taylor W, et al. Arthritis Rheum. 2006;54(8):2665-2673; Congi L, Roussou E. Clin Exp Rheumatol. 2010;28(3):304-310; Gottlieb A, et al. J Am Acad Dermatol. 2008;58(5):851-864.
9
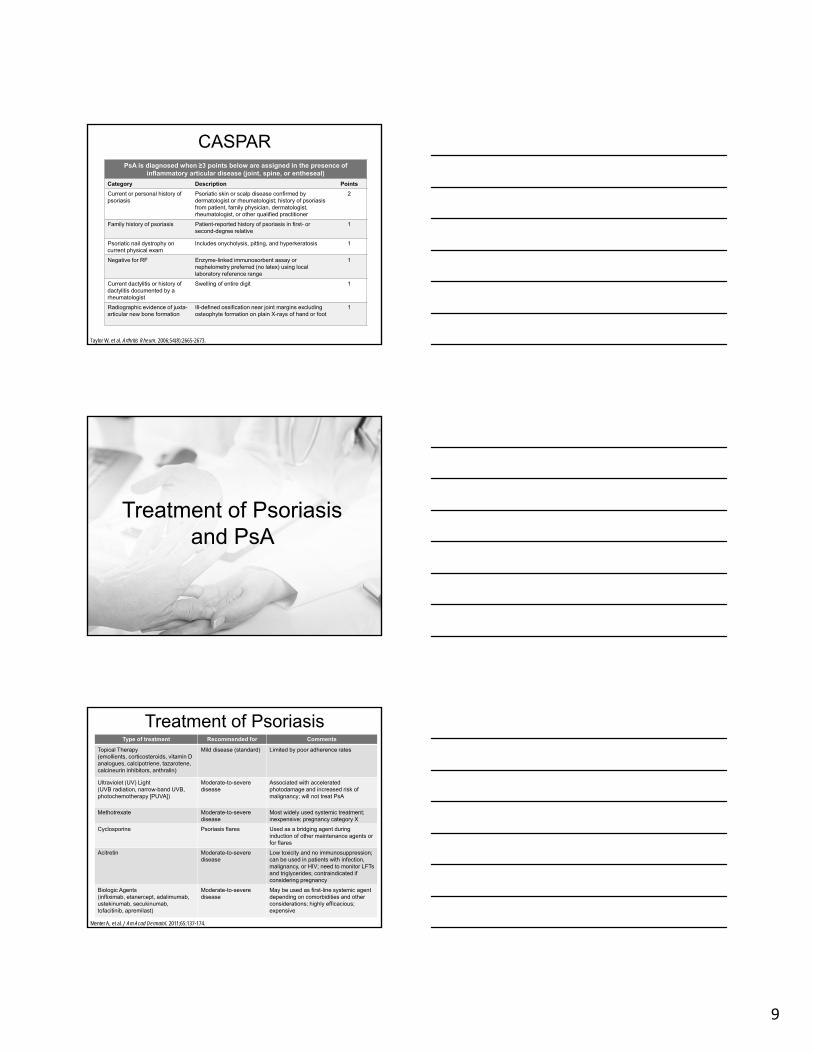
PsA is diagnosed when ≥3 points below are assigned in the presence of inflammatory articular disease (joint, spine, or entheseal)
Category Description Points
Current or personal history of psoriasis
Psoriatic skin or scalp disease confirmed by dermatologist or rheumatologist; history of psoriasis from patient, family physician, dermatologist, rheumatologist, or other qualified practitioner
2
Family history of psoriasis Patient-reported history of psoriasis in first- or second-degree relative
1
Psoriatic nail dystrophy on current physical exam
Includes onycholysis, pitting, and hyperkeratosis 1
Negative for RF Enzyme-linked immunosorbent assay or nephelometry preferred (no latex) using local laboratory reference range
1
Current dactylitis or history of dactylitis documented by a rheumatologist
Swelling of entire digit 1
Radiographic evidence of juxta-articular new bone formation
Ill-defined ossification near joint margins excluding osteophyte formation on plain X-rays of hand or foot
1
CASPAR
Taylor W, et al. Arthritis Rheum. 2006;54(8):2665-2673.
Treatment of Psoriasis and PsA
Treatment of PsoriasisType of treatment Recommended for Comments
Topical Therapy(emollients, corticosteroids, vitamin D analogues, calcipotriene, tazarotene, calcineurin inhibitors, anthralin)
Mild disease (standard) Limited by poor adherence rates
Ultraviolet (UV) Light(UVB radiation, narrow-band UVB, photochemotherapy [PUVA])
Moderate-to-severe disease
Associated with acceleratedphotodamage and increased risk of malignancy; will not treat PsA
Methotrexate Moderate-to-severedisease
Most widely used systemic treatment; inexpensive; pregnancy category X
Cyclosporine Psoriasis flares Used as a bridging agent during induction of other maintenance agents or for flares
Acitretin Moderate-to-severe disease
Low toxicity and no immunosuppression; can be used in patients with infection, malignancy, or HIV; need to monitor LFTs and triglycerides; contraindicated if considering pregnancy
Biologic Agents(infliximab, etanercept, adalimumab, ustekinumab, secukinumab, tofacitinib, apremilast)
Moderate-to-severedisease
May be used as first-line systemic agent depending on comorbidities and other considerations; highly efficacious; expensive
Menter A, et al. J Am Acad Dermatol. 2011;65:137-174.
10
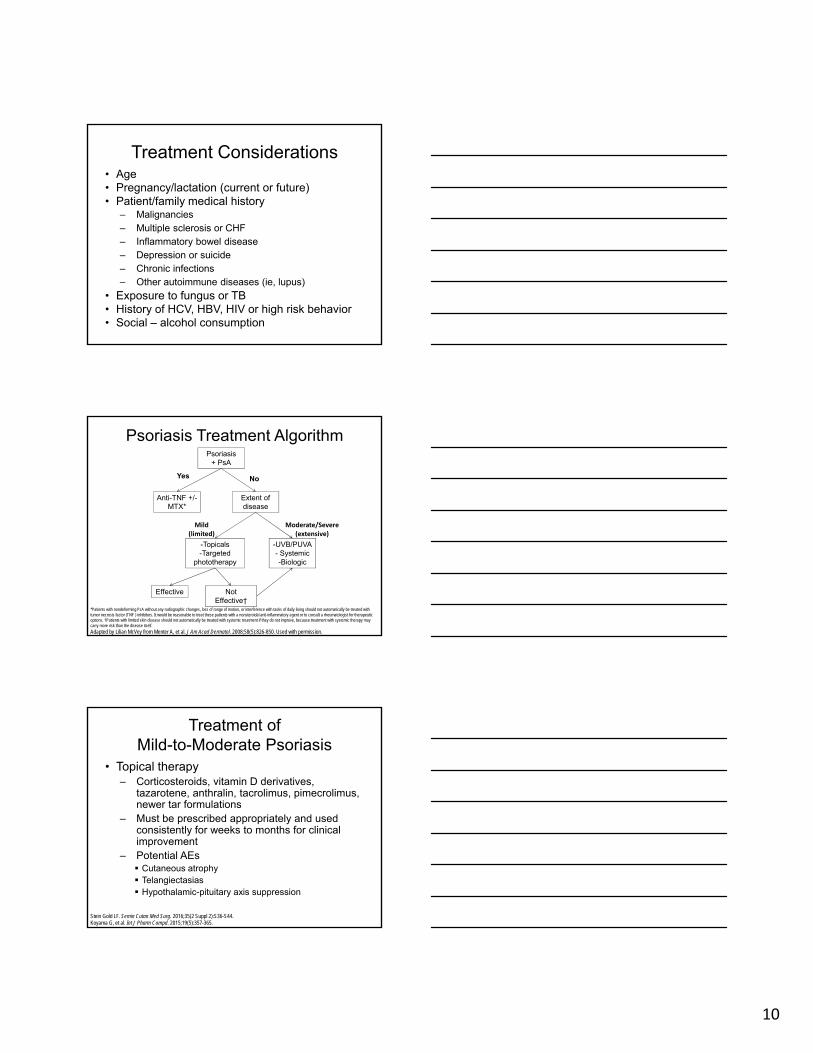
Treatment Considerations• Age• Pregnancy/lactation (current or future)• Patient/family medical history
– Malignancies– Multiple sclerosis or CHF– Inflammatory bowel disease– Depression or suicide– Chronic infections– Other autoimmune diseases (ie, lupus)
• Exposure to fungus or TB• History of HCV, HBV, HIV or high risk behavior• Social – alcohol consumption
Psoriasis Treatment AlgorithmPsoriasis
+ PsA
Anti-TNF +/-MTX*
Extent of disease
-Topicals-Targeted
phototherapy
-UVB/PUVA- Systemic-Biologic
Effective Not Effective†
Mild(limited)
No
Moderate/Severe(extensive)
Yes
*Patients with nondeforming PsA without any radiographic changes, loss of range of motion, or interference with tasks of daily living should not automatically be treated with tumor necrosis factor (TNF ) inhibitors. It would be reasonable to treat these patients with a nonsteroidal anti-inflammatory agent or to consult a rheumatologist for therapeutic options. †Patients with limited skin disease should not automatically be treated with systemic treatment if they do not improve, because treatment with systemic therapy may carry more risk than the disease itself.
Adapted by Lilian McVey from Menter A, et al. J Am Acad Dermatol. 2008;58(5):826-850. Used with permission.
Treatment of Mild-to-Moderate Psoriasis
• Topical therapy– Corticosteroids, vitamin D derivatives,
tazarotene, anthralin, tacrolimus, pimecrolimus, newer tar formulations
– Must be prescribed appropriately and used consistently for weeks to months for clinical improvement
– Potential AEs Cutaneous atrophy Telangiectasias Hypothalamic-pituitary axis suppression
Stein Gold LF. Semin Cutan Med Surg. 2016;35(2 Suppl 2):S36-S44.Koyama G, et al. Int J Pharm Compd. 2015;19(5):357-365.
11
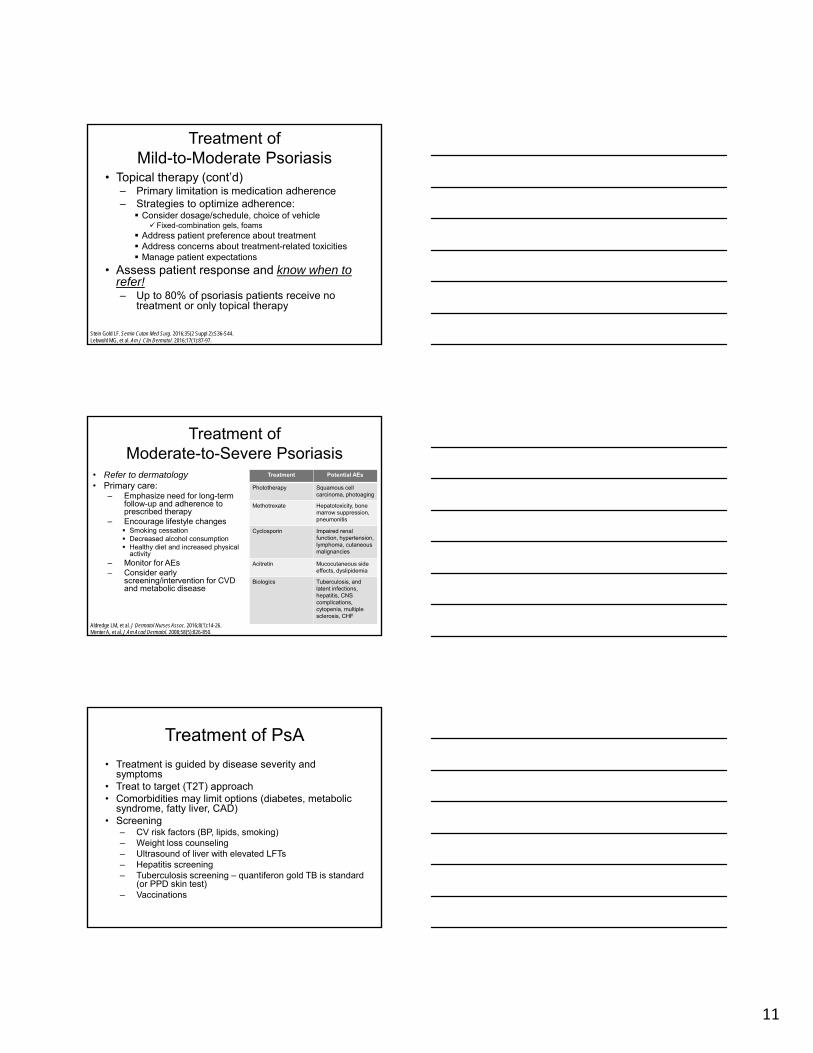
Treatment of Mild-to-Moderate Psoriasis
• Topical therapy (cont’d)– Primary limitation is medication adherence– Strategies to optimize adherence: Consider dosage/schedule, choice of vehicle
Fixed-combination gels, foams Address patient preference about treatment Address concerns about treatment-related toxicities Manage patient expectations
• Assess patient response and know when to refer!– Up to 80% of psoriasis patients receive no
treatment or only topical therapy
Stein Gold LF. Semin Cutan Med Surg. 2016;35(2 Suppl 2):S36-S44.Lebwohl MG, et al. Am J Clin Dermatol. 2016;17(1):87-97.
Treatment of Moderate-to-Severe Psoriasis
• Refer to dermatology• Primary care:
– Emphasize need for long-term follow-up and adherence to prescribed therapy
– Encourage lifestyle changes Smoking cessation Decreased alcohol consumption Healthy diet and increased physical
activity– Monitor for AEs– Consider early
screening/intervention for CVD and metabolic disease
Treatment Potential AEs
Phototherapy Squamous cell carcinoma, photoaging
Methotrexate Hepatotoxicity, bone marrow suppression, pneumonitis
Cyclosporin Impaired renal function, hypertension,lymphoma, cutaneousmalignancies
Acitretin Mucocutaneous side effects, dyslipidemia
Biologics Tuberculosis, and latent infections,hepatitis, CNS complications, cytopenia, multiple sclerosis, CHF
Aldredge LM, et al. J Dermatol Nurses Assoc. 2016;8(1):14-26.Menter A, et al. J Am Acad Dermatol. 2008;58(5):826-850.
Treatment of PsA
• Treatment is guided by disease severity and symptoms
• Treat to target (T2T) approach • Comorbidities may limit options (diabetes, metabolic
syndrome, fatty liver, CAD)• Screening
– CV risk factors (BP, lipids, smoking)– Weight loss counseling– Ultrasound of liver with elevated LFTs– Hepatitis screening – Tuberculosis screening – quantiferon gold TB is standard
(or PPD skin test)– Vaccinations
12
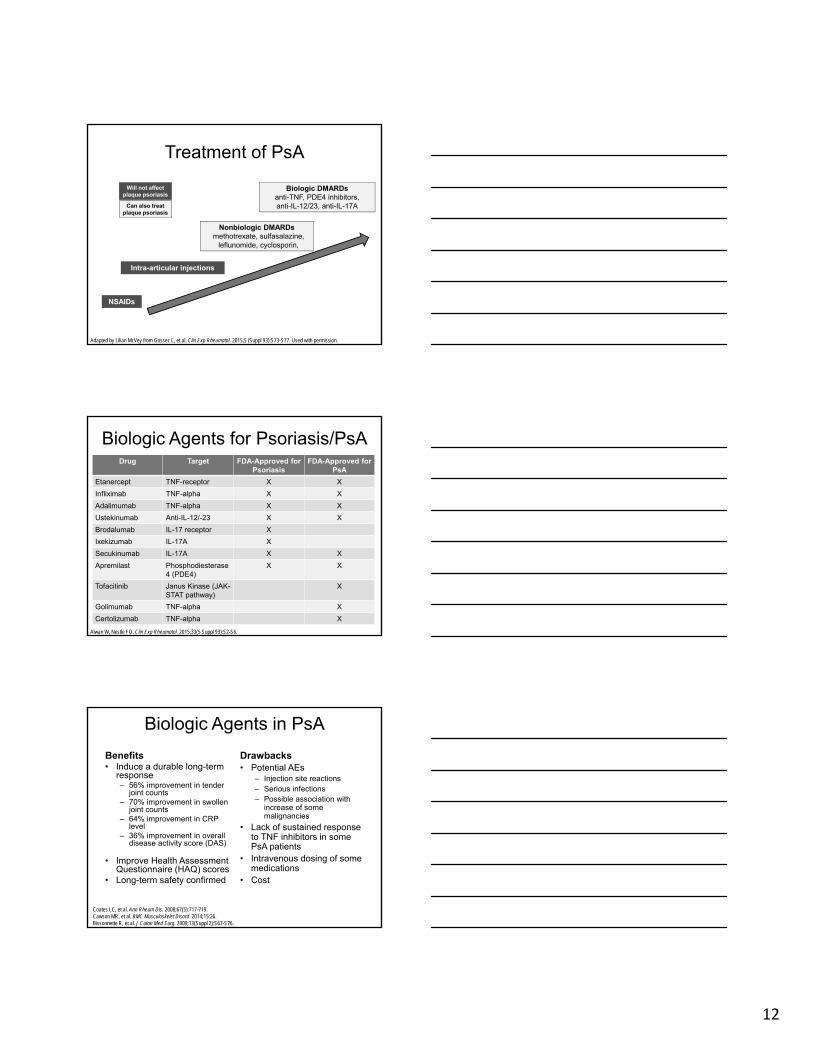
Treatment of PsA
NSAIDs
Intra-articular injections
Nonbiologic DMARDsmethotrexate, sulfasalazine,
leflunomide, cyclosporin,
Biologic DMARDsanti-TNF, PDE4 inhibitors, anti-IL-12/23, anti-IL-17A
Adapted by Lilian McVey from Gossec L, et al. Clin Exp Rheumatol. 2015;5 (Suppl 93):S73-S77. Used with permission.
Will not affect plaque psoriasis
Can also treat plaque psoriasis
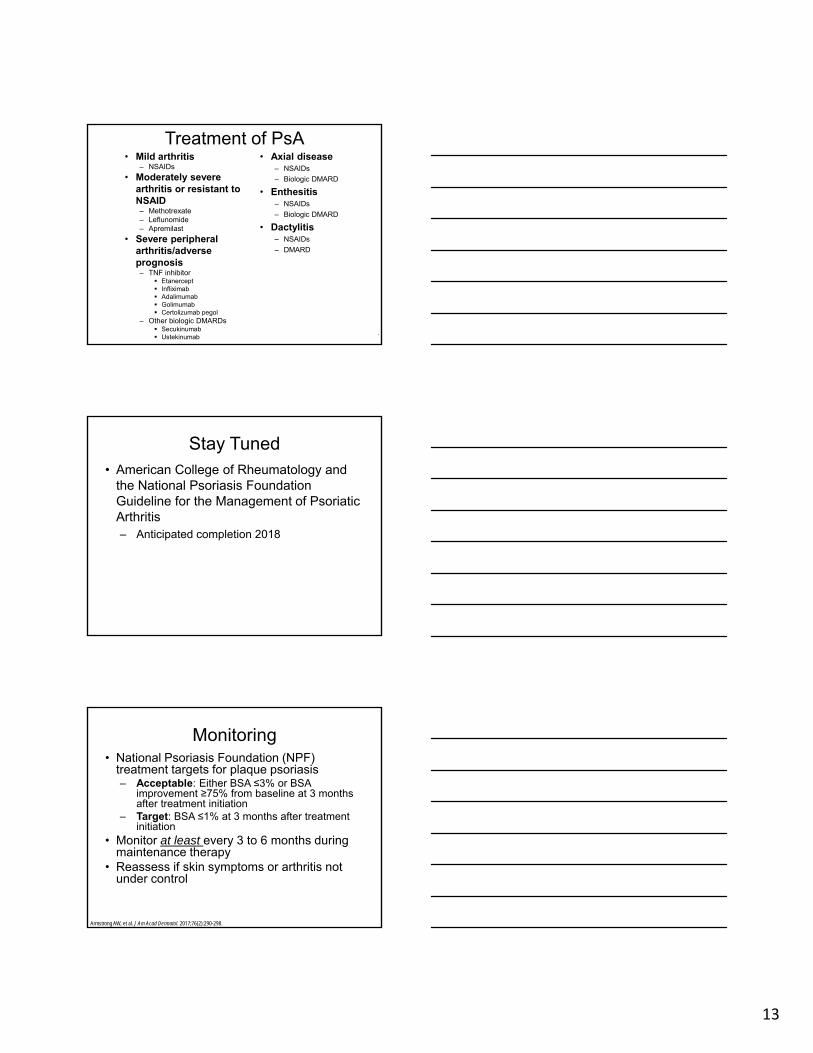
Biologic Agents for Psoriasis/PsADrug Target FDA-Approved for
PsoriasisFDA-Approved for
PsA
Etanercept TNF-receptor X X
Infliximab TNF-alpha X X
Adalimumab TNF-alpha X X
Ustekinumab Anti-IL-12/-23 X X
Brodalumab IL-17 receptor X
Ixekizumab IL-17A X
Secukinumab IL-17A X X
Apremilast Phosphodiesterase 4 (PDE4)
X X
Tofacitinib Janus Kinase (JAK-STAT pathway)
X
Golimumab TNF-alpha X
Certolizumab TNF-alpha X
Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33(5 Suppl 93):S2-S6.
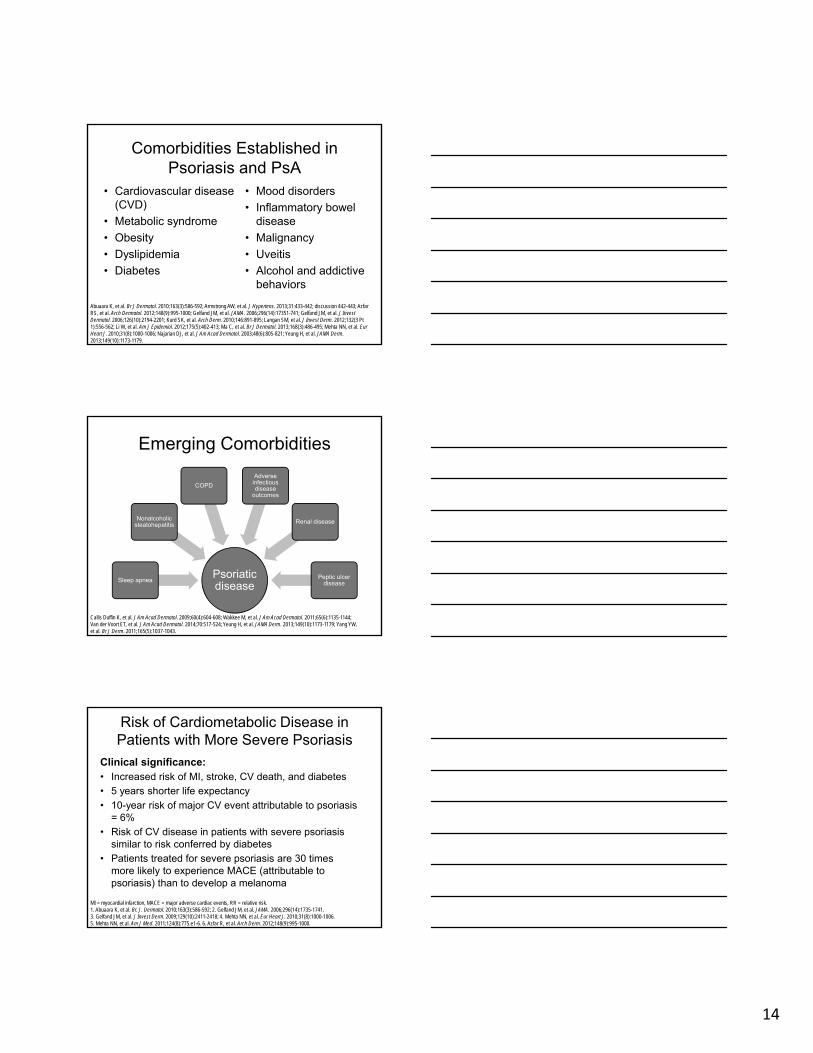
Biologic Agents in PsA
Benefits• Induce a durable long-term
response– 56% improvement in tender
joint counts– 70% improvement in swollen
joint counts– 64% improvement in CRP
level– 36% improvement in overall
disease activity score (DAS)
• Improve Health Assessment Questionnaire (HAQ) scores
• Long-term safety confirmed
Drawbacks• Potential AEs
– Injection site reactions– Serious infections– Possible association with
increase of some malignancies
• Lack of sustained response to TNF inhibitors in some PsA patients
• Intravenous dosing of some medications
• Cost
Coates LC, et al. Ann Rheum Dis. 2008;67(5):717-719.Cawson MR, et al. BMC Musculoskelet Disord. 2014;15:26.Bissonnette R, et al. J Cutan Med Surg. 2009;13(Suppl 2):S67-S76.
13
Treatment of PsA• Mild arthritis
– NSAIDs
• Moderately severe arthritis or resistant to NSAID– Methotrexate– Leflunomide– Apremilast
• Severe peripheral arthritis/adverse prognosis– TNF inhibitor
Etanercept Infliximab Adalimumab Golimumab Certolizumab pegol
– Other biologic DMARDs Secukinumab Ustekinumab
• Axial disease– NSAIDs
– Biologic DMARD
• Enthesitis– NSAIDs
– Biologic DMARD
• Dactylitis– NSAIDs
– DMARD
.
Stay Tuned• American College of Rheumatology and
the National Psoriasis Foundation Guideline for the Management of Psoriatic Arthritis– Anticipated completion 2018
Monitoring• National Psoriasis Foundation (NPF)
treatment targets for plaque psoriasis– Acceptable: Either BSA ≤3% or BSA
improvement ≥75% from baseline at 3 months after treatment initiation
– Target: BSA ≤1% at 3 months after treatment initiation
• Monitor at least every 3 to 6 months during maintenance therapy
• Reassess if skin symptoms or arthritis not under control
Armstrong AW, et al. J Am Acad Dermatol. 2017;76(2):290-298.
14
Comorbidities Established in Psoriasis and PsA
• Cardiovascular disease (CVD)
• Metabolic syndrome
• Obesity
• Dyslipidemia
• Diabetes
• Mood disorders
• Inflammatory bowel disease
• Malignancy
• Uveitis
• Alcohol and addictive behaviors
Abuaara K, et al. Br J Dermatol. 2010;163(3):586-592; Armstrong AW, et al. J Hypertens. 2013;31:433-442; discussion 442-443; AzfarRS, et al. Arch Dermatol. 2012;148(9):995-1000; Gelfand JM, et al. JAMA. 2006;296(14):17351-741; Gelfand JM, et al. J Invest Dermatol. 2006;126(10):2194-2201; Kurd SK, et al. Arch Derm. 2010;146:891-895; Langan SM, et al. J Invest Derm. 2012;132(3 Pt 1):556-562; Li W, et al. Am J Epidemiol. 2012;175(5):402-413; Ma C, et al. Br J Dermatol. 2013;168(3):486-495; Mehta NN, et al. EurHeart J. 2010;31(8):1000-1006; Najarian DJ, et al. J Am Acad Dermatol. 2003;48(6):805-821; Yeung H, et al. JAMA Derm. 2013;149(10):1173-1179.
Emerging Comorbidities
Psoriatic disease
Sleep apnea
Nonalcoholic steatohepatitis
COPD
Adverse infectious disease
outcomes
Renal disease
Peptic ulcer disease
Callis Duffin K, et al. J Am Acad Dermatol. 2009;60(4):604-608; Wakkee M, et al. J Am Acad Dermatol. 2011;65(6):1135-1144; Van der Voort ET, et al. J Am Acad Dermatol. 2014;70:517-524; Yeung H, et al. JAMA Derm. 2013;149(10):1173-1179; Yang YW, et al. Br J Derm. 2011;165(5):1037-1043.
Risk of Cardiometabolic Disease in Patients with More Severe Psoriasis
Clinical significance:• Increased risk of MI, stroke, CV death, and diabetes
• 5 years shorter life expectancy
• 10-year risk of major CV event attributable to psoriasis = 6%
• Risk of CV disease in patients with severe psoriasis similar to risk conferred by diabetes
• Patients treated for severe psoriasis are 30 times more likely to experience MACE (attributable to psoriasis) than to develop a melanoma
MI = myocardial infarction, MACE = major adverse cardiac events, RR = relative risk.1. Abuaara K, et al. Br. J. Dermatol. 2010;163(3):586-592; 2. Gelfand JM, et al. JAMA. 2006;296(14):1735-1741. 3. Gelfand JM, et al. J Invest Derm. 2009;129(10):2411-2418; 4. Mehta NN, et al. Eur Heart J. 2010;31(8):1000-1006. 5. Mehta NN, et al. Am J Med. 2011;124(8):775.e1-6. 6. Azfar R, et al. Arch Derm. 2012;148(9):995-1000.
15
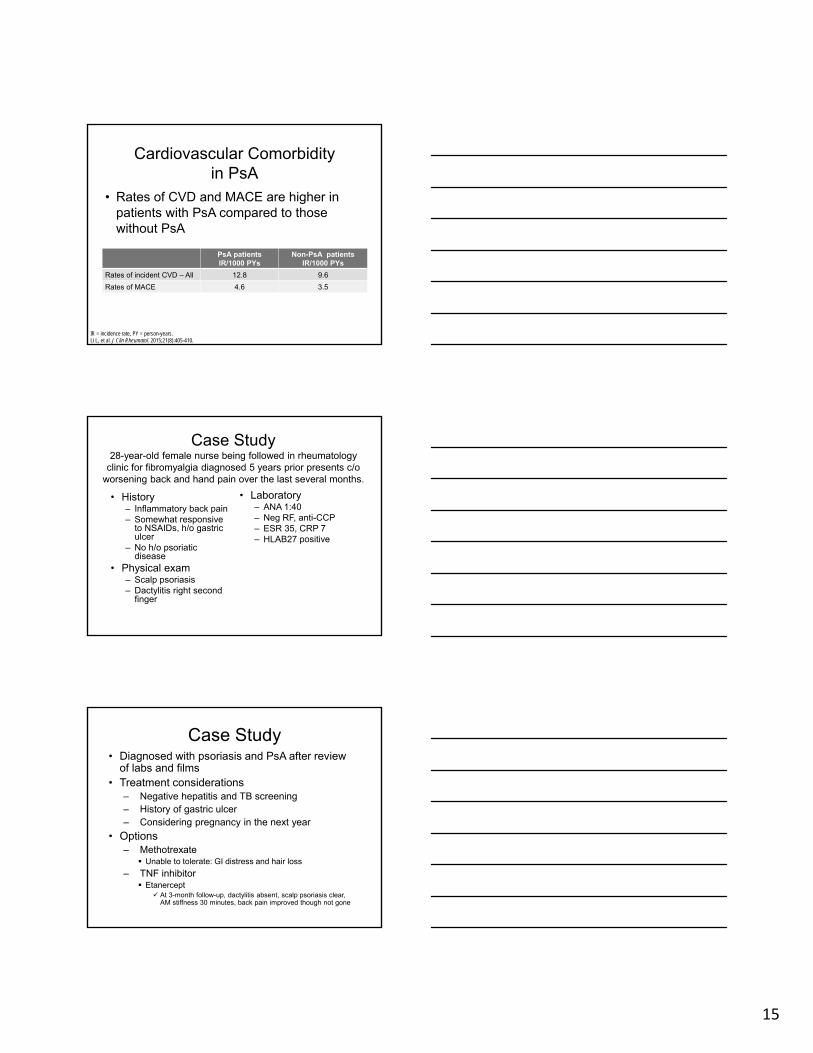
Cardiovascular Comorbidity in PsA
PsA patientsIR/1000 PYs
Non-PsA patients IR/1000 PYs
Rates of incident CVD – All 12.8 9.6
Rates of MACE 4.6 3.5
• Rates of CVD and MACE are higher in patients with PsA compared to those without PsA
IR = incidence rate, PY = person-years.Li L, et al. J Clin Rheumatol. 2015;21(8):405-410.
Case Study28-year-old female nurse being followed in rheumatology
clinic for fibromyalgia diagnosed 5 years prior presents c/o worsening back and hand pain over the last several months.
• History– Inflammatory back pain– Somewhat responsive
to NSAIDs, h/o gastric ulcer
– No h/o psoriatic disease
• Physical exam– Scalp psoriasis– Dactylitis right second
finger
• Laboratory – ANA 1:40– Neg RF, anti-CCP– ESR 35, CRP 7– HLAB27 positive
Case Study• Diagnosed with psoriasis and PsA after review
of labs and films• Treatment considerations
– Negative hepatitis and TB screening– History of gastric ulcer– Considering pregnancy in the next year
• Options– Methotrexate
Unable to tolerate: GI distress and hair loss
– TNF inhibitor Etanercept
At 3-month follow-up, dactylitis absent, scalp psoriasis clear, AM stiffness 30 minutes, back pain improved though not gone
16
Case Study• Two years later, stopped etanercept with
pregnancy confirmation• Back pain worse during pregnancy• At 2 months postpartum
– Scalp psoriasis worse, patches on elbows and hands
– Joint pain and stiffness in hands and knees– Difficulty with ADLs– Resumed etanercept with reduction in
symptoms
Primary Care Pearls
• Take a good history from the patient• Complete a thorough skin
examination• Assess for joint signs and symptoms• Monitor patients for comorbidities
sooner than the general population• Monitor for side effects and treatment
complications
Primary Care Pearls• Assess for adherence to therapy• Ensure all age-appropriate screening• Assess for QoL and ADLs• Assess for psychosocial• Patients on biologics or
immunosuppressants– Do not give live vaccines– Notify specialist (dermatology or
rheumatology) if patient develops Serious signs or symptoms of infection Change in medical condition
Updates in Psoriasis and Psoriatic Arthritis Management: Best Practices for Effective Care
References
Abuaara K, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Cause-specific mortality in patients with severe psoriasis: a population-based cohort study in the U.K. Br J Dermatol. 2010;163(3):586-592.
Ainsworth C. Immunology: A many layered thing. Nature. 2012;492(7429):S52-S54.
Aldredge LM, Young MS. Providing guidance for patients with moderate-to-severe psoriasis who are candidates for biologic therapy: role of the nurse practitioner and physician assistant. J Dermatol Nurses Assoc. 2016;8(1):14-26.
Alenius GM, Berglin E, Rantapää Dehlqvist S. Antibodies against cyclic citrullinated peptide (CCP) in psoriatic patients with or without joint inflammation. Ann Rheum Dis. 2006;65(3):398-400.
Alwan W, Nestle FO. Pathogenesis and treatment of psoriasis: exploiting pathophysiological pathways for precision medicine. Clin Exp Rheumatol. 2015;33(5 Suppl 93):S2-S6.
Armstrong AW, Diegel MP, Bagel J, et al. From the Medical Board of the National Psoriasis Foundation: Treatment targets for plaque psoriasis. J Am Acad Dermatol. 2017;76(2):290-298.
Armstrong AW, Harskamp CT, Armstrong EJ. The association between psoriasis and hypertension: a systematic review and meta-analysis of observational studies. J Hypertens. 2013;31(3):433-442; discussion 442-443.
Armstrong AW, Schupp C, Wu J, Bebo B. Quality of life and work productivity impairment among psoriasis patients: findings from the National Psoriasis Foundation survey data 2003-2011. PLoS One. 2012;7(12):e52935.
Arumugam R, McHugh NJ. Mortality and causes of death in psoriatic arthritis. J Rheumatol Suppl. 2012;89:32-35.
Azfar RS, Seminara NM, Shin DB, Troxel AB, Margolis DJ, Gelfand JM. Increased risk of diabetes mellitus and likelihood of receiving diabetes mellitus treatment in patients with psoriasis. Arch Dermatol. 2012;148(9):995-1000.
Bissonnette R, Ho V, Langley RG. Safety of conventional systemic agents and biologic agents in the treatment of psoriasis. J Cutan Med Surg. 2009;13(Suppl 2):S67-S76.
Callis Duffin K, Wong B, Horn EJ, Krueger GG. Psoriatic arthritis is a strong predictor of sleep interference in patients with psoriasis. J Am Acad Dermatol. 2009;60(4):604-608.
Cawson MR, Mitchell SA, Knight C, et al. Systematic review, network meta-analysis and economic evaluation of biological therapy for the management of active psoriatic arthritis. BMC Musculoskelet Disord. 2014;15:26.
Coates LC, Cawkwell LS, Ng NW, et al. Sustained response to long-term biologics and switching in psoriatic arthritis: results from real life experience. Ann Rheum Dis. 2008;67(5):717-719.
Congi L, Roussou E. Clinical application of the CASPAR criteria for psoriatic arthritis compared to other existing criteria. Clin Exp Rheumatol. 2010;28(3):304-310.
Eder L, Chandran V, Pellet F, et al. Human leucocyte antigen risk alleles for psoriatic arthritis among patients with psoriasis. Ann Rheum Dis. 2012;71(1):50-55.
Eder L, Haddad A, Rosen CF, et al. The incidence and risk factors for psoriatic arthritis in patients with psoriasis: a prospective cohort study. Arthritis Rheumatol. 2016;68(4):915-923.
Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296(14):1735-1741.
Gelfand JM, Shin DB, Neimann AL, Wang X, Margolis DJ, Troxel AB. The risk of lymphoma in patients with psoriasis. J Invest Dermatol. 2006;126(10):2194-2201.
Gelfand, JM, Dommasch ED, Shin DB, et al. The risk of stroke in patients with psoriasis. J Invest Derm. 2009;129(10):2411-2418.
Gladman DD. Mortality in psoriatic arthritis. Clin Exp Rheumatol. 2008;26(5 Suppl 51):S62-S65.
Gossec L, Smolen JS. Treatment of psoriatic arthritis: management recommendations. Clin Exp Rheumatol. 2015;5 (Suppl 93):S73-S77.
Gottlieb A, Korman NJ, Gordon KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 2. Psoriatic arthritis: overview and guidelines of care for treatment with an emphasis on the biologics. J Am Acad Dermatol. 2008;58(5):851-864.
Helmick CG, Lee-Han H, Hirsch SC, Baird TS, Bartlett CL. Prevalence of psoriasis among adults in the U.S.: 2003-2006 and 2009-2010 National Health and Nutrition Examination Surveys. Am J Prev Med. 2014;47(1):37-45.
Icen M, Crowson CS, McEvoy MT, Dann FJ, Gabriel SE, Maradit Kremers H. Trends in incidence of adult-onset psoriasis over three decades: a population-based study. J Am Acad Dermatol. 2009;60(3):394-401.
Johnson SR, Schentag CT, Gladman DD. Autoantibodies in biological agent naive patients with psoriatic arthritis. Ann Rheum Dis. 2005;64(5):770-772.
Karreman MC, Weel AE, van der Ven M, et al. Prevalence of psoriatic arthritis in primary care patients with psoriasis. Arthritis Rheumatol. 2016;68(4):924-931.
Koyama G, Liu J, Scaffidi A, Khazraee M, Epstein B. Novel approaches to topical psoriasis therapy. Int J Pharm Compd. 2015;19(5):357-365.
Kurd SK, Troxel AB, Crits-Christoph P, Gelfand JM. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Derm. 2010;146(8):891-895.
Langan SM, Seminara NM, Shin DB, et al. Prevalence of metabolic syndrome in patients with psoriasis: a population-based study in the United Kingdom. J Invest Derm. 2012;132(3 Pt 1):556-562.
Lebwohl MG, Kavanaugh A, Armstrong AW, Van Voorhees AS. US perspectives in the management of psoriasis and psoriatic arthritis: patient and physician results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis (MAPP) survey. Am J Clin Dermatol. 2016;17(1):87-97.
Li L, Hagberg KW, Peng M, Shah K, Paris M, Jick S. Rates of cardiovascular disease and major adverse cardiovascular events in patients with psoriatic arthritis compared to patients without psoriatic arthritis. J Clin Rheumatol. 2015;21(8):405-410.
Li W, Han J, Choi HK, Qureshi AA. Smoking and risk of incident psoriasis among women and men in the United States: a combined analysis. Am J Epidemiol. 2012;175(5):402-413.
Ma C, Harskamp CT, Armstrong EJ, Armstrong AW. The association between psoriasis and dyslipidaemia: a systematic review. Br J Dermatol. 2013;168(3):486-495.
Mehta NN, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Patients with severe psoriasis are at increased risk of cardiovascular mortality: cohort study using the General Practice Research Database. Eur Heart J. 2010;31(8):1000-1006.
Mehta NN, Yu Y, Pinnelas R, et al. Attributable risk estimate of severe psoriasis on major cardiovascular events. Am J Med. 2011;124(8):775.e1-6.
Menter A, Gottlieb A, Feldman S, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. J Am Acad Dermatol. 2008;58(5):826-850.
Menter A, Korman NJ, Elmets CA. Guidelines of care for the management of psoriasis and psoriatic arthritis. J Am Acad Dermatol. 2011;65(1):137-174.
Najarian DJ, Gottlieb AB. Connections between psoriasis and Crohn’s disease. J Am Acad Dermatol. 2003;48(6):805-821.
Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;361(5):496-509.
Rachakonda TD, Schupp CS, Armstrong AW. Psoriasis prevalence among adults in the United States. J Am Acad Dermatol. 2014;70(3):512-516.
Stein Gold LF. Topical Therapies for Psoriasis: Improving Management Strategies and Patient Adherence. Semin Cutan Med Surg. 2016;35(2 Suppl 2):S36-S44.
Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum. 2006;54(8):2665-2673.
Tollefson MM, Crowson CS, McEvoy MT, Maradit Kremers H. Incidence of psoriasis in children: a population-based study. J Am Acad Dermatol. 2010;62(6):979-987.
Van der Voort ET, Koehler EM, Dowlatshahi EA, et al. Psoriasis is independently associated with nonalcoholic fatty liver disease in patients 55 years old or older: Results from a population-based study. J Am Acad Dermatol. 2014;70(30):517-524.
Villani A, Rouzaud M, Sevrain M, et al. Prevalence of undiagnosed psoriatic arthritis among psoriasis patients: Systematic review and meta-analysis. J Am Acad Dermatol. 2015;73(2):242-248.
Wakkee M, de Vries E, van den Haak P, Nijsten T. Increased risk of infectious disease requiring hospitalization among patients with psoriasis: a population-based cohort. J Am Acad Dermatol. 2011;65(6):1135-1144.
Yang YW, Keller JJ, Lin HC. Medical comorbidity associated with psoriasis in adults: a population-based study. Br J Derm. 2011;165(5):1037-1043.
Yeung H, Takeshita J, Mehta NN, et al. Psoriasis severity and the prevalence of major medical comorbidity: a population-based study. JAMA Derm. 2013;149(10):1173-1179. Young M, et al. Article in press.
Young M, Aldredge L, Parker P. Psoriasis for the primary care practitioner. J Am Assoc Nurse Pract. 2017;29(3):157-178.