Pseudoaneurysms after Cholecystectomy: Not as Rare as … · after perioperative bile duct...
3
Central Bringing Excellence in Open Access JSM General Surgery: Cases and Images Cite this article: Wirsching A, Muehlenberg K, Röhling M, Zorger N, Pech O (2016) Pseudoaneurysms after Cholecystectomy: Not as Rare as You Might think. JSM Gen Surg Cases Images 1(2): 1009. *Corresponding author Andreas Wirsching, Krankenhaus Barmherzige Brüder Regensburg, Prüfeninger Str. 86, 93049 Regensburg, Germany, Tel: 4994136994415; Email: andreas. Submitted: 09 September 2016 Accepted: 30 September 2016 Published: 01 October 2016 Copyright © 2016 Wirsching et al. OPEN ACCESS Keywords • Pseudoaneurysms • Hemobilia • Cholecystectomy • Embolization Review Article Pseudoaneurysms after Cholecystectomy: Not as Rare as You Might think Wirsching A¹*, Muehlenberg K¹, Röhling M¹, Zorger N², and Pech O¹ ¹Department of Gastroenterology and Interventional endoscopy, Krankenhaus Barmherzige Brüder Regensburg, Germany ²Department of Radiology, Neuroradiology and Nuclear Medicine, Krankenhaus Barmherzige Brüder Regensburg, Germany Abstract Background: A 63-year old patient presented in our department with a five day history of hematemesis and melena. The source of the bleeding proved to be a pseudoaneurysm of the cystic artery, secondary to laparoscopic cholecystectomy three years before. The pseudoaneurysm was successfully eliminated by coil embolization. Results: A systematic literature research on Pubmed revealed 120 cases (n=94 after laparoscopic cholecystectomy and n=26 after open cholecystectomy). Interventional therapy by means of embolization was successful in 84.7% of the cases where it was the first-line therapy. Surgical approach was the treatment of choice in 17.5% and with a success rate of 85.7%. Conclusion: Pseudoaneurysmatic bleedings as a complication after cholecystectomy are more often than previously thought. Latency time until manifestation of the first symptoms can be up to four years after the surgery. Embolization is the treatment of choice with success rates of approximately 85%. INTRODUCTION Bleedings from the biliary tract usually play a minor role in the differential diagnosis of upper gastrointestinal bleedings. Clinical symptoms are summed up by the Quincke triad: colicky abdominal pain, jaundice and gastrointestinal bleeding [1]. The causes for hemobilia vary from trauma, neoplastic transformations, vascular malformation and iatrogenic causes [2]. Postoperative bleedings from the biliary tract after a cholecystectomy have been reported for both laparoscopic and open surgery. Intraoperative vascular damage mostly involves the right hepatic artery or the cystic artery, which is where most of the pseudoaneurysms ultimately develop [3,4]. We describe a case of hemobilia caused by a pseudoaneurysm after laparoscopic cholecystectomy and perform a systematic literature research. MATERIALS AND METHODS We performed a systematic literature research on Pubmed using the terms “cystic artery aneurysm” and “ hepatic artery aneurysm + cholecystectomy” to visualize the number of existing cases and to discuss the therapeutic approaches. Abstracts were included. RESULTS Recently a 63-year old otherwise healthy man presented in our department with a five day history of hematemesis and melena. The initial hemoglobin level was 8.3 g/dl, the cholestatic liver enzyme levels were elevated: total Bilirubin 3.5 mg/dl (normal value 0.2-1.0 mg/dl), ɣ-glutamyl transferase 707 U/l (normal value 5-66 U/l), alkaline phosphatase 227 U/l (normal value 40-129 U/l). On repetitive gastroscopies, signs of duodenal bleeding were detected, however without finding the actual source. After another episode of hematemesis and bright red blood per rectum, a hemorrhage from the papilla of Vater was discovered during an emergency endoscopy (Figure 1). In the following ERCP, we placed a plastic biliary CLSO drainage to ensure the biliary flow past intraluminal blood clots (Figure 2). The origin of the bleeding was not clear at that moment. The next day, on removal of the drainage, a pulsatile papillary bleeding emerged. The patient was immediately brought to the radiological department for an emergency angiography. An aneurysm of the right hepatic artery was shown where the cystic artery had been located prior to laparoscopic cholecystectomy three years before (Figure 3). Three coils were set to deactivate the aneurysm. Post-interventional radiographic control showed a successful embolization (Figure 4). Active bleeding did not reoccur in this patient during his stay at our department. Our literature research detected 120 cases of pseudoaneurysms after cholecystectomy from 1964 until 2015. In 78.3% cholecystectomy was performed laparoscopically. Embolization was the method used in 72/120 cases (60%) with a success rate of 84.7%. In the cases where embolization was not successful, surgery was performed with a success rate of 81% (9/11). Surgical approach was the treatment of choice in 21/120 cases (17.5%) with a success rate of 85.7%. Three pseudoaneurysms showed spontaneous regression or were only diagnosed on autopsy. In two cases, the application of self-expanding metal stents
Transcript of Pseudoaneurysms after Cholecystectomy: Not as Rare as … · after perioperative bile duct...

CentralBringing Excellence in Open Access
JSM General Surgery: Cases and Images
Cite this article: Wirsching A, Muehlenberg K, Röhling M, Zorger N, Pech O (2016) Pseudoaneurysms after Cholecystectomy: Not as Rare as You Might think. JSM Gen Surg Cases Images 1(2): 1009.
*Corresponding authorAndreas Wirsching, Krankenhaus Barmherzige Brüder Regensburg, Prüfeninger Str. 86, 93049 Regensburg, Germany, Tel: 4994136994415; Email: andreas.
Submitted: 09 September 2016
Accepted: 30 September 2016
Published: 01 October 2016
Copyright© 2016 Wirsching et al.
OPEN ACCESS
Keywords•Pseudoaneurysms•Hemobilia•Cholecystectomy•Embolization
Review Article
Pseudoaneurysms after Cholecystectomy: Not as Rare as You Might thinkWirsching A¹*, Muehlenberg K¹, Röhling M¹, Zorger N², and Pech O¹¹Department of Gastroenterology and Interventional endoscopy, Krankenhaus Barmherzige Brüder Regensburg, Germany²Department of Radiology, Neuroradiology and Nuclear Medicine, Krankenhaus Barmherzige Brüder Regensburg, Germany
Abstract
Background: A 63-year old patient presented in our department with a five day history of hematemesis and melena. The source of the bleeding proved to be a pseudoaneurysm of the cystic artery, secondary to laparoscopic cholecystectomy three years before. The pseudoaneurysm was successfully eliminated by coil embolization.
Results: A systematic literature research on Pubmed revealed 120 cases (n=94 after laparoscopic cholecystectomy and n=26 after open cholecystectomy). Interventional therapy by means of embolization was successful in 84.7% of the cases where it was the first-line therapy. Surgical approach was the treatment of choice in 17.5% and with a success rate of 85.7%.
Conclusion: Pseudoaneurysmatic bleedings as a complication after cholecystectomy are more often than previously thought. Latency time until manifestation of the first symptoms can be up to four years after the surgery. Embolization is the treatment of choice with success rates of approximately 85%.
INTRODUCTIONBleedings from the biliary tract usually play a minor role in
the differential diagnosis of upper gastrointestinal bleedings. Clinical symptoms are summed up by the Quincke triad: colicky abdominal pain, jaundice and gastrointestinal bleeding [1]. The causes for hemobilia vary from trauma, neoplastic transformations, vascular malformation and iatrogenic causes [2]. Postoperative bleedings from the biliary tract after a cholecystectomy have been reported for both laparoscopic and open surgery. Intraoperative vascular damage mostly involves the right hepatic artery or the cystic artery, which is where most of the pseudoaneurysms ultimately develop [3,4]. We describe a case of hemobilia caused by a pseudoaneurysm after laparoscopic cholecystectomy and perform a systematic literature research.
MATERIALS AND METHODSWe performed a systematic literature research on Pubmed
using the terms “cystic artery aneurysm” and “hepatic artery aneurysm + cholecystectomy” to visualize the number of existing cases and to discuss the therapeutic approaches. Abstracts were included.
RESULTSRecently a 63-year old otherwise healthy man presented
in our department with a five day history of hematemesis and melena. The initial hemoglobin level was 8.3 g/dl, the cholestatic liver enzyme levels were elevated: total Bilirubin 3.5 mg/dl (normal value 0.2-1.0 mg/dl), ɣ-glutamyl transferase 707 U/l
(normal value 5-66 U/l), alkaline phosphatase 227 U/l (normal value 40-129 U/l). On repetitive gastroscopies, signs of duodenal bleeding were detected, however without finding the actual source. After another episode of hematemesis and bright red blood per rectum, a hemorrhage from the papilla of Vater was discovered during an emergency endoscopy (Figure 1). In the following ERCP, we placed a plastic biliary CLSO drainage to ensure the biliary flow past intraluminal blood clots (Figure 2). The origin of the bleeding was not clear at that moment. The next day, on removal of the drainage, a pulsatile papillary bleeding emerged. The patient was immediately brought to the radiological department for an emergency angiography. An aneurysm of the right hepatic artery was shown where the cystic artery had been located prior to laparoscopic cholecystectomy three years before (Figure 3). Three coils were set to deactivate the aneurysm. Post-interventional radiographic control showed a successful embolization (Figure 4). Active bleeding did not reoccur in this patient during his stay at our department.
Our literature research detected 120 cases of pseudoaneurysms after cholecystectomy from 1964 until 2015. In 78.3% cholecystectomy was performed laparoscopically. Embolization was the method used in 72/120 cases (60%) with a success rate of 84.7%. In the cases where embolization was not successful, surgery was performed with a success rate of 81% (9/11). Surgical approach was the treatment of choice in 21/120 cases (17.5%) with a success rate of 85.7%. Three pseudoaneurysms showed spontaneous regression or were only diagnosed on autopsy. In two cases, the application of self-expanding metal stents
CentralBringing Excellence in Open Access
Wirsching et al. (2016)Email: andreas
JSM Gen Surg Cases Images 1(2): 1009 (2016) 2/3
successfully eliminated the pseudoaneurysm. No information on the therapeutic approach was available for 22 cases. The great majority of the pseudoaneurysms became symptomatic in the first weeks or months after the surgery. The latency time until the first symptoms occur can be up to four years after the surgery.
DISCUSSIONIn the past decades, the development of pseudoaneurysms
after cholecystectomy has only been described in case reports or smaller case series. Our review with 120 cases illustrates that it might actually be more often than previously thought.
The precise pathogenesis, underlying the development of post-operative pseudoaneurysms, is unclear. Mechanical or thermal injuries probably are the main factors [5]. Furthermore, the cytotoxic character of bile acids might cause vascular damage after a bile leak [6]. There are several case reports with a symptomatic manifestation of the pseudoaneurysm only 1-2 weeks after a laparoscopic cholecystectomy for acute cholecystitis. In these cases, the inflammatory process presumably plays a major role as an additional etiological factor. The same theory might apply for the cases where cholecystectomy was performed due to chronic cholecystitis. In the early days of laparoscopic cholecystectomy, the migration of clips to ligate the cystic duct (“FILSHIE-clips”) into the common bile duct had caused a similar local inflammatory reaction [7].
The onset of the first symptoms such as abdomal pain, hematemesis or melena can occur as late as four years after the surgery [8] which underlines the importance of anamnestic features in the initial approach to patients with hemobilia. The formation of pseudoaneurysms has been noticed in other laparoscopic surgeries et al. [9], describe a pseudoaneurysm of the iliac artery after laparoscopic rectopexy [9,10]. Selective embolization of the pseudoaneurysm has been established as the treatment of choice. When a transcatheter embolization is not feasible, transhepatic embolization can be performed alternatively [11]. In the 120 cases mentioned in this review, embolization as the first line therapy has been successful in 84.7%. A few cases of endovascular stent grafting have been described in the last years [12,13]. Since many cases with symptomatic pseudoaneurysms are potentially life-threatening arterial bleedings, further studies need to be performed to evaluate the role of stent grafts in emergency situations. Good and quick cooperation between endoscopists and interventional radiologists needs to be assured.
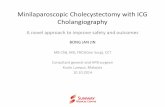
Figure 1 Emergency gastroscopy after hematemesis and bright red blood per rectum: Papillary sicker bleeding, only seen by side-viewing duodenoscope.
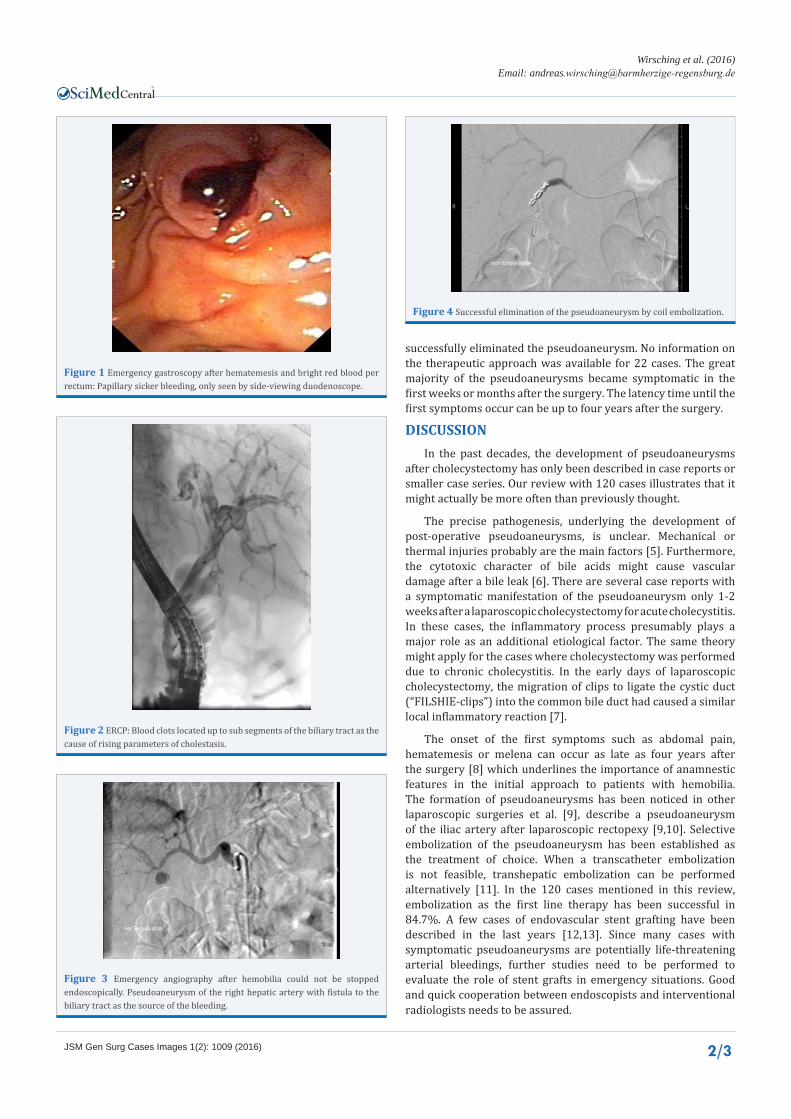
Figure 2 ERCP: Blood clots located up to sub segments of the biliary tract as the cause of rising parameters of cholestasis.
Figure 3 Emergency angiography after hemobilia could not be stopped endoscopically. Pseudoaneurysm of the right hepatic artery with fistula to the biliary tract as the source of the bleeding.
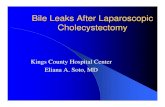
Figure 4 Successful elimination of the pseudoaneurysm by coil embolization.

CentralBringing Excellence in Open Access
Wirsching et al. (2016)Email: andreas
JSM Gen Surg Cases Images 1(2): 1009 (2016) 3/3
Overall however, other post-operative complications after cholecystectomy are more frequent. Bile duct injuries still account for the majority of post-operative complications [14]. Biliary leaks without significant bile duct injury are distinguished from major bile duct injury. Most bile leaks arise from the cystic duct stump [15,16]. Patients usually present with a continuous intraabdominal bile discharge from a percutaneous drain placed during the surgery or abdominal pain in the first postoperative days [17]. The therapy of choice is papillotomy with the optional placement of a transpapillary plastic stent to decrease the intraductal pressure and to facilitate the transpapillary out flow [17].When the bile ducts suffer from major injury, a surgical reconstruction in terms of hepaticojejunostomy is usually required [18], Management of bile duct leaks).
Bile duct strictures develop as a local fibrotic reaction after perioperative bile duct injuries. Female gender, open cholecystectomy and high output of an external biliary fistula were identified among the risk factors for the development of benign bile duct strictures [19]. The endoscopic treatment consists of the placement of multiple plastic stents. Covered self-expanding metal stents can be used alternatively (ESGE Guidelines, 2011). The complete occlusion of the bile duct is the worst complication and requires a reconstruction by an operative bilio-digestive anastomosis.
Combined vasculobiliary injuries after cholecystectomy most commonly affect the right hepatic artery (RHA) due to the anatomic proximity to the common hepatic duct. An estimated 25% of bile duct injuries are associated with RHA injuries. Early biliary reconstruction has been linked with a worse outcome in these cases due to subsequent fibrotic reorganization of the biliary lesion. Many authors recommend a reevaluation after three months with percutaneous transhepatic drainage in the meantime [20].
CONCLUSIONPseudoaneurysmatic bleedings as a complication after
cholecystectomy are more often than previously thought. Latency time until manifestation of the first symptoms can be up to four years after the surgery. Embolization is the treatment of choice with success rates of approximately 85%.
REFERENCES1. Merrell SW, Schneider PD. Hemobilia--evolution of current diagnosis
and treatment. West J Med. 1991; 155: 621-625.
2. Green MH, Duell RM, Johnson CD, Jamieson NV. Haemobilia. Br J Surg. 2001; 88: 773-786.
3. Madariaga JR, Dodson SF, Selby R, Todo S, Iwatsuki S, Starzl TE. Corrective treatment and anatomic considerations for laparoscopic cholecystectomy injuries. J Am Coll Surg. 1994; 179: 321-325.
4. Yelle JD, Fairfull-Smith R, Rasuli P, Lorimer JW. Hemobilia complicating
elective laparoscopic cholecystectomy: a case report. Can J Surg. 1996; 39: 240-242.
5. Madanur MA, Battula N, Sethi H, Deshpande R, Heaton N, Rela M. Pseudoaneurysm following laparoscopic cholecystectomy. Hepatobiliary Pancreat Dis Int. 2007; 6: 294-298
6. Hofmann AF. Bile Acids: The Good, the Bad, and the Ugly. News Physiol Sci. 1999; 14: 24-29.
7. Muehlenberg K, Löffler A. Clip migration in the common bile duct and consecutive calculus formation after laparoscopic cholecystectomy. Z Gastroenterol. 1995; 33: 108-111.
8. GarcíaMarín A, Martín Gil J, Serralta de Colsa D, Pérez Díaz MD, Turégano Fuentes F. Hepatic artery pseudoaneurysm following open cholecystectomy. Rev Esp Enferm Dig. 2010; 102: 65-66.
9. Kakar AK, Saxena R, Gupta V. Iliac artery pseudoaneurysm as a complication of laparoscopic rectopexy. Surg Laparosc Endosc Percutan Tech. 2003; 13: 48-50.
10. Kondo T, Takagi T, Morita S, Omae K, Hashimoto Y, Kobayashi H, et al. Early unclamping might reduce the risk of renal artery pseudoaneurysm after robot-assisted laparoscopic partial nephrectomy. Int J Urol. 2015; 22.
11. Chigot V, Lallier M, Alvarez F, Dubois J. Hepatic artery pseudoaneurysm following laparoscopic cholecystectomy. Pediatr Radiol. 2003; 33: 24-26.
12. Hylton JR, Pevec WC. Successful treatment of an iatrogenic right hepatic artery pseudoaneurysm and stenosis with a stent graft. J Vasc Surg. 2010; 51: 1510-1513.
13. Diéguez-Rascón FJ, Moreno-Machuca FJ, García-León A, Núñez-de-Arenas-Baeza G, Haurie-Girelli J, González-Herraez JV. Successfully endovascular resolution of iatrogenic right hepatic artery pseudoaneurysm. Rev Esp Enferm Dig. 2011; 103: 650-651.
14. Khan MH, Howard TJ, Fogel EL, Sherman S, McHenry L, Watkins JL, et al. Frequency of biliary complications after laparoscopic cholecystectomy detected by ERCP: experience at a large tertiary referral center. Gastrointest Endosc. 2007; 65: 247-252.
15. Agarwal N, Sharma BC, Garg S, Kumar R, Sarin SK. Endoscopic management of postoperative bile leaks. Hepatobiliary Pancreat Dis Int. 2006; 5: 273-277.
16. Kim KH, Kim TN. Endoscopic management of bile leakage after cholecystectomy: a single-center experience for 12 years. Clin Endosc. 2014; 47: 248-253.
17. Nawaz H, Papachristou GI. Endoscopic treatment for post-cholecystectomy bile leaks: update and recent advances. Ann Gastroenterol. 2011; 24: 161-163.
18. Pioche M, Ponchon T. Management of bile duct leaks. J Visc Surg. 2013; 150: 33-38.
19. Lokesh HM, Pottakkat B, Prakash A, Singh RK, Behari A, Kumar A, et al. Risk factors for development of biliary stricture in patients presenting with bile leak after cholecystectomy. Gut Liver. 2013; 7: 352-356.
20. Strasberg SM, Helton WS. An analytical review of vasculobiliary injury in laparoscopic and open cholecystectomy. HPB (Oxford). 2011; 13: 1-14.
Wirsching A, Muehlenberg K, Röhling M, Zorger N, Pech O (2016) Pseudoaneurysms after Cholecystectomy: Not as Rare as You Might think. JSM Gen Surg Cases Images 1(2): 1009.
Cite this article