Providing Treatment, Restoring Hope FAITH BASED COMMUNITY NETWORKS A STRATEGY TO COMBAT HIV/AIDS...
32
Providing Treatment, Restoring Hope FAITH BASED COMMUNITY NETWORKS A STRATEGY TO COMBAT HIV/AIDS PANDEMIC IN TANZANIA
-
Upload
liliana-hood -
Category
Documents
-
view
217 -
download
0
Transcript of Providing Treatment, Restoring Hope FAITH BASED COMMUNITY NETWORKS A STRATEGY TO COMBAT HIV/AIDS...

Providing Treatment, Restoring Hope
FAITH BASED COMMUNITY NETWORKS
A STRATEGY TO COMBAT HIV/AIDS PANDEMIC IN TANZANIA

Slide 2
BACKGROUND
HIV/AIDS is one of the top ten causes of morbidity and mortality in Tanzania
1st case in Tanzania reported in 1983
By December 1985, 20 regions of Tanzania mainland had reported AIDS cases
Currently a national problem affecting every corner of the country

Slide 3
AFRICA

Slide 4
TANZANIA
Estimated total population -39 million National HIV Prevalence: 6% (5.8% M and 6.2% F)
To date, there are 2.2m PLWHA, with estimated # of OVCs: 1.1M (THMIS , MoHSW 2006)
Tanzania’s target is to reach 400,000 patients who are in need of Antiretroviral therapy by 2009.
By end of December 2008, a total of 641,400 patients were enrolled in care & treatment and among them 120,000 were on ARVs

Slide 5
AIDS RELIEF
• AIDSRelief (AR): A PEPFAR funded ART program – Implemented by:• IMA World Health (IMA); Catholic Relief Services
(CRS); Futures Group International (FGI); University of Maryland School of Medicine, Institute of Human Virology (UMSOM-IHV)
• AR is responsible for 4 out of 21 regions in the country – to provide technical assistance and supervise all ART activities.

Slide 6
HIV PREVALENCE (% PER HIV PREVALENCE (% PER REGION)REGION)
* THMIS II 2007
1
2
34
1. MWANZA
2. MARA
3. MANYARA
4.TANGA
5.6 %, Pop.2.8m
7.7 %, Pop. 1.3m
1.2 %, Pop. 1.0m
4.8 %, Pop. 1.6m
REGIONHIV PREV.

Slide 7
ART SERVICES
Current model for ART Services in Tanzania
• Care and Treatment of HIV/AIDS • Prevention of Maternal to Child
Transmission of HIV • TB/HIV• Home Based Care (HBC) • Voluntary Counseling and Testing (VCT)

Slide 8
CHALLENGES FACING ART PROGRAM
1. Inadequate Human resources
a crisis - worsened by HIV/AIDS :
Overburdened Care and Treatment Clinics’ staff and general inadequate resources make outreach services difficult and limited.

Slide 9
CHALLENGES FACING ART PROGRAM
2. Weak or absent linkages between Care and Treatment Clinics and Communities leading to:
• Lack of adherence support to patients on ARVs
• Lack of psychosocial support• Increased number of patients lost to follow
up ( with bad consequences on the ART Program outcomes)

Slide 10
CHALLENGES FACING ART PROGRAM
3. Stigma – contributing to poor enrollment 0.and compliance to ART services
4. Poverty- worsened by the chronic nature of
the disease
5. Increased number of Orphans

Slide 11
CHALLENGES FACING ART PROGRAM……..
How do we handle these challenges?
The fight against HIV/AIDS can only be sustainable if owned by the people in the communities we serve.
Therefore, Community involvement through FBOs, NGOs / CBOs initiatives is imperative!

Slide 12
CHALLENGES FACING ART PROGRAM……..
In considering some of the solutions;
AIDS Relief recognized the importance of developing partnerships with existing FBOs in target regions as a key strategy for increasing access to health services and focusing on sustainability.
In addressing the problem of inadequate linkages between CTCs and the community, IMA through AIDS Relief came up with a simple, sustainable model, which is easy to implement at very low cost.

Slide 13
FBO MODEL
GOVERNMENTHEALTH FACILITY
COMMUNITY
CHURCH

Slide 14
KANISA LA MENONNITE SHIRATI
MODEL
HUB
HEALTH FACILITIES CARE &TREATMENT
CLINICS
SUB- HUBS SUB- HUBSSUB- HUB
V VOLUNTEERS VOLUNTEERS
PLWHAs
15 TO 20 PEOPLE
PLWHAs GROUPS
15 TO 20 PEOPLE
PLWHAs GROUPS
15 TO 20 PEOPLE
CHURCH
AT COMMUNITY
V V
PLWHAs
15 TO 20 PEOPLE
LOCAL GOVERNMENT
NGOs /CBOs

Slide 15
T
THE FBO COMMUNITY NETWORK
Objectives
1. To facilitate easy tracking of patients and reduce loss to follow-up at the treatment centers
2. To create patients treatment clubs for supporting each other to enhance adherence to ART, offer psychosocial support and reduce stigma.
3. To enhance two-way referral systems
4. Community mobilization for service utilization
5. Through organized and coordinated PLWHA groups, to facilitate easy access to other services (IGAs, prevention messages, spiritual support, Psychological support etc)

Slide 16
WHY FBOs
• Have networks that have access to hard to reach populations
• Have the ability to influence the attitudes and behaviors of their community members by building on relationships of trust and respect
• Have existing structures that can coordinate a scalable response
• Are committed to the cause of care and support for those in need from a spiritual perspective

Slide 17
WHY FBOs……
• Are uniquely positioned to promote HIV/AIDS stigma reduction, follow up patients on treatment and send out prevention messages
• The FBO structures at the lower levels (e.g. church level) are usually the first and at the frontline to respond to the patient’s need for support in terms of spiritual and material needs
These attributes make the partnership with them a valuable asset in the fight against HIV/AIDS

Slide 18
SUCCESS/ACCOMPLISHMENTS
• Number of community groups formed 130:
KMT Mara Region – 90 groups
ACT Tanga Region - 40 groups
• A total of 1700 patients have joined the groups.
• In Shirati, >50% of patients enrolled at Care and Treatment Clinics have joined the groups

Slide 19
SUCCESS/ACCOMPLISHMENTS
Reduced lost to follow-up at CTCs.(Out of 176 patients lost to follow -up at Shirati CTC in 2008, 156 patients {89%} were traced back through the program)
Enhanced adherence support among group members – giving wonderful results.
Community groups have created forums for PLWHAs to voice their needs and suggest solutions.

Slide 20
SUCCESS/ACCOMPLISHMENTS
4. Community Groups contribute to HIV prevention by;• encouraging disclosure • Enhancing voluntary testing among community
members• Providing group therapy with members, sharing
their fears and hopes, and encouraging each other • “peer support” for each other
5. Stigma reduction As more people check their sero-status and join the Community groups, stigma and discrimination level slowly declines

Slide 21
SUCCESS/ACCOMPLISHMENTS
6. Local Governments’ buy in; A sign of sustainability Using groups for distribution of support e.g food. Including groups in their annual plans and budgets.
7. Community groups create a sense of responsibility among PLWHAs. They identify the most needy among them to be given priority for the available limited resources.
8. Improved family income; Groups are motivated to start self support activities – IGAIGA

Slide 22
SUCCESS/ACCOMPLISHMENTS
9. Health monitoring
- share body weight results and encourage each other on good nutrition
- remind each other on CD4 check dates/follow-ups visits to clinics
10. FBOs/ CBOs/NGOs are mobilized to network for effective support of PLWHAs, sharing of information, best practices & challenges.

Slide 23
THE IMPACT
1. GRACE’S STORY
GRACE, a widow, with two children was abandoned by her husbands relatives, who took the very few belongings that she had and chased her away from her family home.
Grace was HIV positive and was started on ARVs
A SHELTER FOR GRACE AND HER 2 CHIDREN- DONATED BY A GOOD SAMARITAN

Slide 24
THE IMPACT
This was all what Grace had in her bed-room

Slide 25
IMPACT
Grace decided to stop her ARVs because she had not enough food and had no strength to work .
Jaclyn, Graces’ daughter dropped from school and started working for food to support her mother and her young sister.

Slide 26
IMPACT
GRACE GOT SHELTER AND FOOD SUPPORT, RESUMED HER ARVs
JACLINE WAS RE-ENROLLED IN SCHOOL PROVIDED WITH SCHOOL UNIFORMS AND OTHER NEEDS.
Through the FBO Community network
program…….

Slide 27
THE IMPACT
2. IMMACULATE,S STORY
SERIOUSLY SICK WITH OPPORTUNISTIC INFECTIONS (2007).
“I was waiting for the day of death” she said.

Slide 28
“Thanks to the work of AIDS Relief through the Anglican Church, Tanga” she said
“With the support of PLWHA groups, I have overcome my fears and have attained 100% adherence to my ARVs regimen”.
IMMACULATE ON ARVs
(2008)
THE IMPACT
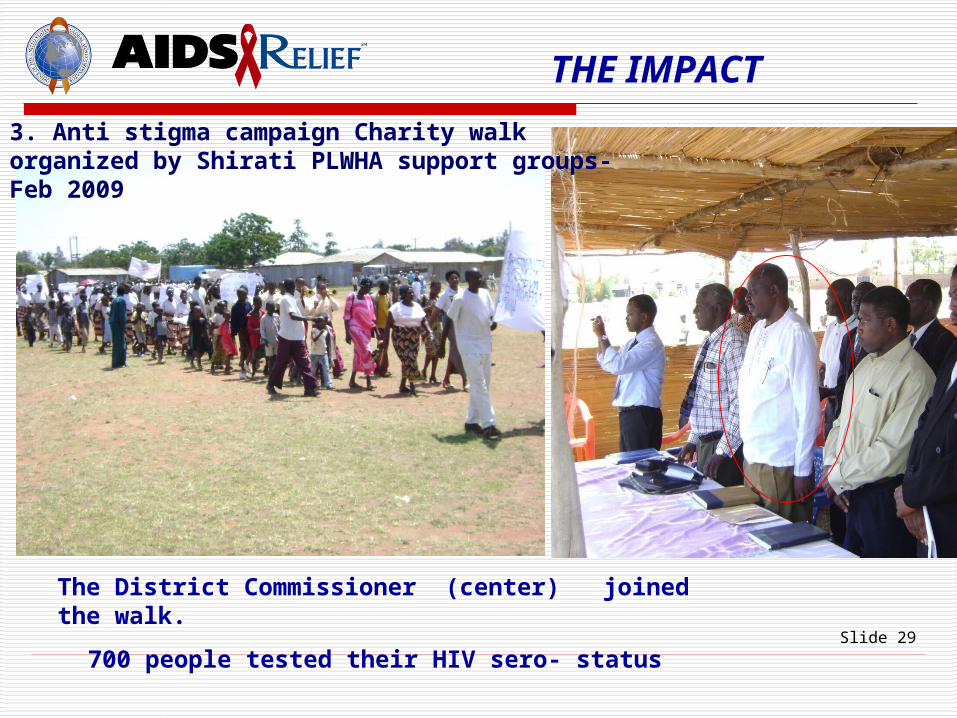
Slide 29
The District Commissioner (center) joined the walk.
700 people tested their HIV sero- status
THE IMPACT
3. Anti stigma campaign Charity walk organized by Shirati PLWHA support groups- Feb 2009

Slide 30
FBO (PLWHA) SUPPORT GROUPS CHALLENGES
• Maintaining functional and sustainable support groups
• Food shortage – interfering with adherence
• Stigma in the community is still an issue that groups have to deal with
• POVERTY- Lack of substantial capital to start IGAs
• Documentation - not always adequate and need continuous capacity building

Slide 31
RECOMMENDATIONS
1. Enhance collaboration between FBOs and government to integrate FBOs as main partners in ART community work
2. Leverage additional resources (sustainable) for full engagement of FBOs so that ART work in the community is accelerated.
3. Systematically document and disseminate lessons learned & best practices of FBO initiatives
4. Encourage inter-religious, inter-Organizational collaboration and networking

Slide 32
PARTNERSHIP IS POWER