
PROVIDER HANDBOOK - Humana
68
PROVIDER HANDBOOK
Transcript of PROVIDER HANDBOOK - Humana
PROVIDER HANDBOOK
ii
Welcome to American Eldercare, Inc.
Thank you for joining our provider network. We look forward to working with
you to provide quality, accessible services to our members.
American Eldercare, Inc. is committed to distributing comprehensive and timely
information to providers through this Provider Handbook. This handbook will
assist you with information on:
♦ Care Management services
♦ Claims submission
♦ Covered Services
♦ Authorization process
You will be notified of updates to this handbook via bulletins and notices posted
on our website at www.americaneldercare.com. If you need further explanation on
any topics discussed in this handbook, please contact your local Provider Relations
Specialist. A complete listing of our offices is located in Section 8, Appendix.
Sincerely,
Provider Relations Department
iii
TABLE OF CONTENTS
Section 1 Introduction………………………………...…………………………… Page 6
Long Term Care Managed Care Program …………………………………….. Page 7
Practice Guidelines..................................................................................................... Page 8
Mission Statement ………………………………………………………………….. Page 8
Office Hours …………………………………………………..............………….... Page 9
AEC Website ………………………………………………………………………. Page 9
Confidentiality Statement…………………………………………………………… Page 9
Section 2 Covered Services .. ………………………………………………………. Page 10
Medical Necessary/Necessity ……………………………………………….. Page 11
Emergency Service Responsibilities ………………………………………… Page 11
Adult Day Care ………………………………………………………………. Page 12
Assistive Care ……………………………………………………………….. Page 12
Assisted Living ……………………………………………………………… Page 12
Behavioral Management …………………………………………………… Page 14
Home Adaptations Accessibility …………………………………………. Page 14
Home Delivered Meals……………………………………………………. Page 15
Home Health Care ………………………………………………..………. Page 15
Hospice ………………………………………………………….………... Page 17
Medical Supplies (Consumable Medical)…………..………………………. Page 18
Medical Supplies (Durable Medical Equipment)………………………….. Page 18
Nursing Facility Services ……………………………………………………. Page 19
Nutritional Assessment/Risk Reduction……………………………………… Page 20
Personal Emergency Response Systems……………………………………. Page 20
Pharmacy Benefits …………………………………………………………… Page 21
Transportation……………………………….………………………………. Page 21
Quality Enhancements ……………………………………………………… Page 21
Section 3 Eligibility ……………………………………………………………….. Page 22
Conditions of Enrollment…………………………………………….…………. Page 22
Medicaid Pending ………………………………………………………………. Page 23
Membership Identification Card ……………………………………………….. Page 23
iv
Referrals to American Eldercare ………………………………………………... Page 24
Member Disenrollment……………………………………………………….. Page 24
Hospice …………………….……………………………………………………. Page 26
Section 4 Care Management ………………………………………………………. Page 27
Authorizations………………………………………………………………….. Page 27
Chronic/Complex Conditions …………………………………………………. Page 28
Abuse, Neglect, Exploitation……………………………………………………. Page 29
Critical Incident Reporting ……………………………………………………… Page 30
Member Rights and Responsibilities ………………………………………….. Page 30
Section 5 Provider Responsibilities………………………………………………… Page 33
Credentialing Committee ……………………………………………………….. Page 33
Initial Credentialing …………………………………………………………….. Page 33
Re-credentialing …………………………………………………………………. Page 34
Provider Monitoring ……………………………………………………………. Page 35
Right to Review and Correct Information ……………………………………… Page 35
Right to Appeal Adverse Credentialing Determination ………………………… Page 35
National Provider Identification ………………………………………………… Page 36
Provider Orientations and Education …………………………………………… Page 36
Notice Obligation ……………………………………………………………….. Page 36
Provider Handbook …………………………………………………………… Page 37
Provider Directory ……………………………………………………………… Page 37
Participating Agreement Standards…………………………………….......... Page 37
Accessibility & Availability …………………………………………………. Page 38
Provider Satisfaction …………………………………………………………. Page 38
Provider Medical/Case Record Review ……………………………………….. Page 38
Termination of Provider Contract ……………………………………………… Page 39
Out-of-Network/Non-Contracted Services ……………………………………… Page 39
Community Outreach/Marketing ………………………………………………. Page 40
Provider Responsibilities ………………………………………………………. Page 41
Provider Complaints …………………………………………………………. Page 41
Cultural Competency ……………………………………………………….. Page 43
Section 6 Claims/Billing ………….……………………………………………….. Page 44
v
Claims Submission …………………………………………………………… Page 44
Electronic Claims …………………………………………………………. Page 44
Paper Claims ……………………………………………………………. Page 45
Encounter Data ……………………………………………………………. Page 46
Assisted Living Facilities Providers ………………………………………….. Page 47
Skilled Nursing Facility Providers …………………………………………… Page 48
Home Health Providers……………………………………………………….. Page 49
Claims Acknowledgement………………………………………………………….. Page 49
Payments……………………………………………………………………… Page 50
Balance Billing ……………………………………………………………… Page 51
Claim Inquiry ……………………………………………………………….. Page 51
Claim Denial……………………………………………………………….. Page 51
Claims Reconsideration of Payment ………………………………………. Page 52
Formal Grievance/Appeals ………………………………………………………… Page 52
Formal Appeal ………………………………………………………………. Page 52
Expedited Appeals …………………………………………………………… Page 54
Beneficiary Assistance Program …………………………………….. Page 54
Unresolved Grievance/Appeals- Medicaid Fair Hearing …………………….. Page 55
Section 7 Forms ……………………………………………………………………… Page 57
Authorization Forms …………………………………………………………. FORMS
Claims Form ………………………………………………………………….. FORMS
Provider Complaint Form …………………………………….……………… FORMS
Provider Change of Notice Form ………………………………………….. FORMS
Section 8 Appendix …………………………………………………………………. Page 58
AEC Locations …………………………………………………………….. Appendix
CARES Offices ……………………………………………………………… Appendix
Denial Codes …………………………………………………………………. Appendix
Remittance Advice ………………………………………………………….. Appendix
6 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
_____________________________________________
1
INTRODUCTION ______________________________________________
American Eldercare Inc. (AEC) is a Provider Service Network (PSN) and home health
agency that provides services to our members in the most appropriate care setting. Our
Long-Term Care Managed Care Plan works directly with the State of Florida to provide our
members with quality community and/or facility care with a focus to coordinate the
member’s primary care through his/her primary insurance. American Eldercare, Inc. was
the only company to be chosen as a state-wide contractor of this program, allowing our
membership to freely move to any county they choose in the state.
Our first goal is to keep our members in their home and provide quality home health care
and community-based services to delay or avoid long-term placement in a nursing facility.
If our members needs a more supervised environment or wants more socialization we will
assist to subsidize and monitor them to receive services in an Assisted Living Facility or an
Adult Family Home. We understand that some of our members will require nursing home
care, and we ensure that they transition to this level of care when it is no longer safe to
remain in a community setting. We offer care to meet the individual needs of each of our
members.
The State of Florida’s goals for this program are:
• Coordinated long-term care across different health care settings.
• A choice of the best long-term care plan for their needs.
• Long-term care plans with the ability to offer more services.
• Access to cost-effective community-based long-term care services.
American Eldercare, Inc. has established guidelines to assist you in understanding the goals
of our program. This handbook will provide you with vital information in order to
develop and maintain an effective partnership in meeting our members’ needs. As
American Eldercare, Inc. (AEC) is a Provider Service Network (PSN) that is contracted with
7 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
the State of Florida to participate in the Long Term Care Managed Care Program. Our primary
goal is to identify members that may safely remain in their home environment and provide them
with quality community-based services in order to delay or avoid long-term placement in a
nursing home. We accomplish this by completing a comprehensive assessment and creating a
care plan that meets the individual needs of our members. If members are no longer able to
safely remain in their home we coordinate services for them to reside in an assisted living
facility, adult family home or a nursing home that meets their level of care. We are successful in
having our members remain in the least restrictive environment that safely meets their needs by
having a care manager specifically assigned to each individual member to coordinate both their
acute and long-term care needs.
LONG-TERM CARE MANAGED CARE PROGRAM
American Eldercare, Inc. is proud to participate as a contractor for the State of Florida to
operate a Medicaid funded program known as the Long-Term Care Managed Care
Program. Medicaid is a program for eligible individuals and/or families with low incomes
and resources. It is a means-tested program that is jointly funded by the state and federal
governments, and is managed by the states. People served by Medicaid must be U.S.
citizens or legal permanent residents, including low-income adults, their children, and
people with certain disabilities. Poverty alone does not necessarily qualify someone for
Medicaid. Medicaid is the largest source of funding for medical and health-related services
for people with limited income in the United States.
The Long-Term Care Managed Care Program is designed to care for all eligible individuals
over the age of 18 who meet a level of care to require nursing home care as well as a
financial criterion; both qualifications are determined by the state. The program provides
eligible individuals to access care in a nursing home or a less restrictive environment in the
community. The goal is to reduce the number of individuals residing in nursing homes that
can be cared for in a less restrictive environment in order to create cost savings for the state.
8 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
PRACTICE GUIDELINES
American Eldercare, Inc. has adopted practice guidelines that are embedded within our
policy and procedures and our daily business practices.
Practice Guideline Requirements:
a) Are based on valid and reliable clinical evidence or a consensus of healthcare
professionals in the field of disabilities and geriatric industry.
b) Considers the needs of the members.
c) Are adopted in consultation with contracted health care professionals when
deemed necessary.
d) Are reviewed and updated periodically as appropriate.
e) AEC will disseminate the guidelines to all affected providers and
upon request to members and potential members.
f) Decisions for utilization management, member education, coverage of services,
and other areas to which these guidelines apply will be consistent throughout the
Policy and Procedure Manual and daily business practices.
MISSION STATEMENT
Our mission is to provide comprehensive, effective, cost-efficient health care and related
services, through a community-based program tailored to the individual.
Core Values:
A - Advocacy
E - Ethics
C - Compassion
9 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
OFFICE HOURS
Our dedicated staff is available to answer any questions between the hours of 8:00 am -
8:00 pm, Monday – Friday. If you have questions regarding services or benefits, you can
call the Provider Help Line at (888) 998-7735. Our provider help-line is available twenty-
four (24) hours a day seven (7) days a week including weekends and holidays. For a
complete listing of our offices, please refer to Section 8, Appendix of this handbook.
AMERICAN ELDERCARE WEBSITE (www.americaneldercare.com)
The American Eldercare, Inc. website is designed to give providers quick access to current
provider and member information twenty four (24) hours a day, seven days a week. You
will also find information about other programs and useful information and resources about
American Eldercare, Inc. Please contact your local Provider Relations Specialist with any
questions or concerns regarding the website.
CONFIDENTIALITY STATEMENT
American Eldercare, Inc. maintains a policy to ensure that medical records, claims
information and grievances pertaining to members and providers will remain confidential.
The authorized release of any information is used only for the resolution of medical
problems or to enhance a member’s health. American Eldercare, Inc. will ensure
compliance with the Privacy and Security provisions of the Health Insurance Portability and
Accountability Act (HIPAA).
10 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
____________________________________________
2
COVERED SERVICES ______________________________________________
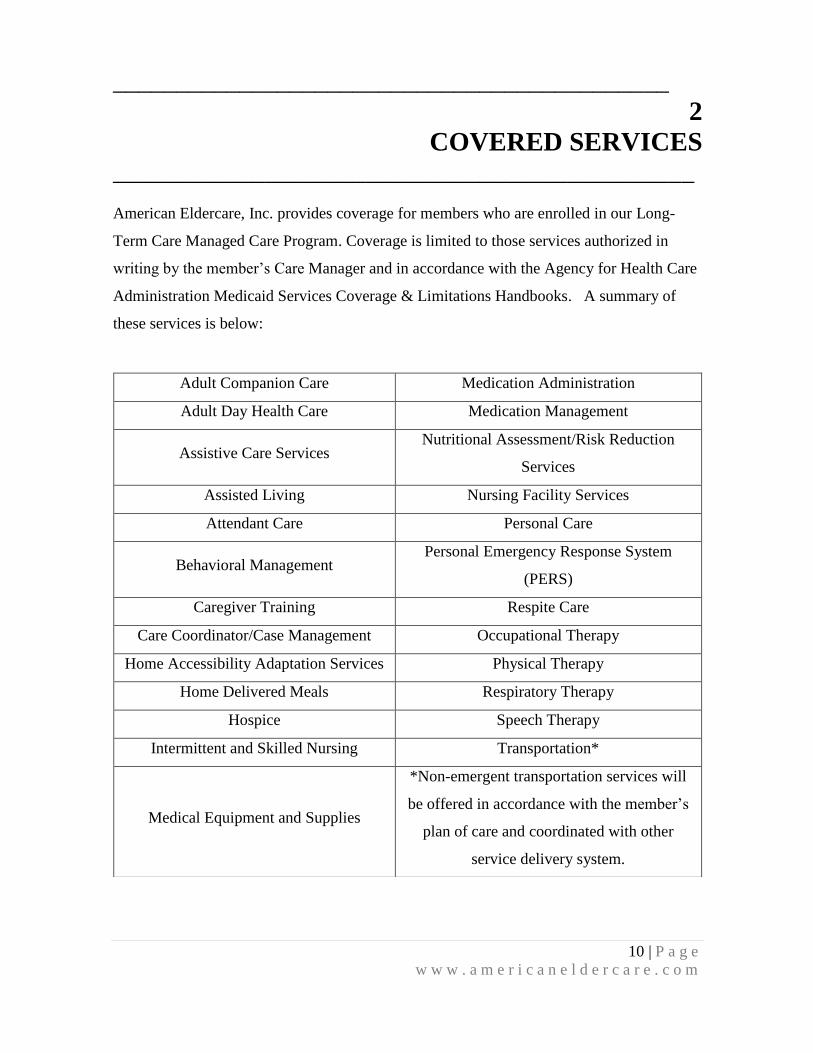
American Eldercare, Inc. provides coverage for members who are enrolled in our Long-
Term Care Managed Care Program. Coverage is limited to those services authorized in
writing by the member’s Care Manager and in accordance with the Agency for Health Care
Administration Medicaid Services Coverage & Limitations Handbooks. A summary of
these services is below:
Adult Companion Care Medication Administration
Adult Day Health Care Medication Management
Assistive Care Services Nutritional Assessment/Risk Reduction
Services
Assisted Living Nursing Facility Services
Attendant Care Personal Care
Behavioral Management Personal Emergency Response System
(PERS)
Caregiver Training Respite Care
Care Coordinator/Case Management Occupational Therapy
Home Accessibility Adaptation Services Physical Therapy
Home Delivered Meals Respiratory Therapy
Hospice Speech Therapy
Intermittent and Skilled Nursing Transportation*
Medical Equipment and Supplies
*Non-emergent transportation services will
be offered in accordance with the member’s
plan of care and coordinated with other
service delivery system.
11 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
MEDICAL NECESSARY/NECESSITY
Medical Necessary or Medical Necessity is determined as per 59G-1.010(166) as described
below:
“Medically necessary” or “medical necessity” means that the medical or allied care,
goods, or services furnished or ordered must:
(a) Meet the following conditions:
1. Be necessary to protect life, to prevent significant illness or significant disability, or
to alleviate severe pain;
2. Be individualized, specific, and consistent with symptoms or confirmed diagnosis of
the illness or injury under treatment, and not in excess of the patient’s needs;
3. Be consistent with generally accepted professional medical standards as determined
by the Medicaid program, and not experimental or investigational;
4. Be reflective of the level of service that can be safely furnished, and for which no
equally effective and more conservative or less costly treatment is available
statewide; and
5. Be furnished in a manner not primarily intended for the convenience of the
recipient, the recipient's caretaker, or the provider.
(b) “Medically necessary” or “medical necessity” for inpatient hospital services
requires that those services furnished in a hospital on an inpatient basis could not,
consistent with the provisions of appropriate medical care, be effectively
furnished more economically on an outpatient basis or in an inpatient facility of a
different type.
(c) The fact that a provider has prescribed, recommended, or approved medical or
allied care, goods, or services do not, in itself, make such care, goods or services
medically necessary or a medical necessity or a covered service.
EMERGENCY SERVICE RESPONSIBILITIES
If a member requires emergency acute care services, contact their primary insurance for
pre-certification or send them to the emergency room as deemed appropriate. Please
contact their assigned Care Manager or AEC Customer Service department once the
emergency is addressed so the Care Manager may follow up to coordinate care.
12 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
If a member requires emergency care that is a covered long-term care service, please
contact the Care Manager or AEC Customer Service Department to receive precertification.
If it is after business hours, please follow the prompts to reach our after-hours staff.
ADULT DAY CARE (ADC)
This service provides member with supervision, socialization and therapeutic activities in
an outpatient setting. This also provides caregiver with respite. Meals are included as part
of this service when the member is at the center during meal times.
Adult Day Care health services include but not are limited to the following:
1. Licensed nurse full-time
2. Supervised, recreational activities at least 80% of the day
3. Physical exercises
4. Cognitive exercises
5. Lunch and snacks
6. Coordination of transportation
7. Medication administration and management
8. Vital signs monitoring
9. Basic health monitoring, to include glucose level checks
10. Referral to physical therapy screening (conducted on-site)
11. Hands-on assistance with personal care, such as toileting, eating, ambulating and
grooming
ASSISTIVE CARE
24-hour services for Members in assisted living facilities, adult family care homes and
residential treatment facilities.
ASSISTED LIVING (ALF)
This service provides member with an alternative living arrangement where there is access
to 24-hour staff. Meals, personal care and housekeeping services are provided by staff.
Facility may be used for respite care. The facility provides a “home-like” environment to
13 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
members. The Community will provide member with the following services or as indicated
in each individual provider contract:
1. 24- hour access to staff
2. Bathing assistance
3. Medication management
4. Three meals per day, plus snacks
5. Incontinence management
6. Incontinence supplies
7. Nutritional supplements
8. Housekeeping
9. Personal laundry & linen service
10. Utilities
11. Transportation or coordination of transportation
12. Alarmed doors or locked unit
13. Personal hygiene items
14. Escort to dining room
15. Emergency/Disaster Plan
16. Dementia care
Respite Care – Provides caregivers with relief, for short periods of time. (May be
provided by an Assisted Living Community) Respite care does not substitute for the
care usually provided by a registered nurse, a licensed practical nurse or a therapist.
Transportation – All AEC contracts with ALFs require the ALF to coordinate
transportation for our members. AEC enrollees are eligible for transportation trips to
long-term care covered services as authorized by AEC. Please contact the enrollee’s
Care Manger for authorization approval. Our members will use their Medicaid gold
card or their current acute Medicaid health plan ID card respectively for all trips to
non-LTC covered services (including emergent transportation) as they do now.
14 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
AEC Welcome Home Program
Discharge planning from Hospital & Rehabilitation – AEC has a “Welcome Home
Program” in place in order to assist our members to return to your facility as soon as
their needs can be met in your community. Our Care Management staff will assist in
the coordination of their discharge including access to Medicare Home Health
services if needed. The success of this program requires your facility to participate
by evaluating your residents in a timely manner to coordinate a safe return.
Facilities that are not willing to participate in the Welcome Home Program may not
be eligible for a bed-hold payment.
Hospice
Providers are required to inform AEC staff of any changes or concerns they may
identify while providing services to a member in order to ensure their needs are
being met. This includes notification of a member being admitted to a hospital
and/or enrolling in a Medicare Hospice program. Notification must be provided
within twenty four (24) hours of the admission. Medicaid Hospice services require
pre-authorization from AEC.
BEHAVIORAL MANAGEMENT
This service provides behavioral health care services to address mental health or substance
abuse needs of long-term care members. The services are used to maximize reduction of
the member’s disability and restoration to the best functional level.
HOME ADAPTATIONS ACCESSIBILITY
These services provide member with home modifications, which promote safety. This
Includes installation of grab bars, ramps and widening of doors. Services do not include
home modifications, which are considered home improvements. All services must be
provided in accordance with applicable state and local building codes.
15 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Members or caregivers will be contacted within two (2) business days of receipt of
authorization from the AEC Care Manager to schedule an appointment. Installation will
take place within two (2) weeks.
HOME DELIVERED MEALS
This service provides members who are unable to shop or cook with nutritionally sound
meals that are delivered to the home hot, cold, frozen, dried, or canned with a satisfactory
storage life. Each meal is designed to provide 1/3 of the Recommended Dietary Allowance
(RDA). A signature must be obtained from the member or caregiver upon delivery of
meals. Members must go through their Care Manager to make any changes to their meal
delivery. Services will begin within five (5) business days of receiving a written
authorization from the AEC Care Manager.
HOME HEALTH CARE (HHC)
As a contracted provider for AEC the following procedures will be adhered to when
providing services.
a) AEC reserves the right to determine the plan of care for its members, and
will send a request of specific services and frequency in order to meet the
member’s needs. Services may be provided in a member’s home or an
assisted living facility on an hourly or per visit fee as authorized by AEC.
The HHC provider has a maximum of two (2) days to inform AEC staff if
the requested services can be provided and the anticipated start date.
b) HHC staff is required to have the Agency’s designated form signed by the
member verifying that the services were provided at the time of each visit,
including date/time of service and direct care staff that provided the service.
A copy of this form must be submitted to AEC when the claim is submitted.
16 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
c) If an AEC member is entitled to Medicare Home Health benefits, these
benefits will be utilized prior to services being authorized under your
contract with AEC.
Home Health services are authorized by the Care Manager on a weekly basis (Sun – Sat).
Pre-authorization is required by the Care Manager to provide services that exceed the
number of hours authorized in a day or in a week. The only variation that is allowable
without a pre-authorization is to switch the days of services within the same week, with
prior authorization of the member (patient). If the schedule change is permanent, the
provider should inform the Care Manager of the change.
Adult Companion
Companions can perform tasks such as meal preparation, laundry and shopping, while
providing socialization for the member. This includes light housekeeping tasks incidental to
the care and supervision of the member. Services do not include hands-on nursing care or
bathing assistance.
Family Training
This service provides training to family members in order to promote safety while caring
for the member. This includes education on diabetic management, transferring a person,
and how to use safety equipment properly.
Homemaker Services
This service provides member assistance with general household activities to include meal
preparation, laundry and light housekeeping.
Occupational Therapy
This service provides member with treatment to restore, improve or maintain impaired
function in regards to daily living tasks. (E.g. using a fork, shower chair, or cooking from a
wheel chair)

17 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Personal Care
This service provides member with assistance with bathing, dressing, eating, personal
hygiene and other activities of daily living. A personal care worker can do incidental
housekeeping, such as making beds and cleaning up areas where they have performed
services.
Physical Therapy
This service provides member with treatment to restore, improve or maintain impaired
function in regards to ambulation and mobility such as walking, transferring, or using a
walker or wheel chair.
Respite Care
This service provides caregivers with relief, for short periods of time. Respite care may be
provided by a Home Health Agency, Assisted Living Community or a Skilled Nursing
Facility. Respite care does not substitute for the care usually provided by a registered
nurse, a licensed practical nurse or a therapist.
Speech Therapy
This service provides member with evaluation and treatment with regards to oral motor
functions. (E.g. difficulties swallowing or speaking) This service also includes treatment to
restore, improve or maintain impaired functions in order to promote a member’s
independence and capacity to live safely in the home setting. This includes physical,
occupational and speech therapies.
HOSPICE
This service provides forms of palliative medical care and services designed to meet the
physical, social, psychological, emotional and spiritual needs of terminally ill members and
their families. Care Managers will coordinate this care with members enrolled in Medicare
Hospice services. If a member requires any hospice service traditionally covered by
Medicaid, pre-authorization is required from the Care Manager.
18 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
MEDICAL SUPPLIES (CONSUMABLE)
These services provide member and caregiver with supplies that assist in meeting the
member’s needs. Items include incontinent supplies and diabetic supplies not covered by
Medicare. These services do not include personal toiletries, over the counter medications or
household items.
Consumable medical supplies include adult disposable diapers, tubes of ointment, cotton
balls and alcohol for use of injections, medicated bandages, gauze and tape, colostomy and
catheter supplies, and other consumable supplies. Not included are supplies covered under
Home Health service, personal toiletries, and household items such as detergents, bleach,
paper towels, or prescription drugs.
Services require written authorization from the AEC Care Manager. Supplies will be
delivered to the member’s home and the member or caregiver will sign an itemized receipt.
Members must go through their Care Manger to make any changes to their order.
Nutritional supplements require both a Physicians prescription and pre-authorization from
the AEC Care Manager. Members authorized to live in a contracted facility will receive
this service directly from the facility.
MEDICAL SUPPLIES (DURABLE MEDICAL EQUIPMENT)
Durable Medical Equipment is medical equipment that can withstand repeated use; is
primarily and customarily used to serve a medical purpose; is generally not useful in the
absence of illness or injury; and is appropriate for use in the recipient's home. Medicare
and Medicaid Acute Care Programs cover most DME equipment that AEC members need.
Any items needed by AEC members that are not covered by Medicare require pre-
authorization from the AEC Care Manager.

19 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
NURSING FACILITY SERVICES (SNF)
This service provides twenty-four (24) hour assistance and nursing services for the member,
when they can no longer remain in the community. Member must be evaluated by
American Eldercare, Inc. staff to determine if they can be maintained in a less restrictive
environment.
Skilled nursing facility services will be coordinated with the members acute care coverage.
If a member is dual eligible for Medicare/Medicaid, AEC is responsible for coinsurance as
per the Medicaid crossover guidelines. Claims must be submitted with Medicare EOB.
The SNF staff is expected to inform AEC staff of any changes or concerns they may
identify while providing services to a member in order to ensure that their needs are being
met.
Respite Care – Provides caregivers with relief, for short periods of time. (May be
provided by a Skilled Nursing Facility Respite care does not substitute for the care
usually provided by a registered nurse, a licensed practical nurse or a therapist.
Transportation – All AEC contracts with SNFs require the SNF to coordinate
transportation for our members. AEC enrollees are eligible for transportation to
long-term care covered services, as authorized by AEC. Please contact the
enrollee’s Care Manager for authorization approval. Our members will use their
Medicaid gold card or their current acute Medicaid health plan ID card,
respectively, for all transportation trips to non-LTC covered services (including
emergent transportation) as they do now.
Hospice – Providers will inform AEC staff of any changes or concerns they may
identify while providing services to a member in order to ensure their needs are
being met. This includes notification of a member being admitted to a hospital
and/or going to a Medicare or Medicaid Hospice program. Medicaid Hospice
services require pre-authorization from AEC. Notification must be provided within
twenty-four (24) hours of a significant change in the member’s health care needs.
20 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Custodial Care
All members requiring this service must be assessed and determination must be
made by American Eldercare, Inc. that the member can no longer live in a less
restrictive setting. Members who receive approval for placement in a contracted
Nursing Facility for custodial care are required to pay the facility a patient
responsibility based on their income, which is determined by the Department of
Children and Families. Prior authorization is required by AEC.
AEC Welcome Home Program
Discharge planning from Hospital & Rehabilitation – AEC has a “Welcome Home
Program” in order to assist our members to return to the least restrictive
environment that safely meets their needs. Our Care Management staff will assist in
the coordination of our members discharge plan (including access to Medicare
Home Health and/or Assisted Living Placement services if needed). The success of
this program requires your facility to partner with the American Eldercare, Inc. staff
in order to implement a safe discharge plan.
NUTRITIONAL ASSESSMENT/RISK REDUCTION
This service provides member with an assessment, hands-on care and guidance for the
caregiver and members with respect to nutrition. (Provided by a dietitian usually from a
Home Health Agency) AEC reserves the right to determine the plan of care for its
members and will send a request of specific services and frequency in order to meet the
member’s needs. Services may be provided in a member’s home or an assisted living
facility on an hourly or per visit fee as authorized by AEC. The provider has a maximum of
two (2) days to inform AEC staff if the requested services can be provided and the
anticipated start date.
PERSONAL EMERGENCY RESPONSE SYSTEM (PERS)
The installation and service of an electronic device that enables members at high risk of
institutionalization to secure help in an emergency. The PERS is connected to the
21 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
member's phone and programmed to signal a response center once a "help" button is
activated. The member may also wear a portable "help" button to allow for mobility.
PERS services are generally limited to those members who live alone or are alone for
significant part of the day and who would otherwise require extensive supervision.
Provider will train AEC members on the use and monthly testing of the unit upon
installation and will notify AEC via telephone or fax if a member utilizes the system.
Provider is expected to install a medical alert system within five (5) business days after
receiving written authorization from an AEC Care Manager.
PHARMACY BENEFITS
American Eldercare, Inc. provides a $15 over the counter (OTC) benefit for our members.
OTC formulary is available upon request. Members must have a physician’s order to
receive OTC under this benefit.
TRANSPORTATION
All AEC contracts with SNFs, requires the SNT to coordinate transportation for our
members. AEC enrollees are eligible for transportation trips to long-term care covered
services, as authorized by AEC. Please contact the enrollee’s Care Manager for
authorization approval. Our members will use their Medicaid gold care or their current
acute Medicaid health plan card, respectively, for all transportation trips to non-LTC
covered services (including emergent transportation) as they do now.
Transportation for non-medical appointments can be provided for services AEC pre-
authorized only. Please contact the member’s assigned Care Manager for more details.
QUALITY ENHANCEMENTS
Quality enhancement is education and/or community-based services will be coordinated by
the Care Manager to address any concerns related to: safety and fall prevention, disease
management, education on end of life issues, advance directives, and domestic violence.
22 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
______________________________________________
3
ELIGIBILITY _____________________________________________
Enrollment in American Eldercare, Inc’s. Long-Term Care Managed Care Program is
based on standards of eligibility established by the Department of Elder Affairs (DOEA),
Comprehensive Assessment and Review for Long Term Care Services (CARES) unit and
financial eligibility by the Florida Department of Children and Families (DCF).
CONDITIONS OF ENROLLMENT
Recipients eligible for enrollment must be:
18 years of age or older;
Reside in the State of Florida;
Determined by CARES to be at risk of nursing home placement, meet specific
clinical criteria, and can be safely served with home and community-based services;
DCF determines a person’s financial eligibility. Financial eligibility for the
program is the same as Medicaid Institutional Care Program (ICP).
For specific information on the eligibility criteria, you may contact your Provider Relations
Specialist or the Care Management Department near your local office. If you know
someone that may qualify for the program, you may have him or her contact your local
Care Management staff or call the CARES office directly to apply.
CARES Referrals
If a member believes they may qualify, the member or their representative must contact
their local CARES office to apply for the AEC Long-Term Care Managed Care Program
Plan. As a professional, if you decide to assist a potential enrollee in the application
process, first make sure to obtain written consent from the enrollee or their representative.
23 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
MEDICAID PENDING
These are individuals who have applied for the Program and have been determined
medically eligible by CARES but not been determined financially eligible for Medicaid by
DCF. These individual are designated at “Medicaid Pending”.
American Eldercare, Inc. has elected to provide services to these individuals who reside in
the community, and assist them with completing and returning their application to DCF. If
DCF determines the individual is not financially eligible for Medicaid, American Eldercare,
Inc. will terminate services and seek reimbursement from the individual that signed the
Financial Agreement on the member’s behalf. The individual will receive an itemized bill
for services received from AEC during the ineligible span.
If a Medicaid pending enrollee resides in a nursing home, the facility is required to assist
with the Medicaid pending process.
MEMBERSHIP IDENTIFICATION (ID) CARD
Each member of American Eldercare, Inc. Plan receives an American Eldercare, Inc. Plan
member identification (ID) card. If the card is lost or stolen, the member should contact
their Care Manager. A copy of the member’s identification card is below.
MEMBERSHIP CARD
Member & Care Management Services
Toll Free#:
RX BIN # 009430
RX Group # AEC00001
Name:
AEC ID#
Medicaid ID#
Person Code: 01
American Eldercare is your long-term care service provider only. Utilize your
primary insurance for acute care services. All long-term services are required to
have pre-authorization contract your Care Manager at the number listed on the
front of this ID card. After hours:
American Eldercare Member Help Line: 888-998-7732
American Eldercare Provider Help Line: 888-998-7735
Claims: American Eldercare Plan: 14565 Sims Road, Delray Beach, FL 33484
ProCare PBM Pharmacy Network (800) 699-3542
Member: OTC Drugs that are covered by your plan may be filled by
participating pharmacies per your plan requirements. This card is for
identification purposes only, and you may be required to provide additional ID
at the time your prescription is filled. Presentation of this card does not
guarantee eligibility. Unauthorized or fraudulent use of this card is punishable
by law. ProCare PBM reserves the right to revoke this ID card at any time
Pharmacy: ProCare PBM is not responsible for payment of claims to a
nonparticipating Pharmacy
SAMPLE SAMPLE
24 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
REFERRALS TO AMERICAN ELDERCARE
If a person believes he/she may qualify to participate in the program, the person or their
representative must contact the local CARES office to apply for American Eldercare, Inc.
Long-Term Care Managed Care Program Plan. As a provider, if you decide to assist the
person in the application process, you must obtain their consent. The person or the provider
is always welcome to contact AEC prior to or after contacting CARES to obtain
information about our program. To locate the CARES office in your area, please refer to
Section 8, Appendix, of this handbook.
MEMBER DISENROLLMENT
Disenrollment with Cause
If a member is a mandatory enrollee and want to change plans after the initial
ninety (90) day period ends or after open enrollment period ends, the member must have a
state-approved good cause reason to change plans.
State will review and determine approval of the member’s request. Please contact the
Enrollment Broker at (877) 711-3662 for more information. The following are potential
good cause reasons to change managed care plans:
1) The enrollee does not live in a region where the Managed Care Plan is
authorized to provide services, as indicated in FMMIS.
(2) The provider is no longer with the Managed Care Plan.
(3) The enrollee is excluded from enrollment.
(4) A substantiated marketing or community outreach violation has occurred.
(5) The enrollee is prevented from participating in the development of his/her
treatment plan/plan of care.
(6) The enrollee has an active relationship with a provider who is not on the
Managed Care Plan’s panel, but is on the panel of another managed care plan. “Active
relationship” is defined as having received services from the provider within the six (6)
months preceding the disenrollment request.
25 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
(7) The enrollee is in the wrong Managed Care Plan as determined by the Agency.
(8) The Managed Care Plan no longer participates in the region.
(9) The state has imposed intermediate sanctions upon the Managed Care Plan, as specified
in 42 CFR 438.702(a)(3).
(10) The enrollee needs related services to be performed concurrently, but not all
related services are available within the Managed Care Plan network, or the enrollee’s PCP
has determined that receiving the services separately would subject the enrollee to
unnecessary risk.
(11) The Managed Care Plan does not, because of moral or religious objections, cover
the service the enrollee seeks.
(12) The enrollee missed open enrollment due to a temporary loss of eligibility,
defined as sixty (60) days or less for LTC enrollees and one hundred eighty (180) days
or less for MMA enrollees.
(13) Other reasons per 42 CFR 438.56(d)(2) and s. 409.969(2), F.S., including, but not
limited to: poor quality of care; lack of access to services covered under the Contract;
inordinate or inappropriate changes of PCPs; service access impairments due to significant
changes in the geographic location of services; an unreasonable delay or denial of service;
lack of access to providers experienced in dealing with the enrollee’s health care needs; or
fraudulent enrollment.
Some Medicaid recipients may change managed care plans whenever they choose, for any
reason. To find out if a member may change plans, call the Enrollment Broker at (877)-711-
3662.
Disenrollment without Cause
(1) During the ninety (90) days following the enrollee’s initial enrollment, or the date the
Agency or its agent sends the enrollee notice of the enrollment, whichever is later;
(2) At least every twelve (12) months;
(3) If the temporary loss of Medicaid eligibility has caused the enrollee to miss the open
enrollment period;

26 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
(4) When the Agency or its agent grants the enrollee the right to terminate enrollment
without cause (done on a case-by-case basis); or
(5) During the thirty (30) days after the enrollee is referred for hospice services in order to
enroll in another managed care plan to access the enrollee’s choice of hospice provider.
Without cause, for members not subject to open enrollment, is at any time.
HOSPICE
Members can be simultaneously enrolled in American Eldercare, Inc. and Hospice.
Medicaid Hospice services require prior approval from AEC. Dual eligible may enroll in
Medicare hospice, and the Care Manager will assist to coordinate services. Members or
their representative is required to contact their American Eldercare, Inc. Care Manager,
prior to enrolling in a hospice program.
27 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
______________________________________________
4
CARE MANAGEMENT ______________________________________________
The Care Management team provides assistance to members and families to gain access to
community services in order to delay or avoid nursing home placement. If a member needs
can no longer be met safely in a community, the Care Manager will assist in placement and
supervision in a community setting or a nursing home that can safely meet their needs.
The Care Manager is responsible for developing an individualized plan of care that meets
each member’s needs in a safe environment. Most Long-Term Care services and supplies
must be pre-authorized by our Care Management team before they can be provided to an
American Eldercare, Inc. member. Please contact the local Care Management team with
requests for prior authorizations.
Care Managers can assist members with:
Authorization for services (See “Procedures for Authorization of Services”)
Change in services
Coordination of acute care services
Discharge planning from inpatient services
Disenrollment
Eligibility
Obtaining replacement ID Card
Answer any questions
Concerns about their care
AUTHORIZATIONS
If a member requires specialized treatment or services, a Care Manager will issue an
authorization for services to a participating provider. Our Care Managers will assess our
member’s needs prior to ordering any services.
28 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Procedures for Authorization of Services
1. Upon determination that a member needs services from a facility or agency, the
Care Manager will contact your staff to inquire if the services can be provided. If so,
the Care Manager will fax a Request for New Services form. A sample of this
form can be found in Section 7, Forms of this handbook. This authorization is good
for one year of services unless otherwise indicated at the time of authorization. If
dates of services are not established, your staff is responsible to follow up with the
Care Manager with the date services will begin.
2. If a member needs to stop services for a short period of time (e.g. due to a
hospitalization), the Care Manager will fax a Hold/Resume Services Request form.
A sample of this form can be found in Section 7, Forms, of this handbook.
3. If a member no longer needs services from your agency, the Care Manager will fax
a Termination of Services Request form. A sample of this form can be found in
Section 6, Forms of this handbook.
4. If a member needs an increase or decrease in services, the Care Manager will fax a
Change of Services Request form. A sample of this form can be found in Section
7, Forms of this handbook.
If you have any questions or concerns about a member, please contact our Care
Management team in your local area.
Chronic/Complex Conditions
All AEC covered services including but not limited to treatment for chronic and complex
conditions requires pre-authorization from a Care Manager. AEC staff will coordinate
those services with a provider of the member’s choice. If the member requires a service
which is available through Medicaid or Medicare but is not covered by American Eldercare,
Inc., the member may receive the service through other coverage they are enrolled. A Care
Manager will assist with the coordination if it is determined there is a need for the service.
29 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Service Limitations:
Services must be pre-approved
Services must be provided by an active provider in AEC’s provider network
Services must be a covered benefit or approved expanded benefit (see below
“Covered Services”)
Services must be medically necessary:
o Be necessary to protect life, to prevent significant illness or significant
disability, or to alleviate severe pain;
o Be individualized, specific, and consistent with symptoms or confirmed
diagnosis of the illness or injury under treatment, and not in excess of the
patient’s needs;
o Be consistent with generally accepted professional medical standards as
determined by the Medicaid program, and not experimental or
investigational;
o Be reflective of the level of service that can be safely furnished, and for
which no equally effective and more conservative or less costly treatment is
available; statewide; and
o Be furnished in a manner not primarily intended for the convenience of the
recipient, the recipient's caretaker, or the provider.
ABUSE, NEGLECT, EXPLOITATION
American Eldercare, Inc. must notify government authorities if we suspect that one of our
members is a victim of abuse, neglect or exploitation. Our network providers are expected
to report any incidents or concerns regarding our members.
Please report any suspected cases of abuse, neglect, and/or exploitation to Adult Protective
Services toll free: (800) 96ABUSE (962-2873), should you have any questions please call
our local office for assistance.
American Eldercare, Inc. requires all direct service providers who provide hands-on care to
our members to attend and complete Abuse, Neglect & Exploitation Training. If your
30 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
licensure does not require Abuse, Neglect and Exploitation Training and you would like
American Eldercare Inc.’s staff to assist you in developing a program for your staff, please
contact your local Provider Relations Specialist.
CRITICAL INCIDENT REPORTING
Critical incidents are required to be reported to American Eldercare, Inc. staff at the time
they are identified by a provider. A critical incident is defined as an adverse or critical
event that negatively impacts the health, safety, or welfare of a member. Critical incidents
may include events involving abuse, neglect, exploitation, major illness or injury,
involvement with law enforcement, elopement/missing, or major medication incidents.
Critical incidents involving abuse, neglect or exploitation must also be reported by the
provider to Adult Protective Services. Providers are expected to work with AEC staff in
resolving all identified critical incidents in a timely manner to ensure the safety and well-
being of our members.
MEMBER RIGHTS AND RESPONSIBILITIES:
Care Managers provide all members with this information at the time of enrollment and
annually.
You have the right:
To be fully informed in advance of all care and treatment to be provided by
the agency, and changes in care or treatment; the right to receive a copy of
his/her plan of care if he/she so requests.
To be fully informed of services available from the agency and how to access
care.
To be fully informed by a physician of health status unless medically
contraindicated.
To be afforded the opportunity to participate in the planning of the care plan
and to refuse treatment without retribution, while fully informed of the
possible medical consequences of his/her refusal.
To be assured of confidentiality of records and to approve or refuse the release
of information not authorized by law.
31 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
To be treated with consideration, respect, full recognition of dignity and
individuality, including privacy in treatment and in care for personal needs; to
have property treated with respect.
To file a grievance without fear of discrimination or reprisal from the agency;
to be informed of the State Hotline number with hours of operation and
purpose for obtaining information on home health agencies.
To be assured qualified personnel who provide proper identification at time of
visit.
To be served without regard to race, color, creed, sex or age, national origin,
ancestry or handicap/disability.
To be advised, before care is initiated, of the cost of services and the extent to
which payment may be required by the patient.
To receive home and community-based services in a home-like environment and
participate in his or her community regardless of his or her living arrangement.
To direct your care with your own staff and/or providers.
You have a responsibility:
To provide accurate and complete medical and health history information as
he/she understands it.
To participate with the plan of treatment, when possible, and make available
an informal caregiver to assume primary care, as appropriate.
To have a primary care physician who will provide orders (as required) for
skilled home care treatments and services.
To inform agency staff about any changes in health status, medications or
treatments; to inform the agency of any change in financial status that may
affect reimbursement for home care.
To have a plan for management of emergencies and to access this plan if
necessary for safety.
To inform the agency of the presence of advance directives and provide
copies, as appropriate.
To accept services of agency staff, without regard to race, creed, color,
religion, national origin, handicap, sex or age.
To report fraud, abuse, and overpayment :

32 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
(a) To report suspected fraud and/or abuse in Florida Medicaid, call the
Consumer Complaint Hotline toll-free at 1-888-419-3456: FL General Hotline:
1-866-966-7226: AEC Compliance Hotline: 1-877-217-9717 or complete a
Medicaid Fraud and Abuse Complaint Form, which is available online at:
https://apps.ahca.myflorida.com/InspectorGeneral/fraud_complaintform.aspx;
(b) If you report suspected fraud and your report results in a fine, penalty or
forfeiture of property from a doctor or other health care provider, you may be
eligible for a reward through the Attorney General’s Fraud Rewards Program
(toll-free 1-866-966-7226 or 850-414-3990). The reward may be up to twenty-
five percent (25%) of the amount recovered, or a maximum of $500,000 per
case (Section 409.9203, Florida Statutes). You can talk to the Attorney
General’s Office about keeping your identity confidential and protected.
33 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
_________________________________________________
5
PROVIDER RESPONSIBILITIES ________________________________________________
The Provider Relations Department has designed this handbook to assist network providers with
an overview of our operational policies and procedures. As a participating provider, you and
your staff will have a dedicated Provider Relations Specialist who will be a key contact. They
are responsible for ensuring services are available to our members by obtaining contracts,
providing ongoing community and provider training and education about American Eldercare,
Inc.’s Long-Term Care Managed Care Program. They also assist our network providers in
understanding the terms of our contract and resolve any problems you may encounter.
You are encouraged to contact your Provider Relations Specialist whenever you have any
questions, comments or concerns. To locate your local Provider Relations Specialist, please
refer to the list of offices located in Section 8, Appendix of this handbook.
CREDENTIALING COMMITTEE
The Credentialing Committee has the responsibility to establish and adopt, as necessary, criteria
for provider participation and termination and direction of the credentialing procedures,
including provider participation, denial and termination. Committee meetings are held at least
monthly and as deemed necessary. Failure of an applicant to adequately respond to a
request for assistance may result in termination of the application process.
INITIAL CREDENTIALING
Providers seeking participation with American Eldercare, Inc. must complete an application with
required documentation and a signed contract. It is required that all providers maintain active
status with licensure and insurance coverage and will provide proper documentation annually as
documents expire. It is required that American Eldercare, Inc. be immediately notified of any
changes in your licensure, status of insurance coverage, disciplinary actions, and/or ownership.
AEC credentialing review includes but not limited to the following criteria:
34 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
1) Copy of current provider’s medical license, or occupational or facility license as
applicable to provider type, or authority to do business including documentation of
provider qualification as outline by governing Agency;
2) No revocation, moratorium or suspension of license;
3) A satisfactory Level II background check pursuant to guidelines for all treating
providers not currently enrolled in Medicaid’s fee-for –service program;
4) Medicaid ID number for enrollment by state Medicaid program for compliance with
data submission. AEC will take the necessary steps necessary to ensure that your
business is recognized by the state Medicaid program including its enrollment broker
as a participating provider and that your submission of encounter data is accepted by
the Florida MMIS and/or the state’s encounter data warehouse.
5) Certificate of Insurance
a) Proof of General Liability, Professional Liability (as applicable)
b) Proof of Workers Compensation (as applicable);
c) American Eldercare Inc. should be listed as notify agent or Certificate Holder on
the certificate of insurance;
6) Licensure Inspection/AHCA survey as applicable;
7) W-9 indicating Taxpayer Identification Number.
Site Visits
Site visits evaluate appearance, accessibility, recordkeeping practices, and safety procedures.
These visits are performed at assisted living facilities and adult family care homes to evaluate a
home-like environment. Other site visits will be performed as deemed necessary.
RE-CREDENTIALING
Re-credentialing is the process of re-verifying the credentialing information of all providers
previously credentialed. The purpose of this process is to identify any changes in the provider’s
licensure, sanctions, certification, competence or health status, which may affect the ability to
35 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
perform services the provider under contract. Each provider will be re-credentialed at a
minimum every three years. A notification will be sent to the provider for re-verification of
credentialing. All network providers must submit updated documents as it expire. Failure to
provide updated documentation may delay payment. A provider’s agreement may be terminated
if at any time it is determined the credentialing requirements are no longer being met or the
provider fails to complete the re-credentialing process.
.
PROVIDER MONITORING
American Eldercare, Inc. will routinely monitor providers to ensure any changes in licensure
status, sanctions or other adverse actions are reviewed by the Credentialing Committee.
Providers whose license was suspended or revoked are subject to termination.
RIGHT TO REVIEW AND CORRECT INFORMATION
All providers participating with American Eldercare, Inc. have the right to review information
obtained to evaluate their credentialing and/or re-credentialing application. This includes
information obtained from any outside primary source such as the National Practitioner Data
Bank, insurance carriers and other sources as appropriate. This does not allow a provider to
review references, recommendations or other information that is peer review protected.
RIGHT TO APPEAL ADVERSE CREDENTIALING DETERMINATIONS
Providers who are declined participation have the right to request a reconsideration of the
decision in writing within fourteen (14) days of formal notice of denial. All written requests
should include additional supporting documentation in favor of the applicant’s reconsideration
for participation in American Eldercare, Inc. Reconsiderations will be reviewed by the
Credentialing Committee at the next regularly scheduled meeting, but in no case later than sixty
(60) days from the receipt of the additional documentation. The applicant will be sent a written
response to the request within two (2) weeks of the final decision.
36 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
NATIONAL PROVIDER IDENTIFIER (NPI)
The National Provider Identifier is a unique government-issued standard 10 digit identifier
mandated by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). This
identifier will replace all current health care providers’ numbers that are used in HIPAA standard
transactions. American Eldercare, Inc. will require participating provider as appropriate to
comply with this mandate. Please refer to the CMS website at
www.cms.hhs.gov/apps/npi/01_overview.asp for additional information and assistance with
applying for a NPI.
PROVIDER ORIENTATION AND EDUCATION
Your Provider Relations Specialist is available to provide an initial orientation within thirty (30)
calendar days of completing the credentialing process to review American Eldercare, Inc.’s
policies and procedures. These personalized meetings are scheduled at your convenience,
including any staff you would like to attend. Additional educational trainings can be scheduled
anytime by contacting your local Provider Relations Specialist.
NOTICE OBLIGATION
The network provider is responsible for giving the appropriate notices as outlined in this provider
handbook and under the terms of your contract with American Eldercare, Inc.
Changes in your Office
Notify your Provider Relations Specialist immediately of any changes in your office such as:
Physical address change
Tax identification/billing address change (W-9 required)
Demographic changes (e.g. telephone, fax, email, and administrative staff changes)
Name and Ownership change (60-day notice)
This will ensure your information is properly listed in the Provider Directory and all payments
made are properly reported to the Internal Revenue Service. A Provider Notice of Change form
37 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
is located in Section 7, Forms of this handbook. Failure to comply with this section could lead to
a delay in payments.
Providing Covered Services
In the event there are changes in your office that will affect your company’s ability to provide
services to American Eldercare Inc.’s members, please notify the Provider Relations Department
immediately.
PROVIDER HANDBOOK
The Provider Handbook provides comprehensive information to assist you with information on
American Eldercare Inc’s. process and procedures. You will be notified of updates to this
handbook via bulletins and notices posted on our website. You can access the Provider
Handbook by visiting our website at www.americaneldercare.com and click on the Provider tab.
If you would like to receive a hard copy of this handbook mailed to your office at no charge,
please contact your Provider Relations Specialist. While visiting our website, you will find other
educational materials and resources to assist you with the program.
PROVIDER DIRECTORY
The Provider Directory is a monthly listing of all participating network providers with American
Eldercare, Inc. A copy of this document is available upon request from the Provider Relations
Department. You can also access the Provider Directory on our website at
www.americaneldercare.com
PARTICIPATING AGREEMENT STANDARDS
By signing an American Eldercare Inc. contract, providers are required to comply with all
applicable federal and state laws and licensing requirements. Providers are required to maintain
back up procedures for absent employees to ensure services are not interrupted and sufficient
staff. American Eldercare, Inc. may exercise its options to terminate a participating provider
from the provider network with the appropriate notice.
38 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
ACCESSIBILITY AND AVAILABILITY
American Eldercare, Inc. has adopted service standards regarding the availability of participating
provider services. All providers are expected to maintain these standards as outlined in your
contract.
Accessibility Monitoring
Compliance with the availability and accessibility standards are monitored on a regular basis
through random sampling, review of member concerns, and member satisfaction surveys to
ensure members have reasonable access to providers and services.
PROVIDER SATISFACTION SURVEY American Eldercare, Inc. conducts an annual provider satisfaction survey which includes
questions to evaluate provider satisfaction with our services such as claims, communications,
utilization management, and provider services. Providers are randomly selected and are kept
anonymous. We encourage you to participate and respond to the survey as the results are
analyzed and used to form provider related quality improvement initiatives.
PROVIDER MEDICAL/CASE RECORD REVIEW
1. AEC staff will conduct reviews at all the following provider and facility provider sites
every other year:
a. Adult Family Care Homes
b. Assisted Living Facilities
c. Adult Foster Care Facility Sites
d. Home Health Agencies
2. For service providers with multiple office locations, staff will conduct reviews at each
practice site at least every three (3) years.
39 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
3. Specific review tools applicable to each type of provider will be shared with the provider
and utilized to conduct the reviews after establishment of inter-rater reliability.
4. A minimum of five (5) records or 5% of the member census (whichever is greater) will
be reviewed per site. The cases will be selected randomly and be evaluated for
compliance in meeting nationally recognized accrediting body medical/case record
review standards.
5. Medical Record confidentiality will be maintained by use of patient ID numbers and
records will not be removed from the provider or facility provider location for security
reasons.
6. After each provider review is complete, the data will be submitted to the Corporate Q/I
department where it will be analyzed, aggregated and compared.
7. On a quarterly basis, the Q/I department will report the results of the record reviews to
the COO, Senior Management team and the Provider Relations department with
recommendations for further action if indicated.
TERMINATION OF PROVIDER CONTRACT
Each provider has the right to terminate his/her contract with American Eldercare, Inc. You
must submit your request in writing and provide a sixty (60) days notice. All termination
requests should be mailed to the following:
American Eldercare, Inc.
14565 Sims Road
Delray Beach, FL 33484
Attention: Provider Relations Department
OUT-OF-NETWORK / NON-CONTRACTED SERVICES
An out-of-network provider is any provider that is not directly contracted with American
Eldercare, Inc. American Eldercare, Inc. is not responsible for payment of any services provided
by an out-of-network provider without written prior authorization.
Non-contracted services are any services not defined on Schedule B of your contract. American
Eldercare, Inc. is not responsible for payment of non-contracted services. If you or your staff
identifies a service that a member may require that is not listed in your contract please contact
the members Care Manager to evaluate the members needs and determine if the service can be
40 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
authorized by AEC. If the Care Manager determines the services should be authorized by AEC,
they will contact your local Provider Relations Specialist to discuss adding an addendum to your
contract.
American Eldercare, Inc. is not responsible for payments of any services ordered by a member
from a participating provider, without written pre-authorization from an American Eldercare,
Inc. Care Manager. Please contact the member‘s assigned Care Manager to request authorization
prior to providing services.
COMMUNITY OUTREACH/MARKETING
All providers must comply with the following standards regarding outreach marketing activities
in your office or at sponsored events:
1. Providers may display health plan specific materials in their own offices.
2. Providers cannot orally or in writing compare benefits or provider networks among
Plans, other than to confirm whether they participate in a Plan’s network.
3. Providers may announce a new affiliation with health plan and include it on a list
given to their patients with plans with which they contract.
4. Health care providers may co-sponsor events, such as health fairs and advertise in
indirect ways; such as television, radio, posters, fliers, and print advertisement.
5. Providers may not furnish lists of their Medicaid patients to another Plan with which
they contract, or any other entity, nor can providers furnish other health plans’
membership lists to the health plan, nor can providers take applications in their office.
6. Providers may distribute information about non health plan-specific health care
services and the provision of health, welfare and social services by the State of
Florida or local communities, as long as any inquiries from prospective members are
referred to member services or the Agency enrollment broker.
The use of American Eldercare, Inc. name will require written notice prior to use in television,
radio, posters, fliers, and print advertisement.
41 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
PROVIDER RESPONSIBILITIES
The Provider should adhere to the following:
Provide all services in a culturally competent manner accommodate those with
disabilities and not discriminate against anyone based on his/her health status.
Treat all members with respect and dignity, provide them with appropriate privacy and
treat member disclosures and records confidentially, giving members the opportunity to
approve or refuse their release.
Maintain a safe environment and comply with City, State, and Federal regulations
concerning safety and public hygiene.
Ensure accessibility and availability of services to members.
Participate and cooperate in quality management, utilization review, and continuing
education with other similar programs to provide quality care in a responsible and cost
effective manner.
Participate in and cooperate with grievance procedures when notified of any member
complaints or grievances.
Comply with all applicable federal and state laws regarding the confidentiality of member
records.
Maintain communication with the appropriate agencies to provide quality member care.
Ensure enrollment by state Medicaid program for compliance with data submission.
American Eldercare, Inc. providers should refer to their contract for complete information
regarding providers’ responsibilities and obligations. Failure to comply with could result in
contract termination.
PROVIDER COMPLAINT SYSTEM
Providers have the right to register a provider complaint involving a dispute with American
Eldercare, Inc. policies, procedures or any aspect of the Plan’s administrative function. Every
effort will be made to resolve the issue informally. In the event the issue cannot be resolved
42 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
informally, a complaint may be filed telephonically at (561) 860-8660 or toll free at (888) 970-
6663. You can also submit the compliant in writing by mailing to the Provider Relations
Department at:
American Eldercare, Inc.
14565 Sims Road
Delray Beach, FL 33484
ATTN: Provider Relations – Provider Complaint
Provider Complaint Review
Upon receipt of a complaint, American Eldercare, Inc. will thoroughly investigate each
complaint using applicable statutory, regulatory, contractual and provider contract provisions,
collecting all pertinent facts from all parties and applying the Plan’s written policies and
procedures. A provider complaint may be filed using the following steps:
Verbal Complaint
A Provider Relations Specialist will receive the initial call and attempt to resolve any
issues or concerns at the time of the call. If the Provider requests to file a complaint, the
Provider Relations Specialist will log the details in the Provider Relations Module
immediately.
All complaints will be acknowledged in writing within three (3) business days from the
initial call. The provider will be notified verbally or in writing that the complaint has
been received and the expected date of resolution. The Provider will be notified in
writing regarding the results of the inquiry within fifteen (15) calendar days from receipt
of the initial complaint.
Written Complaint
The Provider will complete the Provider Complaint Form (see Section 7 – Forms) and fax
or mail the form. The complaint will be logged in the Provider Relations Module on the
same day of receipt.
43 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
All complaints will be acknowledged in writing within three (3) business days from the
initial call. The provider will be notified verbally or in writing that the complaint has
been received and the expected date of resolution. The Provider will be notified in
writing regarding the results of the inquiry within fifteen (15) calendar days from receipt
of the initial complaint.
The Provider has forty-five (45) calendar days to file a written complaint for issues that are
claims related.
CULTURAL COMPETENCY
American Eldercare, Inc. expects our members will receive understandable and respectful care
that is provided in a manner compatible with their cultural health beliefs and practices and
preferred language. AEC encourages participatory and collaborative partnerships with
communities to be utilized in a variety of formal and informal mechanisms to facilitate
community and member involvement in designing and implementing culturally and linguistically
appropriate services. AEC staff will coordinate language assistance to our members who have a
limited English proficiency.
Providers may access the full AEC Cultural Competency Plan on our website or you can request
a hard copy of the Cultural Competency Plan at no charge by contacting the Provider Relations
Customer Service Line at (888) 998-7735.
44 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
_________________________________________________
6
CLAIMS/BILLING _________________________________________________
American Eldercare, Inc. maintains and complies with HIPAA standards for the submission and
adjudication of claims. This section will provide you information regarding the submission and
payment process.
CLAIM SUBMISSION
A clean claim is a claim that can be processed without obtaining additional information from the
provider of the service or from a third party. It does not include a claim from a provider who is
under investigation for fraud or abuse, or a claim under review for medical necessity, pursuant to
42 CFR 447.45.
All claims should be submitted to American Eldercare Inc. within six (6) months from the date
of service. If AEC is the secondary payer, claims should be submitted within ninety (90)
calendar days after the final determination of the primary payer. The Managed Care Plan shall
not deny claims submitted by a non-participating provider solely based on the period between the
date of service and the date of clean claim submission, unless that period exceeds three-hundred
sixty-five (365) days. Claims that are incomplete, illegible or missing any identifiable
information may delay payment or could result in a denial of payment.
ELECTRONIC CLAIMS
American Eldercare, Inc. is capable of receiving electronic claims submission. The acceptable
formats include X12 5010 837 institutional, professional, and dental formats. American
Eldercare, Inc. also allows for direct data entry (DDE) through our company portal. To be set up
with electronic claim submission, please contact the eBilling department below:
Email Address: [email protected]
Phone Number: 561.665.4415
45 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
PAPER CLAIMS
Please submit claims on one of the following claim form types:
Form CMS 1500
(Adult Day Care, Assisted Living Facility, Home Health, Home Delivered Meals, Consumable
Medical Supplies, Environmental Adaptation)
Form UB04 (Skilled Nursing Facility, Hospitals)
Please make sure that the description of services listed on your claim form matches the Service
Requests authorization document forwarded by the Care Manager.
To avoid a delay in processing your claims, please include the following information on claims:
Member’s name (Last, First)
Member’s date of birth
Member’s address
Provider information (Provider’s name, address and tax identification)
Provider signature
Description of service and code provided
Service / Procedure/ HCPCS code
Date(s) of service
Units of Service (amount of service hours provided or quantity of items provided)
Total number of units billed and total dollar amount billed
Amount of hours services provided or quantity of items provided
AEC Member ID or Medicaid ID, if available
Plan Identification
Mail all paper claims to the following address:
American Eldercare, Inc.
Attn: Claims Department
14565 Sims Road
Delray Beach, FL 33484
46 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
If you have any questions or require training regarding submitting claims, please contact your
local Provider Relations Specialist.
ENCOUNTER DATA
Transportation and capitated providers will need to submit encounter data claims and encounter
data is also required for any service American Elder Care directly pays (not claims processed
through the Medicaid fiscal agent). American Eldercare is authorized to take the necessary steps
to ensure that providers are recognized by the state Medicaid program, including its enrolment
broker contractor(s) as a participating provider of the Plan and your submission of encounter data
is accepted by the Florida MMIS and/or the state’s encounter data warehouse.
Protocols for submitting encounter data:
1) All Transportation providers and any provider that has services directly paid by American
Eldercare, Inc. are required to submit encounter data to AEC to reflect the authorized
services provided to our members.
2) All Transportation providers and any provider that has services directly paid by American
Eldercare, Inc. who bill AEC via paper claims (HCFA1500, UB92), or electronically
need to ensure all the required fields are completed in their submission in order for AEC
to extract the encounter data information.
3) All Transportation providers and any provider that has services directly paid by American
Eldercare, Inc. who submit claims that are not submitted in one of the above formats for
payment, are required to submit the appropriate 837i, 837p or 837d for their line of
business for encounter data purposes. (applies to PBM only)
4) Please review required fields for claims submissions in the AEC companion guide.
5) If you have any questions on what is required of your agency/company please contact
your Provider Relations Specialist or call the Provider Customer Service number at (888)
998-7735.
47 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
ASSISTED LIVING FACILITY PROVIDERS
Assisted Living Facilities are encouraged to participate in our automatic payment process. Any
provider participating in this process will be paid for existing members by the 10th
of the current
month without submitting a claim. Any existing members that were enrolled by the previous
month and have an open care plan in the current month will be paid.
Please note that if a member leaves your facility for any reason that would require American
Eldercare, Inc. to recoup money, your facility will see a debit adjustment on the following
month’s payment and/or will receive an invoice for payment.
Also note that a claim is required prior to payment for the first month that a member enters the
facility or the first month of enrollment.
All providers that do not participate in the automatic payment process must submit claims after
the end of the current month. These claims will be paid within thirty (30) days of receipt.
Room and Board Rate
Members are responsible to pay their room and board rate (as indicated in the provider’s
contract) plus patient responsibility (as determined by the Department of Children and Families).
Prorated fees will be determined for members who do not reside in the community for a full
month. AEC will be responsible for payment using the following formula:
Contracted ALF Rate minus Room & Board Rate minus Patient Responsibility = AEC Payment
These amounts will be reflected on each member‘s individual Service Requests sent by the Care
Managers. The patient responsibility is subject to change based on the Notice of Case Action
(NOCA) received by DCF or estimated member responsibility until the appropriate NOCA is
completed.
48 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
The provider is required to notify AEC within twenty-four (24) hours of a member
hospitalization or leave of absence from the community.
Bed-Hold Payments
AEC Plan will pay up to a fourteen (14) day bed-hold when our member is not in your
community except in the following occurrences:
1. Member loses Medicaid Eligibility
2. Member expires
3. Member is placed in a Skilled Nursing Facility for Long-Term Care
4. The community fails to notify AEC Plan within twenty-four (24) hours of a
hospitalization or leave of absence from the community.
5. Prorated fees will be determined for members who reside in a facility for less than a
full month.
Bed-holds OR stop payment begins the day the member leaves the facility. The facility
will not be paid for the day of discharge unless the member is eligible for a bed hold. If the
facility fails to notify AEC of a member leaving the community within (24) hours of discharge,
this will result in a forfeit of payment for the bed-hold. The facility may not charge the member
for AEC’s portion of their bill during this time.
SKILLED NURSING FACILITY PROVIDERS (SNF)
Custodial Care
All members requiring custodial care must be assessed and determination must be made by
American Eldercare, Inc. that the member can no longer live in a less restrictive setting.
Members who receive approval for placement in a contracted Skilled Nursing Facility for
custodial care are required to pay the facility a patient responsibility based on their income,
which is determined by the Department of Children and Families. Prior authorization is
required.
49 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Bed-Holds for Custodial Care Members
AEC follows the same guidelines as Medicaid. If your facility is requesting payment for a bed-
hold on an AEC member, please submit a copy of your census along with your claim for the
time-frame in question.
Custodial Care Payments
The facility will be reimbursed by AEC at the current Medicaid Per-Diem Rate established with
the State minus any patient responsibility determined by the Department and Children and
Families.
HOME HEALTH PROVIDERS
Home Health providers must attach, to all claims submitted, a form signed by the member
verifying what services were provided including date/time of service and direct care staff who
provided the service. If billing electronically, this information must be made available to
American Eldercare, Inc. “on demand.” It is recommended that services are not billed in a date
range format. Each service should be listed separately by date of service. Ranges should only be
used if billing consecutive days with the same units and amount for each day billed. If you bill
in a date range format, appropriate documentation such as time sheet or nurses notes must be
accompanied to ensure prompt and accurate payment for services rendered.
CLAIM ACKNOWLEDGEMENT
Paper Claims:
Within fifteen (15) business days after receipt of all paper claims submitted to AEC for non-
capitated services, AEC will provide the provider or designee with acknowledgement of receipt
of the claim. AEC will provide access to a web portal and allow the provider or designee to
check the status of all submitted claims. AEC will also provide provider with a provider services
telephone number to call and check the status of their submitted claims.
50 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Within fifteen (15) business days after receipt of all paper claims submitted to AEC for non-
capitated services, AEC will authorize and forward the claim to the Medicaid fiscal agent or
notify the provider or designee that the claim is contested or denied. The notification to the
provider of a contested or denied claim will include an itemized list of additional information or
documents needed to process the claim.
Electronic Claims:
Within twenty-four (24) hours after the beginning of the next business day after receipt of all
electronically submitted claims for non-capitated services, AEC will provide electronic
acknowledgment of receipt of the claim to the provider or the electronic source submitting the
claim.
Within ten (10) business days after receipt of all electronically submitted claims for non-
capitated services, AEC will authorize and forward the claim to the Medicaid fiscal agent or
notify the provider or designee that the claim is contested or denied. The notification to the
provider or designee of a contested or denied claim will include an itemized list of additional
information or documents needed to process the claim.
PAYMENTS
Payments for transportation services will be made by the Medicaid fiscal agent. Reimbursement
will be made for correct, authorized, clean claims according to the Florida Medicaid fee
schedules for reimbursement for covered services provided to enrollees. The Agency or its fiscal
agent will also reimburse non-participating providers on a FFS basis for Provider Service
Network (PSN) authorized services.

51 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
All claims payments made by American Eldercare, Inc. to a provider will be accompanied by an
explanation of payment. The explanation of payment will contain an itemized accounting of the
individual claims included in the payment including the enrollee's name, the date of service, the
procedure code, service units, the amount of reimbursement and the identification of American
Eldercare, Inc. The date of the check will also be included on the explanation of payment. The
date of the check will be considered the date of payment.
BALANCE BILLING
Payments made by or processed through American Eldercare, Inc. are in accordance with the
terms of your agreement. Providers may not balance bill members of American Eldercare, Inc.
for any covered, authorized service.
CLAIM INQUIRY
Providers are encouraged to contact the Claims Customer Service Department to inquire about
the status of a claim, status of reconsideration, or explanation of a denial. A Customer Services
Representative can be reached from 8:00am-7:00pm Monday-Friday at (561) 499-9656
Extension 1987. If you are calling during peak or after-hours, please leave a message and a
representative will return your call within one (1) business day.
CLAIM DENIALS
All denials include an explanation of denial and/or explanation of adjustment when applicable.
Denial codes are subject to change and/ additional codes utilized, please contact the claims
Customer Service Department for any questions or concerns regarding a denial or partial denial
of payment. A copy of denial codes performed by American Eldercare, Inc. and descriptions of
denial codes can be found in Section 8 of this handbook. American Eldercare will not deny
Medicare crossover claims solely based on the period between the date of service and the date of
clean claim submission, unless that period exceeds three (3) years. A copy of denial codes
performed by the Medicaid Fiscal Agent may be found in the applicable Medicaid General
Provider Reimbursement Handbook. If you disagree with a denial received, you have the right to
reconsideration.
52 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
CLAIMS RECONSIDERATION OF PAYMENT
A provider has the right to request reconsideration if they do not believe the determination on a
claim is correct. Parties not involved in the initial determination will review the reconsideration.
All reconsiderations, should be submitted in writing within sixty (60) days of the denial notice
and include any additional information needed.
Claims Reconsideration of payment should be mailed to the following address:
American Eldercare, Inc.
Attn: Claims Department (Reconsiderations)
14565 Sims Road
Delray Beach, FL 33484
FORMAL GRIEVANCES/APPEALS
A provider may file a grievance or an appeal for denial of payment on behalf of an American
Eldercare, Inc. member. Grievances are filed as complaints about services provided or about the
appeal process itself. These may be filed by the member, member representative, or a provider
on behalf of a member. The formal grievance must be submitted orally or in writing either by
letter or by completed grievance/appeal form to the Grievance/Appeal Coordinator within 365
days from the date of the event that caused your concern or grievance.
Formal Appeals are filed in response to American Eldercare, Inc.’s decision to:
Deny payment;
Deny or limit the authorization of a requested service; Or…
Reduce, suspend, or terminate a previously authorized service.
Formal appeals must be made within thirty (30) days of written notice of American Eldercare
Inc.’s decision to reduce, deny services, or payments. Appeals may be made orally or in writing.
Oral appeals must be followed up with a signed, written appeal.
American Eldercare, Inc. considers the member or member’s representative as parties to an
appeal or a grievance. We encourage them to explore the informal complaint process first in an
53 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
attempt to work out the issue directly with the Care Manager and/or their supervisor. If the
concern or complaint was not resolved satisfactorily with the Care Manager, a grievance or
appeal may be filed with American Eldercare, Inc.
Grievance/Appeal Coordinator located address:
American Eldercare, Inc. Plan
Attn: Grievance/Appeal Coordinator
14565 Sims Road
Delray Beach, Florida 33484
Toll Free (866) 352-1192
If the member or representative wish to write a letter to the Grievance/Appeal Coordinator
addressing the concern, the letter should include the member’s name, address, member ID
number, date, and signature. The Care Manager is available to assist with this process if needed.
If the member or representative prefers to call the Grievance/Appeal Coordinator, office hours
are 9:00 a.m. – 5:00 p.m. Eastern Standard Time, Monday – Friday. Telephone messages are
forwarded twenty-four (24) hours a day. The Grievance/Appeal Coordinator will return the
phone call, provide the member or representative with a complete explanation of our procedures,
and mail a grievance/appeal form within three (3) working days. The immediate member or
representative will need to complete this grievance form and mail it back to the
Grievance/Appeal Coordinator at the address provided above.
Upon oral receipt of the grievance or completed grievance form, the Grievance/Appeal
Coordinator will have the concern investigated and a written decision will be mailed to the
member within ninety (90) days.
Upon oral receipt of the appeal (followed by a signed written copy), the Grievance/Appeal
Coordinator will have the concern investigated and a written decision will be mailed to the
member within forty-five (45) days. The person(s) who originally made the decision to reduce
or deny services will not be a decision maker in the determination process.
To request a complete description of American Eldercare, Inc. Plan’s Grievance /Appeals
Procedure, you may call our corporate office toll free at (866) 352-1192.
54 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Expedited Appeals
If the request is deemed urgent by American Eldercare, Inc., an expedited review will take place.
This process can only be utilized if an AEC member is being denied access to services. The
person(s) who originally made the decision to reduce or deny services will not be a decision
maker in the determination process.
Within seventy-two (72) hours (or sooner, if warranted) of the receipt of the request, a decision
will be determined and the member or representative will be notified by phone. The final
determination will be sent to the member in writing.
American Eldercare, Inc. will continue the member’s benefits if:
The appeal is filed timely, meaning on or before the later of the following:
Within ten (10) days of the date on the notice of action (or fifteen (15) days of the notice
is sent via U.S. mail).
The intended effective date of Plan’s proposed action.
The appeal involves the termination, suspension, or reduction of a previously authorized
course of treatment.
The services were ordered by an authorized provider.
The authorization period has not expired.
The member requests extension of benefits.
At the conclusion of the appeal process, in the event of a ruling in favor of American Eldercare,
Inc. the member may have to pay for those services rendered during the appeal process.
Beneficiary Assistance Program
In the event you have received a notice of resolution after your American Eldercare, Inc. internal
appeal, you may request review of that decision within one (1) year by the Beneficiary
Assistance Program. You may not request the review if you have already requested a Medicaid
Fair Hearing. The program is operated by AHCA and may be contacted at:
55 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Agency for Health Care Administration
Beneficiary Assistance Program Building 1, MS
#26
2727 Mahan Drive
Tallahassee, Florida 32308
(850) 412-4502
(888) 419-3456 (toll-free)
Unresolved Grievances/Appeals – Medicaid Fair Hearing
To appeal the decision made by American Eldercare, Inc. Plan’s Grievance/Appeal Committee in
response to their grievance/appeal, the member or their representative may request a Medicaid
Fair Hearing within ninety (90) days from the notice of resolution. An enrollee who chooses to
seek a Medicaid Fair Hearing without pursuing the Managed Care Plan’s process must do so
within ninety (90) days of receipt of the Managed Care Plan’s notice of action.
The member or member representative must contact:
Office of Public Assistance Appeals Hearing
1317 Winewood Boulevard
Building 5, Room 203
Tallahassee, FL 32399-0700
(850) 488-1429
In the event a member or provider wishes to contact the Agency for Health Care Administration,
you can call the State-Wide Consumer Center at (888) 419-3456.
IMPORTANT INFORMATION REGARDING GRIEVANCES/APPEALS
1. Continuation of Benefits
a. American Eldercare, Inc. shall continue the enrollee’s benefits if:
(1) The enrollee or the enrollee’s authorized representative files an appeal with the
American Eldercare, Inc. regarding American Eldercare, Inc.’s decision:
(a) Within ten (10) business days after the notice of the adverse action is mailed;
or
56 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
(b) Within ten (10) business days after the intended effective date of the action,
whichever is later.
(2) The appeal involves the termination, suspension or reduction of a previously
authorized course of treatment;
(3) The services were ordered by an authorized provider;
(4) The original period covered by the original authorization has not expired; and
(5) The enrollee requests extension of benefits.
b. If, at the enrollee’s request, American Eldercare, Inc. continues or reinstates the
benefits while the appeal is pending, benefits must continue until one (1) of the
following occurs:
(1) The enrollee withdraws the appeal;
(2) Ten (10) business days pass after American Eldercare, Inc. sends the enrollee the
notice of resolution of the appeal against the enrollee, unless the enrollee within
those ten (10) days has requested a Medicaid Fair Hearing with continuation of
benefits;
(3) The Medicaid Fair Hearing office issues a hearing decision adverse to the
enrollee; or
(4) The time period or service limits of a previously authorized service have been
met.
c. If the final resolution of the appeal is adverse to the enrollee and American Eldercare,
Inc.’s action is upheld, American Eldercare, Inc. may recover the cost of services
furnished to the enrollee while the appeal was pending to the extent they were
furnished solely because of the continuation of benefits requirement.
d. If the Medicaid Fair Hearing officer reverses American Eldercare, Inc.’s action and
services were not furnished while the appeal was pending, the American Eldercare,
Inc. shall authorize or provide the disputed services promptly.
e. If the Medicaid Fair Hearing officer reverses American Eldercare, Inc.’s action and
the enrollee received the disputed services while the appeal was pending, American
Eldercare, Inc. shall pay for those services in accordance with this Contract.
________________________________________________

57 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
7
FORMS
Authorization Forms:
Change of Services Request
Hold/Resume Service Request
Request for New Services
Termination of Services Request
Claim Forms:
CMS 1500
UB-04
Provider Complaint Form
Provider Change of Notice Form
58 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
_________________________________________________
8
APPENDIX
AEC Locations
CARES Offices
Denial Codes
Remittance Advice
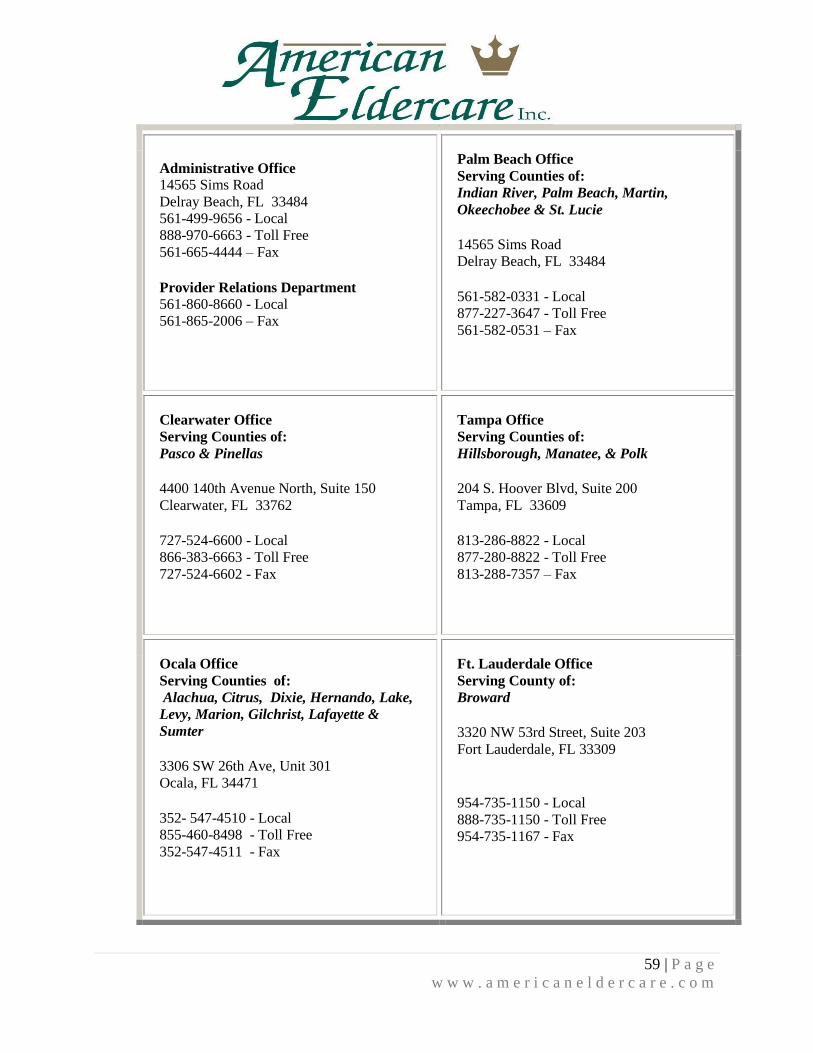
59 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Administrative Office 14565 Sims Road
Delray Beach, FL 33484 561-499-9656 - Local
888-970-6663 - Toll Free
561-665-4444 – Fax
Provider Relations Department 561-860-8660 - Local 561-865-2006 – Fax
Palm Beach Office Serving Counties of:
Indian River, Palm Beach, Martin,
Okeechobee & St. Lucie 14565 Sims Road Delray Beach, FL 33484 561-582-0331 - Local
877-227-3647 - Toll Free
561-582-0531 – Fax
Clearwater Office Serving Counties of:
Pasco & Pinellas 4400 140th Avenue North, Suite 150
Clearwater, FL 33762 727-524-6600 - Local
866-383-6663 - Toll Free
727-524-6602 - Fax
Tampa Office Serving Counties of: Hillsborough, Manatee, & Polk 204 S. Hoover Blvd, Suite 200 Tampa, FL 33609 813-286-8822 - Local
877-280-8822 - Toll Free
813-288-7357 – Fax
Ocala Office Serving Counties of:
Alachua, Citrus, Dixie, Hernando, Lake,
Levy, Marion, Gilchrist, Lafayette &
Sumter 3306 SW 26th Ave, Unit 301 Ocala, FL 34471 352- 547-4510 - Local 855-460-8498 - Toll Free
352-547-4511 - Fax
Ft. Lauderdale Office Serving County of:
Broward 3320 NW 53rd Street, Suite 203 Fort Lauderdale, FL 33309
954-735-1150 - Local
888-735-1150 - Toll Free
954-735-1167 - Fax
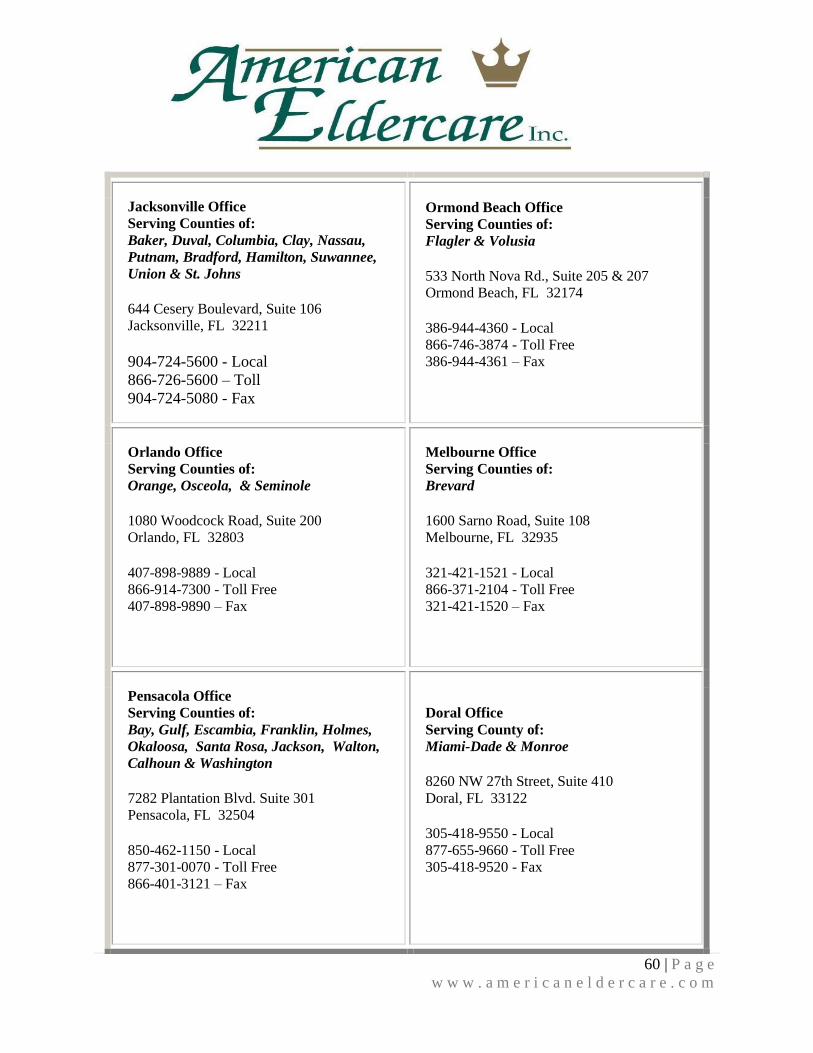
60 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Jacksonville Office Serving Counties of:
Baker, Duval, Columbia, Clay, Nassau,
Putnam, Bradford, Hamilton, Suwannee,
Union & St. Johns 644 Cesery Boulevard, Suite 106
Jacksonville, FL 32211
904-724-5600 - Local
866-726-5600 – Toll
904-724-5080 - Fax
Ormond Beach Office Serving Counties of: Flagler & Volusia 533 North Nova Rd., Suite 205 & 207
Ormond Beach, FL 32174 386-944-4360 - Local
866-746-3874 - Toll Free
386-944-4361 – Fax
Orlando Office Serving Counties of: Orange, Osceola, & Seminole 1080 Woodcock Road, Suite 200
Orlando, FL 32803 407-898-9889 - Local
866-914-7300 - Toll Free
407-898-9890 – Fax
Melbourne Office Serving Counties of: Brevard 1600 Sarno Road, Suite 108
Melbourne, FL 32935 321-421-1521 - Local
866-371-2104 - Toll Free
321-421-1520 – Fax
Pensacola Office Serving Counties of: Bay, Gulf, Escambia, Franklin, Holmes,
Okaloosa, Santa Rosa, Jackson, Walton,
Calhoun & Washington 7282 Plantation Blvd. Suite 301
Pensacola, FL 32504 850-462-1150 - Local
877-301-0070 - Toll Free 866-401-3121 – Fax
Doral Office Serving County of:
Miami-Dade & Monroe 8260 NW 27th Street, Suite 410
Doral, FL 33122 305-418-9550 - Local
877-655-9660 - Toll Free
305-418-9520 - Fax
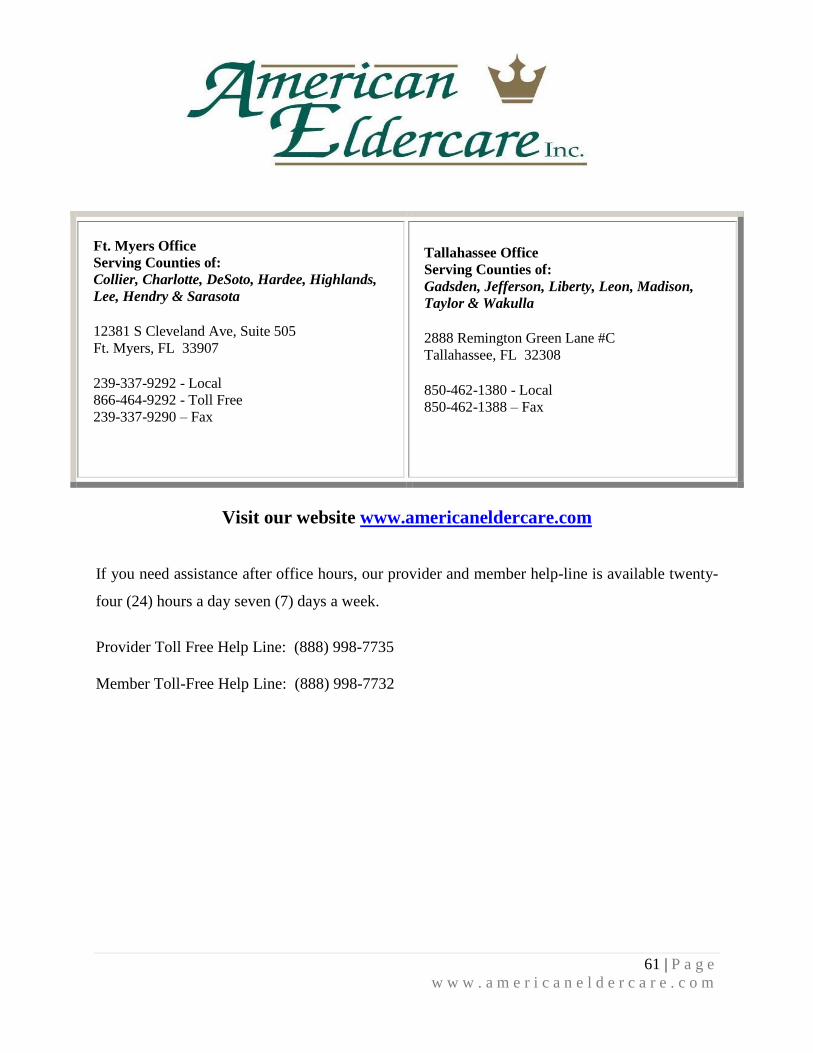
61 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Visit our website www.americaneldercare.com
If you need assistance after office hours, our provider and member help-line is available twenty-
four (24) hours a day seven (7) days a week.
Provider Toll Free Help Line: (888) 998-7735
Member Toll-Free Help Line: (888) 998-7732
Ft. Myers Office Serving Counties of: Collier, Charlotte, DeSoto, Hardee, Highlands,
Lee, Hendry & Sarasota 12381 S Cleveland Ave, Suite 505
Ft. Myers, FL 33907 239-337-9292 - Local
866-464-9292 - Toll Free
239-337-9290 – Fax
Tallahassee Office Serving Counties of: Gadsden, Jefferson, Liberty, Leon, Madison,
Taylor & Wakulla 2888 Remington Green Lane #C
Tallahassee, FL 32308 850-462-1380 - Local
850-462-1388 – Fax
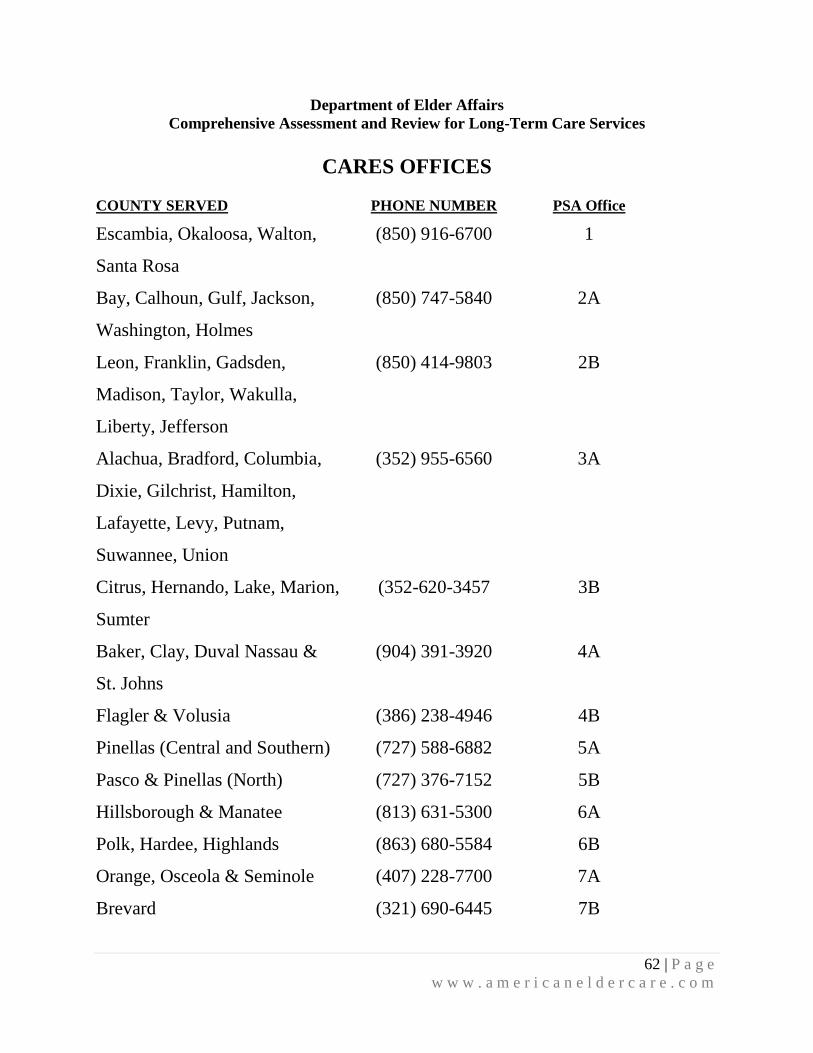
62 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Department of Elder Affairs
Comprehensive Assessment and Review for Long-Term Care Services
CARES OFFICES
COUNTY SERVED PHONE NUMBER PSA Office
Escambia, Okaloosa, Walton,
Santa Rosa
(850) 916-6700 1
Bay, Calhoun, Gulf, Jackson,
Washington, Holmes
(850) 747-5840 2A
Leon, Franklin, Gadsden,
Madison, Taylor, Wakulla,
Liberty, Jefferson
(850) 414-9803 2B
Alachua, Bradford, Columbia,
Dixie, Gilchrist, Hamilton,
Lafayette, Levy, Putnam,
Suwannee, Union
(352) 955-6560 3A
Citrus, Hernando, Lake, Marion,
Sumter
(352-620-3457 3B
Baker, Clay, Duval Nassau &
St. Johns
(904) 391-3920 4A
Flagler & Volusia (386) 238-4946 4B
Pinellas (Central and Southern) (727) 588-6882 5A
Pasco & Pinellas (North) (727) 376-7152 5B
Hillsborough & Manatee (813) 631-5300 6A
Polk, Hardee, Highlands (863) 680-5584 6B
Orange, Osceola & Seminole (407) 228-7700 7A
Brevard (321) 690-6445 7B
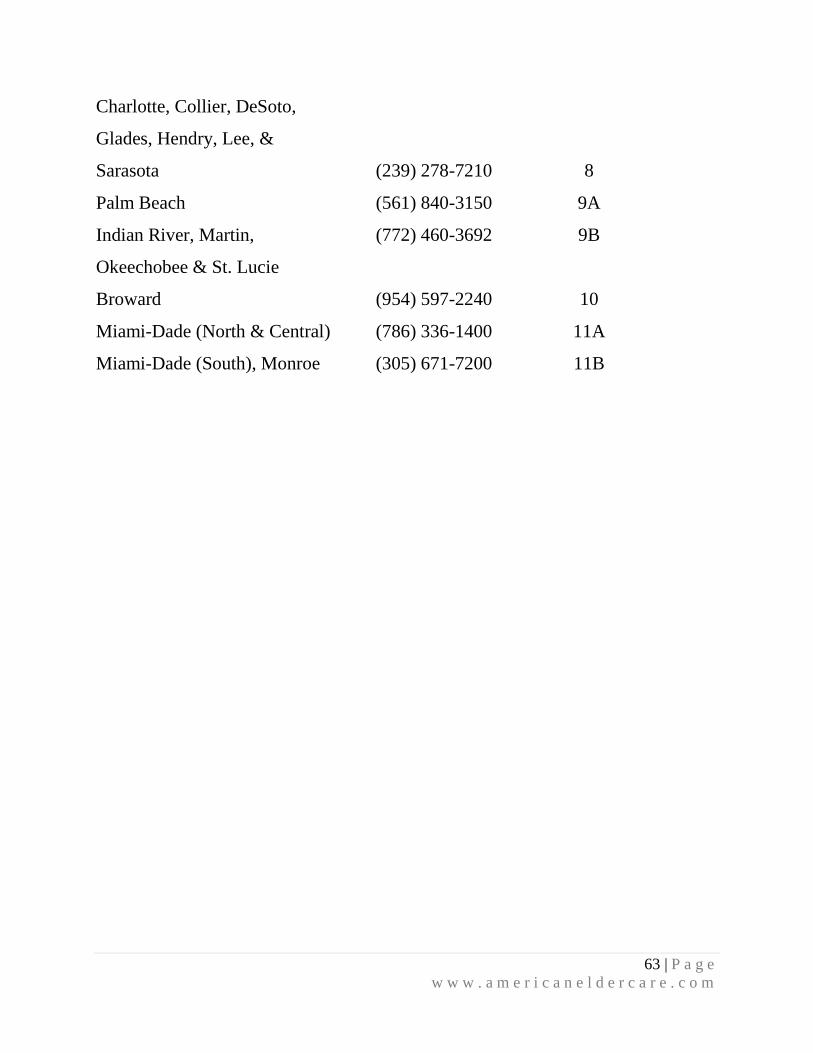
63 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Charlotte, Collier, DeSoto,
Glades, Hendry, Lee, &
Sarasota
(239) 278-7210
8
Palm Beach (561) 840-3150 9A
Indian River, Martin,
Okeechobee & St. Lucie
(772) 460-3692 9B
Broward (954) 597-2240 10
Miami-Dade (North & Central) (786) 336-1400 11A
Miami-Dade (South), Monroe (305) 671-7200 11B
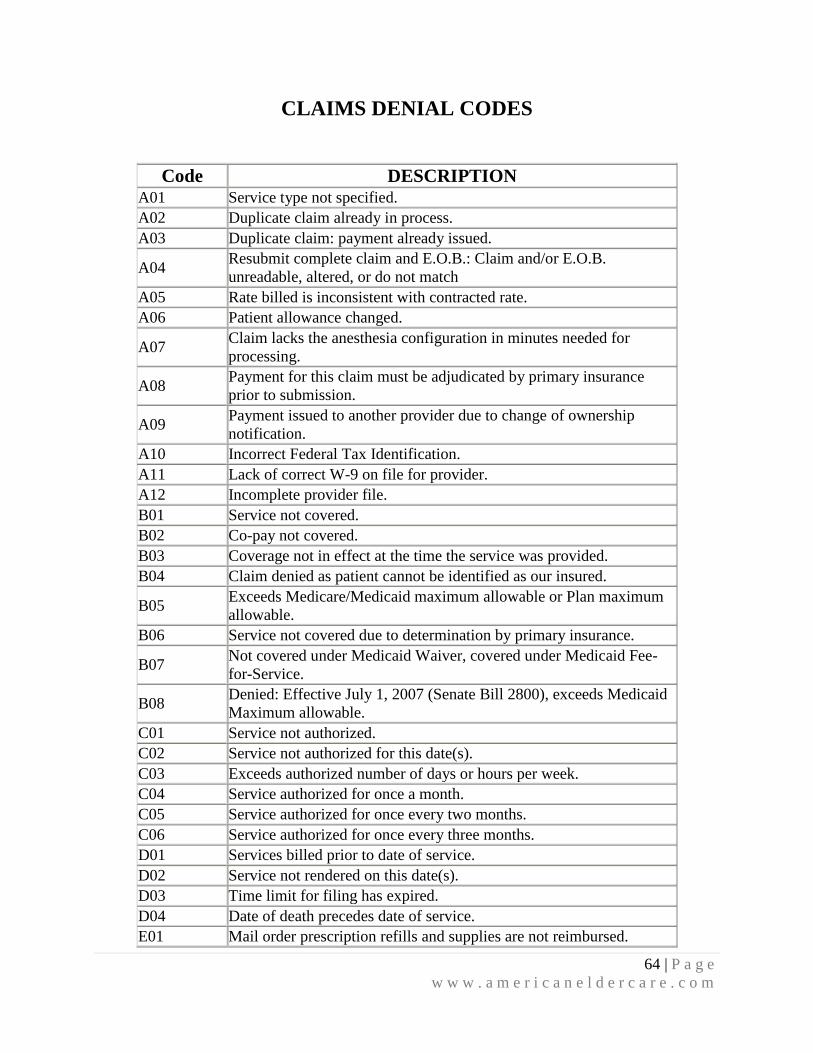
64 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
CLAIMS DENIAL CODES
Code DESCRIPTION A01 Service type not specified.
A02 Duplicate claim already in process.
A03 Duplicate claim: payment already issued.
A04 Resubmit complete claim and E.O.B.: Claim and/or E.O.B.
unreadable, altered, or do not match
A05 Rate billed is inconsistent with contracted rate.
A06 Patient allowance changed.
A07 Claim lacks the anesthesia configuration in minutes needed for
processing.
A08 Payment for this claim must be adjudicated by primary insurance
prior to submission.
A09 Payment issued to another provider due to change of ownership
notification.
A10 Incorrect Federal Tax Identification.
A11 Lack of correct W-9 on file for provider.
A12 Incomplete provider file.
B01 Service not covered.
B02 Co-pay not covered.
B03 Coverage not in effect at the time the service was provided.
B04 Claim denied as patient cannot be identified as our insured.
B05 Exceeds Medicare/Medicaid maximum allowable or Plan maximum
allowable.
B06 Service not covered due to determination by primary insurance.
B07 Not covered under Medicaid Waiver, covered under Medicaid Fee-
for-Service.
B08 Denied: Effective July 1, 2007 (Senate Bill 2800), exceeds Medicaid
Maximum allowable.
C01 Service not authorized.
C02 Service not authorized for this date(s).
C03 Exceeds authorized number of days or hours per week.
C04 Service authorized for once a month.
C05 Service authorized for once every two months.
C06 Service authorized for once every three months.
D01 Services billed prior to date of service.
D02 Service not rendered on this date(s).
D03 Time limit for filing has expired.
D04 Date of death precedes date of service.
E01 Mail order prescription refills and supplies are not reimbursed.
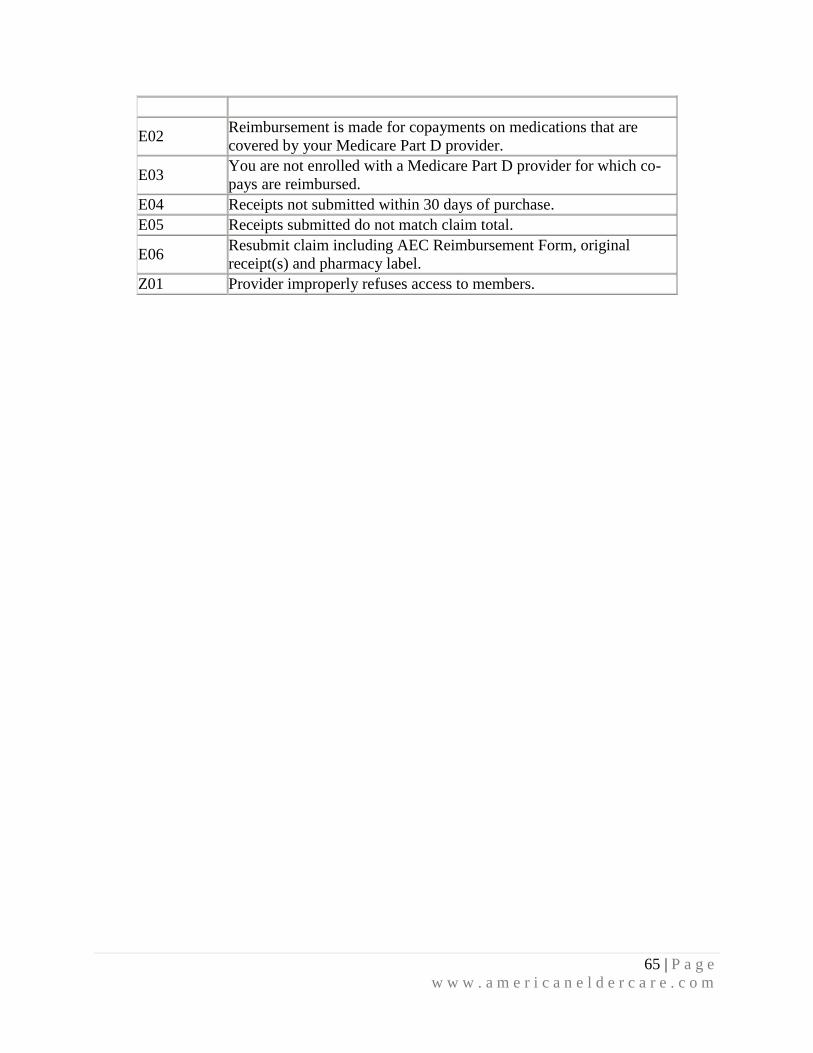
65 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
E02 Reimbursement is made for copayments on medications that are
covered by your Medicare Part D provider.
E03 You are not enrolled with a Medicare Part D provider for which co-
pays are reimbursed.
E04 Receipts not submitted within 30 days of purchase.
E05 Receipts submitted do not match claim total.
E06 Resubmit claim including AEC Reimbursement Form, original
receipt(s) and pharmacy label.
Z01 Provider improperly refuses access to members.
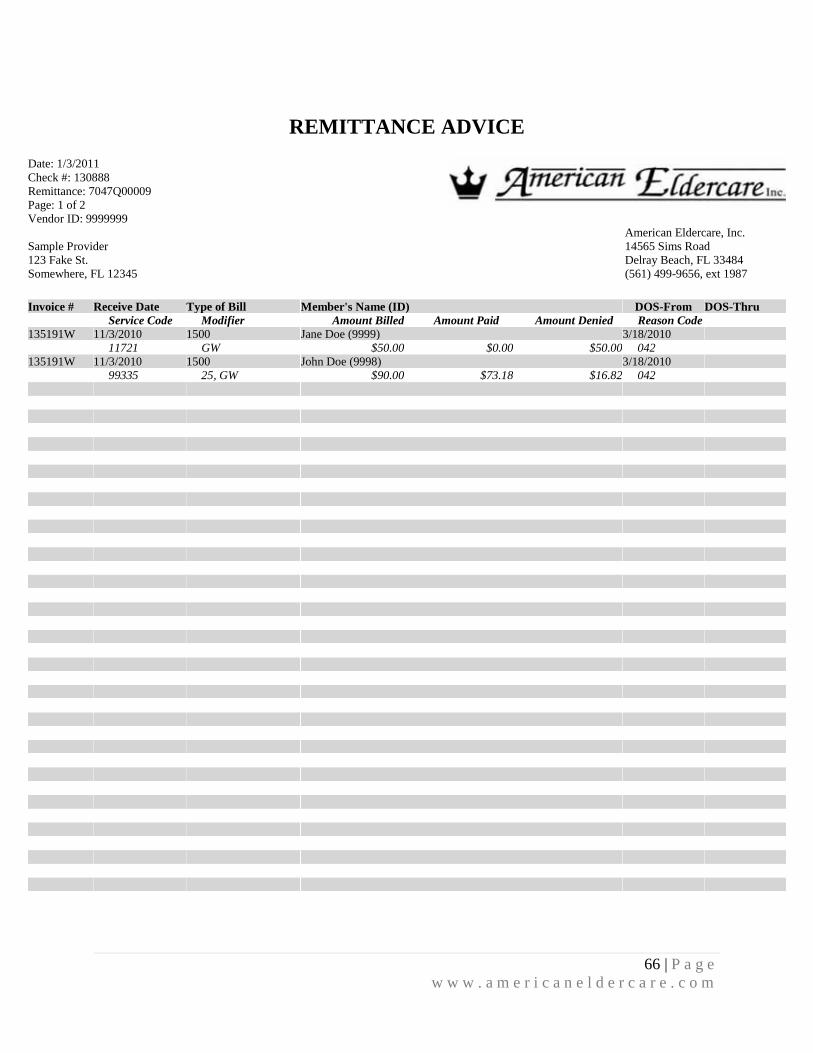
66 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
REMITTANCE ADVICE
Date: 1/3/2011
Check #: 130888
Remittance: 7047Q00009
Page: 1 of 2
Vendor ID: 9999999
Sample Provider
123 Fake St.
Somewhere, FL 12345
American Eldercare, Inc.
14565 Sims Road
Delray Beach, FL 33484
(561) 499-9656, ext 1987
Invoice # Receive Date Type of Bill Member's Name (ID) DOS-From DOS-Thru
Service Code Modifier Amount Billed Amount Paid Amount Denied Reason Code
135191W 11/3/2010 1500 Jane Doe (9999) 3/18/2010
11721 GW $50.00 $0.00 $50.00 042
135191W 11/3/2010 1500 John Doe (9998) 3/18/2010
99335 25, GW $90.00 $73.18 $16.82 042
67 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Right of Reconsideration - If you believe the determination on this claim is incorrect, you have the right to request a reconsideration. The reconsideration will be reviewed by parties not involved in the initial determination. In order to
request a reconsideration, you must submit your request in writing within 60 days of this notice. Once you have completed the request, you should mail it to the Claims Department.
CONFIDENTIALITY NOTICE: This Remittance Advice is intended only for the use of the individual or entity to which it is addressed and may contain information that is privileged, confidential and exempt from disclosure under
applicable law. Any unauthorized review, use, disclosure, or distribution is prohibited. If you have received this document in error, please do not distribute it. Please notify the sender by the United States Postal Service at the address
shown above. Date: 1/3/2011
Check #: 130888
Remittance: 7047Q00009
Page: 2 of 2
Vendor ID: 9999999
Sample Provider
123 Fake St.
Somewhere, FL 12345
American Eldercare, Inc.
14565 Sims Road
Delray Beach, FL 33484
(561) 499-9656, ext 1987
Reason Codes
042: Charges exceed Medicaid maximum allowable amount.
68 | P a g e
w w w . a m e r i c a n e l d e r c a r e . c o m
Corporate office:
American Eldercare, Inc.
14565 Sims Road
Delray Beach, FL 33484
Approved 5/17/13
08/01/13

















