
Provider Care Primary Partners Care The Learn: Lunch Care Love Lunch and... · Care Partners...
7
Care Partners Primary Care Provider Lunch & Learn: Why PCPs Love Collaborative Care Presenter: Wayne Bentham, MD • The advantage of the collaborative care model of depression management in primary care is leveraging the skills of a wellͲtrained depression care manager, with the clinical expertise of a PCP , to coordinate care, follow outcomes, and make sure patients are responding to treatment. 2 Objectives By the end of the session, participants will be able to: • Understand the rationale for treating depression in primary care using a team approach • Talk to patients about depression and Collaborative Care in the context of a 15Ͳminute appointment • Communicate and collaborate within the care team 3 1990 1 Lower respiratory infection 2 Conditions arising during the perinatal period 3 Diarrheal diseases 4 Unipolar major depression 5 Ischemic heart disease 6 Vaccine-preventable disease 2020 1 Unipolar major depression 2 Ischemic heart disease 3 Road traffic accidents 4 Cerebro-vascular disease 5 Chronic obstructive pulmonary disease 6 Lower respiratory infections Murray & Lopez, WHO: Global Burden of Disease, 1996; Michaud, JAMA, 2001 GLOBAL BURDEN OF DISEASE: WORLD HEALTH ORGANIZATION 4 Making a Diagnosis Symptoms Functional Impairment Disorder UnderͲRecognition/ Undertreatment • Only 29% of persons with depression reported contacting a mental health professional in the past year* • 30%Ͳ70% of depression missed by PCPs • 50% stop medication within 3 months • 50% of treated patients in primary care remain depressed after 1 year *NHANES, 2005-6 6 Why PCPs Love Collaborative Care 10/19/2016 1
Transcript of Provider Care Primary Partners Care The Learn: Lunch Care Love Lunch and... · Care Partners...
Care Partners Primary Care ProviderLunch & Learn:
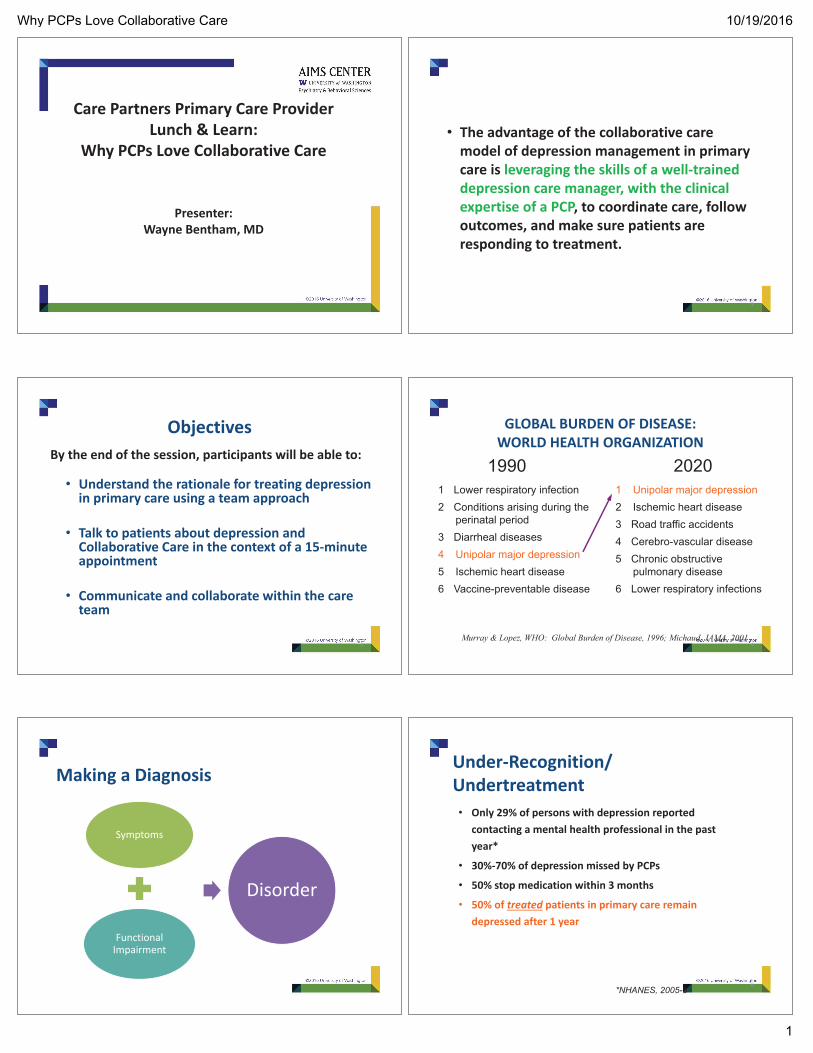
Why PCPs Love Collaborative Care
Presenter:Wayne Bentham, MD
• The advantage of the collaborative caremodel of depression management in primarycare is leveraging the skills of a well traineddepression care manager, with the clinicalexpertise of a PCP, to coordinate care, followoutcomes, and make sure patients areresponding to treatment.
2
ObjectivesBy the end of the session, participants will be able to:
• Understand the rationale for treating depressionin primary care using a team approach
• Talk to patients about depression andCollaborative Care in the context of a 15 minuteappointment
• Communicate and collaborate within the careteam
3
1990 1 Lower respiratory infection2 Conditions arising during the
perinatal period3 Diarrheal diseases4 Unipolar major depression5 Ischemic heart disease6 Vaccine-preventable disease
20201 Unipolar major depression2 Ischemic heart disease3 Road traffic accidents4 Cerebro-vascular disease5 Chronic obstructive
pulmonary disease6 Lower respiratory infections
Murray & Lopez, WHO: Global Burden of Disease, 1996; Michaud, JAMA, 2001
GLOBAL BURDEN OF DISEASE:WORLD HEALTH ORGANIZATION
4
Making a Diagnosis
Symptoms
FunctionalImpairment
Disorder
Under Recognition/Undertreatment• Only 29% of persons with depression reported
contacting a mental health professional in the pastyear*
• 30% 70% of depression missed by PCPs
• 50% stop medication within 3 months
• 50% of treated patients in primary care remaindepressed after 1 year
*NHANES, 2005-66
Why PCPs Love Collaborative Care 10/19/2016
1

Depression is Associated with. . .
• Smoking• Overweight• Poor Glycemic Control• Decreased Medication Adherence• Increased hospitalizations• Increased Costs• Suicide
7
Cycle of Depression
How many of these people with mental healthconcerns will see a mental health provider?
No Treatment Primary Care Provider
Mental Health Provider
Wang P, et al., Twelve-Month Use of Mental Health Servicesin the United States, Arch Gen Psychiatry, 62, June 2005
A PCP from Family Health Centers of San Diegoposed the following scenario:• A patient comes into my exam room complaining ofhip pain, even though the appointment wassupposed to be about her diabetes. On top of that, Ireviewed the PHQ 9 she just filled out and her scoreis 18. How am I supposed to prioritize my limitedtime with this patient? How would I fit a review ofthe PHQ 9, a discussion about depression, and awarm handoff/connection into this appointment?
10
Other questions you may have:
• What exactly is collaborative care fordepression?
• Why am I being asked to do this?• Who is this depression care manager that Ikeep hearing about?
• Why can’t I use the psychiatrist I have? Whycan’t we hire another psychiatrist?
11 12
The Evidence
Why PCPs Love Collaborative Care 10/19/2016
2

PCP
Patient
Usual Care
13
Introducing the Collaborative Care Model & Team
PCP oversees all aspects of patient’s care.Introduces collaborative care teamDiagnoses common mental disordersStarts & prescribes pharmacotherapyMakes treatment adjustment in consultation with team
PCP
Patient CareManager
PsychiatricConsultant
Psychotherapist
CoreProgram
Additional ClinicResources
14
Twice as Many People Improve
Percen
t(%)Improvem
ent
Participating Organizations
50 % or greater improvement in depression at 12 months
Unützer et al., JAMA 2002; Psych Clinics North America 2004
0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8
Usual Care IMPACT
US Preventive Services Task ForceRecommendation
• Screening adults for depression when staffassisted depression care supports are in placeto assure accurate diagnosis, effectivetreatment, and follow up.
Grade: B recommendation
16
17
The Care Model
Introducing the Collaborative Care Model & Team
PCP oversees all aspects of patient’s care.Introduces collaborative care teamDiagnoses common mental disordersStarts & prescribes pharmacotherapyMakes treatment adjustment in consultation with team
PCP
Patient CareManager
PsychiatricConsultant
Psychotherapist
CoreProgram
Additional ClinicResources
18
Why PCPs Love Collaborative Care 10/19/2016
3

What do the care managers do?
• Take an in depth mental health history• Provide psycho education• Provide brief, evidence based interventionslike Problem Solving Treatment andBehavioral Activation
• Medication adherence monitoring• Follow up with patients• Do relapse prevention planning
19
Care Manager Tasks
• Facilitates patient engagement and education• Works closely with PCP to manage caseload of allpatients engaged in active treatment
• Performs systematic initial and follow up contacts• Assists PCP and Psych Consultant with clinicalassessment and differential diagnosis (Therapist)
• Systematically tracks treatment response• Cues team to change treatment when indicated
Care Manager Tasks
• Supports medication management by PCP• Provides brief, structured evidence based therapy(Therapist)
• Reviews challenging patients with the psychiatricconsultant weekly
• Facilitates referral to other services as needed andavailable– Internal and/or external referral
• Completes relapse prevention with patient
Role for Care Manager in MedicationTreatment
• Time• Different relationship
Opportunity
• Engaging• Assessing / collecting information• Supporting
Skills
• The advantage of the collaborative caremodel of depression management in primarycare is leveraging the skills of a well traineddepression care manager, with the clinicalexpertise of a PCP, to coordinate care, followoutcomes, and make sure patients areresponding to treatment.
23
Comparison of Contacts inUsual Care vs. IMPACT
USUAL CARE3.5 PCP Contacts per year
Based on HRSA report of average PCP visit rates for FQHCs
20% 40% treatment response/improvement
12 months0
Why PCPs Love Collaborative Care 10/19/2016
4

Comparison of Contacts inUsual Care vs. IMPACT
Collaborative Care• 3.5 PCP Contacts per year• 10 contacts with CM (on average)• 2 case consultations from psychiatric
consultant to CM/PCP (on average)
50% - 70% treatment response/improvement
12 months0
Follow Up Contacts• Weekly or every other week during acutetreatment phase– In person or by telephone to evaluate symptomseverity (PHQ 9, GAD 7) and treatment response
• Initial focus on– Adherence to medications– Side effects– Follow up on activation and PST plans
• Later focus on– Complete resolution of symptoms andrestoration of functioning
– Long term treatment adherence
Common Measures
• Depression: PHQ 9
The “PHQ9” is like the “A1C” of Depression
DepressionPHQ9
DiabetesA1C
28
Engaging Patients in the Model in 15minutes• The Provider’s Role
– Reviewing the PHQ 9– Introducing Collaborative Care to the patient– Warm Handoffs/Connections– Follow up of on going care
29
Warm Connections (Hand offs):personal introductions emphasize teambased care.
“Please let me introduceour care manager Mary.
We work as a team to helpyou manage your mood”
30
Why PCPs Love Collaborative Care 10/19/2016
5

Model Introduction• “We provide mental health care as a team at this clinic.”• “You will be cared for by a team.”
– PCP will still be your medical provider– A care manager to help improve your day to day function– A psychiatric consultant works “behind the scenes” to make sure we
offer you the best treatment options possible– Other team members
• “We communicate about your care.”• “When you are working with one team member you are
working with whole team.”• “I want to set up an appointment for you to meet her/him
OR introduce you to her/him right now.”• “If you have any concerns or doubts about the program, call
me to discuss them.”
31
Cycle of Depression
Typical Duration of Care Management
• 6 Months (average)• Best if determined by clinical outcomes,not preset– 50% 70% of patients need at least one change intreatment to improve
– Only 30% 50% patients respond fully to 1sttreatment
– Each change of Tx moves an additional ~20% ofpatients into response or remission
A PCP from Family Health Centers of San Diegoposed the following scenario:• A patient comes into my exam room complaining ofhip pain, even though the appointment wassupposed to be about her diabetes. On top of that, Ireviewed the PHQ 9 she just filled out and her scoreis 18. How am I supposed to prioritize my limitedtime with this patient? How would I fit a review ofthe PHQ 9, a discussion about depression, and awarm handoff/connection into this appointment?
34
So, to summarize:
• Screen patients for depression• Make discussion of screening results a priority• Have a plan for introducing your care managerto your patient
• Your care manager is your friend!!• Have a plan for your care manager to follow upwith you
• Schedule follow up appointments to specificallyaddress depression treatment
35
Principles
Evidence Based Care. Providers use treatments that have researchevidence for effectiveness.
Population Based Care. A defined group of clients is tracked in aregistry so that no one falls through the cracks.
Treatment to Target. Progress is measured regularly and treatmentsare actively changed until clinical goals are achieved.
Patient Centered Collaboration. Primary care and mental healthproviders collaborate effectively using shared care plans.
Accountable Care. Providers are accountable and reimbursed forquality of care and clinical outcomes, not just volume of care.
Why PCPs Love Collaborative Care 10/19/2016
6

37
Opportunities!!
Questions?
• Thoughts?• Ideas?
39
Discussion
• What else would be helpful for you?
40
Why PCPs Love Collaborative Care 10/19/2016
7


















