PROUD: Results and participant experiences Presented by Mitzy Gafos, behalf of the PROUD team
17
PROUD: Results and participant experiences Presented by Mitzy Gafos, behalf of the PROUD team http://www.proud.mrc.ac.uk/
-
Upload
brandon-caldwell -
Category
Documents
-
view
221 -
download
0
description
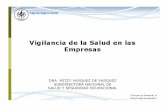
PROUD Pilot GMSM reporting condomless anal sex last/next 90days; 18+; and willing to take a pill every day Risk reduction includes Truvada AFTER 12M Randomize HIV negative MSM (exclude if treatment for HBV/Truvada contra-indicated) Main endpoints in Pilot: recruitment and retention From April 2014: HIV infection in first 12 months Follow 3 monthly for up to 24 months Risk reduction includes Truvada NOW
Transcript of PROUD: Results and participant experiences Presented by Mitzy Gafos, behalf of the PROUD team

PROUD: Results and participant experiences
Presented by Mitzy Gafos, behalf of the PROUD team
http://www.proud.mrc.ac.uk/

Clinical trial evidence for oral PrEP Effect size (CI)
iPrEx: daily Truvada(MSM - America’s, Thailand, South Africa)
44% (15; 63)
TDF2: daily Truvada(Heterosexuals men and women- Botswana) 62% (22; 84)
Partners PrEP: daily Truvada(Discordant couples – Kenya, Uganda)
75% (55; 87)
Partners PrEP: daily Tenofovir(Discordant couples – Kenya, Uganda)
67% (44; 81)
FEMPrEP: daily Truvada(Women – Kenya, South Africa, Tanzania)
6% (-52; 41)
MTN003/VOICE: daily Truvada(Women – South Africa, Uganda, Zimbabwe)
-4% (-49; 27)
Bangkok Tenofovir Study: daily Tenofovir(IDUs– Thailand)
49% (10; 72)
MTN003/VOICE: daily Tenofovir(Women - South Africa, Uganda, Zimbabwe)
-49% (-129; 3)
Effectiveness (%)Source: Adapted from Abdool Karim SS. Lancet 2013

PROUD PilotGMSM reporting condomless anal sex last/next 90days;
18+; and willing to take a pill every day
Risk reduction includes Truvada AFTER 12M
Randomize HIV negative MSM(exclude if treatment for HBV/Truvada contra-indicated)
Main endpoints in Pilot: recruitment and retentionFrom April 2014: HIV infection in first 12 months
Follow 3 monthly for up to 24 months
Risk reduction includes Truvada NOW

HIV IncidenceGroup No. of
infectionsFollow-up
(PY)Incidence
(per 100 PY)90% CI
Overall 23 465.6 4.9 3.4–6.8
Immediate 3 243.5 1.2 0.4–2.9
Deferred 20 222.1 9.0 6.1–12.8Effectiveness =86% (90% CI: 64 – 96%)P value =0.0001
Rate Difference =7.8 (90% CI: 4.3 – 11.3)Number Needed to Treat =13 (90% CI: 9 – 23)
*174 courses of PEP for 85(31%) deferred

0
10
20
30
40
Per
cent
age
0 1 2-4 5-9 10-19 20+
All partners
0
10
20
30
40
Per
cent
age
0 1 2-4 5-9 10-19 20+
All partners
0
10
20
30
40
Per
cent
age
0 1 2-4 5-9 10-19 20+
Participant receptive, no condom
0
10
20
30
40
Per
cent
age
0 1 2-4 5-9 10-19 20+
Participant receptive, no condom
Baseline 12 months
Immediate Deferred
P=0.47
P=0.04
Sexual Behaviour

STIs
Any STI
Gonorrh
oea
Chlamydi
a
Syphili
s
Rectal G
C/CT0
10
20
30
40
50
60 p=0.08
p=0.44
p=0.08
p=0.32
p=0.44
ImmediateDeferred
CaveatNumber of screens differed between the groups:
e.g. Rectal gonorrhoea/chlamydia 974 in the IMM group and 749 in the DEF
Adjusted OR=1.00, p=0.99

PROUD: In-depth Interviews
Immediate11
Deferred14
Increased risk behaviour
HIGH ADHERENCE
6
Same risk behaviour
HIGH ADHERENCE
3
Increased risk behaviour
7
Increased risk behaviour
LOW ADHERENCE
1
Same risk behaviour
LOW ADHERENCE
0
Same risk behaviour
5
SPECIAL
1
SPECIAL
2
Purposeful Sampling: Risk-adherence matrix

Condom realities
Condom use
PleasureErectionIntimacySobriety
Risk taking
Never Sometimes Want not to with partner
Attempt to
“I am not going to
not bareback" “I felt like I was
holding the lid on a boiling pot of water so hard
that I just couldn’t hold it
any more”
“It was a form of self harm I would
say”
“If I thought someone was generally
reckless then I would be
somewhat wary about doing anything"
“I’ve never reached organism inside of
one which is an unbelievably
frustrating thing”
“It is an absolutely
terrifying thing to him to think that he might infect me, it is his absolute
worst nightmare”
“I have my set of rules …I try to only
have sex with people who are undetectable …I sometimes trust people that are top exclusively that are
negative

PrEP positioningExclusive
Additional
Alternative
Partner type
Partner status
Positioning
Ejaculation
Cond
om u
se “I am more looking at the person now,
everyone likes the meet up with a better looking
person”
“I would not go to the position of accepting
ejaculate”
“I have definitely experienced more as a bottom since, still very
small as a percentage….I am more relaxed about allowing a guy to fuck
me”
“I have a partner who is HIV positive and we have
gone without condoms since being on the study
which we wouldn’t do before”
“It slightly loosens the boundaries
rather than taking them off
altogether”

Impact of PrEP
“I wanted to make him a bit less anxious about
having sex with me, I just wanted to reassure him
that I was taking additional precaution”
“If I wasn’t taking it, sooner or later the inevitable is going to happen”
“I will get a lot of extra piece of
mind being on it”
“It is like a defence
mechanism, you know, don’t tempt
fate”
“It takes away any possible worry
afterwards, I just feel like there is this protective
bubble there”
“It has been an absolute life saver… if I hadn’t
been on it … I don’t know how I would have
remained negative to be honest ”
Reduced anxiety,
fear, guilt, more in control, achieve desired
sex
“It certainly lets you feel
better about yourself after
sex” “I like it, it is a
security blanket”

Perception of PrEP duration• Seasons of risk
– Until not sexually active, monogamous, married, children, bored of wild sex scene, deals with demons
– Only 1 person expected to take long term
“You don’t see many 55 year old men doing
group sex, clearly it is a period, a moment … it is
not going to be a lifetime”
“I want to explore this wild sex scene that cities like London or
Berlin can offer… but I am beginning to loose
interest ”

Summary• HIV incidence – was much higher than expected in PROUD,
despite high PEP use• Effectiveness – was greater in the real world than preceding
placebo controlled trials, with an average adherence of 88%• Other STIs – were no greater in those on PrEP or not on PrEP in
PROUD, although very common in the study populations• Sexual behaviour – changes in behaviour were limited in the
quantitative data and this is supported by the qualitative data which shows slight amendments to existing high risk behaviours
• Periods – PrEP is perceived as an important additional prevention option for periods of risk
• Our findings strongly support the addition of PrEP to the standard of prevention for men who have sex with men at risk of HIV infection.

Acknowledgements (1)
Study participants
MRC CTU at UCLSarah Banbury, Liz Brodnicki, Christina Chung, Yolanda Collaco-Moraes, Monica Desai, David Dolling, David Dunn, Mitzy Gafos, Sajad Khan, Brendan Mauger, Sheena McCormack, Yinka Sowunmi, Gemma Wood
HIV & STI Dept, PHEMonica Desai, Sarika Desai, Noel Gill, Anthony Nardone, GUMCAD team, HIV team
ClinicsVanessa Apea, John Saunders, Mags Portman (Barts Health NHS Trust), Christine Bowman (Sheffield Teaching Hospitals NHS Foundation Trust), Michael Brady (Kings College Hospital NHS Foundation Trust), Martin Fisher, Amanda Clarke (Claude Nichol Centre), Julie Fox (Guy’s and St Thomas’s NHS Foundation Trust), Richard Gilson (The Mortimer Market Centre), Charles Lacey (York Hospitals NHS Foundation Trust), Nicola Mackie (St Mary’s Hospital), Alan McOwan, Simone Antonucci (56 Dean Street), Iain Reeves (Homerton University Hospital NHS Foundation Trust), Gabriel Schembri (Manchester Centre for Sexual Health), Ann Sullivan (John Hunter Clinic for Sexual Health), Steve Taylor, David White (Heart of England NHS Foundation Trust)

Acknowledgements (2)Trial Steering CommitteeIndependent members: Mike Adler (Co-Chair), Gus Cairns (Co-Chair), Dan Clutterbuck,
Rob Cookson, Claire Foreman, Stephen Nicholson, Tariq Sadiq, Matthew Williams
Investigator members: Brian Gazzard, Noel Gill, Anne Johnson, Sheena McCormack, Andrew Phillips
Gilead: Matt Bosse, Rich Clarke, Jim Rooney, Murad RufUniversity of Liverpool: Saye KhooIndependent Data Monitoring Committee: Anton Pozniak, Simon Collins, Fiona LampeCommunity Engagement GroupCommunity: Yusef Azad (NAT), Gus Cairns (NAM), Rob Cookson (LGF),
Tom Doyle (Mesmac), Justin Harbottle (THT), Marion Wadibia (NAZ),Matthew Hodson (GMFA), Cary James (THT), Roger Pebody (NAM)
Clinics: Anthony Bains, Alan McOwan (Lead), MRC CTU at UCL: Sheena McCormack, Mitzy Gafos, Annabelle SouthSocial Science Advisory GroupInterviewers: Caroline Rae, Gill Bell, Michael Rayment, Sonali Wayal, Will Nutland,
Mitzy GafosAdvisors: Ingrid Young, Ford Hickson, Lisa McDaid, Marsha Rosengarten,
Nicolas Lorente, Agata Pacho, Elizabeth Poliquin, Anthony Nardone, Catherine Dodds, Adam Bourne, David Dolling, Sheena McCormack, Rob Horne

Friday Saturday Sunday Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Ipergay : Event-Driven PrEP
2 tablets (TDF/FTC or placebo) 2-24 hours before sex
1 tablet (TDF/FTC or placebo) 24 hours later
1 tablet (TDF/FTC or placebo) 48 hours after first intake

mITT results
Group No. of infections
Incidence(per 100 PY)
TDF/FTC 2 0.94Placebo 14 6.6
Effectiveness =86% (95% CI: 40 – 99%)P value =0.002Number Needed to Treat =18Median number of pills/month (IQR): • 16 pills (10-23) in the placebo arm• 16 pills (12-24) in the TDF/FTC arm (p=0.84)

Adherence by Pill Count
Median number of pills/month (IQR): 16 pills (10-23) in the placebo arm and 16 pills (12-24) in the TDF/FTC arm (p=0.84)
48 participants (12%) received PEP25 (13%) in the TDF/FTC arm and 23 (11%) in the placebo arm (p=0.73)
0 : full bottles returned (all tablets)
Nb pills used / month
missing : 294/2798 visits (10.5%)Perc
enta
ge o
f par
ticip
ants
0
10
20
30
40
50
60
70
80
90
100
M1 M2 M4 M6 M8 M10 M12 M14 M16 M18 M20 M22 M24 M26 M28 M30Visits
] 0 - 4 ]
] 4-11]
]11-18]
]18-25]
]25-30]
382 352 315 288 236 190 162 143 128 115 105 93 88 72 63 45N part..