Protocol Summary - VCU Massey Cancer Center Web viewThis document is designed using the...
59
Virginia Commonwealth University Massey Cancer Center Investigator-Initiated Therapeutic Clinical Protocol Template (For Use with Protocols Requiring an IND) Version 2 TEMPLATE INSTRUCTIONS This template is meant to serve as a tool to help you through the process of writing a clinical trial protocol. Although the template contains typical sections and language that can be used as a starting point for your protocol, you will need to tailor it to best suit the objectives of your protocol. Comments and instructions are in blue italics and should be removed from the final document. Underlined words represent place holders that should be replaced with protocol-specific information. The Virginia Commonwealth University (VCU) Internal Review Board (IRB) Informed Consent Template is appended at the end of this document. Sections 6.02-6.15 of ICH Guideline for Good Clinical Practice (E6) are provided throughout the template on a blue background. These are meant to serve as a ready reference for you when writing the protocol, and they should be deleted from the final document. References to other protocol sections are highlighted in green to facilitate finding these references and making sure that the appropriate section number is cited. The highlights should be removed from the final document. To facilitate the development of consistently formatted Massey Cancer Center (MCC) investigator-initiated protocols, please do not modify or delete major protocol headings (1, 2, 3, etc.) when they are NOT used. Instead, please indicate that they are “not applicable.” This document is designed using the “style” feature of Microsoft Word. By following a few simple instructions you will get consistent formatting throughout the document, an outline structure that is easy to apply and does not “break”, and a table of contents that MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
Transcript of Protocol Summary - VCU Massey Cancer Center Web viewThis document is designed using the...
Virginia Commonwealth UniversityMassey Cancer Center
Investigator-Initiated Therapeutic Clinical Protocol Template(For Use with Protocols Requiring an IND)
Version 2TEMPLATE INSTRUCTIONS
This template is meant to serve as a tool to help you through the process of writing a clinical trial protocol. Although the template contains typical sections and language that can be used as a starting point for your protocol, you will need to tailor it to best suit the objectives of your protocol.
Comments and instructions are in blue italics and should be removed from the final document.
Underlined words represent place holders that should be replaced with protocol-specific information.
The Virginia Commonwealth University (VCU) Internal Review Board (IRB) Informed Consent Template is appended at the end of this document.
Sections 6.02-6.15 of ICH Guideline for Good Clinical Practice (E6) are provided throughout the template on a blue background. These are meant to serve as a ready reference for you when writing the protocol, and they should be deleted from the final document.
References to other protocol sections are highlighted in green to facilitate finding these references and making sure that the appropriate section number is cited. The highlights should be removed from the final document.
To facilitate the development of consistently formatted Massey Cancer Center (MCC) investigator-initiated protocols, please do not modify or delete major protocol headings (1, 2, 3, etc.) when they are NOT used. Instead, please indicate that they are “not applicable.”
This document is designed using the “style” feature of Microsoft Word. By following a few simple instructions you will get consistent formatting throughout the document, an outline structure that is easy to apply and does not “break”, and a table of contents that automatically updates with a couple of mouse clicks. Please review the MCC Protocol Template Guide for this information before you begin editing.
Completion of the title page is best done with the “show gridlines” feature turned on for tables.
If you need help with the templates or have any questions, please contact:
Kevin T. Hogan, Ph.D.Senior Scientific WriterMassey Cancer CenterOffice: 804-628-4915E-mail: [email protected]
Heidi Sankala Bauer, Ph.D.Scientific WriterMassey Cancer CenterOffice: 804-628-3028E-mail: [email protected]
Delete this page prior to submission.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
Title: Insert title here.
MCC Protocol #: To be assigned by the PRMC Coordinator.
FDA IND #: To be assigned by the FDA.
Principal Investigator/Study Chair/Coordinating Center/Sponsor-Investigator: (Use one as appropriate)NameAddressAddressTelephoneFaxE-mail address
IND Sponsor: (If not sponsor-investigator)NameAddressAddressTelephoneFaxE-mail address
Subinvestigator/Responsible Investigator: (Use one as appropriate)Same information as per PIA Responsible Investigator must be listed for each participating site in a multi-institutional study)
Subinvestigator/Responsible Investigator: (Use one as appropriate)Same information as per PI
Subinvestigator/Responsible Investigator: (Use one as appropriate)Same information as per PI
Subinvestigator/Responsible Investigator: (Use one as appropriate)Same information as per PI
Subinvestigator/Responsible Investigator: (Use one as appropriate)Same information as per PI
Subinvestigator/Responsible Investigator: (Use one as appropriate)Same information as per PI
Subinvestigator/Responsible Investigator: (Use one as appropriate)Same information as per PI
Subinvestigator / Responsible Investigator: (Use one as appropriate)Same information as per PI
Biostatistician:Same information as per PI
Responsible Research Nurse:Same information as per PI
Funding Sponsor: (or other designation as appropriate; delete if not needed)NameContact information
Funding Sponsor: (or other designation as appropriate; delete if not needed)NameContact information
Investigational Agent(s): Provide each agent name and indicate if its use is “commercial” or “investigational use” stock.
Version #: ### Version Date: MM/DD/YYYY
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

PROTOCOL SUMMARY
A description of the type/design of the trial to be conducted (e.g., double-blind, placebo-controlled, parallel design) and a schematic diagram of trial design, procedures and stages. [6.4.2] (See also section 3, STUDY DESIGN.)
Limit the length of the Protocol Summary to no more than 2 pages.
Title:
Protocol Number:
IND Sponsor: If applicable
Principal Investigator /Study Chair/ Coordinating Center/Sponsor-Investigator:
Study Sites:
Clinical Trial Phase: I, II, III, or IV
Study Disease:
Main Eligibility Criteria:
Primary Objectives:
Secondary Objectives:
Endpoints:
Study Design:
Study Agent/ Intervention Description:
Name, dose, frequency, duration, and route of administration
Number of Subjects:
Subject Participation Duration:
Estimated Time to Complete Enrollment:
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
Statistical Methodology:
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
SCHEMA
Insert a schema (figure or table) that concisely describes the study.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

REVISION HISTORYRevision history is presented in reverse order so that the information pertaining to the most current version of the protocol is presented first in this section.
Version 1, Version Date MM/DD/YYYY
Initial submission of the protocol.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

TABLE OF CONTENTS
PROTOCOL SUMMARY...............................................................................................................3SCHEMA.......................................................................................................................................5REVISION HISTORY................................................................................................................6TABLE OF CONTENTS................................................................................................................7LIST OF ABBREVIATIONS..........................................................................................................91 BACKGROUND............................................................................................................10
1.1 STUDY DISEASE (REPLACE HEADER WITH STUDY DISEASE)...............................................101.2 INVESTIGATIONAL AGENT(S) (REPLACE HEADER WITH INVESTIGATIONAL AGENT; USE
ADDITIONAL HEADERS IF MORE THAN ONE INVESTIGATIONAL AGENT IS USED).....................101.3 OTHER AGENTS (REPLACE HEADER WITH OTHER AGENTS USED IN THE STUDY)..................111.4 CORRELATIVE STUDIES BACKGROUND.............................................................................11
2 OBJECTIVES...............................................................................................................112.1 PRIMARY OBJECTIVES.....................................................................................................112.2 SECONDARY OBJECTIVES................................................................................................11
3 STUDY DESIGN...........................................................................................................113.1 GENERAL DESCRIPTION...................................................................................................113.2 PRIMARY OUTCOME MEASURE(S) (PRIMARY ENDPOINT[S])...............................................113.3 SECONDARY OUTCOME MEASURE(S) (SECONDARY ENDPOINT[S]).....................................12
4 PATIENT SELECTION.................................................................................................124.1 INCLUSION CRITERIA.......................................................................................................124.2 EXCLUSION CRITERIA......................................................................................................12
5 STUDY ENTRY AND WITHDRAWAL PROCEDURES...............................................135.1 STUDY ENTRY PROCEDURES...........................................................................................135.2 STUDY WITHDRAWAL PROCEDURES.................................................................................13
6 TREATMENT PLAN.....................................................................................................146.1 BASELINE TESTS AND PROCEDURES (IF APPLICABLE).......................................................146.2 INVESTIGATIONAL AGENT ADMINISTRATION (OR OTHER APPROPRIATE TITLE; “RADIATION
THERAPY” MIGHT BE APPROPRIATE FOR A RADIATION ONCOLOGY PROTOCOL)...................146.3 DEFINITION OF DLT (APPLICABLE ONLY FOR PHASE 1 TRIALS)...........................................156.4 ADDITIONAL TREATMENT MODALITIES (IF APPLICABLE)......................................................166.5 GENERAL CONCOMITANT MEDICATION AND SUPPORTIVE CARE GUIDELINES (IF APPLICABLE)
......................................................................................................................................166.6 DURATION OF THERAPY...................................................................................................166.7 MONITORING SUBJECT COMPLIANCE (IF APPLICABLE).......................................................166.8 FOLLOW-UP PERIOD.......................................................................................................16
7 DOSING DELAYS/DOSE MODIFICATIONS...............................................................168 ADVERSE EVENTS: DEFINITIONS AND REPORTING REQUIREMENTS...............18
8.1 DEFINITIONS....................................................................................................................188.2 KNOWN AES LIST............................................................................................................20
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
8.3 TIME PERIOD AND GRADE OF AE CAPTURE.....................................................................208.4 PROCEDURES FOR RECORDING AES, SAES, AND UPS....................................................208.5 ROUTINE REPORTING PROCEDURES FOR AES.................................................................218.6 EXPEDITED REPORTING PROCEDURES FOR SAES, SARS, UPS, AND DLTS......................21
9 PHARMACEUTICAL INFORMATION..........................................................................239.1 AGENT #1 (REPLACE HEADER WITH APPROPRIATE INFORMATION; REPEAT THIS SECTION AS
NEEDED FOR EACH INVESTIGATIONAL OR COMMERCIAL AGENT).........................................24
10 MEASUREMENT OF EFFECT.....................................................................................2510.1 ANTI-TUMOR EFFECT (SOLID TUMORS OR HEMATOLOGIC MALIGNANCIES AS APPROPRIATE)
......................................................................................................................................2510.2 OTHER RESPONSE PARAMETERS.....................................................................................25
11 CORRELATIVE STUDIES/SPECIAL STUDIES..........................................................2511.1 LABORATORY CORRELATIVE #1.......................................................................................2611.2 LABORATORY CORRELATIVE #1.......................................................................................2611.3 SHIPPING INSTRUCTIONS.................................................................................................26
12 STUDY CALENDAR.....................................................................................................2613 STATISTICAL CONSIDERATIONS.............................................................................26
13.1 STUDY DESIGN AND ANALYSIS.........................................................................................2713.2 SAMPLE SIZE/ACCRUAL RATES........................................................................................2713.3 STRATIFICATION FACTORS...............................................................................................2713.4 ANALYSIS OF SECONDARY ENDPOINTS.............................................................................27
14 DATA AND SAFETY MONITORING PLAN (DSMP)...................................................2814.1 STUDY TEAM...................................................................................................................2814.2 AUDIT COMMITTEE..........................................................................................................2814.3 DSMB............................................................................................................................28
15 REGULATORY COMPLIANCE AND ETHICS............................................................2915.1 ETHICAL STANDARD........................................................................................................2915.2 REGULATORY COMPLIANCE.............................................................................................2915.3 INSTITUTIONAL REVIEW BOARD........................................................................................2915.4 INFORMED CONSENT PROCESS........................................................................................2915.5 SUBJECT CONFIDENTIALITY AND ACCESS TO SOURCE DOCUMENTS/DATA.........................30
16 DATA HANDLING AND RECORD KEEPING.............................................................3016.1 DATA MANAGEMENT RESPONSIBILITIES............................................................................3116.2 SOURCE DOCUMENTS.....................................................................................................3116.3 CASE REPORT FORMS (OR OTHER APPROPRIATE TITLE TO REFLECT THE STUDY-SPECIFIC
MANNER IN WHICH PROTOCOL-SPECIFIC DATA WILL BE RECORDED)...................................3116.4 STUDY RECORD RETENTION............................................................................................32
17 REFERENCES.............................................................................................................3318 APPENDIX 1. INSERT TITLE HERE...........................................................................3419 INFORMED CONSENT TEMPLATE............................................................................35
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
LIST OF ABBREVIATIONS
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

1 BACKGROUND
Name and description of the investigational product(s). [GCP 6.2.1]
A summary of findings from nonclinical studies that potentially have clinical significance and from clinical trials that are relevant to the trial. [GCP 6.2.2]
Summary of the known and potential risks and benefits, if any, to human subjects. [GCP 6.2.3]
Description of and justification for the route of administration, dosage, dosage regimen, and treatment period(s). [GCP 6.2.4]
Description of the population to be studied. [GCP 6.2.6]
References to literature and data that are relevant to the trial, and that provide background for the trial. [GCP 6.2.7]
The outline below illustrates one way in which the background information can be organized in this section. However this information is organized, it is important to include each of the items required by Good Clinical Practice (GCP) guidance.
1.1 Study Disease (replace header with study disease)
Provide background information related to the disease to be studied.
1.2 Investigational Agent(s) (replace header with investigational agent; use additional headers if more than one investigational agent is used)
Provide the name and description of each investigational agent to be used in the study. Include background information on the agent, including the mechanism of action, summaries of nonclinical and clinical studies, nonclinical and clinical pharmacokinetics, major route of elimination, safety profile, and the rationale for the proposed dose or dose escalation scheme, as well as the route of administration, dosage regimen, and treatment period. Include information on the metabolism of the agent in humans and its potential for drug interactions, if available. The “Preclinical Data” and “Clinical Data” sections below may be useful in organizing this information. They may be used or deleted as appropriate.
1.2.1 Preclinical Data
1.2.2 Clinical Data
1.2.3 Known and Potential Risks and Benefits
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
Provide a summary of the known and potential risks and benefits to the study subjects.
1.2.4 Rationale
Provide the overall rationale for evaluating this agent in this disease.
1.3 Other Agents (replace header with other agents used in the study)
1.4 Correlative Studies Background
Provide background information for each of the planned correlative studies.
2 OBJECTIVES
A detailed description of the objectives and the purpose of the trial. [GCP 6.3]
The objectives should state the scientific question(s) that the study seeks to answer. The objectives should indicate why the study is being done and differ from the study endpoints which are the parameters used to evaluate the objectives. The primary objectives are generally therapeutic in nature (to assess the safety of…, to determine the efficacy of…, to determine the DLT [Dose-limiting toxicity] of…) while the secondary objectives are frequently related to correlative studies.
2.1 Primary Objectives
2.1.1 Insert primary objectives here.
2.2 Secondary Objectives
2.2.1 Insert secondary objectives, if any, here.
3 STUDY DESIGN
A specific statement of the primary endpoints and the secondary endpoints, if any, to be measured during the trial. [6.4.1]
A description of the type/design of the trial to be conducted (e.g. double-blind, placebo-controlled, parallel design) and a schematic diagram of trial design, procedures and stages. [6.4.2] (See also the SCHEMA section.)
A description of the measures taken to minimize/avoid bias, including: (a) randomization; (b) blinding. [6.4.3]
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
3.1 General Description
Provide a description of the type/design of the trial to be conducted including any measures such as randomization or blinding to be taken to avoid bias (e.g., double-blind, placebo-controlled, parallel design).
3.2 Primary Endpoint(s)
The primary endpoints are the clinical, chemical, biological, etc. parameters that are being measured to evaluate the primary objective(s).
3.2.1
3.3 Secondary Endpoint(s)
The secondary endpoints, if any, are the clinical, chemical, biological, etc. parameters that are being measured to evaluate the secondary objective(s).
3.3.1
4 PATIENT SELECTION
Subject inclusion criteria. [GCP 6.5.1]
Subject exclusion criteria. [GCP 6.5.2]
Medication(s)/treatment(s) permitted (including rescue medication) and not permitted before and/or during the trial. [GCP 6.6.2] (See also the TREATMENT PLAN section.)
The following prompts are suggestions for inclusion and exclusion criteria. The prompts should be replaced with the actual criteria or deleted as is appropriate for the study. See “Inclusion and Exclusion Criteria Guidelines” for additional suggestions.
4.1 Inclusion Criteria
A potential subject must meet all of the following inclusion criteria to be eligible to participate in the study.
Criteria which might be included include: (i) disease including histological or cytological confirmation and stage; (ii) allowable type and amount of prior therapy; time since last treatment; (iii) age restriction, if any; (iv) performance status and scale; (v) life expectancy; (vi) any organ or marrow function requirements; (vii) any laboratory parameter requirements; (viii) willingness to use contraception as required; (ix) any additional inclusion criteria that are appropriate to the study.
4.1.1
4.1.2 Ability to understand and the willingness to sign a written informed consent document.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
4.2 Exclusion Criteria
A potential subject who meets any of the following exclusion criteria is ineligible to participate in the study.
Criteria which might be included include: (i) receiving any other investigational agents; (ii) brain metastases, if a factor; (iii) history of allergic reactions to any of the required agents on the study; (iv) concomitant medications or substances that have the potential to affect the activity or pharmacokinetics of the study agent; (v) uncontrolled or intercurrent illness that would interfere with achieving the study objectives;(vi) pregnant; (vii) HIV-positive; (viii) any additional exclusion criteria that are appropriate to the study.
4.2.1
5 STUDY ENTRY AND WITHDRAWAL PROCEDURES
Subject withdrawal criteria (i.e. terminating investigational product treatment/trial treatment) and procedures for specifying: (a) when and how to withdraw subjects from the trial/investigational product treatment; (b) the type and timing of the data to be collected for withdrawn subjects; (c) whether and how subjects are to be replaced; and (d) the follow-up for subjects withdrawn from investigational product treatment/trial treatment. [GCP 6.5.3] (See also section 6, TREATMENT PLAN; section 13, STATISTICAL CONSIDERATIONS.)
5.1 Study Entry Procedures
5.1.1 Required Pre-Registration Screening Tests and Procedures
Refer to section 11, STUDY CALENDAR, for the screening tests and procedures that are required prior to registration, and for the timing of these events relative to the start of treatment. (sample language)
5.1.2 Registration Process
Describe the process to be used. Who should be contacted and how? What information is required (ICF, HIPAA authorization form, copy of required laboratory tests, eligibility screening worksheet, registration form, etc.)? How soon after registration must the subject begin treatment? What are the procedures to be followed if this is a multicenter trial?
5.2 Study Withdrawal Procedures
5.2.1 A patient may decide to withdraw from the study at any time.
5.2.2 A patient may be removed from treatment for one of the following criteria: (The 2 broad categories are as follows, although the first is frequently made more specific as indicated below.)
5.2.2.1 If in the opinion of the treating physician, it is in the best interest of the patient to do so. (This is a generic statement that some investigators prefer.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

You may want to include more specific criteria such as (i) unwillingness or inability of the patient to comply with the protocol requirements; (ii) disease progression; (iii) intercurrent illness that prevents further administration of treatment; (iv) unacceptable adverse events (AE[s]); and (v) general or specific changes in the patient's condition render the patient unacceptable for further treatment in the judgment of the investigator.)
5.2.2.2 Sponsor’s decision to discontinue the study.
5.2.3 The reason for withdraw from the study and the date the patient was removed from the study must be documented in the case report form (eCRF/CRF [choose one]).
6 TREATMENT PLAN
A description of the trial treatment(s) and the dosage and dosage regimen of the investigational product(s). Also include a description of the dosage form, packing, and labeling of the investigational product(s). [GCP 6.4.4] (See also section 9, PHARMACEUTICAL INFORMATION.)
The expected duration of the subject participation, and a description of the sequence and duration of all trial periods, including follow-up, if any. [GCP 6.4.5]
The treatment(s) to be administered, including the name(s) of all the product(s), the dose(s), the dosing schedule(s), the route/mode(s) of administration, and the treatment period(s), including the follow-up period(s) for subjects for each investigational product treatment/trial treatment group/arm of the trial. [GCP 6.6.1]
Medication(s)/treatment(s) permitted (including rescue medication) and not permitted before and/or during the trial. [GCP 6.6.2] (See also section 4, PATIENT SELECTION.)
Procedures for monitoring subject compliance. [GCP 6.6.3]
Specification of safety parameters. [GCP 6.8.1] (See also section 7, DOSING DELAYS/DOSE MODIFICATIONS; section 8, ADVERSE EVENTS.)
The methods and timing for assessing, recording, and analyzing safety parameters. [GCP 6.8.2] (See also section 8, ADVERSE EVENTS; section 12, STUDY CALENDAR; section 13, STATISTICAL CONSIDERATIONS; section 14, DATA AND SAFETY MONITORING PLAN.)
The type and duration of the follow-up of subjects after adverse events. [GCP 6.8.4]
6.1 Baseline Tests and Procedures (if applicable)
Indicate any tests or procedures that are necessary to confirm that a subject still meets the eligibility requirements, or that are required at baseline for later outcome comparison after study intervention. Alternatively, indicate that this information is located in section 11, STUDY CALENDAR.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
6.2 Investigational Agent Administration (or other appropriate title; “Radiation Therapy” might be appropriate for a radiation oncology protocol)
**’*PHASE 1 STUDIES***
State the starting dose of the investigational agent and describe the dose escalation scheme and treatment regimen (dose, route, duration of infusion for intravenous drugs, and schedule). Use exact dose rather than percentages. State any special precautions or warnings relevant for agent administration (e.g., incompatibility of agent with commonly used intravenous solutions, necessity of administering agent with food, pre-medications, etc.). A table may be used to describe the regimen.
***PHASE 2 STUDIES***
Describe the regimen (agent, dose, route, duration of infusion for intravenous drugs, and schedule) and state any special precautions or warnings relevant for investigational study agent administration (e.g., incompatibility of the agent with commonly used intravenous solutions, necessity of administering agent with food, pre-medications, etc.). Inclusion of a treatment table may be useful in clarifying the regimen.
***INTERVENTIONAL STUDIES INVOLVING OTHER THAN A STUDY DRUG***
If the primary intervention involves something other than a study drug, a different header will most likely be more appropriate for this section. As an example, Radiation Therapy” may more accurately reflect the intervention. The “Additional Treatment Modalities” section below might then be used to describe the concomitant use of other treatment modalities.
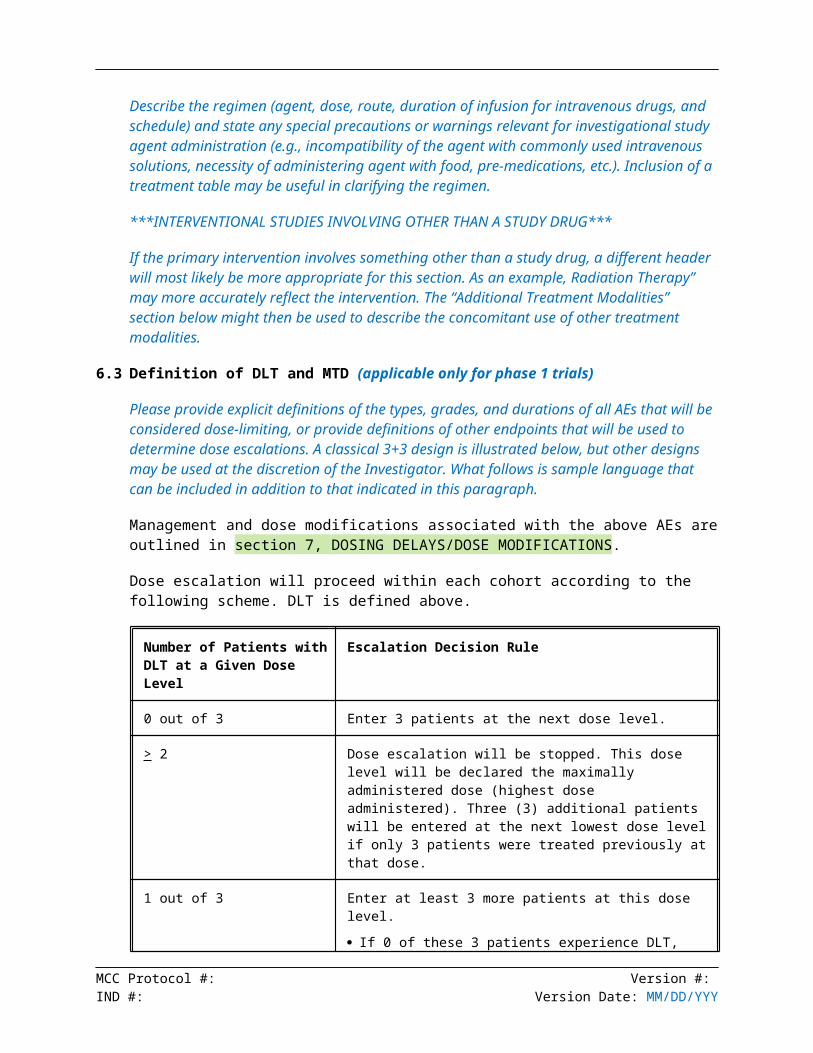
6.3 Definition of DLT and MTD (applicable only for phase 1 trials)
Please provide explicit definitions of the types, grades, and durations of all AEs that will be considered dose-limiting, or provide definitions of other endpoints that will be used to determine dose escalations. A classical 3+3 design is illustrated below, but other designs may be used at the discretion of the Investigator. What follows is sample language that can be included in addition to that indicated in this paragraph.
Management and dose modifications associated with the above AEs are outlined in section 7, DOSING DELAYS/DOSE MODIFICATIONS.
Dose escalation will proceed within each cohort according to the following scheme. DLT is defined above.
Number of Patients with DLT at a Given Dose Level
Escalation Decision Rule
0 out of 3 Enter 3 patients at the next dose level.
> 2 Dose escalation will be stopped. This dose level will be declared the maximally administered dose (highest dose administered). Three (3) additional patients will be entered at the next lowest dose level if only 3 patients were treated previously at that dose.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
1 out of 3 Enter at least 3 more patients at this dose level.
If 0 of these 3 patients experience DLT, proceed to the next dose level.
If 1 or more of this group suffer DLT, then dose escalation is stopped, and this dose is declared the maximally administered dose. Three (3) additional patients will be entered at the next lowest dose level if only 3 patients were treated previously at that dose.
<1 out of 6 at highest dose level below the maximally administered dose
This is generally the recommended phase 2 dose. At least 6 patients must be entered at the recommended phase 2 dose.
6.4 Additional Treatment Modalities (if applicable)
Provide a detailed description of any other modalities (e.g., surgery, chemotherapy, radiotherapy) or procedures (e.g., hematopoietic stem cell transplantation) used in the protocol treatment.
6.5 General Concomitant Medication and Supportive Care Guidelines (if applicable)
Describe in detail any prophylactic or supportive care regimens required for investigational study agent(s) administration and state any special precautions or relevant warnings (e.g., incompatibility of agent with commonly used intravenous solutions, necessity of administering agent(s) with food, pre-medications, etc.). Provide the same information for any other agent used in the study.
State guidelines for use of concomitant medications or any additional appropriate supportive care medications or treatments. The potential for interaction with the cytochrome P450 system should be addressed if applicable.
Precautions or prohibitions regarding herbal products, complementary or alternative medications, and dietary supplements should be included here.
6.6 Duration of Therapy
Describe the number and duration of cycles of therapy. Describe if and how subjects are replaced, if applicable. Reference to the study calendar may be made.
6.7 Monitoring Subject Compliance (if applicable)
Describe the procedures to be used to monitor subject compliance such as the use of a study diary.
6.8 Follow-Up Period
Describe how and for how long the patients will be followed after an AE or after the completion of the treatment phase of the study. The details may be placed in section 11, STUDY CALENDAR, with an appropriate reference made to that section of the protocol. Sample language follows-
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

Patients will be followed for # weeks/months/years after removal from the study treatment or until death, whichever occurs first. Patients removed from the study treatment for unacceptable AEs will be followed until resolution or stabilization of the adverse event.
7 DOSING DELAYS/DOSE MODIFICATIONS
Specification of safety parameters. [GCP 6.8.1] (See also section 6, TREATMENT PLAN; section 8, ADVERSE EVENTS.)
Treatment plans should explicitly identify when treatment (typically dose) modifications are appropriate. Treatment modifications/dosing delays and the factors predicating treatment modification should be explicit and clear. If dose modifications or treatment delays are anticipated, please provide a dose de-escalation schema. The following format for an orally available agent is provided as an example and can be modified, replaced, or deleted as appropriate:
Dose Level Agent Name Dose
-2 XX mg, schedule
-1 XX mg, schedule
0 XX mg, schedule
Note: All treatment modifications must be expressed as a specific dose or amount rather than as a percentage of the starting or previous dose.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
8 ADVERSE EVENTS: DEFINITIONS AND REPORTING REQUIREMENTS
Specification of safety parameters. [GCP 6.8.1] (See also section 6, TREATMENT PLAN; section 7, DOSING DELAYS/DOSE MODIFICATIONS.)
The methods and timing for assessing, recording, and analyzing safety parameters. [GCP 6.8.2]
Procedures for eliciting reports of and for recording and reporting adverse event and intercurrent (See also section 6, TREATMENT PLAN; section 12, STUDY CALENDAR; section 13, STATISTICAL CONSIDERATIONS; section 14, DATA AND SAFETY MONITORING PLAN.) illnesses. [GCP 6.8.3]
8.1 Definitions
8.1.1 Adverse Event (AE)
AE means any untoward medical occurrence associated with the use of a drug in humans, whether or not considered drug related.
8.1.2 Suspected Adverse Reaction (SAR)
Any AE for which there is a reasonable possibility that the drug caused the AE. “Reasonable possibility” means that there is evidence to suggest a causal relationship between the drug and the AE.
An AE with an attribution of possible, probable, or definite (see section 8.3.3 below) is a SAR.
8.1.3 Serious AE (SAE) or Serious SAR (SSAR)
An AE or SAR is considered “serious” if, in the view of either the investigator or sponsor, it results in any of the following outcomes:
death,
a life-threatening AE (An AE or SAR is consider “life-threatening” if, in the view of either the investigator or sponsor, its occurrence places the patient or subject at immediate risk of death. It does not include an AE or SAR that, had it occurred in a more severe form, might have caused death.),
inpatient hospitalization or prolongation of existing hospitalization,
a persistent or significant incapacity or substantial disruption of the ability to conduct normal life functions, or
a congenital anomaly/birth defect.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
Important medical events that may not result in death, be life-threatening, or require hospitalization may be considered serious when, based upon appropriate medical judgment, they may jeopardize the patient or subject and may require medical or surgical intervention to prevent one of the outcomes listed in this definition.
8.1.4 Unexpected SAR
A SAR is considered “unexpected” if
it is not listed in the investigator brochure or is not listed at the specificity or severity that has been observed;
or, if an investigator brochure is not required or available, is not consistent with the risk information described in the general investigational plan or elsewhere in the current application, as amended.
“Unexpected” as used in this definition, also refers to SARs that are mentioned in the investigator brochure as occurring with a class of drugs or as anticipated from the pharmacological properties of the drug, but are not specifically mentioned as occurring with the particular drug under investigation.
If the investigator/research nurse/CRA do not plan to reference the investigator brochure or general investigation plan to determine if a SAR is unexpected, then a comprehensive listing of SARs needs to be placed within the protocol so that the determination can be made without reference to the external documents.
8.1.5 Unanticipated Problem (UP)
Unanticipated problems include any incident, experience, or outcome that meets all of the following criteria:
unexpected (in terms of nature, severity, frequency) given (a) the research procedures that are described in the protocol-related documents, such as the IRB-approved research protocol and informed consent document; and (b) the characteristics of the subject population being studied;
related or possibly related to participation in the research (possibly related means there is a reasonable possibility that the incident, experience, or outcome may have been caused by the procedures involved in the research); and
suggests that the research places subjects or others at a greater risk of harm (including physical, psychological, economic, or social harm) than was previously known or recognized.
8.1.6 AE Description and Grade
The descriptions and grading scales found in the revised Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 will be utilized for AE reporting.
8.1.7 AE Expectedness
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

AEs can be ‘Unexpected’ or ‘Expected’.
Expected AEs are listed in section 8.2 below.
Unexpected AEs are those AEs occurring in one or more subjects participating in the research protocol, the nature, severity, or frequency of which is not consistent with either:
The known or foreseeable risk of AEs associated with the procedures involved in the research that are described in (a) the protocol-related document, such as the IRB-approved research protocol, any applicable investigator brochure, and the current IRB-approved informed consent document, and other relevant sources of information, such as product labeling and package inserts; or
The expected natural progression of any underlying disease, disorder, or condition of the subject(s) experiencing the AE and the subject’s predisposing risk factor profile for the AE.
8.1.8 AE Attribution
Definite – The AE is clearly related to the study treatment.
Probable – The AE is likely related to the study treatment.
Possible – The AE may be related to the study treatment.
Unlikely – The AE is doubtfully related to the study treatment.
Unrelated – The AE is clearly NOT related to the study treatment.
8.2 Known AEs List
Provide a list of the AEs and potential risks associated with the investigational agent and/or study protocol.
8.3 Time Period and Grade of AE Capture
The time period over which AEs will be captured should be specified, as well as the grade of the adverse events to be captured. The period of capture is often defined as running from the beginning of any study procedures through 30 days following the end of the study treatment.
8.4 Procedures for Recording AEs, SAEs, and UPs
Describe the procedures by which AEs, SAEs, and UPs will be recorded including the time points and method of recording (such as using CRFs).
8.5 Routine Reporting Procedures for AEs
Describe the frequency and procedure by which routine AEs will be reported to the Sponsor, Sponsor-Investigator, Principal Investigator, Collaborating Company, or Monitoring Entity (choose as is appropriate for the study).
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
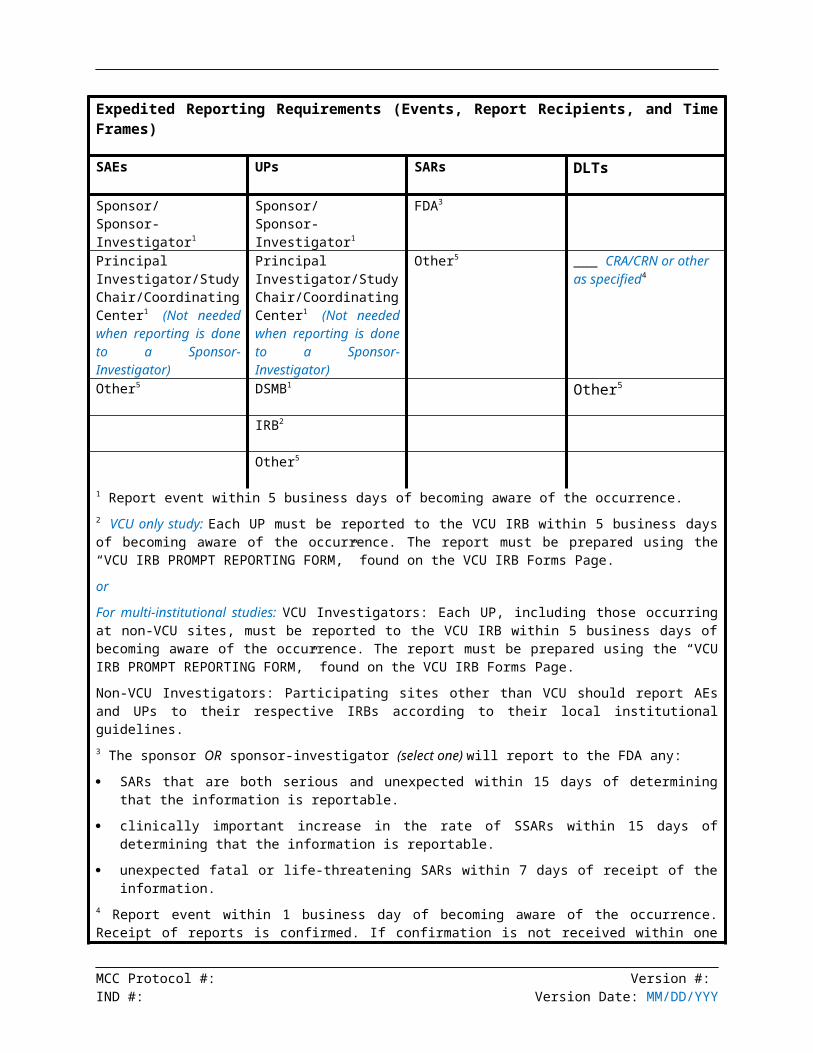
8.6 Expedited Reporting Procedures for SAEs, SARs, UPs, and DLTs
The following table should be used for phase 1 trials with DLT reporting requirements:
Expedited Reporting Requirements (Events, Report Recipients, and Time Frames)
SAEs UPs SARs DLTs
Sponsor/Sponsor-Investigator1
Sponsor/Sponsor-Investigator1
FDA3
Principal Investigator/Study Chair/Coordinating Center1 (Not needed when reporting is done to a Sponsor-Investigator)
Principal Investigator/Study Chair/Coordinating Center1 (Not needed when reporting is done to a Sponsor-Investigator)
Other5 ___ CRA/CRN or other as specified4
Other5 DSMB1 Other5
IRB2
Other5
1 Report event within 5 business days of becoming aware of the occurrence.2 VCU only study: Each UP must be reported to the VCU IRB within 5 business days of becoming aware of the occurrence. The report must be prepared using the “VCU IRB PROMPT REPORTING FORM,” found on the VCU IRB Forms Page.
or
For multi-institutional studies: VCU Investigators: Each UP, including those occurring at non-VCU sites, must be reported to the VCU IRB within 5 business days of becoming aware of the occurrence. The report must be prepared using the “VCU IRB PROMPT REPORTING FORM,” found on the VCU IRB Forms Page.
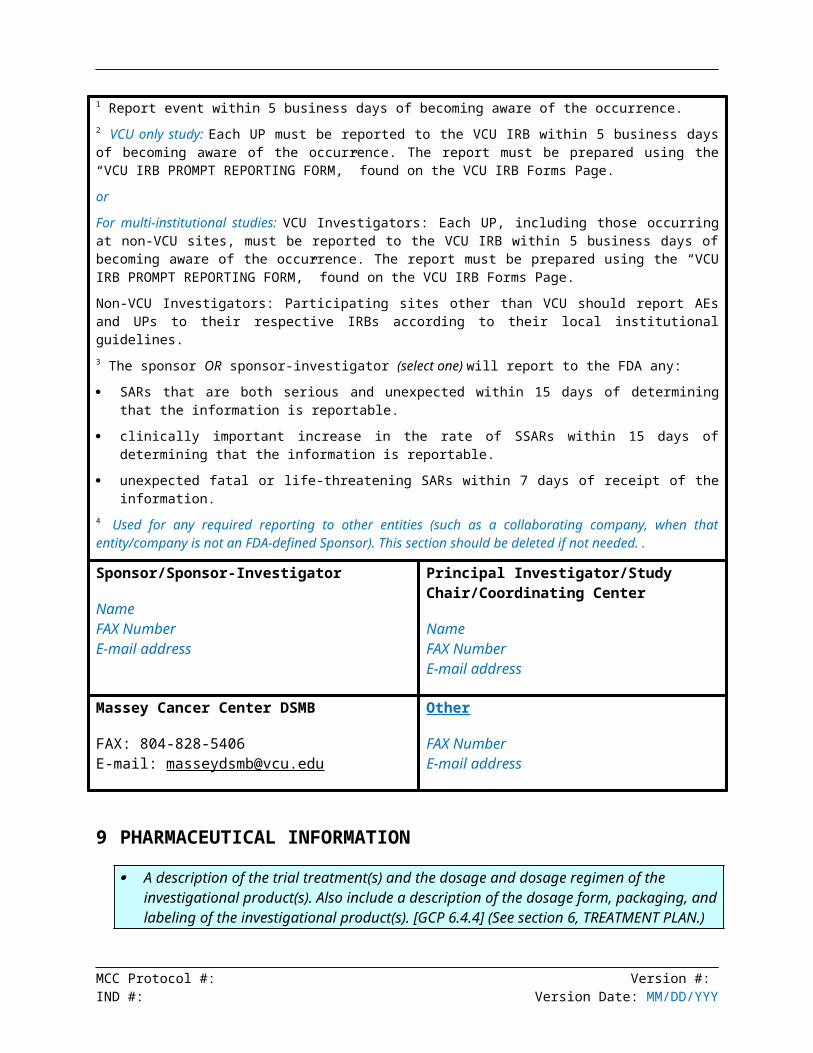
Non-VCU Investigators: Participating sites other than VCU should report AEs and UPs to their respective IRBs according to their local institutional guidelines.3 The sponsor OR sponsor-investigator (select one) will report to the FDA any:
SARs that are both serious and unexpected within 15 days of determining that the information is reportable.
clinically important increase in the rate of SSARs within 15 days of determining that the information is reportable.
unexpected fatal or life-threatening SARs within 7 days of receipt of the information.4 Report event within 1 business day of becoming aware of the occurrence. Receipt of reports is confirmed. If confirmation is not received within one working day, the coordinating center should be called by telephone (804- - ).5 Used for any required reporting to other entities (such as a collaborating company, when that entity/company is not an FDA-defined Sponsor). This section should be deleted if not needed..
Sponsor/Sponsor-Investigator
Name
Principal Investigator/Study Chair/Coordinating Center
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

FAX NumberE-mail address
NameFAX NumberE-mail address
Massey Cancer Center DSMB
FAX: 804-828-5406E-mail: [email protected]
CRA/CRN or other as specified
FAX NumberE-mail address
Other
FAX NumberE-mail address
The following table should be used for protocols that do not have DLT reporting requirements.
Expedited Reporting Requirements (Events, Report Recipients, and Time Frames)
SAEs UPs SARs
Sponsor/Sponsor-Investigator1
Sponsor/Sponsor-Investigator1
FDA3
Principal Investigator/Study Chair/Coordinating Center1 (Not needed when reporting is done to a Sponsor-Investigator)
Principal Investigator/Study Chair/Coordinating Center1 (Not needed when reporting is done to a Sponsor-Investigator)
Other4
Other4 DSMB1
IRB2
Other4
1 Report event within 5 business days of becoming aware of the occurrence.2 VCU only study: Each UP must be reported to the VCU IRB within 5 business days of becoming aware of the occurrence. The report must be prepared using the “VCU IRB PROMPT REPORTING FORM,” found on the VCU IRB Forms Page.
or
For multi-institutional studies: VCU Investigators: Each UP, including those occurring at non-VCU sites, must be reported to the VCU IRB within 5 business days of becoming aware of the occurrence. The report must be prepared using the “VCU IRB PROMPT REPORTING FORM,” found on the VCU IRB Forms Page.
Non-VCU Investigators: Participating sites other than VCU should report AEs and UPs to their respective IRBs according to their local institutional guidelines.3 The sponsor OR sponsor-investigator (select one) will report to the FDA any:
SARs that are both serious and unexpected within 15 days of determining that the information is
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
reportable.
clinically important increase in the rate of SSARs within 15 days of determining that the information is reportable.
unexpected fatal or life-threatening SARs within 7 days of receipt of the information.4 Used for any required reporting to other entities (such as a collaborating company, when that entity/company is not an FDA-defined Sponsor). This section should be deleted if not needed..
Sponsor/Sponsor-Investigator
NameFAX NumberE-mail address
Principal Investigator/Study Chair/Coordinating Center
NameFAX NumberE-mail address
Massey Cancer Center DSMB
FAX: 804-828-5406E-mail: [email protected]
Other
FAX NumberE-mail address
9 PHARMACEUTICAL INFORMATION
A description of the trial treatment(s) and the dosage and dosage regimen of the investigational product(s). Also include a description of the dosage form, packaging, and labeling of the investigational product(s). [GCP 6.4.4] (See section 6, TREATMENT PLAN.)
Accountability procedures for the investigational product(s), including the placebo(s) and the comparator(s), if any. [GCP 6.4.7]
Each investigational or commercial agent should have its own section. The level of detail needed is dependent upon whether the agent is investigational or commercial. Refer to the Investigator’s Brochure, pharmaceutical data sheet, and/or package insert for this information. The source of information should be included in this section.
9.1 Agent #1 (replace header with appropriate information; repeat this section as needed for each investigational or commercial agent)
9.1.1 Product Description
Include the available dosage forms, ingredients, and packaging as appropriate.
9.1.2 Solution Preparation
Describe how a dose is prepared. Include reconstitution directions and directions for further dilution, if appropriate.
9.1.3 Storage Requirements
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
Include the requirements for the original dosage form, reconstituted solution, and the final diluted product, as applicable.
9.1.4 Stability
Include the stability of the original dosage form, reconstituted solution, and final diluted product as applicable.
9.1.5 Route of Administration
Include a description of the method to be used and the rate of administration, if applicable.
9.1.6 Handling
Include any special handling requirements including the need for handling precautions or special equipment.
9.1.7 Availability
Include the supplier of the agent and how the agent will be distributed to investigators.
9.1.8 Agent Ordering
Describe how the agent will be obtained. If a multicenter study, indicate that each site is responsible for ordering their own supply.
9.1.9 Agent Accountability
Describe how agent accountability records will be kept. The following text is modified from the CTEP model protocols and can be used or further modified as appropriate:
The investigator, or a responsible party designated by the investigator, must maintain a careful record of the inventory and disposition of all agents received from drug source using the Drug Accountability Record Form.
9.1.10 Agent Destruction and Return
Describe how any unused agent will be destroyed or returned to the supplier. Sample text:
At the conclusion of the study, any unused agent will be destroyed according to institutional policies. The destruction will be recorded on the Drug Accountability Record Form.
10 MEASUREMENT OF EFFECT
Specification of the efficacy parameters. [GCP 6.7.1]
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
Methods and timing for assessing, recording, and analyzing of efficacy parameters. [GCP 6.7.2] (See also section 12, STUDY CALENDAR; section 13, STATISTICAL CONSIDERATIONS.)
Provide the response criteria for the study. Separate documents are available with RECIST criteria for solid tumors, as well as additional criteria for hematologic malignancies.
10.1 Anti-tumor Effect (Solid Tumors or Hematologic Malignancies as Appropriate)
If applicable, please provide appropriate criteria for evaluation of response and methods of measurement.
10.2 Other Response Parameters
Other endpoints and the criteria for their measurement should be entered below or reference should be made to the protocol section where these criteria may be found.
11 CORRELATIVE STUDIES/SPECIAL STUDIES
Briefly describe all planned correlative studies. For each, indicate if it is mandatory or optional. Explicit instructions for the handling, preserving, and assaying of the specimens should be provided below or in a referenced biospecimen manual. If samples will be shipped to a central laboratory for processing and analysis, responsible parties and contact information should be provided below.
A plan for statistical analysis of the results of the correlative studies should be provided in section 13.4, Analysis of Secondary Endpoints.
11.1 Laboratory Correlative #1
11.2 Laboratory Correlative # 2
11.3 Shipping Instructions
12 STUDY CALENDAR
The identification of any data to be recorded directly on the CRFs (i.e. no prior written or electronic record of data), and to be considered a source of data. [GCP 6.4.9]
Methods and timing for assessing, recording, and analyzing of efficacy parameters. [GCP 6.7.2] (See also section 10, MEASUREMENT OF EFFECT ; section 13, STATISTICAL CONSIDERATIONS.)
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
The methods and timing for assessing, recording, and analyzing safety parameters. [6.8.2] (See also section 6, TREATMENT PLAN; section 8, ADVERSE EVENTS; section 13, STATISTICAL CONSIDERATIONS; section 14, DATA AND SAFETY MONITORING PLAN.)
A detailed study calendar in the form of a table should be provided here. The study calendar should describe the treatments and procedures to be performed at each time point throughout the study. It may be useful to subdivide the calendar into 3 sections: (1) pre-treatment; (2) treatment; and (3) post-treatment/follow-up. The timing of any pre-registration and/or baseline scans should be noted. Where appropriate, incorporate flexibility into the timing of the study calendar items (e.g., ± 1 day).
13 STATISTICAL CONSIDERATIONS
A description of the “stopping rules” or “discontinuation criteria” for individual subjects, parts of trial and entire trial. [GCP 6.4.6]
Maintenance of trial treatment randomization codes and procedures for breaking codes. [GCP 6.4.8]
Subject withdrawal criteria (i.e. terminating investigational product treatment/trial treatment) and procedures for specifying: (a) when and how to withdraw subjects from the trial/investigational product treatment; (b) the type and timing of the data to be collected for withdrawn subjects; (c) whether and how subjects are to be replaced; and (d) the follow-up for subjects withdrawn from investigational product treatment/trial treatment. [GCP 6.5.3] (See also section 5, STUDY ENTRY AND WITHDRAWAL PROCEDURES.)
Methods and timing for assessing, recording, and analyzing of efficacy parameters. [GCP 6.7.2] (See also section 5, STUDY ENTRY AND WITHDRAWAL PROCEDURES; section 10, MEASUREMENT OF EFFECT; section 12, STUDY CALENDAR.)
The methods and timing for assessing, recording, and analyzing safety parameters. [GCP 6.8.2] (See also section 6, TREATMENT PLAN; section 8, ADVERSE EVENTS; section 12, STUDY CALENDAR; section 14, DATA AND SAFETY MONITORING PLAN.)
A description of the statistical methods to be employed, including timing of planned interim analysis(ses). [GCP 6.9.1]
The number of subjects planned to be enrolled. In multicenter trials, the numbers of enrolled subjects projected for each trial site should be specified. Reasons for choice of sample size, including reflections on (or calculations of) the power of the trial and clinical justification. [GCP 6.9.2]
The level of significance to be used. [GCP 6.9.3]
Criteria for the termination of the trial. [GCP 6.9.4]
Procedures for accounting for missing, unused, and spurious data. [GCP 6.9.5]
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

Procedures for reporting any deviation(s) from the original statistical plan (any deviation(s) from the original statistical plan should be described and justified in the protocol and/or in the final report, as appropriate). [GCP 6.9.6]
The selection of subjects to be included in the analyses (e.g. all randomized subjects, all dosed subjects, all eligible subjects, evaluable subjects). [GCP 6.9.7]
The Statistical Design section must be written in consultation with the study biostatistician. The study biostatistician must also approve this section. The outline given in sections 13.1-13.4 is typical of many study designs, but may be modified to meet the needs of a particular study.
13.1 Study Design and Analysis
13.2 Sample Size/Accrual Rates
Specify the planned sample size and accrual rate (e.g., patients/month).
13.3 Stratification Factors
Specify any planned patient stratification factors. Indicate whether interim monitoring and efficacy determination will be done for each stratum individually.
13.4 Analysis of Secondary Endpoints
If secondary endpoints are included in this study, please specify how they will be analyzed. In particular, brief descriptions should be given of analyses of pharmacokinetic, biologic, and correlative laboratory endpoints.
14 DATA AND SAFETY MONITORING PLAN (DSMP)
The methods and timing for assessing, recording, and analyzing safety parameters. [GCP 6.8.2] (See also section 6, TREATMENT PLAN; section 8, ADVERSE EVENTS; section 12, STUDY CALENDAR; section 13, STATISTICAL CONSIDERATIONS.)
Quality Control and Quality Assurance [GCP 6.11]
MCC requires that all study protocols include a study team. Study protocols that involve more than minimal risks are also required to have an Audit Committee and a DSMP. The default DSMP is a DSMB which is assigned by the Office of Clinical Research. If the investigator proposes a DSMP other than a DSMB, the plan must be specified below. The following model language should be tailored to the needs of the study.
Include the following statement for a minimal risk study:
The DSMP for this study will consist of a single element, a study team:
Include the following statement for a study involving more than minimal risk.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
The DSMP for this study will consist of the following 3 elements:
14.1 Study Team
This section should be included for all studies. The following language is tailored for a study that involves more than minimal risk. It should be modified as necessary to meet the needs of a particular study.
The study team minimally consists of the principal investigator, the research nurse, the clinical research associate, and the study biostatistician. While subjects are on treatment, the principal investigator, the research nurse, and the clinical research associate will meet at least monthly, and will meet at least quarterly with the study biostatistician, to review study status (attendees and time periods should be modified so as to make sense within the context of the study). This review will include, but not be limited to, reportable AEs and UPs, and an update of the ongoing study summary that describes study progress in terms of the study schema. The appropriateness of further subject enrollment and the specific intervention for a next subject enrollment are addressed. All meetings including attendance are documented.
14.2 Audit Committee
This trial will be audited by the MCC Audit Committee.
14.3 DSMB
Include this section if an MCC DSMB will be used. If the DSMP for the study involves other than an MCC DSMB, this section should be modified accordingly.
The study will be monitored by the MCC DSMB.
15 REGULATORY COMPLIANCE AND ETHICS
A statement that the trial will be conducted in compliance with the protocol, GCP [language indicating compliance with GCP will not be included in the protocol until such time that MCC follows the guidelines] and the applicable regulatory requirement(s). [GCP 6.2.5]
Description of ethical considerations relating to the trial. [GCP 6.12]
15.1 Ethical Standard
This study will be conducted in conformance with the principles set forth in The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research (US National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research, April 18, 1979).
15.2 Regulatory Compliance
This study will be conducted in compliance with:
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
The protocol
Federal regulations, as applicable, including: 21 CFR 50 (Protection of Human Subjects/Informed Consent); 21 CFR 56 (Institutional Review Boards); 21 CFR 312 (IND Application); and 45 CFR 46 Subparts A (Common Rule), B (Pregnant Women, Human Fetuses and Neonates), C (Prisoners), and D (Children)
15.3 Institutional Review Board
Each participating institution must provide for the review and approval of this protocol and the associated informed consent documents and recruitment material by an appropriate IRB registered with the Office for Human Research Protections (OHRP). Any amendments to the protocol or consent materials must also be approved. In the United States and in other countries, only institutions holding a current US Federalwide Assurance issued by OHRP may participate.
15.4 Informed Consent Process
Informed consent is a process that is initiated prior to the individual’s agreeing to participate in the study and continues throughout the individual’s study participation. Extensive discussion of risks and possible benefits of this therapy will be provided to the subjects and their families. Consent forms describing in detail the study interventions/ products, study procedures, and risks are given to the subject and written documentation of informed consent is required prior to starting intervention/administering study product. Consent forms will be IRB-approved and the subject will be asked to read and review the document. Upon reviewing the document, the investigator will explain the research study to the subject and answer any questions that may arise. The subject will sign the informed consent document prior to any procedures being done specifically for the study. The subjects should have the opportunity to discuss the study with their surrogates or think about it prior to agreeing to participate. The subjects may withdraw consent at any time throughout the course of the trial. A copy of the informed consent document will be given to the subjects for their records. The rights and welfare of the subjects will be protected by emphasizing to them that the quality of their medical care will not be adversely affected if they decline to participate in this study.
15.5 Subject Confidentiality and Access to Source Documents/Data
Subject confidentiality is strictly held in trust by the sponsor/sponsor-investigator (choose one as appropriate), participating investigators, and any staff, [and the sponsor(s) and their agents] (include bracketed portion if applicable). This confidentiality includes the clinical information relating to participating subjects, as well as any genetic or biological testing.
The study protocol, documentation, data, and all other information generated will be held in strict confidence. No information concerning the study or the data will be released to any unauthorized third party without prior written approval of the sponsor/sponsor-investigator/principal investigator/study chair (choose one as appropriate).
If not covered in a separate agreement, the sponsor should ensure the investigators/institutions will allow access to all source data and documents for the purposes of monitoring, audits, IRB review, and regulatory inspections. Sample text below:
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
The sponsor/sponsor-investigator/principal investigator/study chair (choose one as appropriate) will allow access to all source data and documents for the purposes of monitoring, audits, IRB review, and regulatory inspections. Source documents provided to coordinating center for the purpose of auditing or monitoring will be de-identified and labeled with the study number, subject ID, and patient initials (include this sentence if protocol is conducted at more than one site).
The study monitor or other authorized representatives of the sponsor/sponsor-investigator/principal investigator/study chair (choose one as appropriate) may inspect all documents and records required to be maintained by the investigator, including but not limited to, medical records (office, clinic, or hospital) and pharmacy records for the subjects in this study. The clinical study site will permit access to such records.
16 DATA HANDLING AND RECORD KEEPING
Access to Source Documents/Data: The sponsor should ensure that it is specified in the protocol or other written agreement that the investigator(s)/institution(s) will permit trial-related monitoring, audits, IRB/IEC review, and regulatory inspection(s), providing direct access to source data/documents. [GCP 6.10]
Data handling and record keeping. [GCP 6.13]
Include instructions for special data handling or record keeping procedures required for maintaining participant confidentiality, any special data securing requirements, and record retention per the sponsor’s requirements in this section. If not contained in another written agreement, include information allowing the sponsor to have access to all trial-related data.
Briefly describe steps to be taken to assure that the data collected are accurate, consistent, complete and reliable. The description should include reference to source documentation, CRFs, instructions for completing forms, data handling procedures, and procedures for data monitoring. Details may be provided in another referenced document.
The following subdivisions may prove useful for organizing this section.
16.1 Data Management Responsibilities
Describe responsibilities for data handling and record keeping as they specifically relate to the sponsor, clinical site, laboratory, and data coordinating center. Information should include the role in data collection, review of data, trial materials, and reports. Sample text for a multi-site study involving an IND is given below (modify accordingly to meet the needs of a particular study):
The sponsor/sponsor-investigator is responsible for: (i) reviewing SAE reports; (ii) determining if SARs need to be reported to the FDA, and if so, filing the report; (iii) filing annual IND reports; and (iv) filing IND amendments.
The sponsor-investigator/principal investigator is responsible for: (i) the overall conduct of the investigation; (ii) ongoing review of trial data including all safety reports; and (iii) apprising participating sites of any UPs.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
The responsible investigator at each site is responsible for: (i) the data management at his or her site; and (ii) reporting SAEs, UPs, and DLTs as required in section 8.
Any laboratory conducting correlative studies must maintain the laboratory records and documentation (laboratory notebooks, laboratory protocols, print-outs, recordings, photographs, etc.).
16.2 Source Documents
Provide a description of the source documents which include all information, original records of clinical findings, or other activities in a clinical trial necessary for the reconstruction and evaluation of the trial. Sample text below:
Source documents for clinical information (patient history, diagnosis, clinical and diagnostic test reports, etc.) are maintained in the patient’s clinical file. Source documents for the correlative studies are maintained in laboratory conducting the study.
16.3 Case Report Forms (or other appropriate title to reflect the study-specific manner in which protocol-specific data will be recorded)
Sample text below for eCRFs:
MCC Oncore data management will provide standard electronic case report forms (eCRFs) and create study-specific eCRFs to capture all the information required by the protocol. The eCRFs will be approved by the study team to ensure the most effective data acquisition. All information on eCRFs will be traceable to the source documents which are generally maintained in the subject’s file. All eCRFs should be completed and available for collection within a timely manner, preferably no more than 14 days after the subject’s visit.
If the study does not involve eCRFs, a description of the manner in which the data will be recorded and maintained should be provided. If handwritten documents will be maintained, the following text can serve as a model for data entry.
All entries on the case report forms (CRFs) should be made legibly in black ink. Errors, when made, should be corrected by drawing a single line through the incorrect entry (do not erase, white-out, or tape over errors) and then entering the correct data above the original entry. Entry corrections should be initialed and dated. Explain missing data with “ND” for “not determined” and “NA” used for “not applicable.”
16.4 Study Record Retention
Specify the length of time for the investigator to maintain the records pertaining to this study. The 5 year period in the following paragraph is based on the “VCU Research Data Ownership, Retention, and Access Policy.” Research data collected for product application to the FDA may be subject to additional data retention requirements as specified by the sponsor and/or the FDA.
As applicable, study records will be maintained a minimum of 5 years beyond: (i) the publication of any abstract or manuscript reporting the results of the protocol; (2) the submission of any sponsored research final report; or (iii) submission of a final report to clinicaltrials.gov.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
17 REFERENCES
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
18 APPENDIX 1. INSERT TITLE HERE.
Add material.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

19 INFORMED CONSENT TEMPLATE
The VCU IRB Biomedical Template (rev 5-15-12) is incorporated below. You should check the IRB Web site prior to customizing the template to ensure that it is the most current version available. If a newer template is available it should be used rather than the version below.
Instructions for completion are imbedded in the document.
Language in blue below is suggested or required language from CTEP Informed Consent Template (August 2011)
TITLE:
VCU IRB PROTOCOL NUMBER:
INVESTIGATOR:
SPONSOR: [if no sponsor for this research, delete this field]
This template is based on a drug or device research study. The same elements/sections are required for other research studies (psychology, sociology, etc.). See Social-Behavioral Consent Template on VCU IRB Web site.
Instructions and comments are in italics and [ ]. Block and delete most after reading and following if needed. Find “drug name” and replace the initial use of the term with the actual generic name of the drug if it exists and any brand, chemical, or slang name you will be using later in the consent. Subsequent replacement of “drug name” may be with the generic, brand, chemical, or slang name of the drug, in a consistent manner. Find “disease name” and replace with the actual disease or condition. Delete those sections that are not applicable.
If any information contained in this consent form is not clear, please ask the study doctor or the study staff to explain any information that you do not fully understand. You may take home an unsigned copy of this consent form to think about or discuss with family or friends before making your decision.
[Include if appropriate] In this consent form, “you” always refers to the research participant. If you are a legally authorized representative, please remember that “you” refers to the study participant.
PURPOSE OF THE STUDY
[What follows are only examples. If they are not applicable, remove the language and explain the purpose of the study.]
[Option 1] The purpose of this research study is to test the safety, tolerability, and effectiveness of the drug name when used to treat disease name. You are being asked to participate in this study because you have been diagnosed with disease name, and may meet the study entry requirements.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
[Option 2] Disease causes symptoms or condition, which may involve [insert short discussion of how or why the drug might affect the disease or condition. Cannot promise efficacy or safety. Alter the wording if the study has a different purpose, for example, is limited only to safety and tolerability, no efficacy.].
DESCRIPTION OF THE STUDY
[What follows is an example. If not applicable, remove this language and provide a description of the study.]
Drug name is an investigational drug, which means it has not been approved by the U.S. Food and Drug Administration (FDA). In this study, drug name will be compared to , an approved drug, and to placebo (a look-alike inactive substance). [or other, depending on design]
Your participation in this study will last up to [insert length of time]. Approximately [insert how many] individuals will participate in this study.
Significant new findings developed during the course of the research [Insert new findings such as additional risks or discomforts] which may relate to your willingness to continue participation will be provided to you.
PROCEDURES
[If any of the treatments or procedures have not been well studied, include a statement that the treatment or procedure might involve risks to the participant, which are currently unforeseeable.]
[What follows is an example. Your narrative must include any invasive and/or non-standard procedures, and any procedures that are experimental.]
If you decide to be in this research study, you will be asked to sign this consent form after you have had all your questions answered.
At your first study visit (Visit 1), your medical history will be taken and a physical exam will be performed. This exam will include measurements of your weight and vital signs (pulse, blood pressure and temperature). Blood and urine samples will be collected for routine lab tests. Approximately 1 to 2 tablespoons of blood will be collected. [If done, mention pregnancy test at this time.]
Ex: Women of childbearing potential will have a pregnancy test done.
[If tests are done that require reporting of positive results to the Health Department (e.g., hepatitis, HIV, STDs), these must be mentioned, along with that information.]
Ex: Your blood sample will also be tested for hepatitis and HIV. Virginia state law requires the study staff to report the results of positive tests for hepatitis and HIV to a local health agency.
You will have an electrocardiogram (ECG - tracing of the electrical activity of the heart).
[If random]
You will be randomly assigned (like the flip of a coin) to receive either [insert] or [Insert]. [Can also list as bullets, if several arms]
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

You have [insert] chance in [insert] of being assigned to placebo, and [insert] chance in [insert] of receiving [insert].
[Or can say] You have an equal chance of being assigned to any one of the groups.
[If double-blind]
Neither you nor the study doctor will know which study drug (or procedure or treatment, etc.) you are receiving. This information is available to the study doctor if needed in an emergency. This is done (blinding) so that a fair evaluation of results may be made.
[If single blind] [Be sure the procedure discussion does not “blow the blind”]
You will not know which study drug you are receiving. This is done (blinding) so that a fair evaluation of results may be made.
[If visits are frequent, complicated, or involve varying activities, consider inserting a table in this section, or providing a pull out table as an appendix]
Visit 2 will take place [insert] after Visit 1. Your vital signs will be measured, and [insert]. If you qualify for the study, you will be given study drug and you will be instructed on how to take your study drug.
Visits 3 through 6 will be scheduled at [insert]. At each visit except Visit 6, your vital signs will be checked, and [insert]. You will be asked about your health since the last visit. You will receive a new supply of study drug and [insert].
Visit 6, the last visit, will include a physical exam, ECG and blood and urine samples for lab tests. You will be asked about your overall experience with the study drug.
At each visit, you should bring all of your remaining study drug supply to the research clinic.
[List tests and procedures and their frequency under the categories below. Include whether a patient will be at home, in the hospital, or in an outpatient setting.]
Before you begin the study …
You will need to have the following exams, tests or procedures to find out if you can be in the study. These exams, tests or procedures are part of regular cancer care and may be done even if you do not join the study. If you have had some of them recently, they may not need to be repeated. This will be up to your study doctor.
[List tests and procedures as appropriate. Use bulleted format.]
During the study …
If the exams, tests and procedures show that you can be in the study, and you choose to take part, then you will need the following tests and procedures. They are part of regular cancer care.
[List tests and procedures as appropriate. Use bulleted format.]
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
You will need these tests and procedures that are part of regular cancer care. They are being done more often because you are in this study.
[List tests and procedures as appropriate. Use bulleted format. Omit this section if no tests or procedures are being done more often than usual.]
You will need these tests and procedures that are either being tested in this study or being done to see how the study is affecting your body.
[List tests and procedures as appropriate. Use bulleted format. Omit this section if no tests or procedures are being tested in this study or required for safety monitoring.]
[For randomized studies:] You will be "randomized" into one of the study groups described below. Randomization means that you are put into a group by chance. A computer program will place you in one of the study groups. Neither you nor your doctor can choose the group you will be in. You will have an [equal/1 in 3/etc.] chance of being placed in any group.
If you are in group 1 (often called "Arm A") … [Explain what will happen for this group with clear indication of which interventions depart from routine care.]
If you are in group 2 (often called "Arm B")… [Explain what will happen for this group with clear indication of which interventions depart from routine care.]
[For studies with more than 2 groups, an explanatory paragraph containing the same type of information should be included for each group.]
When I am finished taking [drugs or intervention]…[Explain the follow-up tests, procedures, exams, etc. required, including the timing of each and whether they are part of standard cancer care or part of standard care but being performed more often than usual or being tested in this study. Define the length of follow-up.]
[Optional Feature: In addition to the mandatory narrative explanation found in the preceding text, a simplified calendar (study chart) or schema (study plan) may be inserted here. The schema from the protocol should not be used as it is too complex, however a simplified version of the schema is encouraged. Instructions for reading the calendar or schema should be included. See examples.]
Study Chart [Example]
You will receive [drug(s) or intervention] every [insert appropriate number of days or weeks] in this study. This [insert appropriate number of days or weeks] period of time is called a cycle. The cycle will be repeated [insert appropriate number] times. Each cycle is numbered in order. The chart below shows what will happen to you during cycle 1 and future treatment cycles as explained previously. The left-hand column shows the day in the cycle and the right-hand column tells you what to do on that day.
Cycle 1
Day What you doTwo days Get routine blood tests.
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

before starting studyDay before starting study
Check-in to _____________ the evening before starting study.
Day 1 Begin taking ______ once a day. Keep taking _____ until the end of study, unless told to stop by your health care team.
Day 2 Leave _______________ and go to where you are staying.
Day 8 Get routine blood tests.Day 15 Get routine blood tests.Day 22 Get routine blood tests.
Day 28 Get routine blood tests and exams. Get 2nd chest x-ray for research purposes.
Day 29 Return to your doctor’s office at _______ [insert appointment time] for your next exam and to begin the next cycle.
Future cycles
Day What you do
Days 1-28
Keep taking _____ once a day if you have no bad side effects and cancer is not getting worse. Call the doctor at _____________ [insert phone number] if you do not know what to do.
Get routine blood tests each week (more if your doctor tells you to). Get routine blood tests and exams every cycle (more if your doctor tells you to). Get routine X-rays, CT scans, or MRIs every other cycle (more if your doctor tells you
to).
Study Plan [Example]
Another way to find out what will happen to you during the study is to read the chart below. Start reading at the top and read down the list, following the lines and arrows.
RISKS AND DISCOMFORTS
[What follows is only an example.]
[If there are more than 3-4 side effects in a list, please present in a vertical, bulleted format for ease of reading. Also please use the non-technical meaning, rather than a medical term (ex, use “gas” instead of “flatulence”, or “weakness” instead of “asthenia”)] Ex:
Possible side effects associated with the use of drug name include:
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
Continue with study details
Start Here

headache
dizziness
sleepiness
nausea
indigestion
Allergic reaction to drug name is possible. Severe allergic reactions can be life-threatening.
[Or side effect information supplied by the sponsor]
[If any of the treatments or procedures have not been well studied in pregnant women, include a statement that the treatment or procedure might involve risks to the participant (if applicable, insert: or to the embryo or fetus, if the participant is or may become pregnant) that are currently unforeseeable.]
[Include risks and side effects for each comparator drug, if any].
[IF APPLICABLE]
[For women only studies]
As the study procedures might injure an unborn child, pregnant women may not participate. Women who might become pregnant should use a medically accepted form of birth control such as total abstinence, birth control pills, an IUD, diaphragm, progesterone injections or implants, or condoms plus a spermicide. Methods of birth control other than total abstinence are not 100% effective, and should a women become pregnant there is a risk of injury to an unborn child. For similar reasons, women who are nursing an infant may not participate.
[For studies with women and men]
As the study procedures might injure an unborn child, pregnant women may not participate. Women who might become pregnant should use a medically accepted form of birth control such as total abstinence, birth control pills, an IUD, diaphragm, progesterone injections or implants, or condoms plus a spermicide. Methods of birth control other than total abstinence are not 100% effective, and should a women become pregnant there is a risk of injury to an unborn child. For similar reasons, women who are nursing an infant may not participate.
For men, the study procedures might increase the risks for birth defects of any child conceived during treatment and several months after treatment is stopped. Men in this study who have the potential of fathering children should be aware of this possibility and consider using a medically accepted form of birth control.
[For men only studies]
For men, the study procedures might increase the risks for birth defects of any child conceived during treatment and several months after treatment is stopped. Men in this study who have the potential of fathering children should be aware of this possibility and consider using a medically accepted form of birth control. For men this would include total abstinence and condoms plus a
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
spermicide, or for the female partner, birth control pills, an IUD, diaphragm, progesterone injections or implants. Methods of birth control other than total abstinence are not 100% effective, and should a women become pregnant there is a risk of injury to an unborn child.
[List risks of other procedures if needed especially any invasive procedure (ex, if study required tympanocentesis, or endoscopy, or endometrial biopsy, etc.). Also include imaging and x-ray studies if in excess of what would be done as part of standard treatment.]
[If a treatment study, include]
Your condition may not get better or may become worse while you are in this study.
[If study drug is taken home, include]
Only the study participant can take the study drug. It must be kept out of the reach of children and persons who may not be able to read or understand the label.
While participating in this clinical trial, your study doctor advises that you stop taking all herbal products, certain dietary supplements, and any complementary or alternative medications, as these may have unexpected or bad effects on your health in combination with the experimental drugs being used in this trial. Tell all your study team and health care providers about any medications you take, including prescription drugs, over-the-counter medicines, herbal products, vitamins, dietary supplements, or complementary or alternative therapies. Give your providers a full picture of what you do to manage your health. This will help ensure coordinated and safe care. For tips about talking with your health care providers about complementary or alternative health care practices, see NCCAM’s Time to Talk campaign at http://nccam.nih.gov/timetotalk/forpatients.htm.
BENEFITS TO YOU AND OTHERS
[What follows are examples. If not applicable, remove this language and describe any benefits to the participants and others, which may reasonably be expected from the research.]
There is no guarantee that you will receive any medical benefits from being in this study.
[If not a treatment study] This is not a treatment study, and you are not expected to receive any direct medical benefits from your participation in the study. The information from this research study may lead to a better treatment in the future for people with disease name. You may benefit from the physical exams, ECGs, lab tests, and other study procedures.
[Include if appropriate] Please be aware that the investigative team and the university may receive money for the conduct of this study.
COSTS
Study drug will be provided by the sponsor. There are no charges for the study visits. [Or other list as appropriate] [If will be billed for any additional costs, need to tell them, also that insurance may not pay for research charge.]
You and/or your health plan/ insurance company will need to pay for some or all of the costs of treating your cancer in this study. Some health plans will not pay these costs for people taking
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

part in studies. Check with your health plan or insurance company to find out what they will pay for. Taking part in this study may or may not cost your insurance company more than the cost of getting regular cancer treatment.
(If applicable, inform the patient of any tests or procedures for which there is no charge. Indicate if the patient and/or health plan is likely to be billed for any charges associated with these ‘free’ tests or procedures.)
(Include the following section if a study agent is manufactured by a drug company and provided.)
The (identify study agent supplier here using the most appropriate choice of the following options: NCI, Cooperative Group, or another NCI-supported Clinical Trials Network) will supply the [study agent(s)] at no charge while you take part in this study. The (insert name of study agent supplier identified in first sentence) does not cover the cost of getting the [study agent(s)] ready and giving it to you, so you or your insurance company may have to pay for this.
Even though it probably won’t happen, it is possible that the manufacturer may not continue to provide the [study agent(s)] to the (insert name of study agent supplier identified in first sentence) for some reason. If this would occur, other possible options are:
You might be able to get the [study agent(s)] from the manufacturer or your pharmacy but you or your insurance company may have to pay for it.
If there is no [study agent(s)] available at all, no one will be able to get more and the study would close.
If a problem with getting [study agent(s)] occurs, your study doctor will talk to you about these options. (End of section)
(Include the following section if a study agent is manufactured by the NCI and provided at no charge)
The NCI will provide the [study agent(s)] at no charge while you take part in this study. The NCI does not cover the cost of getting the [study agent(s)] ready and giving it to you, so you or your insurance company may have to pay for this.
Even though it probably won’t happen, it is possible that the NCI may not be able to continue to provide the [study agent(s)] for some reason. If this would happen, the study may have to close. Your study doctor will talk with you about this, if it happens. (End of section)
PAYMENT FOR PARTICIPATION
[Only need to have if are paying, or the protocol says must inform are not paying. Use straightforward language and always include the per visit amount.]
Ex: You will be paid $_____ if you complete all scheduled study visits. If you withdraw from the study before completion, you will be paid $_____ per completed study visit. Total payments within one calendar year that exceed $600 will require the university to annually report these
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

payments to the IRS and you. This may require you to claim the compensation you receive for participation in this study as taxable income. VCU is required by federal law to collect your social security number. Your social security number will be kept confidential and will only be used to process payment.
ALTERNATIVE TREATMENT
If you decide not to enter this study, there are other treatments available. These include [List of major drugs and/or therapies]. The study doctor will discuss these with you. You do not have to participate in this study to be treated for disease name.
[If not a treatment study - Remove “Treatment” from section title and add] Your alternative is not to participate in this study.
CONFIDENTIALITY
Potentially identifiable information about you will consist of [List e.g., tissue samples, surveys, interview notes and recordings, audiotapes of consultations and interviews, and data abstracted from the medical record]. Data is being collected only for research purposes. [Note how the data will be identified, stored and protected]. Ex: Your data will be identified by ID numbers and birthdates, not names, and stored separately from medical records in a locked research area. All personal identifying information will be kept in password protected files and these files will be deleted note time frame]. Other records [Note which ones] will be kept in a locked file cabinet for [Note time frame] after the study ends and will be destroyed at that time. [Note which files] will be kept indefinitely. Access to all data will be limited to study personnel. A data and safety monitoring plan is established.
You should know that research data or (medical information if applicable) about you may be reviewed or copied by the sponsor of the research or by Virginia Commonwealth University. Personal information about you might be shared with or copied by authorized officials of the Federal Federal Drug Administration, or the Department of Health and Human Services (if applicable).
[Include this language (required by the FDA) if this study is a clinical trial] A description of this clinical trial will be available on http://www.ClinicalTrials.gov, as required by U.S. Law. This Website will not include information that can identify you. At most, the Web site will include a summary of the results. You can search this Web site at anytime.
[If research is conducted in foreign countries include the following statement:] If the research is conducted in foreign countries (where a study drug or device may be considered for approval), personal information pertaining to you may be shared or copied by authorized agents of governmental agencies in those countries.
Although results of this research may be presented at meetings or in publications, identifiable personal information pertaining to participants will not be disclosed.
DATA REGISTRIES
[Consider implementing the following layered levels of consent if a registry is being created or you will be contributing to an existing registry. Layers may not be required, although participants
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
may feel they have more control over their participation. If utilizing these layers, your registry must have provisions for respecting them.]
1. I give permission for my data/tissue samples to be stored and used for research related to [insert topic]
YES ____________________ NO ____________________
2. I give permission for my data/tissue samples to be stored and used for future research about other health problems.
YES ____________________ NO ____________________
3. I give permission for my data/tissue samples to be stored; however, I want to be contacted prior to any future use of my data/tissue samples for research.
YES ____________________ NO ____________________
GENETIC TESTING
[Only need to have if genetic testing is involved.]
[For Multicenter protocols (not initiated at VCU)]
[Include a description of the research plan with attention to the special concerns raised by genetic testing. (These concerns may be inferred from the section on VCU-initiated protocols below.) Investigators may need to modify the proposed informed consent form in order to provide this information. If participants may make choices concerning the use of their samples, these should be indicated in a check-off format (see below). Investigators should take care, however, that the modified informed consent form reflects that the actual research plan. This may be difficult if the research plan is vague.]
[For VCU-initiated protocols, the following issues should be addressed]
Background information: The research involves genetic testing. Genetic testing may reveal information about the likelihood that a person or his or her relatives may develop certain diseases. Genetic testing may reveal information about who is related to whom. If known to employers or insurance companies, the results of genetic testing might affect a person's ability to obtain a job or health or life insurance.
Current and future studies: [Consider implementing the following layered levels of consent:]
[If giving the patient this option, there must be a process in place to ensure that the choice can be complied with.]
1. My blood/tissue samples may be stored and used for future research about [insert topic].
YES NO initial initial
2. My blood/tissue samples may be stored and used for future research about other health problems (for example, heart disease, osteoporosis, diabetes, etc.)
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY

YES NO initial initial
Future contact concerning further genetic testing research: [Describe the circumstances under which participants might be contacted in the future concerning further participation in this or related genetic testing research. Consider offering the participant the option of opting out of such contacts at this time with a Yes/No response to a question formatted like those above.]
Future contact concerning genetic testing results: [If planned or possible future genetic testing results are unlikely to have clinical implications, then a statement that the results will not be made available to participants may be appropriate. If results might be of clinical significance, then describe the circumstances and procedures by which participants would receive results. Describe how participants might access genetic counseling for assistance in understanding the implications of genetic testing results, and whether this might involve costs to participants. Investigators should be aware that federal regulations, in general, require that testing results used in clinical management must have been obtained in a CLIA-certified laboratory.]
Withdrawal of genetic testing consent: [Describe whether and how participants might in the future request to have test results and/or samples withdrawn in order to prevent further analysis, reporting, and/or testing.]
Confidentiality: [Describe the extent to which genetic testing results will remain confidential and special precautions, if any, to protect confidentiality.]
COMPENSATION FOR INJURY or ILLNESS [This element is required for greater than minimal risk research as per §46.116(a)(6) and 21CFR50. It is not required, and generally not appropriate, for expedited research; no waiver of this element needs to be requested]
If you are injured by, or become ill, from participating in this study, please contact your study doctor immediately. Medical treatment is available at the Virginia Commonwealth University Health System (VCU Health System). Your study doctor will arrange for short-term emergency care at the VCU Health System or for a referral if it is needed.
Fees for such treatment may be billed to you or to appropriate third party insurance. Your health insurance company may or may not pay for treatment of injuries or illness as a result of your participation in this study.
To help avoid research-related injury or illness it is very important to follow all study directions.
VOLUNTARY PARTICIPATION AND WITHDRAWAL
Your participation in this study is voluntary. You may decide to not participate in this study. Your decision not to take part will involve no penalty or loss of benefits to which you are otherwise entitled. If you do participate, you may freely withdraw from the study at any time. Your decision to with draw will involve no penalty or loss of benefits to which you are otherwise entitled.
Your participation in this study may be stopped at any time by the study doctor or the sponsor without your consent. The reasons might include:
the study doctor thinks it necessary for your health or safety;
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
you have not followed study instructions;
the sponsor has stopped the study; or
administrative reasons require your withdrawal.
If you leave the study before the final regularly scheduled visit, [Insert any consequences of a participant’s decision to withdraw from the research (i.e., side effects of tapering off of study drug(s),condition may worsen)) and procedures for orderly termination of participation by the subject (i.e., tapering off of study drug(s), follow-up visits with study team or patient’s physician).]
QUESTIONS
If you have any questions, complaints, or concerns about your participation in this research, contact:
[Insert name and contact information of contact person for study]
and/or
[Insert name and contact information of additional contact person for study – (optional)]
[List the name of the contact person and his/her contact information here. The contact person should be a full-time faculty or staff person. More than one contact may be listed. Give name and role of primary contact first. Use bold type and larger font for names and contact information.]
The researcher/study staff named above is the best person(s) to call for questions about your participation in this study.
If you have general questions about your rights as a participant in this or any other research, you may contact:
Office of ResearchVirginia Commonwealth University800 East Leigh Street, Suite 113P.O. Box 980568Richmond, VA 23298Telephone: (804) 827-2157
Contact this number for general questions, concerns, or complaints about research. You may also call this number if you cannot reach the research team or if you wish to talk to someone else. General information about participation in research studies can also be found at http://www.research.vcu.edu/irb/volunteers.htm
Do not sign this consent form unless you have had a chance to ask questions and have received satisfactory answers to all of your questions..
CONSENT
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
[Change consent to permission if parents or legal guardian are agreeing to child’s participation. Add “My child” language as needed]
I have been provided with an opportunity to read this consent form carefully. All of the questions that I wish to raise concerning this study have been answered.
By signing this consent form, I have not waived any of the legal rights or benefits, to which I otherwise would be entitled. My signature indicates that I freely consent to participate in this research study. I will receive a copy of the consent form once I have agreed to participate.
________________________________________________Participant Name, printed
________________________________________________ ________________Participant Signature Date
[NOTE: DELETE THE PARENT OR LEGAL GUARDIAN LINES UNLESS THE STUDY ALLOWS FOR THE ENROLLMENT OF CHILDREN] 1
_______________________________________________Name of Parent or Legal Guardian(Printed)
_______________________________________________ ________________Parent or Legal Guardian Signature Date
[NOTE: DELETE THE LEGALLY AUTHORIZED REPRESENTATIV LINES UNLESS THE STUDY ALLOWS FOR THE INVOLVEMENT OF ADULTS WHO ARE UNABLE TO PROVIDE CONSENT] 2
_______________________________________________Name of Legally Authorized Representative(Printed)
_______________________________________________ ________________Legally Authorized Representative Signature Date
________________________________________________Name of Person Conducting Informed ConsentDiscussion / Witness 3
(Printed)
________________________________________________ ________________Signature of Person Conducting Informed Consent DateDiscussion / Witness
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY
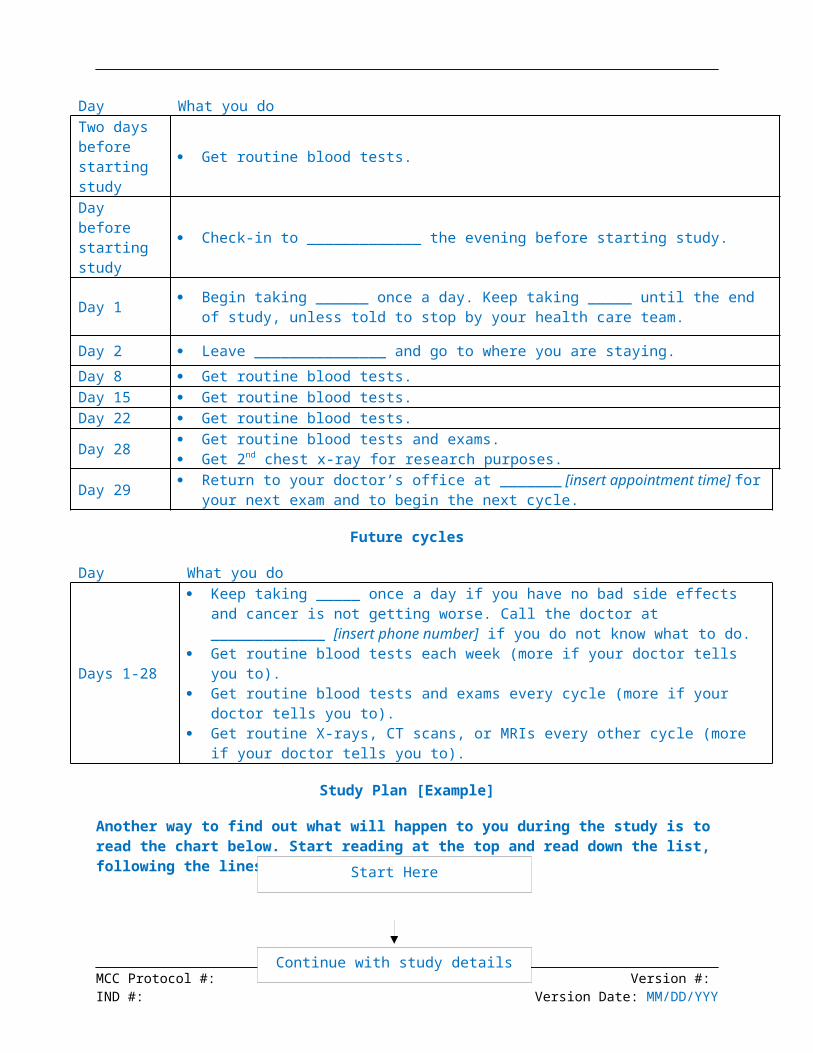
________________________________________________ ________________Principal Investigator Signature (if different from above) Date 4
1 [If the study allows for the involvement of children, the permission of BOTH parents is required for certain categories of research unless one is deceased, unknown, incompetent, or only one parent has legal responsibility for care and custody. The categories of research are: (a) research involving greater than minimal risk and no prospect of direct benefit to individual subjects, but likely to yield generalizable knowledge about the subject’s disorder or condition (45.CFR 46.406) or (b) research not otherwise approvable which presents an opportunity to understand, prevent, or alleviate a serious problem affecting the health and welfare of children. (45.CFR 46.407) Include lines for BOTH parents to print their names and lines for BOTH signatures and date if the research involves one of the two categories listed above.]
2 [If the study allows for the involvement of adults who are unable to provide consent, the consent of a legally authorized representative is required.]
3 [A witness to the signature of a research participant is required by VA Code. If the witness is to be someone other than the person conducting the informed consent discussion, include a line for the witness to print his/her name and lines for signature and date.]
4 [The purpose of this signature is to ensure that the principal investigator is aware of who has been enrolled in studies. The principal investigator’s signature date need not correspond to that of subject or witness, but should be provided after both the subject and witness have signed.]
MCC Protocol #: Version #: IND #: Version Date: MM/DD/YYY