Protein Electrophoresis 1/1 Serum Protein Electrophoresis Electrophoresis of serum proteins is a...
30
-
Upload
barnaby-wheeler -
Category
Documents
-
view
217 -
download
0
Transcript of Protein Electrophoresis 1/1 Serum Protein Electrophoresis Electrophoresis of serum proteins is a...


Protein Electrophoresis 1/1 Serum Protein Electrophoresis Electrophoresis of serum proteins is a commonly used clinical test. It provides considerable diagnostic information, especially when supplemented by complimentary tests like immunoelectrophoresis, quantitation of immunoglobulins and other specific proteins; T and B lymphocytes and lymphoblast transformation studies. Principle Ionized proteins, when placed in an electrical field, move toward the oppositely charged electrode: The relative migration depends on the protein. Using cellulose acetate, serum proteins can be separated into six fractions: albumin and five globulin groups ‑ alpha 1, alpha 2, beta (often subdivided into two distinct groups ‑ beta 1 and beta 2) and gamma. Electrophoretic separation permits study of the biological and physical characteristics of proteins.
Normal Pattern
Total Protein 6.0 ‑ 8.0 g/dL
Fraction Reference (g/dL) Reference (%)Albumin 3.2 - 5.0 58 ± 5Alpha 1 Globulins 0.1 - 0.4 3 ± 1.5Alpha 2 Globulins 0.6 -1.0 9 ± 3Beta Globulins 0.6- 1.3 14±13Gamma Globulins 0.7 - 1.5 16 ± 4

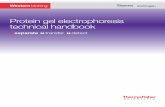
4‑AMINO ACIDS AND PROTEINS Figure 4‑12. Electrophoretic patterns typical of normal and of some pathological conditions (agarose gel). Upright and down arrows () indicate increase and decrease from the reference range, respectively. Slanting right or left arrows indicate variation from normal to an increase or from normal to a decrease from the reference range, respectively. 'Hp 2‑2 phenotype.

CAPILLARY ELECTROPHORESIS

PROTEINS OF BODY FLUIDS
A. E. FELICE M.D., Ph.D.
A: Objectives; 1. To understand normal composition of proteins in body fluids especially of plasma, urine and CSF and changes associated with disease. 2. To understand structure and function of important classes/unique proteins.
B: NOTE THAT: 1. Probably over 100,000 structural genes in DNA code for different proteins; among these 3,000 ‑ 5,000 may be expressed in different cell types (housekeeping/expressed differentiation programmes). About 300 identified in plasma (2‑D electrophoresis). 2. Major body fluids are Plasma, Urine and Cerebrospinal fluid. Plasma is Serum plus fibrinogen (and some other proteins of haemostasis. consumed in clotting.) Serum is often preferred in investigation and experimental work because high concentration of fibrinogen creates difficulties. Minor body fluids are Amniotic fluid, peritoneal and pleural fluids, tears, sweat and saliva. Minor compartments can occupy major volumes in disease (e.g. Ascites, nephroses etc.)

3. All body 'fluids contain some protein which is derived
a. by direct secretion (from liver, plasma cells, endocrine etc);
b. shedding from cell surfaces (2 microglobulin);
c. released by cellular necrosis (LDH isozymes);
d. leakages from other compartments (depend on MW/size);
e. specific transport mechanisms.
4. The protein composition of fluid compartments is not static. It may change because of;
a. developmental regulation (‑fetoprotein to albumin at 20‑30 weeks gestation);
b. physiological changes (pregnancy, endocrine status, ageing)
c. Nutrition (Alb. RBP, EPO)
d. Disease e.g. (Acute Phase Reactants and Inflammation; cellular necrosis)
e. Pharmacological agents.

5. Classes of Proteins in Body Fluids: a. Enzymes; proteases and anti‑proteasesb. Transporters; specific (Transferrin and Iron; lipoproteins and lipids) or non‑specific (Albumin and 2 macroglobulin) .c. Regulation; Hormones, Growth Factors and Cytokines.d. Protective mechanisms; Complement, Immunoglobulins, Coagulation and Fibrinolysis.e. Markers; of tissue/cell necrosis (LDH/CK and myocardial infarction, alkaline Phosphatase and bone disease; salivary LDH and periodontal disease) or of developmental anomalies (-Fetoprotein = AFP and Neural Tube Defects) or tumours (AFP, Carcino‑embryonic Antigen = CAE, Prostate Specific Antigen = PSA).
C : PLASMA PROTEINS: Plasma is obtained by separation of blood cells from blood collected with anti‑coagulant (=Ca.. chelators, Na2 EDTA/Citrate or others, Heparin = Anti‑thrombin III cofactor)
Blood collected without anti‑coagulant clots and forms serum. Cells may be separated by sedimentation under gravity. The Erythrocyte Sedimentation Rate reflects properties of cells and composition of the plasma (ESR is, increased in many inflammatory conditions. Fibrinogen may also be removed from plasma by mixing with glass beads (defibrination).

Plasma may be frozen rapidly for use as Fresh Frozen Plasma in further fractionation into blood products or as plasma expanders. The latter application is rapidly being replaced by purified Albumin solutions. Thawing of FFP results in persistence of an insoluble fraction = cryoprecipitate enriched in F8‑vWF and other coagulation factors and that can be used either directly (for vWillebrand's disease) or after further purification into F8 for haemophilia A.
Human and animal Plasma is potentially contaminated by virus (Human = Hep A, B, C, CMV and HIV; others in animals). Viral reduction procedures include heat and solvent detergent treatment. The need to sterilise must be balanced against fragility of the proteins.
Serum (foetal calf) is often included as a component of cell culture media. For many cells the serum function can be replaced by albumin, insulin or insulin like growth factors and transferrin, but this is not possible for all cell types (e.g. BFUe). Serum is used for clinical protein analysis because it is depleted of fibrinogen which otherwise confuses interpretations.
The conc. of protein in human plasma is 6 ‑ 8 g/dL; in aged and recumbent this value is down by 0.2g. Albumin accounts for 40 ‑ 60 percent of this with an Albumin to Globulin ratio of 1.2 : 1.

Hypoproteinaemia results from;
a. dilution due to salt & water retention
b. decreased biosynthesis due to liver disease
c. decreased intake of protein due to undernutrition
d. increased losses due to renal disease
e. Increased catabolism due to tumour cachexia (TNF)
Hyperproteinaemia is associated with Hyperviscosity Syndrome and results from;
a. dehydration
• increased concentration of a specific protein usually present smaller quantities e.g. monoclonal gammopathy in myeloma.
The function of plasma proteins may be considered as the properties of
a. global physical properties of a protein solution
i. rheological properties of blood flow(viscosity)
ii. osmotic properties and fluid distribution between anatomical compartments
iii. buffering at physiological pH
b. nutritional supply of amino acids.
c. function of discrete classes
d. function of specific/unique protein e.g. hemopexin/ haptoglobulin.

Synthesis is in liver, plasma cells and others. Catabolism is mainly in liver following uptake through a sialoglycoprotein receptor. A variety of physical methods can be used for quantification of individual proteins or groups of proteins with common features in diagnosis of disease as well as for preparative purification for use as therapeutics (plasma expanders, replacement therapy, immunological support). These include; 1. Temperature : Cryoprecipitate (F8‑vWF)
2. Salting Out: Albumin/Globulins = 1.2 : 1.0 ALBUMIN = 58% 1 GLOBULIN = 3% 2 GLOBULIN = 9% β GLOBULIN = 14% γ GLOBULIN = 16%
3. COHN FRACTIONATION; Temp, Ethanol, pH, Salt Conc. 4. Ultracentrifugation; Lipoproteins with different density
5. Chromatography; Ion Exchange for Albumin & IgG Immunoaffinity for F8, F9 a.o. 6. Electrophoresis; most versatile for analytical use in clinical diagnoses and follow up of disease; cellulose acetate/agarose; isoelectricfocussing.

Order of electrophoretic mobility on Agarose gel (pH = 6.4)
PROTEIN CONC. mg/dl
M.WT
KdAPR NOTES
Pre-AlbuminAlbumin
20 - 403500-5000
54.469
--
2% Tryptophan
1 Region;1 anti-trypsin1 acid gp1 Lipoprotein fetoprotein
78 - 20050 - 150170 - 3250.003
55402006.9
+++
high CHOorosomucoidD = 1.093; 1.149 = HDLmarker
2 REGION;Haptoglobulin2 MacroglobulinCaeruloplasmin
30 - 215125 - 41020 - 50
85800160
+ -
binds Hbnephrotic syndrome Cu, Wilson's Disease
1 REGION;Transferrin lipoprotein
200 - 35060 - 155
773,000
- Iron transport - Anaemia
VLDL=0.98-1.002,LDL=1.03
2 REGION;Fibrinogen2 microglobulin
200 - 4000.1 - 0.2
340 12
+
coagulation/fibrinolysisrenal tubular function
REGION;Ig GIg AIg MC Reactive Protein
525- 1650 40 - 390 25 - 310<0.8
160 170120120
pl = 6.3 - 7.3 inflammation

Different electrophoretograms arise from; 1. monoclonal disease (multiple myeloma; gammopathies). 2. genetic variants (albumin; agamaglobulinaemia). 3. drugs binding albumin. 4. increased conc of a normal protein not usually seen (transferrin in iron deficiency anaemia) . 5. acute phase reactants (decreased albumin ; increased Ig, a.o. ‑ see below). 6. typical patterns associated with specific disease. 7. endocrine status (glucocorticoids ‑ lipoprotein; androgen ‑ haptoglobulin; oestrogen ‑ caeruloplasmin). D.THE ACUTE PHASE REACTION: The acute phase reaction is a non specific marker of disease and results from acute inflammation; surgery/trauma, infarction, infection or tumours. It is mediated by small peptides released at the site. The levels of individual APR proteins change at different rates; this is useful to monitor the progress of disease or the response to treatment; Rapid APR (<12 hr); C‑Reactive Protein, 1 antichymotrypsinogen + Intermediate APR (about 12 hr); 1 acid glycoprotein, 1 anti‑trypsin, haptoglobulin, C4, Fibrinogen + Late APR; C3, caeruloplasmin. ‑ APR; Albumin & pre‑Albumin, Transferrin & ‑lipoprotein.

E. (SELECTIVE) REVIEW OF SPECIFIC PLASMA PROTEINS:
Pre‑Albumin (PA) & Retinol Binding Protein (RBP);
Both migrate ahead of albumin, they are synthesized in the liver and have short half lives. RBP is 2% tryptophan an essential amino acid. Thus RBP is a very sensitive indicator of protein nutrition. Both are transport proteins; PA binds T3 and T4. it forms a 1:1 complex with RBP which is displaced by the RBP ligand, Vit A. Zn is necessary for biosynthesis of RBP.
Albumin; replaces a fetoprotein after 20th week of gestation as major plasma protein. Synthesized in liver, no storage form. It is taken up by pinocytosis into many cell types to provide amino acids for biosynthesis.
Functions in transport of many physiological and pharmacological ligands. Contributes in a major way to physical properties of plasma/serum (viscosity, osmolality etc).
Less than 150 mg lost in urine per day (microalbuminuria). Increased levels of glycated albumin are found in Diabetes.

1 anti‑trypsin; is an APR with anti‑protease activity targeted against neutrophil elastase and collagenase, thus protects tissue in lung and liver in the course of inflammatory infiltration. Congenital deficiency is associated with emphysema in lung and cirrhosis in liver. The enzyme is polymorphic with three common alleles, M, Z and S. MM is the wild type with 100% activity; SS has intermediate activity (=60%) and ZZ is least active ( = 15%). Heterozygotes for any of these alleles have intermediate levels of activity. A modified enzyme is available for replacement therapy. 1 Acid Glycoprotein; also known as orosomucoid is glycated for 45% of M.W. AAG is a + APR and a tumour marker. AAG plays some role in inflammation, drug binding and inactivation, and in Prostaglandin transformations foetoprotein; is the major plasma protein up to about 30 weeks of gestation after which it is replaced by albumin. Elevated levels in adults may be a marker of cytogenetic disorders, (congenital) neural tube defects or a malignancy. Haptoglobulin; is a + APR that binds free plasma Hb which is released from RBC following intra‑vascular haemolysis (Hb is nephrotoxic). Thus tissues are protected from toxic effects of extra‑erythrocytic Hb, and amino acids as well as iron are preserved for recycling through biosynthesis. HAP binds Hb irreversibly via the Hb subunits. The plasma HAP may take up to 3 g Hb into the RES. Synthesis is in liver.

HAP is a tetramer composed of two pairs of unlike polypeptides designated and held together by disulphide bonds (unlike Hb). The subunit is polymorphic with three alleles; 1s/2f (s = slow. f = fast) and 2. Consequently, there are three HAP phenotypes:
The HAP 1‑1 phenotype is associated with 21S2 or 21f2
The HAP 2‑2 phenotype is associated with 1(s/f)22
The HAP 2‑2 phenotype is associated with 222
Frequency: HAP 1‑1 > 2‑1 > 2‑2.
2 Macroglobulin; is a large protease inhibitor with apparent specificity for large substrates. Levels are increased in pregnancy and by oestrogen. Urinary losses occur late in the progression of glomerular disease as proteinuria becomes less selective. AMG has ill defined roles in immunology and inflammation.
Caeruloplasmin; is a late APR composed of 7 moles of Copper per mole of protein. Caeruloplasmin incorporates copper in hepatocytes and carries it to several cells from which it is recovered after internalization. It is not in this sense a true Copper transport protein. Caeruloplasmin has properties of an oxidase.
Hereditary deficiency results in Wilson's disease with copper accumulation in liver and other tissues.
Transferrin (TRF); is a ‑ APR and the principal iron transport molecule in plasma (measured as SI = serum iron) where it binds 2 FeIII and one HC03
‑ on each molecule. Synthesized and secreted from liver
depending on availability of iron. Iron deficiency results in increased TRF and thus of Total Iron Binding Capacity (=TIBC) with decreased iron saturation = SI /TIBC. Iron is transported to Ferritin stores.

2 micro globulin; M.Wt. = 12,000. BMG is present on the surface of nearly all nucleated cells as part of the HLA complex and from where it is shed into plasma. Because of its small size, BMG is easily filtered through GMB but less than 1 % is excreted in urine due to effective tubular reabsorption. BMG elevations in plasma may accompany certain forms of leukaemia.
C‑Reactive protein (CRP); is the most sensitive + APR. It binds the C polysaccharide of the wall of S. pneumoniae. It is closely related to a form of serum amyloid.
Amyloid; is a translucent and structureless proteinaceous deposit which stains like starch. It is derived from plasma proteins by unknown processes. It has a fibrillar component with pleated sheaths that are resistant to proteolysis and insoluble. Various types are known; some of which are hereditary.
F. PROTEINS IN URINE:
Less than 150 mg of protein are excreted per day in urine. most of this is albumin (microalbuminuria) with small amounts of Tamm Horsfall Protein secreted from the distal tubules and which precipitate as casts. The protein/creatinine index is a better parameter to monitor the degree of proteinuria.
The initial stages of glomerular disease are characterized by a selective proteinuria; i.e. proteins of lower molecular weight. As disease advances, larger MW proteins (AMG) appear.
G. PROTEINS IN CSF: Over 80 % of protein in CSF is an ultrafiltrate of plasma with LMW proteins predominating. Very small amounts are synthesized intrathecally.


The characteristic appearance of the albumin fraction depends on its biochemical homogeneity. Albumin is a serum protein with a molecular weight around 70,000 daltons and an isoelectric point of 4.7. Its low molecular weight confers on it the property of migrating most anodally. Albumin forms complexes with many proteins, permitting transport of calcium and biliary pigments. Albumin plays a major role in main taining blood volume and osmotic pressure. Electrophoresis of serum proteins separates four groups of globulins with molecular weights much greater than albumin. Alpha and beta globulins are also transport proteins. They combine with pigments, metals, carbohydrates, and lipids. These proteins are very heterogeneous; their molecular weights range from 40,000 to over 1,000,000 daltons. Gamma globulins, or immunoglobulins, have molecular weights from approximately 150,000 daltons to more than 1,000,000 for IgM. Immunoglobulins play an essential role in the immune defense system, providing antibodies needed for immune response to bacteria, viruses and toxins.

1 ‑ Acute Inflammation
The rapid breakdown of tissue is frequently found in acute inflammation and is characterized by localized biochemical response (activation of complement) and by cellular response (mobilization of phagocytes, increased synthesis of proteins).
Clinical findings in acute inflammation include:
- fever, resulting from the release of toxic substances that stimulate the central nervous system
‑ elevated erythrocyte sedimentation rate, increased levels of alpha 1 and alpha 2 globulins and fibrinogen
‑ leukocytosis, following phagocytic activity
- increased level of acute phase proteins, such as alpha 1 antitrypsin, orosomueeid, haptoglobin, C reactive protein, alpha 2 macroglobulin and ceruloplasmin
Increased acute phase proteins are seen in the following disorders:
‑ acute infection (bacterial, viral or parasitic)
‑ trauma of all sorts (mechanical, physical, chemical, etc.) resulting in tissue damage (contusions, surgery, thrombosis, etc,)
‑ cardiac failure
‑ metabolic coma (uremia, shock, etc.)

Increased acute phase proteins are seen in the following disorders: ‑ acute infection (bacterial, viral or parasitic) ‑ trauma of all sorts (mechanical, physical, chemical, etc.) resulting in tissue damage (contusions, surgery, thrombosis, etc,) ‑ cardiac failure ‑ metabolic coma (uremia, shock, etc.) Subacute Inflammation This condition represents an intermediate stage between the two possible courses of acute inflammation: total convalescence with a return to normal or the onset of a chronic inflammatory condition. Severe, acute inflammation is characterized by a massive increase of all acute phase proteins. When recovery begins, there is a characteristic decrease, followed by a return to normal of the alpha 1 globulins (orosomucoids and alpha 1 antitrypsin), complement (beta 1A‑beta 1C globulin) and albumin. The beginning of the immune response is marked by a slight, generally selective, increase in gamma globulins (particularly IgA). Alpha 2 globulins may remain more or less elevated (particularly haptoglobin). C reactive protein disappears or remains at a low level.

Chronic inflammatory conditions are associated with increases of certain proteins referred to as "chronic phase proteins". Electrophoretically, this response is seen as a slight to moderate increase in the alpha 2 globulins and slight increase in the beta globulins (primarily due to complement). Albumin may be slightly suppressed with a polyclonal increase of gamma globulins. Chronic phase proteins are seen in the following disorders: - chronic infections (brucellosis, tuberculosis, Hodgkin's Disease, etc.) - collagen or connective tissue disease - allergies - malignancies - autoimmune disorders
2 ‑ Chronic Inflammation

3 ‑ Liver Disease
Since the liver is the site of albumin and alpha globulin synthesis, diseases affecting this organ can be expected to affect in vivo levels of albumin and alpha globulin. The liver, however, has considerable reserve synthesis capability, and decreased albumin levels are seen only in advanced hepatocellular disease. Below are major hepatic problems and the associated serum protein electrophoresis patterns: ‑ acute viral hepatitis: increased levels of IgG and IgM ‑chronic liver disease (including cirrhosis): marked increased of IgG, IgM and IgA with a decrease of albumin and transferrin ‑ biliary destruction: increased levels of C, and beta lipoprotein.

4 ‑ Nephrotic Syndrome
The loss of large quantities of albumin from the kidneys is consistent with nephrotic syndrome. This syndrome can be caused by diabetes mellitus, connective tissue disease, glomerular disease and circulatory disease.
It is characterized by:
- hypoproteinemia
- hypoalbuminemia
- edema
- hyperlipidemia
- proteinuria
Albumin and other low molecular weight proteins (transferrin and alpha 1 antitrypsin) are lost through the glomerular tubules. There is an associated increase in certain large molecular weight proteins (macroglobulin, IgM, lipoproteins). The electrophoresis pattern may be mimicked by acute inflammatory conditions associated with increased alpha 1 and alpha 2 globulins.

5 ‑ Hypogammaglobulinemia and Agammaglobulinemia
Hypogammaglobulinemias are characterized by decreased amounts of most or all immunoglobulins. The majority of deficiencies are hereditary and manifest in infancy (Wiskott‑Aldrich syndrome, Breton's dis ease, ataxia telangiectasia).
Immunoglobulin deficiencies acquired in adulthood can be secondary to disease states, such as mono clonal gammopathies, or induced by immunosuppresive therapy. Bence Jones proteins are frequently found in adults with hypogammaglobulinemia. Immunoelectrophoresis or immunofixation electrophoresis (IFE) should be performed to detect and identify monoclonal gammopathies.
Decreases can also involve selective immunoglobulin classes like IgA, sub‑classes (IgG„ IgGz, IgG„ IgG,, IgA,, IgA,), or selective light chain deficiency of kappa or lambda type.

6 ‑ Monoclonal and Biclonal Gammopathies
Monoclonal Gammopathies
Monoclonal gammopathies represent disorders of immunoglobulin synthesis associated with proliferation of clones of B lymphocytes. Electrophoresis shows one homogeneous peak (corresponding to the paraprotein) in the beta‑gamma area (sometimes in the alpha 2 area), and is generally associated with decreases in normal immunoglobulins. These homogeneous paraproteins are formed from a single type of heavy chain that filters through the glomerular tubules and forms Bence Jones proteins (free light chains).

8 ‑ Protein Losing Gastroenteropathies
Excessive gastrointestinal loss of albumin and other proteins is seen in a variety of gastrointestinal disorders. Proteins are affected to various degrees in relation to the severity of the protein losing disorder.
Protein losing enteropathies are generally secondary to pathophysiological conditions (such as those related to lymphatic abnormalities, e.g. secondary to increased blood pressure in patients with constrictive pericarditis) or to congenital abnormalities (as in primary intestinal lymphangiectasis). Decreased serum albumin may also be secondary to mucosal disease or from direct loss of serum into the intestines, as in inflammatory bowel disease.
Electrophoresis results are best when supplemented by complementary investigations, like IEP or IFE when a monoclonal or biclonal gammopathy is present. Quantitation of specific immunoglobulins is also recommended. A variety of techniques are used: radial immunodiffusion, Laurell electroimmunodiffusion, nephelometry, etc. Protein quantitation permits establishment of "a protein profile" that can be associated with certain pathologic conditions.

9 ‑ Decreased Levels of Alpha 1 Antitrypsin
Congenital Alpha 1 Antitrypsin Deficiency
Approximately 95% of all individuals have a serum alpha 1 antitrypsin concentration of 200 to 400 mg/dL. Certain hereditary abnormalities involve deficiencies in the synthesis of this globulin. In heterozygous individuals, alpha 1 antitrypsin levels are decreased to 30 ‑ 50% of normal levels. In homozygous individuals, the alpha 1 antitrypsin level varies according to ethnic group and can be decreased as much as 80 to 90%. Homozygous individuals are predisposed to pulmonary emphysema.
Acquired Alpha 1 Antitrypsin Deficiencies
Acquired deficiencies are seen in severe nephrotic syndrome due to urinary loss of this low molecular weight protein and in liver disease.

Alpha 1 antitrypsin phenotyping is essential for precise diagnosis of alpha 1 antitrypsin deficiencies. Phenotyping can be done by two dimensional immunoelectrophoresis or by isoelectrofocusing in polyacrylamide gel with comparison to a reference of known phenotype.
In a study of patients over the age of 70, only 8% of serum or urine monoclonal gammopathies were pathological. The majority of these monoclonal gammopathies remained benign. High monoclonal protein levels and decreased levels of other immunoglobulins may be associated with a malignancy.
Biclonal Gammopathies
Occasionally, the presence of two (and very rarely three) monoclonal proteins can be observed. Observance of these paraproteins by electrophoresis is not sufficient for complete identification. Immunoelectrophoresis (IEP) or the newer technique of immunofixation (IFE) must be performed. Immunofixation electrophoresis consists of agarose gel electrophoresis followed by immunoprecipitation by direct application of specific antisera.


Polyclonal gammopathies are characterized by broad, diffuse increases in the gamma region of the serum protein electrophoresis pattern. The three major immunoglobulins (IgG, IgA, IgM) are usually increased in variable relative concentrations. After hypoalbuminemia, polyclonal gammopathy is the most common protein abnormality seen. Continued evaluation of polyclonal patterns has some prognostic value. For example, clinical improvement in a primary disease state is marked by a decrease of the gamma fraction. Polyclonal gammopathies are seen in a number of disorders including:
- chronic liver disorders - collagen disorders - chronic infections - metastatic carcinoma - cystic fibrosis - thermal burns during recovery stage
7 ‑ Polyclonal Gammopathies