
Protecting the most vulnerable: IPC in the neonatal … · Protecting the most vulnerable: IPC in...
33
Fakulteit Gesondheidswetenskappe Faculty of Health Sciences Protecting the most vulnerable: IPC in the neonatal nursery Dr Angela Dramowski ([email protected]), Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa ICAN Harare 2014
Transcript of Protecting the most vulnerable: IPC in the neonatal … · Protecting the most vulnerable: IPC in...
Fakulteit Gesondheidswetenskappe
Faculty of Health Sciences
Protecting the most vulnerable:
IPC in the neonatal nursery
Dr Angela Dramowski ([email protected]), Paediatrics and Child Health,
Stellenbosch University, Cape Town, South Africa
ICAN Harare 2014
Overview
• Why are neonates particularly vulnerable to HAI?
• Which organisms cause outbreaks in NNU?
• HAI outbreaks in NNU in South Africa
• Neonatal outbreaks & bloodstream infections over 6 years at
Tygerberg Children’s Hospital, Cape Town
• What can we do in Africa to reduce HAI rates in newborns?
Why are neonates vulnerable to HAI?
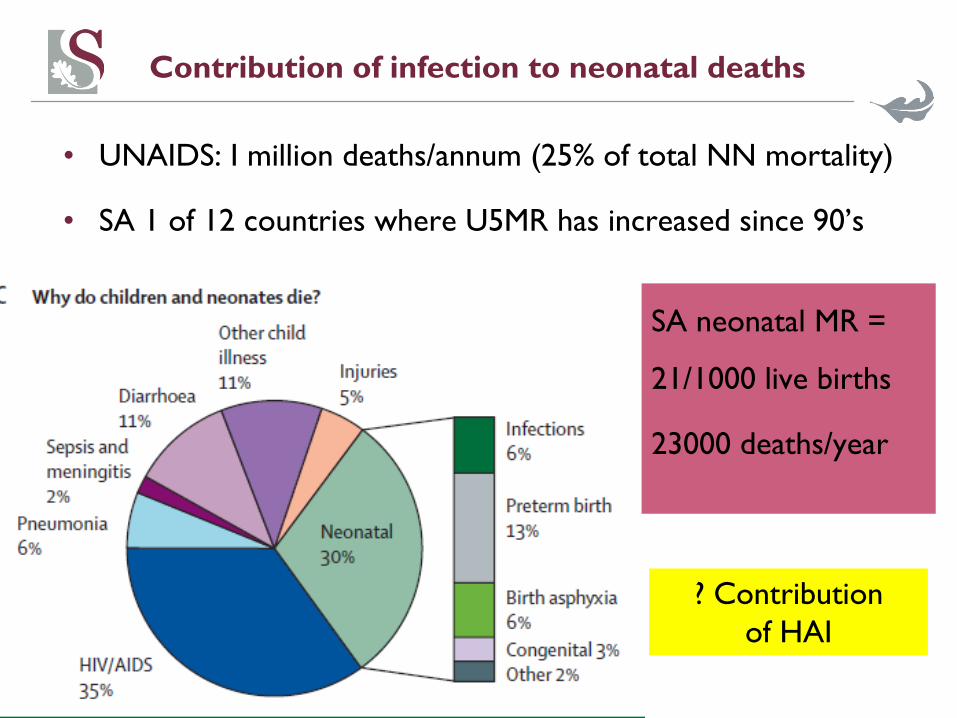
Contribution of infection to neonatal deaths
• UNAIDS: I million deaths/annum (25% of total NN mortality)
• SA 1 of 12 countries where U5MR has increased since 90’s
4
SA neonatal MR =
21/1000 live births
23000 deaths/year
? Contribution
of HAI
Which organisms cause outbreaks in NNU?
• Bacteria
- Klebsiella pneumonia, E coli (ESBL)
- Acinetobacter baumanni, Pseudomonas aeruginosa
- Staphylococcus aureus incl. MRSA
- Emerging pathogens: Serratia marcescens
• Viruses
- Rota virus, Noro virus
- RSV, parainfluenza, influenza
• Fungi
- mostly Candida spp
(Risk factors: low birth weight, broad spectrum antibiotics, central lines)

Outbreaks in Neonatal Nurseries
• a vulnerable population
• exposure to infections- in utero or postnatally
• HCW, parents, patients, hospital environment, equipment
• ID exposures microbial colonisation
infectious morbidity and mortality
nosocomial outbreaks
• high risk of outbreaks:
• overcrowding
• understaffing
• sharing and reuse of equipment
Enterobacter outbreak - Pelonomi FS 2004
Dirty hands... and six babies die
March 25 2004 at 04:45pm
A pharmacy assistant's dirty hands were the main reason why six babies died earlier this month in the Pelonomi Hospital in Bloemfontein.
Dr Victor Litlhakanyane, head of the Free State health department, said on Thursday that the assistant who prepared foodstuffs for the babies had washed his hands in a dirty basin.
"The results of forensic post mortem tests showed the babies died from septicaemia caused by Enterobacter bacteria. This caused the babies' organs to bleed, which led to their death
Klebsiella outbreak - Mahatma Ghandi KZN 2005
• Contaminated IV fluids
• Multi use of IV’s to limit cost
• Inadequate handwashing
• Understaffing

Norovirus outbreak – Charlotte Maxeke GP 2009
Contributing factors:
• Overcrowding
• Insufficient facilities &
equipment
• Poor IC practice
Recommendations:
• Support hospital managers
to encourage IC & QA
• In-service training of staff
Epidemic Gastroenteritis outbreak:
Sunday 16 May 2009 – cluster of 17
neonates with vomiting & diarrhoea –
7 deaths
Investigation yielded norovirus
Highly infectious GI virus
Contact and droplet spread
Source unknown - ? HCW/mother/visitor

10
Case study Acta Paediatrica, 2006; 95: 535-539
• 3 month old baby in Paeds ICU
• no household TB exposure
• ex-prem nursed in KMC ward for 3 weeks
• mother recalled sharing room with another
mom who looked ill & coughed continuously
• traced potential adult source case
• confirmed smear + pTB
• identical molecular fingerprint
• Of 8/11 infant contacts traced,
• 4/8 (50%) had TB Rx < 6months after KMC
• No known community TB contacts
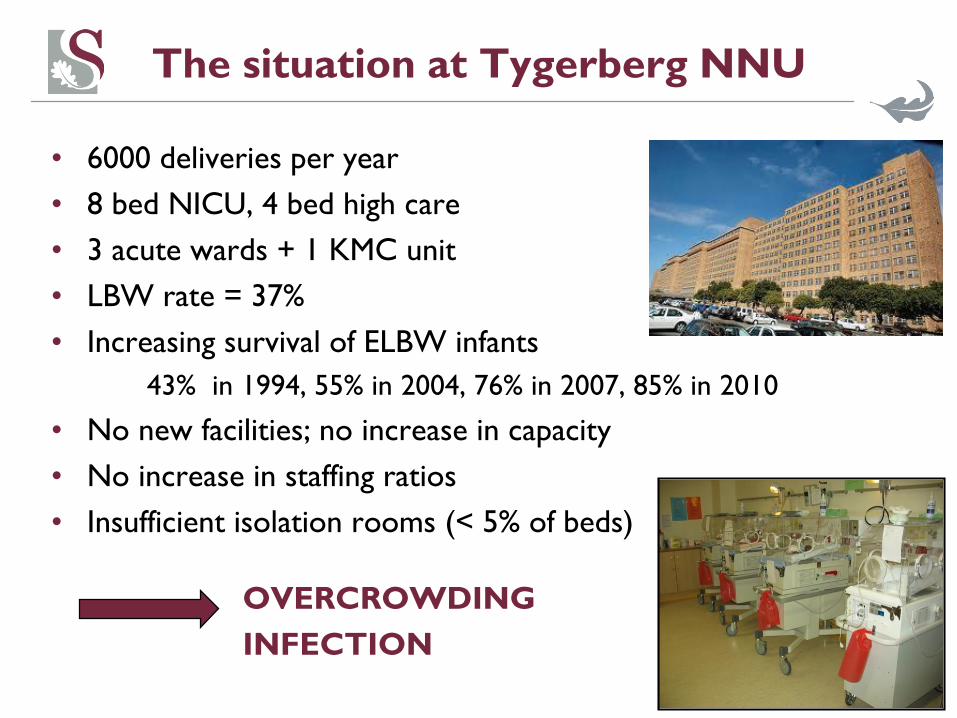
The situation at Tygerberg NNU
• 6000 deliveries per year
• 8 bed NICU, 4 bed high care
• 3 acute wards + 1 KMC unit
• LBW rate = 37%
• Increasing survival of ELBW infants
43% in 1994, 55% in 2004, 76% in 2007, 85% in 2010
• No new facilities; no increase in capacity
• No increase in staffing ratios
• Insufficient isolation rooms (< 5% of beds)
OVERCROWDING
INFECTION
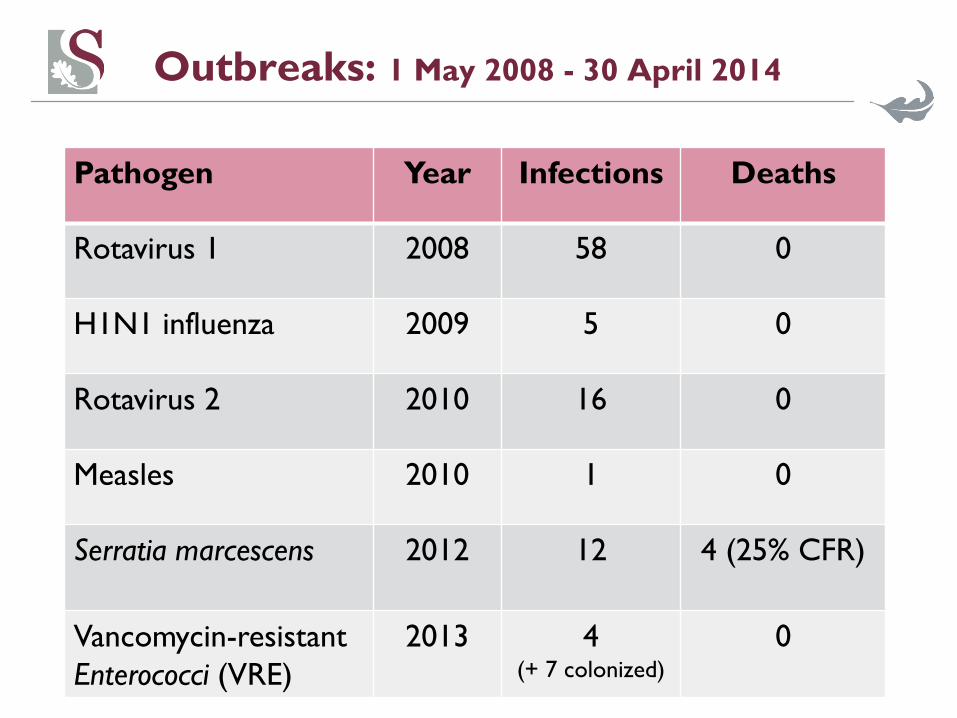
Outbreaks: 1 May 2008 - 30 April 2014
Pathogen Year Infections Deaths
Rotavirus 1 2008 58 0
H1N1 influenza 2009 5 0
Rotavirus 2 2010 16 0
Measles 2010 1 0
Serratia marcescens 2012 12 4 (25% CFR)
Vancomycin-resistant
Enterococci (VRE)
2013 4(+ 7 colonized)
0
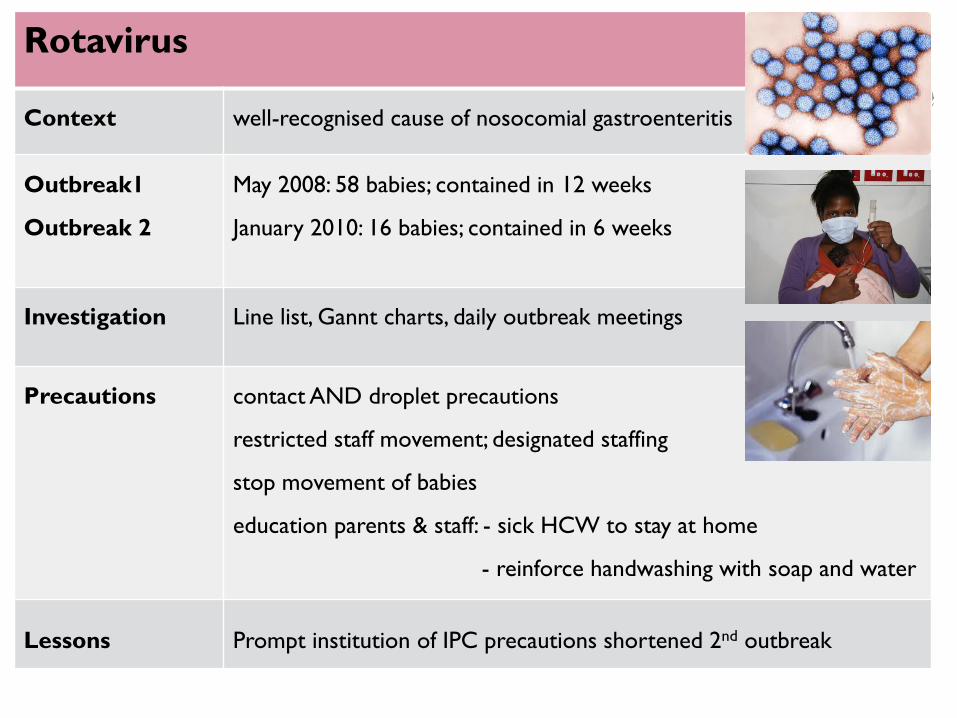
Rotavirus
Context well-recognised cause of nosocomial gastroenteritis
Outbreak1
Outbreak 2
May 2008: 58 babies; contained in 12 weeks
January 2010: 16 babies; contained in 6 weeks
Investigation Line list, Gannt charts, daily outbreak meetings
Precautions contact AND droplet precautions
restricted staff movement; designated staffing
stop movement of babies
education parents & staff: - sick HCW to stay at home
- reinforce handwashing with soap and water
Lessons Prompt institution of IPC precautions shortened 2nd outbreak

H1N1 influenza
Context Pandemic H1N1 (>12000 cases in SA; 91 deaths in 2009)
TBH situation Additional ventilator beds/wards opened (obstetrics)
TCH: 26 paeds cases; 1 child died from multi-organ failure
Neonates 5 infected; 4 prophylaxis (all LBW/premature), all survived
Precautions Droplet precautions, cough etiquette, hand hygiene compliance
Cohort isolation
Visitor restriction & excluded ill staff members
Oseltamivir to exposed and infected neonates
Lessons Need for better isolation facilities
Need for staff and high-risk patient immunisation
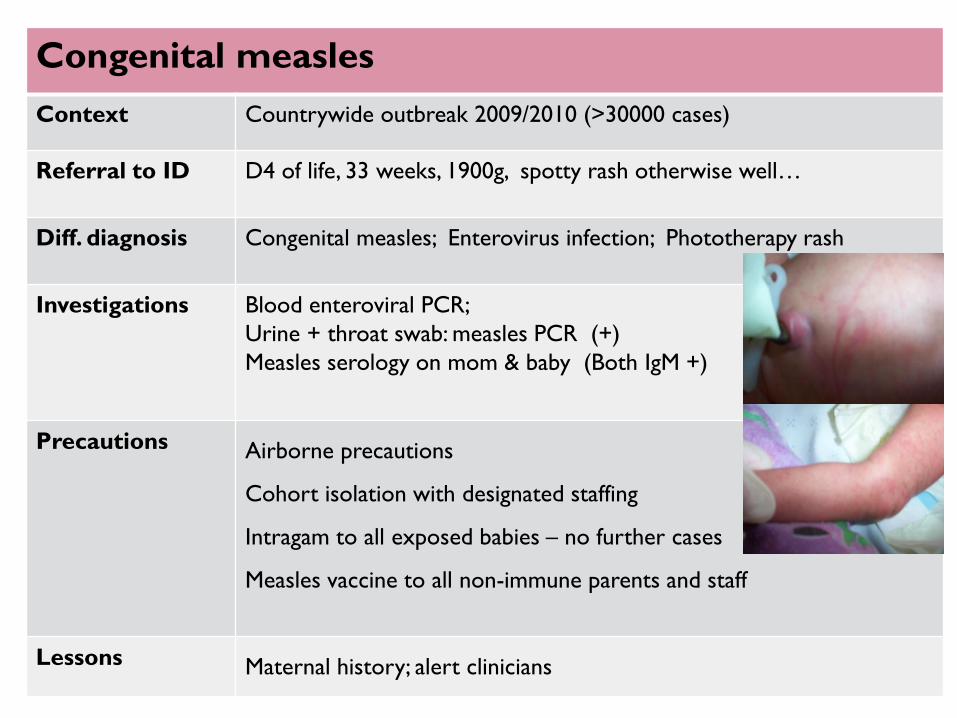
Congenital measles
Context Countrywide outbreak 2009/2010 (>30000 cases)
Referral to ID D4 of life, 33 weeks, 1900g, spotty rash otherwise well…
Diff. diagnosis Congenital measles; Enterovirus infection; Phototherapy rash
Investigations Blood enteroviral PCR;
Urine + throat swab: measles PCR (+)
Measles serology on mom & baby (Both IgM +)
Precautions Airborne precautions
Cohort isolation with designated staffing
Intragam to all exposed babies – no further cases
Measles vaccine to all non-immune parents and staff
Lessons Maternal history; alert clinicians
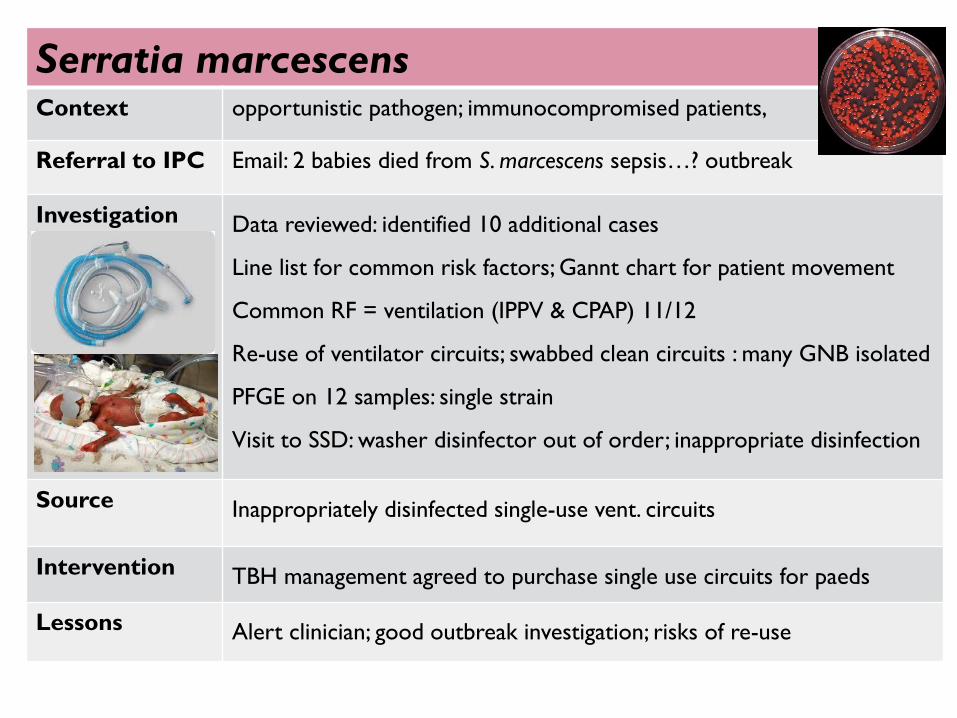
Serratia marcescensContext opportunistic pathogen; immunocompromised patients,
Referral to IPC Email: 2 babies died from S. marcescens sepsis…? outbreak
Investigation Data reviewed: identified 10 additional cases
Line list for common risk factors; Gannt chart for patient movement
Common RF = ventilation (IPPV & CPAP) 11/12
Re-use of ventilator circuits; swabbed clean circuits : many GNB isolated
PFGE on 12 samples: single strain
Visit to SSD: washer disinfector out of order; inappropriate disinfection
Source Inappropriately disinfected single-use vent. circuits
Intervention TBH management agreed to purchase single use circuits for paeds
Lessons Alert clinician; good outbreak investigation; risks of re-use
Vancomycin-resistant Enterococci (VRE)
Context immunocompromised patients, surgical procedures
Referral to IPC 2 cases of VRE in the NICU (CLABSI)
Investigation 2 rounds of rectal screening in NICU, 1 month apart
Initial 3/19 colonized (16%) increasing to 8/12 (67%)
Ongoing transmission despite contact precautions + staff education
2 babies went to operating theatre – no communication of risk
Source Uncertain, propagated by poor hand hygiene
Intervention Education!! Adherence to HH and contact precautions
Lessons Need for better communication and more education
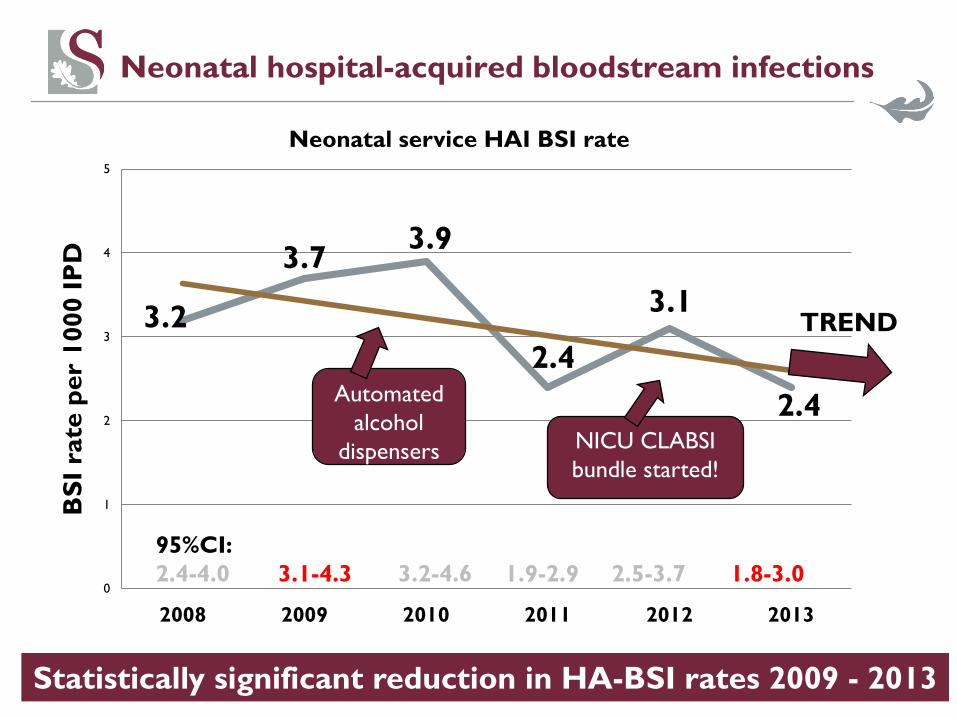
Neonatal hospital-acquired bloodstream infections
3.2
3.73.9
2.4
3.1
2.4
0
1
2
3
4
5
2008 2009 2010 2011 2012 2013
BS
I ra
te p
er
1000 I
PD
Neonatal service HAI BSI rate
TREND
NICU CLABSI
bundle started!
95%CI:
2.4-4.0 3.1-4.3 3.2-4.6 1.9-2.9 2.5-3.7 1.8-3.0
Statistically significant reduction in HA-BSI rates 2009 - 2013
Automated
alcohol
dispensers

Endemic bacteraemia: the big four!
1. Klebsiella spp 1.84
2. Serratia marcescens 0.62
3. Acinetobacter spp 0.58
4. MRSA 0.43
(BSI per 1000 IPD)

Endemic bacteraemia: organism profilesB
SI
rate
per
1000 I
PD SERRA
PSEUD
MRSA
KLEB
ENTER
ACINE
2012
Serratia
outbreak

Resistance profiles
MSSA = Methicillin sensitive Staphylococcus aureus
MRSA = Methicillin resistant Staphylococcus aureus
ESBL = extended spectrum B-lacatamase producer
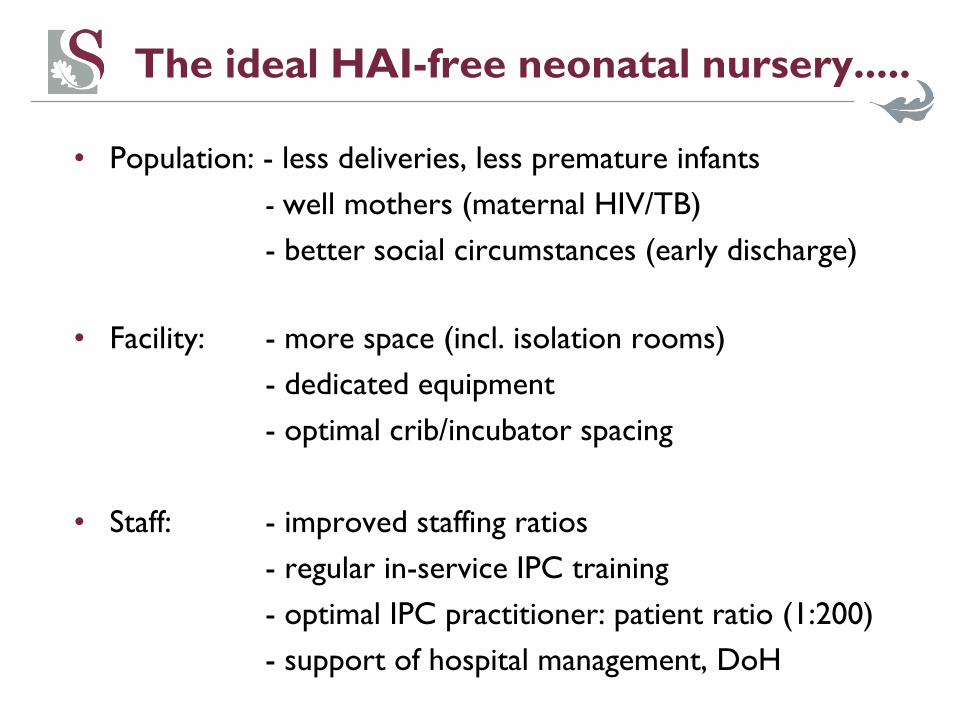
The ideal HAI-free neonatal nursery.....
• Population: - less deliveries, less premature infants
- well mothers (maternal HIV/TB)
- better social circumstances (early discharge)
• Facility: - more space (incl. isolation rooms)
- dedicated equipment
- optimal crib/incubator spacing
• Staff: - improved staffing ratios
- regular in-service IPC training
- optimal IPC practitioner: patient ratio (1:200)
- support of hospital management, DoH

One can only dream…
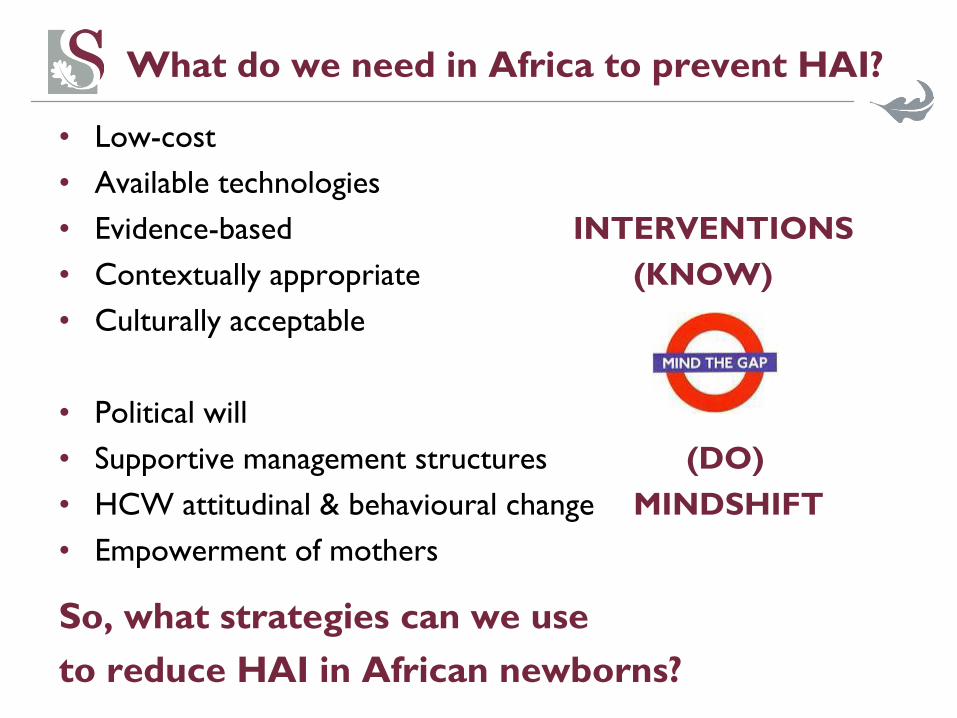
What do we need in Africa to prevent HAI?
• Low-cost
• Available technologies
• Evidence-based INTERVENTIONS
• Contextually appropriate (KNOW)
• Culturally acceptable
• Political will
• Supportive management structures (DO)
• HCW attitudinal & behavioural change MINDSHIFT
• Empowerment of mothers
So, what strategies can we use
to reduce HAI in African newborns?
25
Kangaroo Mother Care
• Skin to skin contact
• Thermo-stable
• Bonding
• Ease of breastfeeding
• Facilitates early discharge
• Decreases burden on nursing staff
• Opens up space for acutely ill neonates
• Decreased mortality & morbidity
from NEC, sepsis, pneumonia

Breastmilk
• 2010 WHO revised infant feeding guidelines
• SA again advocating breastfeeding for HIV-exposed infants
• Use flash or Pretoria pasteurisation of HIV+ mom’s EBM
• Where EBM not available use donor EBM
• Need strict SOP for management of EBM & DBM
• Outbreaks often associated with formula feeds
• Breastfeeding = decreased incidence & mortality
from gastroenteritis & pneumonia
Nasal CPAP
• Relatively cheap & widely available
• Minimal training required – suitable for Level 1 hospitals
• Can be used with in-out surfactant for ELBW
• Avoids risk of ventilator associated pneumonia
• Decreases bed pressure on NICU facilities & referral hospitals

Hand hygiene
• KNOW DO
• Low compliance globally – especially doctors!
• Lack of basins, soap, towels, water ?!?
• Personal alcohol handrub
• Bare below the elbows
• Improvement with re-training and feedback ? sustainability
Staffing
• All categories remain understaffed
• Nurses fulfil additional functions eg portering, cleaning
• High staff turnover; use of agency nurses to fill the gaps
• Often work in multiple clinical areas; often lack accountability
• BUT - very willing to learn
- safety-focused
- passionate about neonates
- willingness to work with link nurses/nurse educators
Facility Management – partners in IPC
• Sometimes adversarial relationship with staff
• Lack of insight into IPC priorities
• All about saving costs
• BUT willing to listen and assist!
“We need to train our managers to understand the basic
economics of infection control – the fewer infections the less cost
to health services. Investment in IC pays high dividends.”
Shaheen Mehtar
Political Will
• Recognition of the integral role of IPC in health services
• IPC one of the top priorities listed by Dr Motsoaledi
• Launch of the National Core Standards in South Africa
• In SA baseline audit only 50% national ave. IPC compliance
• IPC should capitalise on this momentum
(together with importance of IPC highlighted by Ebola)
32
Good IPC = vulnerable newborns to thriving babies
Acknowledgements
• Dr Theuns Avenant
• Dr Adrie Bekker
• Prof Ben Marais
• Colleagues at TCH
• Mothers & babies of TCH


















