Prosthetic restoration of the canine - jdao-journal.org · Prosthetic restoration of the canine...
21
Prosthetic restoration of the canine Pascal AUROY, Jean LECERF ABSTRACT There are many ways dentists can restore teeth prosthetically. Depending on its condition of relative integrity or more serious breakdown and the patient’s loss of other teeth, the practitioner can choose from a variety of quite different procedures ranging from the fabrication of a single ceramo-ceramic crown on a vital tooth to correction of considerable loss of teeth with an implant supported bridge. This paper will evaluate most of these treatment modalities and, in addition to purely prosthetic considerations, will discuss the integration into treatment of periodontal, implant, occlusal, and functional concepts. KEYWORDS Prosthesis Dental occlusion Oral rehabilitation Canine. Address for correspondence: P. AUROY, J. LECERF, 2 place Pasteur, 35000 Rennes. [email protected] D0l: 10.1051/odfen/2010202 J Dentofacial Anom Orthod 2010;13:112-132 Ó RODF / EDP Sciences 112 Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2010202
Transcript of Prosthetic restoration of the canine - jdao-journal.org · Prosthetic restoration of the canine...

Prosthetic restorationof the canine
Pascal AUROY, Jean LECERF
ABSTRACT
There are many ways dentists can restore teeth prosthetically. Depending onits condition of relative integrity or more serious breakdown and the patient’sloss of other teeth, the practitioner can choose from a variety of quite differentprocedures ranging from the fabrication of a single ceramo-ceramic crown on avital tooth to correction of considerable loss of teeth with an implant supportedbridge. This paper will evaluate most of these treatment modalities and, inaddition to purely prosthetic considerations, will discuss the integration intotreatment of periodontal, implant, occlusal, and functional concepts.
KEYWORDS
Prosthesis
Dental occlusion
Oral rehabilitation
Canine.
Address for correspondence:
P. AUROY,J. LECERF,2 place Pasteur,35000 [email protected]
D0l: 10.1051/odfen/2010202 J Dentofacial Anom Orthod 2010;13:112-132� RODF / EDP Sciences
112
Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2010202

1 - INTRODUCTION
Dentists should view the prostheticrestoration of a canine tooth as aprocess that is situated at the con-fluence of occlusal, functional, me-chanical, aesthetic, periodontal, andsurgical imperatives. In this light weshall pass into the territories of relatedspecialties when certain specificpoints of their domain clearly have animpact on the therapeutic success ofour prosthetic therapy. But the subjectis vast and we have no intention ofcovering it in an exhaustive fashionbecause to that we should have had toembrace the quasi-totality of prosthe-tic dentistry. Nor have we planned topresent a catalogue of the traditional
therapies pigeon-holed into the habi-tual subdivisions of our specialty but,instead, to offer some thoughts de-voted to the canine tooth organised inrelation to its deterioration, its ab-sence, and to the extent of theedentulousness that sometimes ac-companies those unhappy develop-ments.
We have prepared an abundantpresentation of illustrations to vivifythe concepts that have arisen from ourintrospections. We hope that ourcolleagues in dento-facial orthopae-dics, whose interest in dental prosthe-tics we share, will find in these pagesthe synthesis they anticipated.
2 - RESTORATION OF A SINGLE BROKEN DOWN CANINE TOOTH
Our first thoughts on the restorationof single deteriorated canine teethfocus on those that have managed toremain vital despite the serious de-predations caused by decay or trauma.
The protocols for the preparation
of a fixed prosthesis placed on a
vital tooth have been codified formany years56. Dentists primarily maketheir decision about a keeping acanine tooth vital or treating it endo-dontically before rehabilitating it pros-thetically on the basis of an evaluationof the health of the pulp and of aperiapical X-ray. Dentists prepare thetooth under a water spray using sharpnew rotary instruments. They makethe temporary crown by thoroughlycooling the thermally cured plastic,eventually taking advantage of theopenings of dentinal tubules to gainits reliable retention as well as that of
the permanent crown that will indefi-nitely preserve all of the tooth’smechanical and biological potential56.(fig. 1 and 2). In every case thetemporary crown protects the pre-pared crown during the indispensableseveral week rest period (fig. 3)needed before the permanent crown(fig. 4) can be cemented.
For experienced practitioners whofollow the protocols we have outlinedthe failure rate, defined as inflamma-tion or necrosis of the pulp that wouldrequire endodontic intervention, isabout the same as the failure rate ofeconomic treatment itself. Theendodontic of health care serviceindicate to us that no matter whatthe precise failure rate of the twoconcepts may be, the practitioner whoroutinely performs endodontic treat-ment on all teeth that are candidates
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 113
for crowns, whether they are vital ornot, will, from the simple mathematicsof the matter, extract more teethbecause of failure than a colleaguewho preserves the vitality of selectedteeth in preparing them for crowns.Let us remember that dentists shouldprepare affected teeth in accordancewith accepted procedure, using appro-
priate filling materials on vital teethwhen indicated.
But if the diagnosis shows that atooth’s vitality has already been com-promised, or that the pulp is so largethat the required reduction of thetooth’s hard tissue to accommodate thebulk of the restoration will endanger it,
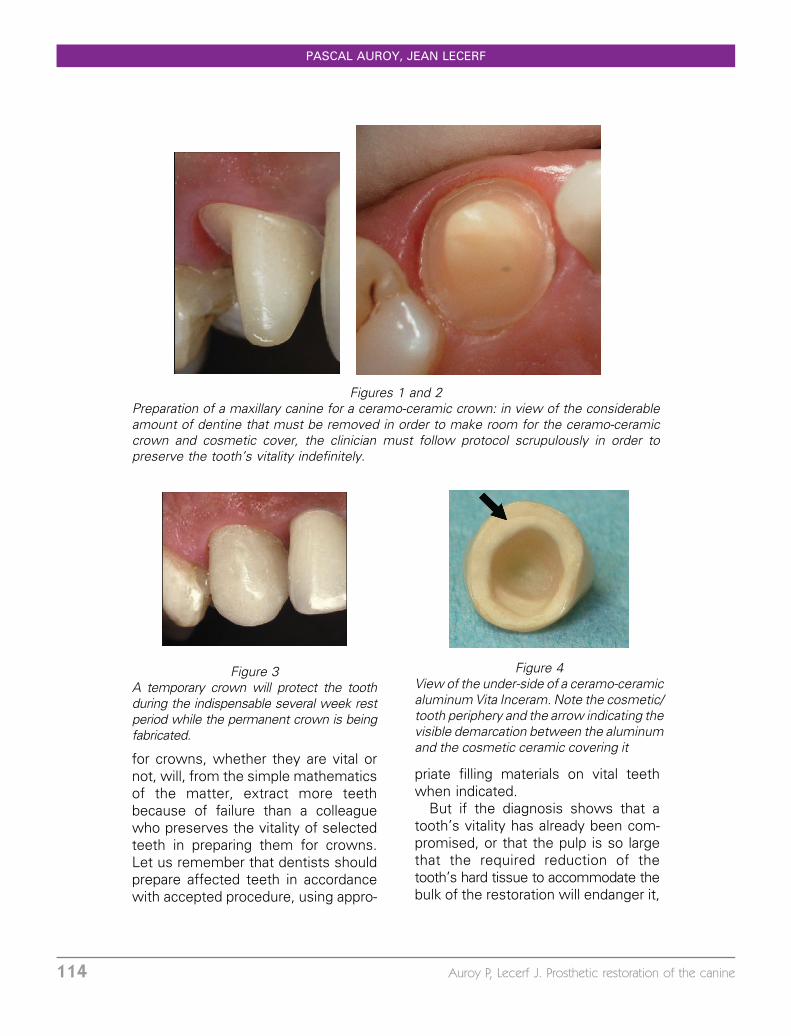
Figures 1 and 2Preparation of a maxillary canine for a ceramo-ceramic crown: in view of the considerableamount of dentine that must be removed in order to make room for the ceramo-ceramiccrown and cosmetic cover, the clinician must follow protocol scrupulously in order topreserve the tooth’s vitality indefinitely.
Figure 3A temporary crown will protect the toothduring the indispensable several week restperiod while the permanent crown is beingfabricated.
Figure 4View of the under-side of a ceramo-ceramicaluminum Vita Inceram. Note the cosmetic/tooth periphery and the arrow indicating thevisible demarcation between the aluminumand the cosmetic ceramic covering it
PASCAL AUROY, JEAN LECERF
114 Auroy P, Lecerf J. Prosthetic restoration of the canine

endodontic treatment becomes neces-sary as well as a reconstruction of
crown and root.
At this point the dentist and patientmust decide on the type of construc-tion of the crown. Should it be cast asis done for the traditional inlay-coreprocedure or milled? Indications forthis newer type of milled restoration
are now also perfectly well codified1:presence of the three elements of atooth’s hard structure of at least 1 mmin thickness and a height greater thanhalf of the proposed prosthetic crown.The removal of tooth substanceshould never enter into the sulcusspace so that clinically the junctionbetween crown and tooth can behidden in the sulcus and encirclingdentinal structure. Finally, more forcanines than for other teeth, the ruleof dentists having have good accessi-bility in preparing it and maintaining itin complete isolation from the fluids ofthe oral cavity in bonding or cementingit is an indispensable requirement forsuccess1,5,8.
With these points in mind, webelieve that milled crown-root rehabi-litation is contra-indicated and that acast reconstruction21,25,50 is re-quired. No matter what material isemployed in fabrication the properpreparation for the root post willdemand reduction of the root wallsto less than 1 mm in thickness and theremoval of a considerable amount ofdentine.
Because the modules of elasticity ofthe metal making up the cast replace-ment crown and root are 10 to 30times greater than those of the naturaldentine itself, occlusal constraints aretransmitted almost in full force to theroot structures. That is why it is bestto select materials with weak modules
of elasticity, which is why dentistsshould not utilise zircon, oxide ofzirconium, whose module of elasticityis 60 times greater than that ofdentine.
In order to understand this problemwell, we must consider the flow ofconstraints at the interface of theprosthesis and the dentine: for a givenamount of occlusal forces, the largerthe surface of the interface the morewidely and thus less densely, theforces are distributed. So the practi-tioner should increase the size of thepreparation in the root as much aspossible thus increasing the amountof dentine that will contact the in-serted post. But this must be done bymaking the preparation longer, notwider, because that would reducethe thickness of the dentinal wallsand make them more fragile. Thus wekeep the bore of our preparations,and, accordingly the diameter of theposts that will fit into them, as narrowas possible, but of lengths equalto 2/3 to 3/4 of the depth of thealveolus in which the tooth’s rootresides11,12,30,36. (fig. 5).
We bond the inlay-core rather thancement it, thus reinforcing the attach-ment of the prosthesis to the root andencouraging the diffusion of occlusalconstraints1,10,11,12. All these modal-ities are particularly pertinent to canineteeth, in view of the heavy nature ofthe occlusal forces to which they aresubjected. By carefully following thepreparation protocol we have sug-gested, practitioners can reduce therisk of a prosthesis on a canine toothbecoming uncemented or debondedor of the tooth’s root being fractured.
In order to make prosthetic crowns
placed on canine teeth aestheticallysatisfactory the best materials for
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 115

dentists to choose are ceramo-ceramicfor vital teeth and ceramo-metallic forendodontically treated canines whosepreparation has not been aestheticallyoriented2,13,46,48,52.
A primordial requirement for anyprosthetic rehabilitation is that theinvolved teeth must be invested in ahealthy periodontal environment, thatis that the periodontal fibers be sturdyand free from inflammation. In orderto maintain them in that condition, thedentist’s tooth preparation should beentirely supra-gingival except wherethe circumference of the crown will bedirectly visible or when existing sulcu-lar lesions or contours force thepractitioner to place the junction ofcrown and tooth within the sulcus. Inthese situations the dentist shouldrespect the principles that Gaarguilo22
proposed in a 1961 article. The posi-tion of the edges of the prosthesisshould respect the epithelium of thejunction by preserving a margin oferror. They will not be tolerated unless
they are set at a minimum distance .4mm from leading edge cells of theepithelial attachment. Accordingly,prosthesis should never be set moredeeply than .5 mm in a sulcus 1 mm indepth. There is today a strongconsensus that with junctions ofprosthesis to tooth of equal qualitythose that are placed more deeply inthe dento-alveolar sulcus will provokethe most in f l ammatory reac -tions15,19,20,22,32,40,51,55.
Preferably, dentists should makethe buccal aspect of a rehabilitatedcanine one of a ceramico-tooth junc-tion rather than one that is metallic-tooth, for obvious aesthetic reasons.This is rapidly becoming the standardapproach because modern well for-mulated techniques allow for an ex-cellent cervical adaptation, of less than80 microns (cf. fig. 30). Nowadays, thetooth-prosthesis buccal or labial junc-tions of ceramo-ceramic crowns canbe virtually invisible and are placedvery slightly, .3 mm, beneath thesulcus or at the gingival level becausethey have no unattractive metal be-neath their outer surfaces40,51,55.
To prepare teeth properly for cer-amo-metallic crowns with tooth pros-thesis joints that are ceramic as wellas for crowns that are entirely ceramo-ceramic, dentists must use largeflame burs to make shoulders withrounded internal angles. The onlydistinction between the two types isthe thickness of the preparation re-quired, 1.2 to 1.8 mm for the first and.8 to 1.2 mm for the second. All otherforms of preparation have now be-come outmoded because of newtechniques, new materials, and mod-ern prosthetic methods and materer-ials16-18 (cf. fig. 1, 2).
Figure 5We believe that it is important for theposts be narrow in diameter but longenough to equal 2/3 to 3/4 of the lengthof the root.
PASCAL AUROY, JEAN LECERF
116 Auroy P, Lecerf J. Prosthetic restoration of the canine

3 - REPLACING MISSING CANINES
Apart from orthodontic solutions, amissing maxillary permanent caninetooth is usually best replaced by aprosthetic crown placed on an im-plant. Generally speaking the intra-oralconstraints that upper canines aresubjected to, in lateral as well as inprotrusive excursions make their re-storation with a traditional bridge adelicate and questionable enterprise.A multi-unit bridge, for example an-chored on premolar or incisal teethshould certainly not be considered asa proper restoration because of thelikelihood that it will transmit iatro-genic traumatic forces to the period-ontal membranes of the abutmentteeth. In the same way a bridgehaving as its only abutments thepremolar teeth and a lateral incisor
will eventually cause the loss of thelateral because the root structure andinvesting periodontal tissues of thistooth resist lateral forces poorly. Ex-tending the bridge to include thecentral incisor whose structural make-up is better suited to resist difficultocclusal stress rarely solves the pro-blem because splinting together thepremolars and the incisors of thesame side imparts to those incisors adistal component of force which pro-gressively opens up a mesial space ordiastema.
These types of bridges succeed,despite this dire prognosis, on thoserare occasions when the root supportis especially robust and the occlusalconstraints are especial ly fee-ble42,49,53,54. In general, the participa-tion of the canine in disoccluding theposterior teeth in lateral and protrusiveexcursions makes it necessary for thedentist include in the reconstruction toreplace a missing canine all the teethfrom the premolars on the ipsilateralside and at least the central incisor,and possibly the lateral incisor andcanine on the contralateral side (fig. 6).This extended type of rehabilitation isless indicated on the mandiblebecause there lateral occlusalconstraints are largely directed lin-gually and are distributed and dissi-pated through inter-arch contactpoints and into the supporting bone,which is far denser than maxillarybone49,53.
Finally, whatever form the bridge maytake, bonded splints or cementedcrowns, the obligatory inclusion of nu-merous abutments greatly complicatesthe fabrication of this type of rehabilita-tion of a missing canine and makes the
Figure 6Replacing missing maxillary caninessometimes requires the construction oflarge multi-unit bridges. The powerfulforces that act on them (depicted in theorange arrow) sometimes results in theopening up of an unattractive space whenthe bridge does not incorporate any dentalunits on the other side of the midline. Therange of risk is shown within the arrow ofa colored range scheme running from highrisk in red to low risk in blue.
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 117

choice of a crown placed on an implant aseductively attractive treatment plan,especially in the maxilla.23,43.
The surgical placement of a single
implant to replace the root of a missingmaxillary canine does not usually poseany problems. When a large amount ofbone is available and the space be-tween the first premolar and the lateralincisor is adequate, access is easy. Butthe surgeon must take care to positionthe implant exactly at the midpointbetween the premolar and the lateraland somewhat palatally so as to leave asufficient amount of gingival tissue inplace to lend a natural appearance tothe artificial tooth. This will also allowthe prosthodontist to utilise an implantwhose collar will be wider than thecollar of the post and still leave enoughspace buccally for soft tissues. Unfor-tunately the buccal anatomy of themaxilla in the canine area when thetooth has been missing for any lengthof time is concave, often excessivelyabove the area where the canine bulgeought to be. Because the quantity ofbone palatally is always sufficient andthey fear they will risk fenestration, ifthey place the implant too close tocortical buccal bone, oral surgeons aretempted to position their implants withthe apex too far palatally, which oftenmakes the pivot emerge too far buc-cally6,7,9,14,26,47(fig. 7).
This type of emergence has seriousundesirable aesthetic and health con-sequences for the soft tissues. So theprosthodontist and the oral surgeonshould carefully analyse the computedtomographic films taken pre-opera-tively with a radio opaque radiologicalguide to plan the provisional orienta-tion of the implant and its futureemergence. The surgeon will thenuse the surgical guide to reproduce
the planned placement in the mouthoperatively4,26. More than the angula-tion itself, which, if not precisely whatit ought to be, can be corrected withan angulated post, is the precise spot ofthe implant’s emergence, whichwill determine the success or failureof the implant/prosthetic replacementof a missing canine6,7. (fig. 8, 9, 10, 11).
Because the aesthetic immediateloading of a crown is not without riskduring the first few weeks of theosteo-integration of an implant placedin a maxillary canine site practitionersshould try to protect it from all occlusalconstraints during this critical period.But this is rarely possible because ofthe functional role this tooth is des-tined to play.
But dentists can also rehabilitate amissing upper cane with a removable
prosthesis. However this type ofrestoration has many drawbacks, theunsightly buccal clasps that have to be
Figure 7The scanner image and a schematicrepresentation of a section at the level ofthe maxillary canine. The implant, ingreen, is well placed but the implant inred is too buccal, Even if an angulatedpost could correct the axis of the pros-thesis, it emergence in the gingiva wouldbe unsightly and the future of the buccalsoft tissues uncertain.
PASCAL AUROY, JEAN LECERF
118 Auroy P, Lecerf J. Prosthetic restoration of the canine
used for its retention and the prepara-tion of occlusal rests that have to bemade on adjacent teeth especiallythose on lateral teeth, which are illsuited to support the impact of con-straints on the region of their cingu-lums. Perhaps more troubling is therequired design of the frame of thepartial denture that has to extendthroughout almost the full extent ofthe upper arch to seek a hypotheticalretention on the second or even thirdmolar on the contra-lateral side.
Prosthodontists will find the ensembleof these requirements difficult tosatisfy in their attempt to produce apartial denture serving a canine func-tion that won’t be too readily dislodgedand whose relation to the naturalgingival tissues will not be unsightly.So partial dentures designed to replacesingle missing maxillary canine teethare of distinctly marginal utility. On theother hand, when many maxillary teethare missing many prosthodontists to-day still believe that removable partialdentures are often fully indicated toreplace them.
4 - REHABILITATION OF A MISSING CANINE IN AN ARCH WITH NUMEROUSMISSING TEETH
Even today, the many perceivedmedical, anatomic, or financial disad-vantages of prosthetic therapy basedon implants persuade some patientsto prefer removable partial dentures
to replace missing teeth.
Since the work of Picton andWills41, who demonstrated the viscoe-lastic properties of the periodontalligament and the mucous membrane,the reliance on clasp retained partialdentures built on rigid metal frames
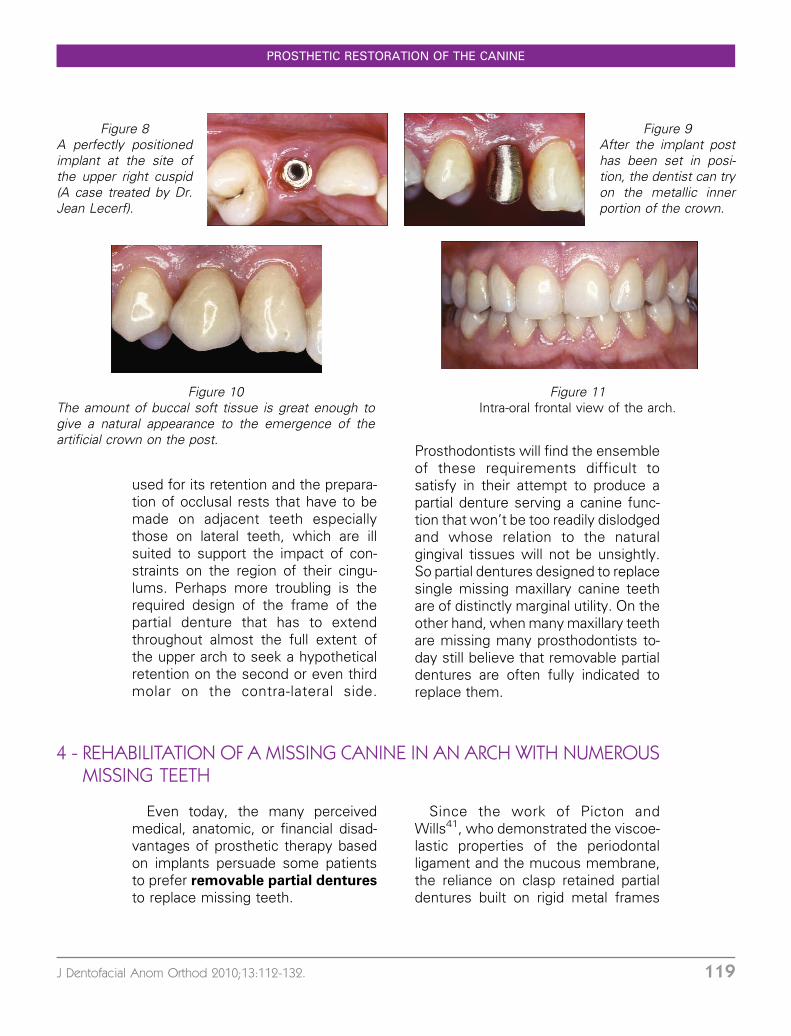
Figure 8A perfectly positionedimplant at the site ofthe upper right cuspid(A case treated by Dr.Jean Lecerf).
Figure 9After the implant posthas been set in posi-tion, the dentist can tryon the metallic innerportion of the crown.
Figure 10The amount of buccal soft tissue is great enough togive a natural appearance to the emergence of theartificial crown on the post.
Figure 11Intra-oral frontal view of the arch.
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 119

has been replaced with a new conceptthat, while retaining some of thepositive features of the traditionalpartial dentures, distributes occlusalforces not just to supporting teeth butalso to osteo-mucous structures, thepartial use of rigid frames, and pa-tient’s not wearing the partial full time.These principals relegate the remova-ble plastic partial denture withouttooth born clasp support to a provi-sional status.
In determining how to replace miss-ing teeth, practitioners must first fullyunderstand the complexity and thedifficulties they will encounter in treat-ment. In effect, when a fixed prosthesisfails, this outcome is usually immedi-ately and obvious. But the failure of aremovable partial denture may be un-detectable when it is first worn andshow up only later. In addition, incontrast to a widespread notion, justas much precision is called for castingthe metal frame of a partial than it is forcasting a fixed bridge. Finally, thedifference in compressibility of osteo-mucosal structures and teeth, which arethe elements that support a removablepartial denture, add to the difficulties oftreatment a need for exquisitely sophis-ticated impression taking that is notrequired for either fixed bridgework ortotal partial dentures.
The key element in the success of amaxillary partial denture is whether ornot proper canine function can bemaintained. The second depends ondentists seeing patients frequently forcheck-up visits and on patients follow-ing a good oral hygiene regimen.
The loss of a canine tooth alwayscomplicates the prognosis for treat-ment of arches with numerous missingteeth with partial dentures. Only therobust health of the remaining teeth in a
healthy periodontium as well as arobust ridge in the edentulous areascan assure successful rehabilitationwith an extended removable denturethat will function well and not causeiatrogenic damage (fig. 12 and 13).
When a canine is lost to an arch thathas already had multiple extractions,dentists must consider the advisabilityof making it completely edentulous
so that a full and not a partial denturecan be constructed.
In effect, the desired goal in suchcases is not an effective prosthesisnor well executed prosthetic treat-ment, but durable rehabilitation andreturn to good function. Thinking inthis way, dentists should always con-sider that patients with multiple miss-ing teeth might be better off if theywere completely edentulous. Theworst strategy is to keep an extensive
Figure 12Placement on a model made of animpression of a partially edentulous archshowing the left and right first and secondmolars with anatomically prepared crownssplinted together with supporting ma-trices for resilient function, stress-break-ing ASC52 attachments. The alveolarridge is robust and the palate deep makingretention of the partial ideal and allowingfor re-creating bilateral canine functioningwithout difficulty.
PASCAL AUROY, JEAN LECERF
120 Auroy P, Lecerf J. Prosthetic restoration of the canine

partial denture retained by a fewremaining teeth in a periodontium ofdoubtful quality at any cost until thefinal days when the last feeble toothmust be extracted. In these situations,patients, often well on in years, willfinally have to submit to the alwaysdifficult learning curve of dealing witha full denture. The best strategy is toto prepare the remaining teeth in theirweakened periodontium endodonti-cally so that they can eventuallysupport post attachments to anchor afull denture (fig. 14, 15, 16, 17).
Practitioners should attempt to pre-serve the roots of a patient’s lastremaining teeth even ones in anunfavourable periodontal environmentbecause they will bestow an intactproprioception to a future denture andhelp the patient to masticate withoutinsurmountable difficulty thanks to thesensory-motor interactions of theirperiodontal receptors. These patientswill not have to undergo the brutal re-learning curve of how to chew again.Even if those enfeebled residual roots
survive for only a few months under anew full denture, the progressive lossof sensory receptors as the period-ontium fades away will ease thepassage of patients from a lifetime ofchewing with teeth to a new status ofmasticating with dentures. Then, onthe day when their last remainingteeth, other than the treated roots,have to be extracted their neuro-muscular systems will already havemade the necessary adjustments andthe simple insertion of the male part ofthe attachment into the underside of
Figure 13Intra-oral view of metal frame removable partial denturein place. Note how precisely it is adapted to the mucosaand to the metal crowns. The rigid arms of the clasps andthe crown bars fit well in the palatal shapes of the crownsthat have not been over-contoured.
Figure 14These four seriously broken down teeth, in anotherwise edentulous arch, were preserved to maintaintheir periodontal proprioception.
Figure 15Their residual roots received copings that wouldsupport ZAAG overdenture attachments for the upperright canine and central and the left central and asimple cap for the left lateral. Once the copings arecemented to the roots, the male parts, in nylon, areplaced in the matrices of the full denture and, coveredin resin, are set into the copings. While bonding issetting in the moth the patient maintains pressure bybiting on the denture.
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 121

the denture will suffice to maintain thefunctional effectiveness of the fulldenture made months or even yearsearlier.
The teeth the most suitable for thisover-denture concept, now referred toas a complete tooth-bone-mucosalsupported full denture are the uppercentral incisors, the upper and lowerpremolars and molars, and, especially,the upper and lower canines. Theseare the teeth the most richly endowedwith sensory receptors and they areoften the last ones remaining in thearch.
The treating dentist will always tryto maintain symmetry on both sides ofthe midline in choosing teeth tosupport an over-denture. So if only afew teeth persist on only one side ofthe arch the dentist should extractthem rather them than use them tosupport an over-denture that willinevitably suffer from uni-lateral mas-tication provoked by uni-lateral pro-
prioception. The occlusal concept thatdentists should systematically bear inmind for this type of mastication is thepermanence of bi-lateral contacts inlateral movements and antero-poster-ior contacts in propulsive movement,which is to say a balanced bi-lateralocclusion.
Of course implant-based prosthe-
tic therapies, when they are indi-cated, can take the place of a fewremaining teeth, after they have beenextracted, and act as substitutes forthem in partial denture rehabilitation.
In the mandible, by placing twoimplants, at the canine sites, dentistscan insure that a full over-denture willbe stable and retentive. This is theminimum reference standard as es-tablished by a 2002 conference atMcGill University in Montreal. Byfollowing this protocol dentists canfabricate reliable full lower dentures ina straightforward fashion at a moder-ate price28 (fig. 18, 19). In the maxillathe extensive supporting area sup-plied by the palate as well as ridgesthat are sturdier than those in themandible make the need for implant
Figure 17The underside of the denture shows the male parts ofthe attachments enveloped in their bonding base. Anenlargement of the attachment in canine area is shownin the upper left.
Figure 16The complete tooth-bone-mucosa supported full den-ture shows in its outer surface traces (black arrows) ofthe excess of the self-polymerising resin that bondedthe male parts of the retention apparatus to the dentureexcept in the canine area where the acrylic is too thickand the bonding succeeded without any perforation ofthe denture. The attachments amplify the denture’snatural retentive qualities and because of the remainingroot structures greatly enhance its proprioceptiveperformance.
PASCAL AUROY, JEAN LECERF
122 Auroy P, Lecerf J. Prosthetic restoration of the canine

supported full dentures far less fre-quent.
Where indicated, when the amountof resorption and the crown heightremain adequate, dentists can con-struct conventional implant supportedbridges4. In these cases implants arepositioned in selected sites, usuallythe regions of the central incisors, thecanines, and sometimes premolarsand molars, in such a way as to allowthe prosthetic posts to suit the pa-tient’s periodontium. When seriousgingival and mucosal resorption has
occurred that would require long postsand an unsightly bridge with anunfavourable crown/implant ratio theconcept of ‘‘all-on-four’’ bridge intro-duced by Dr. Paulo Malo around 2000may be indicated. This type of implantsupported bridge uses artificial acrylicgingiva around prosthetic teeth thatare carried by a metallic frame in-serted into implants that do notnecessarily follow the emergencepath of the natural teeth they re-place29,33,34 With this technique thetwo posterior implants can be inclineddistally so they don’t risk impinging oncritical zones like the mandibular canaland the maxillary sinus. This increasesinitial stability and allows the dentist toplace an immediate full denture sup-ported by four implants on the day ofsurgery33,34 (fig. 20, 21, 22, 23, 24).This extensive type of rehabilitationpresupposes durable osteo-integrationof the four implants. If just one ofthem fails, this will compromise theentire enterprise. So dentists have toconsider using rehabilitation techni-ques with a greater margin of erroron posts placed in 6 to 8 implants inwhich the entire project will not have
Figure 18A complete lower denture stabilised by two implants.The matrix of the Locator@ attachments is clearlyvisible on the denture’s underside.
Figure 19A view of the male parts of the denture attachmentsemerging from two implants set in the sites of thelower canines.
Figure 20The all-on-four technique. The four upper implants inplace with their provisional posts (Dr. Jean Lecerf’scase. Dr. Patrick Limbourg did the surgery).
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 123

to be abandoned just because one ofthe implants fails. But this moreprudent approach will cost more whileproviding the same same functions38.The extensive implant supported re-constructions, whether they functionin immediate or delayed canine dis-occlusion or in group function, imposethe equivalent constraints on theimplants and their superstructures.Because of this dentists should makea choice of the dynamics of occlusionbased more on the character of theopposing arch than on the arch thatwill be restored with a partial den-ture24,35,37,39 (table 1).
Cases of extensive tooth loss
When dentists cannot restore thefunction of a missing canine with apartial removable denture because theanatomy of the ridge would notprovide it with sufficient stability andretentivity, they must consider fabrica-tion of implant supported prosthesis.
But because an osteo-integratedimplant is not housed in a periodontalmembrane it does not have theresilience of a natural tooth, the
Figure 21The emergence of the implants and the multi-unitposts (Nobel Biocare@) fifteen days after the non-flapsurgery that left no gingival scarring.
Figure 22Try-on of the metal frame on the final posts.
Figure 23The bridge with false gingiva and plastic teeth (labtechnician Yves Gastard).
Figure 24Bridge in place in the mouth. Note the spaces abovethe false gingiva that are indispensable for good oralhygiene but that sometimes interfere with patientspronouncing words properly. Unlike a dentition with ahealthy periodontium and natural canines in place, thisartificial denture functions with the false canines out ofocclusion in lateral movements.
PASCAL AUROY, JEAN LECERF
124 Auroy P, Lecerf J. Prosthetic restoration of the canine

differential in the response of tissuesinvesting implants and natural poses aproblem to dentists planning a mixedimplant-tooth born prosthesis: shouldthe restoration connect the naturaland artificial roots?
A thoughtful review of the litera-ture31,35,44,45,54,57 would lead a readerto answer that question with a ‘‘no.’’Still, some authors recommend such aunion and many such restorations havelasted for years, but no statistics for thefailure rates of connected and non-connected prostheses are available.
So it is really not possible topropose an all inclusive answer
because very case has its own uniqueclinical indications. A prosthesis sup-ported by multiple implants risksmaking the natural teeth to whichthey are joined by a cantilever-typebar an extension of themselves(fig 25). To avoid this, the connectorshould be semi-rigid with a flexibleinterrupter of forces placed as closelyas possible to the implants to reducethe amplitude of the lever arm. Thecase shown in figure 25 can becompared to the one depicted in figure12. These two types of Class IVmaxillary edentulousness would seemto be similar but the shallowness of
Arch
opposing
bridge
Full
denture
Partial
denture
Anterior
teeth
including
canines
missing
Partial
denture
Anterior teeth
missing but
natural
canines in
place
Partial
denture
Right and
left buccal
teeth,
including
canines
missing
place
Partial denture
Right and left
buccal teeth
missing but
natural canines
still in place
Full arch of
natural teeth or
fully rehabilitated
with fixed
bridges
Occlusal
Dynamics
Bilateral
balanced
occlusion
Group
function
Canine
disoccluded
Group
function
Canine
disoccluded
Canine
disoccluded
Table 1Indication of occlusal dynamics that focuses more on the opposite arch than on the arch beingreconstructed with a removable partial denture.
Figure 25Five short implants were placed in the highly resorbed anterior sector of the maxillary ridgeto support a bridge on posts that replaced a removable partial denture that had functionedpoorly. The multi-unit posts (Nobel Biocare@) can be seen emerging from the freshly healedgingiva. The natural posterior teeth rehabilitated with inlay-cores were prepared to receivesplinted crowns (Dr. Anne-Laure Auroy-Guillot did the surgical procedure).
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 125

the ridge offered feeble retention to aremovable partial denture in the secondcase. Accordingly, the treating dentisthad to construct an implant supported
denture. Its semi-rigid connector withsliding grooves allowed for periodontalplay in its tooth supported sectors andalso contributed to its capacity to resistthe lateral and anterior constraints theimplant supported sector was sub-jected to (fig. 25, 26, 27).
5 - REHABILITATION OF A BROKEN-DOWN CANINE IN AN ARCH WITHMANY MISSING TEETH
Full arch or nearly full arch recon-struction is no longer difficult toachieve so long as the canines canbe restored whether the bridge issupported entirely by natural teeth orby a combination of natural teeth andimplants. Dentists will usually achievesuccess if they have restored thepatient’s periodontium to good healthand if they have respected the typeand quality of the tooth-prosthetic jointas stipulated in the principles outlinedabove and in fig. 28, 29, and 30.
They should have reduced the sizeof the inlay-core preparations enough
to allow for the placement of crownsand their cosmetic coverings thatwould harmonise with the proportionsof the original natural teeth and theiremergence from the gingive27. Theyshould also constructed the restora-tions in such a way that they will havecontact points just above the gingivaand will be convex enough to allowpatients good access for the main-tenance of effective oral hygiene. It isalso crucial for dentists to constructrehabilitations that will have scrupu-lous respect for occlusal dynamics byhaving registered them and mounted
Figure 26Try-on of partial denture frame and the tooth supportedfixed prostheses. The semi-grid connectors bind the twotypes of prosthetic appliances together while allowingperiodontal play under the tooth supported sectors andalso contributing to the appliance’s capacity to resist thehorizontal constraints transmitted to the short implants.In the inset is a palatal view of the semi-rigid connectormesial to the upper right first molar. (Christophe Flabeauis the dental technician who fabricated the prosthesis.)
Figure 27Intra-oral view of the reconstruction in place. This typeof design allows for a canine-protected occlusionwhose constraint on the prosthesis do not dislodge itduring lateral or propulsive excursions as was the casewhen the patient wore a partial removable denture.
PASCAL AUROY, JEAN LECERF
126 Auroy P, Lecerf J. Prosthetic restoration of the canine

them on articulators to determinecondylar inclination and Bennet’s an-gle. Finally, for rehabilitation of anentire arch dentists must make atherapeutic choice of occlusion: max-imal inter-cuspation in centric occlu-
sion, because that is the only that theycan re-register over the course oftreatment. They should also, in mostcases, instead of group function,select canine protected occlusion inlateral movements as well disengage-ment of the buccal teeth by theprotection of the group of incisorsand canines in propulsive movements.Of course, they must adjust theseprinciples when the condition of theopposing jaw requires it (cf. table 1).
Under these conditions, the biologi-cal and functional integration of afixed, multi-unit rehabilitation of abroken down canine will be assured.
These principles also apply in therehabilitation of a broken down canineby a multi-unit partial removable pros-thesis.
Figure 28Fixed rehabilitation of a broken down maxillary canine.Because both canines were present the prosthodontistwas able to fabricate a full arch bridge without usingimplants. The prosthodontist restored the periodon-tium to a healthy condition and carefully respected itduring tooth preparation, which facilitated the nextchair side steps including impression taking, try-ons,occlusal adjustments, and cementation.
Figure 29Mirror view of the prosthesis. Note the ceramic-toothjoints for the incisor canine group and the metal-toothjoints in the bicuspid molar area (dental technicianJean-Chritophe Flabeau).
Figure 31At six months the prosthesis appears well integrated
Figure 30The ceramic crowns had enough bulk for the technicianto give them a life-like appearance and a natural lookingemergence from the gingiva.
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 127

These extensive rehabilitations thatoften incorporate broken down ca-nines and other teeth adjacent to theedentulous sites into fixed bridgesassociated with recoverable partialdentures are sometimes referred toas ‘‘combined prostheses’’ but in-stead of this outdated nomenclaturewe prefer the term ‘‘composite pros-theses’’ because composed as theyare of conjoined elements like those incomposite fillings they have in theirensemble characteristics superior to
those that would have been achievedif their components operated individu-ally side by side.
These reconstructions also have toreact to the different compressibilityof the structures that support them. Ineffect, the periodontal compressibilityof the fixed elements of the compo-site prosthesis is on the order of100 microns while the mucosal
Figure 32This older patient was unhappy with the effect thecongenital absence of her upper lateral incisors had onthe appearance of her smile. But she was unwilling toundergo orthodontic treatment to correct the problem.So we prepared her vital central incisors, canines, andpremolars to receive crowns.
Figure 33We made an anterior bridge for her in which herincisors, canines, and premolars were splinted togetherto improve her smile and to articulate by means ofinvisible ASC52 attachment with a removable posteriorpartial denture.
Figure 34This intra-oral view shows the excellent aestheticintegration of the fixed anterior bridge and theremovable partial denture (ceramicist Jean-Paul Laur-emboule, frames of the two prostheses by technicianBruno Charbonier).
Figure 35At the left a view of the underside and the male part ofthe attachment in the facing of the matrix splintingthe frame of the partial with the fixed anterior bridge.At the right the attachment is entirely embedded inthe premolar sector of the removable partial so that it iscompletely invisible when the partial is in place in themouth.
PASCAL AUROY, JEAN LECERF
128 Auroy P, Lecerf J. Prosthetic restoration of the canine

compressibility of the tissues beneaththe removable elements can be great-er than one millimeter. Under thesevarying conditions in order for occlusalconstraints to be harmoniously distrib-uted throughout the composite pros-thesis between bone and soft tissuesupporting areas the dentist mustemploy accurate sophisticated im-pression techniques. The over-all com-posite impression, as its namesuggests, may be composed of threeor four different materials used suc-cessively in an individualized impres-sion tray. Or the dentist may chooseto employ the correction impressiondescribed by McCracken that utilizesthe metal frame of the removablepartial denture made from the initialimpression as an impression tray inorder to register secondarily the vary-ing compressibility of mucosa and ofteeth.
These metal frames are often con-structed to articulate with conjoinedelements by means of attachmentsthat are machine made clasps thatmust, like all clasps, serve the triad ofthe equilibrium of partial dentures as
described by Housset: retention, sta-bility, and support.
The position of the canine in thearch in addition to the strength of theanchorage provided by its sturdy rootmake it an ideal pillar to sustain theattachments of partial dentures. Evenso, canines are not sufficiently unmo-vable to resist indefinitely the con-straints that those machine madeclasps will subject them to. Accord-ingly, dentists should routinely splintreconstructed canines to fixed bridgesconstructed on other rehabilitatedadjacent teeth so that occlusal forcescan be distributed to this consolidatedgroup as well as to the conjoinedpartial denture.
The principal benefit derived fromlaboratory fabricated attachments overfactory made clasps, in addition totheir improved retention capacities, isundoubtedly aesthetic. But the forcesthey transmit to the dento-periodontalstructures are so great that dentistsshould be sure that the quality and thenumber of the roots supporting themare capable of resisting those con-straints (fig. 3, 33, 34, 35).
6 - CONCLUSION
There is always an element of risk inthe rehabilitation of canine teeth heigh-tened by the importance of the aes-thetic and functional roles they play.
Even though dentists can expectthat the reconstruction of brokendown canines usually enjoys a goodprognosis, they must remember thatthe loss of this ‘‘keystone of thedental arch’’ would pose numerousproblems and complicate therapy.
But, whatever the complexity andthe extent of the rehabilitation pro-cesses, only by taking into accountthe over-all value of the canine in theoro-facial complex, and particularly itsperiodontal, occlusal, and functionalaspects, can dentists accurately as-sess all the diagnostic issues andmake the proper decisions that willlead to clinical success.
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 129

BIBLIOGRAPHY
1. ANAES: Indications et contre-indications des reconstitutions corono-radiculaires pre-prothetiques coulees et inserees en phase plastique. Service d’evaluation technolo-gique, 2003.
2. Andersson M, Razzoog ME, Oden A, Hegenbarth EA, Lang BR. Procera: a new way toachieve an all-ceramic crown. Quintessence Int 1998;29(5):285-96.
3. Akca K, Uysal S, Cehreli MC. Implant-tooth-supported fixed partial prostheses:correlations between in vivo occlusal bite forces and marginal bone reactions. ClinOral Impl Res 2006 Jun;17(3):331-6.
4. Balmer S, Mericske-Stern R. Implant-supported bridges in the edentulous jaw. Clinicalaspects of a simple treatment concept. Schweiz Monatsschr Zahnmed2006;116(7):728-39.
5. Bolla M, Bennani V. La reconstruction corono-radiculaire pre-prothetique des dentsdepulpees. Guide clinique. Editions CdP.
6. Cardaropoli D, Debernardi C, Cardaropoli G. Immediate placement of implant intoimpacted maxillary canine extraction socket. Int J Periodontics Restorative Dent 2007Feb;27(1):71-7.
7. Chiapasco M, Zaniboni M. Clinical outcomes of GBR procedures to correct peri-implantdehiscences and fenestrations: a systematic review. Clin Oral Implants Res 2009Sep;20 Suppl 4:113-23.
8. CovoL. Reconstitutions corono-radiculaires et facteurs influençant leur retention RevueFrançaise d’Odonto-Stomatologie 2000;29(1).
9. de Oliveira RR, Novaes AB Jr, Papalexiou V, Muglia VA, Taba M Jr. Influence ofinterimplant distance on papilla formation and bone resorption: a clinical-radiographicstudy in dogs. J Oral Implantol 2006;32(5):218-27.
10. Diaz-Arnold AM, Vargas MA, Haselton DR. Current status of luting agents for fixedprosthodontics. J Prosthet Dent 1999;81(2):135-41.
11. Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration ofendodontically treated teeth: a systematic review of the literature – Part1. Compositionand micro- and macrostructure alterations.Quintessence Int 2007;38(9):733-43.
12. Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration ofendodontically treated teeth: a systematic review of the literature, Part II (Evaluation offatigue behavior, interfaces, and in vivo studies). Quintessence Int 2008;39(2):117-29.
13. Donovan TE. Factors essential for successful all-ceramic restorations. J Am DentAssoc 2008 Sep;139 Suppl:14S-18S.
14. Dong J, Ikebe K, Gonda T, Nokubi T. Influence of abutment height on strain in amandibular overdenture. J Oral Rehabil 2006 Aug;33(8):594-9.
15. Dragoo MR et Williams GB. Periodontal tissue reactions to restorative procedures. Int JPeriodont Rest Dent 1981;1:9-23.
16. Dwan A, Yaman P, Razzoog ME, Wang RF. Effect of cement on fracture: resistance ofall-ceramic crowns. J Dent Res 1996; 75(abstr 2136):284.
17. Eames W’B, O’Neal SJ, Monterio J, Miller C, Roan JD et Cohen KS. Techniques toimprove the seating of castings. J Amer Dent Ass 1978;96:432-7.
18. Fasbinder DJ. Clinical performance of chairside CAD/CAM restorations. J Am DentAssoc 2006 Sep;137 Suppl:22S-31S.
19. Felton DA, Kanoy BE, Bayne SC et Witrhman GP. Effect of in vivo crown margindiscrepancies on periodontal health. J Prosth Dent 1991;65:357.
20. Fleiter B, Martin D. Criteres d’integration parodontal et esthetique des constructionsceramiques anterieures. Journal de parodontologie Vol14, N� 2/95:215-24.
21. Gantel C, Aboudharam G, Dejou J, Blanchard JP. Enquete sur la pratique desreconstitutions corono-radiculaires. Cahiers de prothese 2006;133:21-9.
PASCAL AUROY, JEAN LECERF
130 Auroy P, Lecerf J. Prosthetic restoration of the canine

22. Gargiulo AW, Weintz FM, Orban B. Dimensions and relations of the dento gingivaljunction in human. J Periodont 1961;32:261-7.
23. Hegenbarth E. Use of the Procera CAD/CAM System for metal-free crowns on single-tooth implants. Quintessence Dent Tech 1998;1:27-37.
24. IsidoriM, MalquartiG, ChavrierC. Concepts occlusaux en prothese fixee implantaire.Implant 1998;4(1):29-40.
25. Joe Editorial Board. Restoration of the endodontically treated tooth: an online studyguide. J Endod 2008 May;34(5 Suppl):e187-90.
26. Jung RE, Pjetursson BE, Glauser R, Zembic A, Zwahlen M, Lang NP. A systematicreview of the 5-year survival and complication rates of implant-supported singlecrowns. Clin Oral Implants Res 2008 Feb;19(2):119-30. Epub 2007 Dec 7.
27. Knode H, Sorensen JA. Fracture strength of ceramic single tooth implant restoration. JDent Res 1992;71(abstr 1137):248.
28. KrennmairG, WeinlanderM, Krainhofner M, PiehslingerE. Implant-supported mandibularoverdentures retained with ball or telescopic crown attachments: a 3-year prospectivestudy. Int J Prosthodont 2006 Mar-Apr;19(2):164-70.
29. Lai YL, Chou IC, Liaw YC, Chen HL, Lin YC, Lee SY. Triple immediate therapy (ridgeexpansion, soft tissue augmentation, and provisional restoration) of maxillary anteriorsingle implant. J Periodontol 2007 Jul;78(7):1348-53.
30. Larson TD. Part two: The restoration of non-vital teeth: structural, biological, andmicromechanical issues in maintaining tooth longevity. Northwest Dent 2006;85(6):23-5, 27, 29-32.
31. Le Gall MG, Saadoun AP. Liaison entre dents naturelles et implants. Limites etindications. Cah Proth 2004;127:17-28.
32. LundgrenD. Prosthetic reconstruction of dentitions seriously compromised by period-ontal disease. J Clin Periodontol 1991 Jul;18(6):390-5.
33. Malo P, Rangert B, Nobre M. «All-on-Four» immediate-function concept withBrånemark System implants for completely edentulous mandibles: a retrospectiveclinical study. Clin Implant Dent Relat Res 2003;5 Suppl 1:2-9.
34. Malo P, Nobre Mde A, Petersson U, Wigren S. A pilot study of complete edentulousrehabilitation with immediate function using a new implant design: case series. ClinImplant Dent Relat Res 2006;8(4):223-32.
35. Mariani P, Margossian P, Labprde G. Choix d’un concept occlusal en implantologie. 1repartie: donnees fondamentales. Strategie Prothetique 2008;8(1):5-13.
36. Marshall B F. Reconstitution des dents apres traitement endodontique. Revue deparodontie et de dentisterie restauratrice 7-29.
37. OrthliebJD, BrocardD, SchittlyJ, Maniere-EzvanA. Occlusodontie pratique. Paris: CdP2000;210p.
38. OyamaK, KanJY, KleinmanAS, Runcharassaeng K, Lozada JL, Goodacre CJ. Misfit ofimplant fixed complete denture following computer-guided surgery. Int J OralMaxillofac Implants 2009;24(1):124-30.
39. Okano N, Baba K, Igarashi Y. Influence of altered occlusal guidance on masticatorymuscle activity during clenching. J Oral Rehabil 2007;34(9):679-84.
40. Persson GR. Perspectives on periodontal risk factors. J Int Acad Periodontol 2008 Jul;10(3):71-80.
41. Picton DC, Wills DJ. Viscoelastic properties of the periodontal ligament and mucousmembrane. J Prosthet Dent 1978;40(3):263-72.
42. Pjetursson BE, Sailer I, Zwahlen M, Hammerle CH. A systematic review of the survivaland complication rates of all-ceramic and metal-ceramic reconstructions after anobservation period of at least 3 years. PartI: Single crowns. Clin Oral Implants Res 2007Jun;18 Suppl 3:73-85. Erratum in: Clin Oral Implants Res 2008;19(3):326-8.
43. Pjetursson BE, Bragger U, Lang NP, ZW Ahlen M. Comparison of survivaland complication rates of tooth-supported fixed dental prostheses (FDPs) and
PROSTHETIC RESTORATION OF THE CANINE
J Dentofacial Anom Orthod 2010;13:112-132. 131

implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res 2007 Jun;8Suppl 3:97-113. Erratum in: Clin Oral Implants Res 2008;19(3): 326-8.
44. RangertB, GunneJ, Glantz PO, Svensson A. Vertical load distribution on a three-unitprosthesis supported by a natural tooth and a single Brånemark implant. An in vivostudy. Clin Oral Impl Res 1995;6(1):40-6.
45. RangeriB. Biomecanique des implants de Brånemark. Implant 1995;1(1):63-74.46. Samama Y, Ollier J. La prothese ceramo-ceramique et implantaire. Reussir
Quintessence editeur.47. Sarment DP, Meraw SJ. Biological space adaptation to implant dimensions. Int J Oral
Maxillofac Implants 2008;23(1):99-104.48. Sadowsky SJ. An overview of treatment considerations for esthetic restorations: a
review of the literature. J Prosthet Dent 2006;96(6):433-42.49. SailerI, Pjetursson BE, Zwahlen M, Hammerle CH. A systematic review of the survival
and complication rates of all-ceramic and metal-ceramic reconstructions after anobservation period of at least 3years. Part II: Fixed dental prostheses. Clin Oral ImplantsRes 2007 Jun;18 Suppl 3:86-96. Erratum in: Clin Oral Implants Res 2008;19(3):326-8.
50. Serfati E, Decloquement C, Radiguet J. Les preparations corono-radiculaires des dentsdepulpees. Realites cliniques 1996;7(4):433-46.
51. Sharkey S, Chaollai AN, O’Sullivan M. A review of aggressive periodontitis and anassociated case report. Dent Update. 2009;36(1):38-40, 43-4, 47-50.
52. Spear F, Holloway J. Which all-ceramic system is optimal for anterior esthetics? J AmDent Assoc 2008;139 Suppl:19S-24S.
53. StuderS, Pietrobon N, Wohlwend A. Maxillary anterior single-tooth replacement:comparison of three treatment modalities. Pract Periodontics Aesthet Dent1994;6(1):51-60; quiz 62.
54. Tan K, Pjetursson BE, Lang NP, Chan ES. A systematic review of the survival andcomplication rates of fixed partial dentures (FPDs) after an observation period of at least5 years. Clin Oral Impl Res 2004;15(6):654-66.
55. Viargues P. La position des limites cervicales de preparation en prothese fixee. Analysede la litterature: consequences cliniques. Rev Odont Stomat 2005;34:3-18.
56. Wassell RW, Smart ER, St George G. Crowns and other extra-coronal restorations:cores for teeth with vital pulps. Br Dent J 2002;192(9):499-502, 505-9.
57. Zhiyong L, Arataki T, ShimamuraI, Kishi M. The influence of prosthesis designs loadingconditions on the stress distribution of tooth-implant supported prostheses. Bull TokyoDent Coll 2004;45(4):213-21.
PASCAL AUROY, JEAN LECERF
132 Auroy P, Lecerf J. Prosthetic restoration of the canine