Promote Breastfeeding Project Evaluation - City of Ballarat - … report 2010 cob... · Executive...
72
Promote Breastfeeding Project Evaluation BEST START PROJECT Final Report Dec 2010
Transcript of Promote Breastfeeding Project Evaluation - City of Ballarat - … report 2010 cob... · Executive...

1.
Promote Breastfeeding Project Evaluation
BEST START PROJECT
Final Report
Dec 2010

2.
Glossary of Terms
Executive Summary
Background
Evaluation of the Project
Methodology
Summary of Data
Review of the 2005-2010 Action Plan
Themes and from the Consultation process with Project Partners
Outcomes from the Breastfeeding Charter survey
Outcomes from the Infant Feeding Survey (July 2010)
Summary of all Recommendations
APPENDIX 1: Progress against the Ballarat Best Start Promoting Breastfeeding Action Plan
APPENDIX 2: Results from the City of Ballarat Infant Feeding Survey (July 2010)
3
4
6
7
8
9
14
16
25
27
30
33
46
Table 1: Number of total births in the City of Ballarat 2002-2009
Table 2: Percentage of children fully breastfed at discharge from hospital in Ballarat
Table 3: Percentage of children fully breastfed at 2 weeks in Ballarat
Table 4: Percentage of children fully breastfed at 3 months in Ballarat
Table 5: Percentage of children fully breastfed at 6 months in Ballarat
Figure 2: Percentage of children fully breastfed at discharge from hospital in Ballarat
Figure 3: Percentage of children fully breastfed at 2 weeks in Ballarat
Figure 4: Percentage of children fully breastfed at 3 months in Ballarat
Figure 5: Percentage of children fully breastfed at 6 months in Ballarat
9
10
11
12
13
10
11
12
13
Table of Contents
List of Tables and Figures
City of BallaratFinal Report against the Action Plan to Promote Breastfeeding in BallaratDecember 2010
3.
ABA
BCH
BDDGP
BFHI
BFWA
BHS
BLX
CALD
CoB
DEECD
GP
IBC
LC
LGA
MCH
PD
PND
SJOG
WHO
UFS
UNICEF
PODS
Australian Breastfeeding Association
Ballarat Community Health
Ballarat & District Division of General Practice
Breastfeeding Friendly Hospital Initiative
Breastfeeding Friendly Workplace Accreditation
Ballarat Health Service
Ballarat Learning Exchange
Culturally and Linguistically Diverse
City of Ballarat
Department of Education and Early Childhood Development
General Practitioner
International Board Certified
Lactation Consultant
Local Government Area
Maternal and Child Health
Professional Development
Post Natal Depression
St John of God Hospital
World Health Organisation
United Friendly Societies
United Nations Children’s Fund
Providing Opportunities and Developing Services for Young Parents
Glossary of Terms

4.
Since 2000/2001, breastfeeding rates across Ballarat have consistently been reported as being “below average” when measured at discharge, two weeks, 3 months and 6 months and compared to the Grampians regional average and the Victorian average. The low breastfeeding rates combined with the steady increase in the number of births indicated a need to implement strategies that would improve breastfeeding rates across the City of Ballarat. The Best Start ‘Promoting Breastfeeding Project’ worked with a number of key stakeholders to improve breastfeeding rates across Ballarat.
A ‘Promoting Breastfeeding Project’ Reference Group was established in 2004 as part of the Best Start project. Initial planning developed an Action Plan that involved a number of community organisations working collaboratively to address low breastfeeding rates in Ballarat. This Reference Group was initially formed and relied on project partners to volunteer time and resources. In February 2008, the City of Ballarat employed a project coordinator to progress the project further. At this time, priorities were identified by the Reference Group for implementation.
This evaluation has been developed in consultation with the Reference Group, and has been designed to provide a broad system review regarding the effectiveness of the partnership in promoting breastfeeding across the City of Ballarat. Several components are included in this review, including a summary of trend data (Section 1), a summary of the initial rationale and recommendations from the Action Plan 2005-2010 (Section 2), outcomes from consultations with individual project partners (Section 3) and outcomes from consultations with participants in the Ballarat Breastfeeding Charter (Section 4). In addition, parent experiences and influences on decision making were sought through a survey which was distributed through Maternal and Child Health services (Section 5), and a summary of all recommendations identified in this review is included in Section 6. Specific progress outcomes as measured against the Action Plan have been included in detail in Appendix 1.
The results of this review highlight several key issues. There is consensus within the Reference Group as well as across the community that it remains difficult to change community attitudes in order to develop a culture which is more supportive of breastfeeding. This culture has been encouraged through the marketing strengths of commercial stakeholders (e.g. pharmacies) and this practice is no longer consistent with the current research and evidence based practice.
Executive Summary

5.
There is consistent positive support for the value of the Ballarat Breastfeeding Charter in challenging some of these entrenched community values, which also promotes a positive culture towards breastfeeding practices within the community. However, there is also a “disconnect” between the positive views of project partners about the value of the Charter, and the experiences of Charter signatories. There is a clear indication from Charter signatories that they would value additional practical information and resources that would support them further.
Some of the clear outcomes of the project have centered around the value of the project coordination role which has been led by the City of Ballarat. There has been consistently positive in feedback from a range of stakeholders, with comments indicating that this is the best model to progress changes in community attitudes. No single partner has been able to take this lead role as effectively as Council, and there has been unanimous recognition and support for the value of this role.
One recommendation consistently raised was the need for an ongoing commitment to developing more consistent and collaborative data that can be used to inform planning and can be more responsive to changes that occur following the implementation of specific strategies. At this time, data is collected in different systems and with different reporting requirements, and therefore is not able to be used to its full potential.
In addition, there was strong and consistent support for the establishment of a breastfeeding support ‘drop in’ centre within the community. This centre would ideally be located in central Ballarat and would co-located with other community based parenting/early childhood services rather than an extension of the medical intervention model. Potential locations suggested included Girrabanya, the Library, a Neighbourhood House or a location within Central Square. Further exploration of this model was strongly supported, as many project partners provide part of this service and believe a co-located model would enhance the experience of the mother and increase opportunities to provide more consistent, and specialist information and advice when required.
Recommendations from each of the consultation processes have been included in each individual section. As noted above, Section 6 of this report has summarised all the recommendations made from each of the different consultation processes.

6.
In late 2004, a Reference Group was formed as part of the Ballarat Best Start project, to look at the issue of promoting breastfeeding in Ballarat. The Ballarat Best Start project has a prevention and early intervention focus that aims to improve the health, development, learning and wellbeing of all children from pregnancy through transition to school (usually accepted as 8 years of age).
This Reference Group led a project called the “Promoting Breastfeeding in Ballarat”, and included representatives from the City of Ballarat Best Start project, Ballarat group of the Australian Breastfeeding Association (ABA), Maternal and Child Health (MCH), Ballarat Health Services (BHS), St John of God Hospital Ballarat (SJOG), Childcare and kindergarten, Ballarat Community Health (BCH), Ballarat Regional Multicultural Council (BRMC), the Ballarat and District Aboriginal Cooperative (BADAC), the Department of Human Services, The Ballarat and District Division of General Practice (BDDGP), parents and others.
A key issue in initial consultations and data review was the low and declining breastfeeding rates in Ballarat. The data indicates that while a large proportion of women initiated breastfeeding, the ‘drop off’ rate was very high. The rates for breastfeeding in Ballarat for infants aged 3 months, and 6 months have continued to be lower than the State average, the Metropolitan average, the regional average and the Grampians regional average.
The goal of the ‘Promoting Breastfeeding in Ballarat’ project was that Breastfeeding rates in the City of Ballarat will increase to achieve the national targets for exclusive breastfeeding of 95% at initiation, 80% at 3 months, and 60% at 6 months.
The overall objectives of the project were summarised as follows:
Raise awareness amongst the wider Ballarat community regarding the importance of •breastfeedingStrengthen the capacity and commitment of the professional and business sector in •Ballarat to work collaboratively to promote and support breastfeedingImprove awareness, knowledge and skills amongst parents by providing up to date, •accurate and local informationDevelop supportive environments: schools, hospitals, restaurants, leisure centres, •libraries, shopping centres and so on.
Background

7.
In order to achieve these objectives, a 5 year Action Plan (2005-2010) for the Best Start Ballarat Breastfeeding Project was developed. This identified a range of barriers to breastfeeding in Ballarat, as well as goals and actions to promote breastfeeding. Local barriers aligned with those identified by the Australian Breastfeeding Association (ABA), the World Health Organisation (WHO) and other research. This Action Plan is now finished.
The initial project planning and implementation of the project was based on voluntary contributions including time and resources from project partners. Initial meetings were through open invitation, and this was formalised when the project coordinator commenced. Comments indicated that these early project meetings were often considered to be challenging and individuals defended their own organisations, and that collaborative partnerships were not achieved in these early stages. When the project was formalised, participants in the Reference Group were specifically selected to represent a range of organisations.
Evaluation of the Project
The ‘Promoting Breastfeeding in Ballarat’ project has provided a broad system review against the Action Plan (2005-2010). This has included evaluating the following areas:
Project process and key milestones achieved 1.Impacts and challenges to the implementation of the Action Plan2.Review of the relevance of the Action Plan initiatives3.Review of the strength and effectiveness of the partnership4.Review of the effectiveness of the Breastfeeding Charter 5.Reflections from partners on improving the process for future decision making and 6.coordinated planning of future projectsReview of the data that has been collected and collated to date, including the effectiveness 7.of how this is presented and usedRecommendations from partners for further initiatives 8.
In order to review these outcomes, the following methodology was developed.

8.
Lynne Gleeson, a private consultant, was employed to carry out the evaluation and provide the final report. The City of Ballarat provided day to day guidance for the project, and the “Promoting Breastfeeding in Ballarat” Reference Group provided additional guidance for the evaluation and methodology. The following members of the Promoting Breastfeeding in Ballarat Reference Group participated in the evaluation of the project:
City of Ballarat (Best Start Project Coordinator)1.City of Ballarat (Promoting Breastfeeding Facilitator)2.Ballarat Health Services3.Ballarat Community Health 4.Ballarat & District Division of General Practice (2 representatives)5.Centacare Catholic Diocese of Ballarat6.St John of God Ballarat (2 representatives)7.City of Ballarat Maternal and Child Health Coordinator 8.City of Ballarat Maternal and Child Health Nurse9.
Each of the project partners participated in an individual interview. Two organisations had two representatives interviewed due to different roles or changing staff through the project. This resulted in 11 interviews being completed in August 2010. An online survey was developed to survey the Breastfeeding Charter participants, and 34 email invitations were sent to Breastfeeding Charter signatories in August 2010. This online survey was available for a period of 2 weeks, and 17 Breastfeeding Charter Signatories provided feedback through completed surveys. A further 6 surveys were incomplete, resulting in a total of 23 responses.
The results of the review are presented in the following sections:
Summary of data1.Review of the 2005-2010 Action Plan2.Themes from the Consultation process with Project Partners3.Outcomes from the Breastfeeding Charter survey 4.Outcomes and Recommendations from the City of Ballarat Infant Feeding Survey (July 2010)5.Summary of all Recommendations6.Progress against the Ballarat Best Start Promoting Breastfeeding Action Plan (Appendix 1)7.Results from the City of Ballarat Infant Feeding Survey (July 2010) (Appendix 2)8.
Methodology

9.
1. Summary of Data
Table 1: Number of total births in the City of Ballarat 2002-2009
The Promoting Breastfeeding Partnership was established in 2004, and was the first partnership of its type where all relevant stakeholders came together to address the issue of poor breastfeeding rates, possible reasons for these low rates, but more importantly, identify and implement potential solutions. The group initially invested time to ensure that all stakeholders were represented and able to make decisions, were committed to the overall objective of the project and felt trusted and supported. The partnership has remained in place since that time and has continued to implement projects in line with the Action Plan. The partnership has also contributed to positive changes across the service and community sector and there are now some improvements in breastfeeding rates.
Table 1 below represents the number of births for the City of Ballarat between 2002 and 2009, including data from BHS and SJOG. This indicates a strong increase in the number of births since 2003.

10.
According to the State-wide data provided since project commencement there has been an increase in Ballarat’s Breastfeeding rates at 3 months and 6 months. This can be seen from years 2004 to 2008 in the following graphs:
In 2007/08 the percentage of children fully breastfed at 3 months in Ballarat was •49.3%. An increase of 5.8% from 2004/05. In 2007/08 the percentage of children fully breastfed at 6 months in Ballarat was •34.7%. An increase of 4.5% from 2004/05.
Figure 2 and Table 2 below represent the percentage of children fully breastfed at discharge from hospital within the City of Ballarat. Review of trends indicates inconclusive patterns, as there is a strong increase in 2007-2008 following a sharp decrease in 2006-2007. Further data over a longer period would provide a better perspective of recent trends.
Figure 2: Percentage of children fully breastfed at discharge from hospital in Ballarat
Table 2: Percentage of children fully breastfed at discharge from hospital in Ballarat
Year
Ballarat
Grampians
Victoria
2000-1
77.49
79.1
78.99
2001-02
85.53
82.19
78.56
2002-03
79.15
79.01
77.87
2003-04
74.9
77.4
76.8
2004-05
74.1
76.2
74.8
2005-06
75.9
77.5
75.8
2006-07
67.5
72.8
74.6
2007-08
74.9
76.8
74.7

11.
Figure 3: Percentage of children fully breastfed at 2 weeks in Ballarat
Figure 3 and Table 3 below represent the percentage of children fully breastfed at 2 weeks within the City of Ballarat. This indicates that there is an increase in breastfeeding at this stage from 2006-2007 to 2007-2008. On a positive note, there is an indication that breastfeeding rates are no longer falling, as they were between 2001-2002 and 2004-2005.
Table 3: Percentage of children fully breastfed at 2 weeks in Ballarat
Year
Ballarat
Grampians
Victoria
2000-1
70.22
72.68
72.15
2001-02
79.49
75.71
72.05
2002-03
77.07
71.49
70.32
2003-04
67.1
70.4
69.8
2004-05
65.2
68.1
66.7
2005-06
68.3
69.5
69.7
2006-07
64.9
67.6
68.6
2007-08
67.7
69.8
68.7

12.
Figure 4 and Table 4 below represent the percentage of children fully breastfed at 3 months within the City of Ballarat. This indicates that in 2007/08 the percentage of children fully breastfed at 3 months in Ballarat was 49.3%, representing an increase of 5.8% from 2004/05.
Figure 4: Percentage of children fully breastfed at 3 months in Ballarat
Table 4: Percentage of children fully breastfed at 3 months in Ballarat
Year
Ballarat
Grampians
Victoria
2000-1
51.4
54
53.1
2001-02
53.8
53.1
52
2002-03
47.5
50.3
50.6
2003-04
42.7
49.1
49.1
2004-05
43.5
48.1
48.5
2005-06
48.5
50.8
51.8
2006-07
45.5
50.4
51.8
2007-08
49.3
51.7
52.4

13.
Figure 5: Percentage of children fully breastfed at 6 months in Ballarat
Figure 5 and Table 5 below represent the percentage of children fully breastfed at 6 months within the City of Ballarat. This indicates that in 2007/08 the percentage of children fully breastfed at 6 months in Ballarat was 34.7%, representing an increase of 4.5% from 2004/05.
Table 5: Percentage of children fully breastfed at 6 months in Ballarat
Year
Ballarat
Grampians
Victoria
2000-1
38.7
41.6
40.1
2001-02
38.9
39.9
398.8
2002-03
35.7
38.8
37.9
2003-04
28.7
37.1
37.1
2004-05
30.2
35.7
37
2005-06
35.1
39.6
38.7
2006-07
34.3
38.3
38
2007-08
34.7
37.4
38.9
Recommendation: Whilst these rates show a slight improvement, the partnership has identified an issue with accurate data collection, as the two hospitals and the MCH service collect this information differently, and at different times. This means that local data can show up to a 20% variation between service collection and state-wide data.

14.
2. Review of the Action Plan 2005-2010
The initial Action Plan for the ‘Promoting Breastfeeding in Ballarat’ project was first initiated after the establishment of a working group in late 2004. The following rationale and summary of evidence provided the framework for the development of the ‘Promoting Breastfeeding in Ballarat’ Action Plan at that time.
Why breastfeeding is important
UNICEF states breastmilk alone is the ideal nourishment for infants for the first six months of life. Only breastmilk contains all the nutrients, antibodies, hormones, immune factors and antioxidants an infant needs to thrive. Colostrum immediately following birth, and the breastmilk that follows, protects infants from disease. In addition to this profound impact on child health and well-being, breastfeeding:
Assists maternal recovery and reduces incidence of cancers•Is convenient and cost-effective •Enhances the special bond between mother and child•Is environmentally friendly•Is the normal way to nurture a baby•
Basic Facts about Breastmilk
The most natural, fresh and best nutrient for all infants•Always safe and free from harmful microbes•Ready at all times without any cost. No special spending•Fully and easily digestible i.e: artificial feeding increases the incidence of diarrhoea, •colic and constipationActivates the immune system, for example, colostrum immediately following birth •protects infants from diseases Contributes to muscular and bone development•Contributes to mental development•Fully meets the water requirements of the infant; there is no need for extra water•Breastfeeding contributes to the health of the mother and baby by reducing the risk of •breast and ovarian cancer

15.
What others are doing
WHO and UNICEF jointly developed the “Global Strategy for Infant and Young Child Feeding” (Geneva, 2003) to revitalise world attention to the impact that feeding practices have on the nutritional status, growth and development, health, and thus the very survival of infants and young children.
The Global Strategy is based on the evidence of nutrition’s significance in the early months and years of life, and of the crucial role that appropriate feeding practices play in achieving optimal health outcomes. Lack of breastfeeding, and especially lack of exclusive breastfeeding during the first six months of life, are important risk factors for infant and childhood morbidity and mortality that are only compounded by inappropriate complementary feeding.
The life-long impact includes poor school performance, reduced productivity, and impaired intellectual and social development. The Strategy is intended as a guide for action; it identifies interventions with a proven positive impact, it emphasises providing mothers and families the support they need to carry out their crucial roles, and it explicitly defines the obligations and responsibilities in this regard of governments, international organisations and other concerned parties.
A DHS report, “Giving Breastfeeding a Boost” (2005), reviewed community based approaches to improving breastfeeding rates and concluded that “strategies often appear to be uncoordinated and lack a centrally driven integrated plan” (page 34). Other groups and organisations, such as the Australian Breastfeeding Association (ABA), have long been supporting breastfeeding and providing information about the importance of breastfeeding.
The ABA’s mission states that: “As Australia’s leading authority on breastfeeding, we educate society and support mothers, using up-to-date research findings and the practical experiences of many women. We work to influence society to acknowledge breastfeeding as normal, and important to skilled and loving parenting.”
Appendix 1 in this report provides the Action Plan and articulates the progress against each initiative. This also provides a summary of the project since the Action Plan was developed in 2005, and includes recommendations for future directions.

16.
1. Themes from the Consultation process with Project Partners
Successful Outcomes of the Project
The most commonly identified key outcome of the project has been an increased awareness
about low breastfeeding rates in the City of Ballarat and an increase in awareness and support for breastfeeding across the community. There were several comments made that the project raised awareness in the community about the importance of breastfeeding and some of the challenges that were apparent, and there was strong consensus that there was still ongoing work to be done to ensure that support for breastfeeding was seen as part of the “social fabric” within the community. This issue was promoted through the use of stickers, postcards, posters, magnets and other resources that support breastfeeding and were specifically targeted to services within Ballarat. There was also recognition of the benefits of these resources being available at a variety of functions and events, and this in turn raised awareness of breastfeeding.
Several project partners raised questions about the appropriateness of the “Oh My God” media campaign which aimed to increase community awareness; however, all partners have been in agreement that the campaign was effective in achieving its objective. The campaign was particularly effective in creating a talking point across a range of sectors within the community and in raising the general awareness of low breastfeeding rates in Ballarat. It is acknowledged that all project partners were in agreement at the time of the initial campaign, however, some project partners changed individual staff representatives and this again raised the question about the appropriateness of this particular campaign.
A second key outcome of the project has been the support from the project and the Steering Group for organisations to achieve Accreditation standards that support breastfeeding. BHS has re-applied
and recently been assessed in terms of achieving accreditation as being a Baby Friendly Hospital Initiative (BFHI) workplace, a process that incorporates encouraging breastfeeding across the health service for staff and for the public. Ballarat Community Health (BCH) and the Department of Education and Early Childhood Development (DEECD) have both initiated the process to achieve Breastfeeding Friendly Workplace Accreditation (BFWA). Centacare Ballarat is also in the initial stages of planning for this accreditation. The City of Ballarat has achieved this accreditation and has also achieved UNICEF acknowledgement as a Child Friendly City. This formal recognition has been achieved by only one other Council in Australia, and the City of Ballarat is the first Council to achieve this in Victoria.
The Breastfeeding Charter was initially established with a “low key” and “passive” approach. There were initial concerns that the “Promoting Breastfeeding in Ballarat” project may be perceived as being aggressive in challenging community attitudes. As a strategy to mitigate this perspective, marketing and promotional materials were generally developed to be delivered in a non intrusive or aggressive approach. There was strong support for the specific strategy to promote and implement the Breastfeeding Charter across the business sector. The Breastfeeding Charter has been effective in increasing awareness of breastfeeding and in promoting breastfeeding friendly workplaces and rooms. The Charter has provided the basis to clarify how businesses can actually support breastfeeding and provide concrete/tangible outcomes.
There has also been consistent support for organisations that support the availability of breastfeeding rooms. This includes those that are supported through the City of Ballarat, for example,

17.
the breastfeeding room at the Phoenix Building and support for breastfeeding at the Girrabanya Children’s Centre. The Girrabanya model has received positive support as it is collocated with other services (including MCH and Reception staff), although it has been only able to operate informally on a limited basis as a “drop in” centre.
There has been strong support for the involvement of a General Practitioner in the Project Group, and the opportunities that this has to link with other GPs. More specifically, there has been a strong appreciation within the group of having a GP who is enthusiastically engaged with the project and who is able to provide considered and relevant information for GPs. This has raised awareness in other GP practices and opportunities to continue to provide information, including LACFACTS, contact information on magnets, access to drug information and links to women’s websites as well as a checklist of breastfeeding. This also extends to the involvement of the Ballarat & District Division of General Practice (BDDGP) which has provided GPs with information on a regular basis.
There has been strong support for the opportunity for relevant professionals to access Professional Development (PD) opportunities. For example, MCH Nurses can now access 8 hours of e-learning through a module that is funded and supported by DEECD. Resources include DVDs and a textbook. This opportunity is available to all permanent staff within the City of Ballarat as well as all Casual MCH staff (funding is provided through Council for Casual MCH staff). This project has also provided support and funding for Lactation Consultant (LC) training. Opportunities to attend and participate in professional conferences and study days also occurred under the umbrella of this project.
There was consistent support for the effectiveness of the facilitator role. Project partners who had been involved in the project since the beginning, consistently articulated that the project had significantly progressed
after the appointment of a project facilitator who was able to allocate specific resources, including time. This provided a catalyst to progress the project and provide support and encouragement to achieve sustainability. The facilitator was also identified as a key and valuable resource to disseminate current and relevant information regarding the latest research. Information provided through both the facilitator role and the ABA was consistently recognised as being valuable, as it provided information from multiple sources. There was consistent support that the project, and the project coordination role, should be located within Council, as Council was best placed to represent broad community needs. There was recognition and appreciation of the leadership role that had been achieved by Council, for example, through the availability of a breastfeeding room in the Phoenix Building.
There was also strong recognition that the project provided an important catalyst for collaboration between different organisations within Ballarat. Many project partners indicated that they were unaware of the low breastfeeding rates across Ballarat, particularly compared to other local government areas. The project provided opportunities for networking and to share information and resources, for example, access to the drug information line and checking medications.
Consultations also highlighted differences in practices between organisations, for example, SJOG has different clientele and different support systems in place. The project was effective in ensuring that project partners were aware of the other service providers in the wider community and how they operate. There were also opportunities to share how the breastfeeding project related to other projects within organisations, for example, Centacare, Catholic Diocese of Ballarat, has a focus in working with parenting education and skills development. Centacare also has a service for “mother support”, for mothers with a mental illness. This project is able to readily link with these specific projects and staff.

18.
Impacts and challenges to the implementation of the Action Plan
The most common issue raised during interviews with project partners was the difficulty reported
by mothers in obtaining consistent advice and information. It was acknowledged by many project partners that mothers reported that information was confusing and they found it difficult to access information at the right time, as the professional person was often changing in the baby’s first two weeks (hospital, domiciliary and MCH), as were the needs of the mother and baby. This creates an opportunity to explore the ability/expectations of mothers in being able to interpret and use the information provided. It was also noted that some health professionals (e.g. some GPs and MCH nurses) were not consistently using evidence based materials.
There was also recognition of the complexities in supporting women who are having difficulties with breastfeeding. This support is required when mothers are particularly vulnerable and sensitive, and there are difficulties in “normalising” breastfeeding in an environment where community attitudes are not consistently supportive. There is a need for role modelling and community education and awareness to support “normalising” breastfeeding practices.
It was also recognised that skill and knowledge levels vary across the sector. This adds further difficulties in being able to deliver consistent advice to mothers. While evidence based information is promoted, not all information is consistent.
This issue of inconsistent information is also apparent with some GPs (acknowledging that some GPs are excellent). It has also been acknowledged that information can be provided to GPs and that the most successful strategy has been developing readily accessible resources, e.g. phone numbers
on magnets. There has been an ongoing issue with engagement of GPs, although the specific support for this project through the GP representative and the BDDGP has consistently been reported as excellent.
It was consistently acknowledged that there were difficulties in continuing to encourage breastfeeding in the immediate period after discharge from hospital. This is represented through the strong decline in breastfeeding rates after the first 2 weeks, and reflects the lack of support available to manage the complexities and challenges of the transition between the hospital service through the Domiciliary service and then linking with the community based MCH service. This difficulty is also exacerbated by data systems which measure breastfeeding differently.
Also, in the past, some individual MCH staff had a history of working closely with commercial companies providing artificial infant formula products, and these products have been stored and used in individual centres, which was in conflict with breastfeeding promotion and evidence based practice. This system has been reviewed during this project. The changes have been implemented successfully, albeit with initial resistance from some individual MCH staff.
There was consistent agreement between project partners about the difficulties in addressing complex community attitudes. There was acknowledgement that community attitudes now appeared to be less positive about breastfeeding, despite the increased evidence base that supports breastfeeding. This is exacerbated within the Ballarat community where breastfeeding rates are historically low and there are prevailing community attitudes which are entrenched through generational behaviours. This

19.
creates additional barriers when trying to support and encourage community change and awareness, and project partners articulated that complaints continue to be made about breastfeeding activity in public places. The difficulty in changing community attitudes has been identified as an ongoing challenge for the project.
Project partners were very supportive of the role of the Breastfeeding Charter in facilitating and supporting the changes in community attitudes. There was strong support for extending the current model and seeking additional members. This would also involve targeting specific selected organisations to be Charter signatories, e.g. Ballarat Learning Exchange (BLX) and the Link Up program. This could also include a review of the role of schools, where the Charter may be relevant for some staff and also for parents (particularly in primary schools).
Project partners raised conflicting views of the role of the Breastfeeding project in schools, and this creates an opportunity to review the role of the project in terms of how breastfeeding education is provided in secondary schools (generally linked with Health & Human Relations). As discussed in the following section, primary schools have been identified as part of extending the current model for the Breastfeeding Charter. However, there is an opportunity to review the role of breastfeeding education in both primary and secondary schools, including how this is incorporated into the school curriculum with a view to “normalising” breastfeeding within the community over the longer term.
Providing recognition for formal qualifications and skills has been identified as an issue for the MCH Nurses. There is currently no additional recognition for MCH staff who have LC qualifications, and
therefore, there is no financial incentive for having this qualification. As noted previously, there has been good support for training and professional development opportunities which have been available through this project.
A further challenge highlighted through the project is the relationship between the MCH service and current business practice in industry, for example, pharmacies. The availability and promotion of artificial infant formula products is well established, and there are ongoing issues with the implementation of evidence based practice which is often not aligned with commercial practice. This is a complex relationship which requires further work to develop a shared understanding of roles and practices. For example, this would include developing a shared understanding of the ethical positions of implementing evidence based practice and informed consent as compared with commercial practice.
Additional issues have been identified in the area of workplace barriers, for example, the demands on women who are returning to the workplace within 6 weeks. It is acknowledged that there is a need for further education and discussion within workplaces about how to return to work and in assisting in developing routines that support breastfeeding within the workplace. This is closely aligned with developing family friendly policies in the workplace, and it is acknowledged that team support, flexibility and good will is required from all parties involved.
There were difficulties identified in managing data, with no consistent criteria in place across different components of the sector. More specifically, there are different systems and definitions in place for the hospital period, the Domiciliary service and the MCH service. These systems are established and

20.
implemented through funding arrangements, with no flexibility in implementation. This exacerbates discrepancies in data between the hospital system and the MCH system, where it is possible to identify differences but not develop a standard report that can be used to benchmark or provide comparisons. There was support for implementing the WHO guidelines for normalised growth charts for babies who have been primarily breastfed. The use of these growth charts would not change breastfeeding rates and the data collected, but would impact on the interpretation of growth charts and create a different evidence base that is more relevant and accurate for breast fed babies. It was noted that the use of the current growth charts is under review, along with other information in the Child Health record book.
The difficulty in obtaining support from some Council Departments was also consistently identified as one of the challenges. This was primarily directed to difficulties in being able to access internet information about breastfeeding, as access to sites were blocked through current CoB policies. This may reflect additional IT security which has been implemented, or may reflect difficulties in MCH staff having access to ongoing training in how to work within these constraints. Difficulties were also articulated in managing the Charter with the current IT system, as registrations to join the Charter received online through the CoB website have not been consistently accessible by project staff since November 2009. This has presented an ongoing difficulty in progressing the Charter. This issue was also reflected with challenges in using the CoB media and promoting materials that include words and images that support breastfeeding. This promoted the inherent message that breastfeeding should be “hidden” from the public view and was supporting the community culture that was not positive about breastfeeding practices. This project
was intended to increase awareness of the positive aspects of breastfeeding, however, partners were very aware of the difficulties in getting this support from some parts of the CoB organisation. This appeared to represent a conflict between policy and practice within the lead organisation.
Challenges for the ongoing project were identified as: the complexities in maintaining project momentum, keeping partners engaged, and the need for ongoing funding. This includes achieving consensus between partners on where to focus energy and resources and a process for re-evaluating the aims and next steps.
Many partners also identified the challenge of consistently engaging with the ABA in Ballarat, which was noted to be a missed opportunity in this project. This identifies an opportunity to develop closer links with the ABA, Ballarat.

21.
Project partners who participated in the interview process were unanimous in confirming that the project was highly relevant for organisations that had continued to be involved. The Action Plan initiatives were relevant and strongly supported by partners, and provided an opportunity for project partners to work collaboratively to promote community support for breastfeeding. It was acknowledged that the Project had provided a key role in distributing information to a range of stakeholders, including parents, the community, other health professionals and GPs. The information was relevant and was able to be used readily in staff training.
Project partners who had been involved since the start of the project were unanimous in their support for the appointment of a project coordinator and the leadership role shown by Council. Project partners were also consistent in their support for placing a high value on the networking that now takes place through the project. One of the key strengths identified was the benefit of being able to share information and resources from different perspectives. Many partners identified how they were often isolated and were not always aware of how the other parts of the system worked together. The effectiveness of the project was enhanced through exchanging information and understanding the transition/journey of the mother through the different systems, including public and private hospital systems as well as MCH, Domiciliary and BCH services.
It was acknowledged that hospital based services only engaged with women for a very short period of time, and had a limited influence on breastfeeding practices, particularly where the main influence was from the community. This project was highly relevant in being able to provide feedback to the hospital system and how this practice can be linked more positively with community based services, leading to a more cohesive transition from the intensive services into the community.
As well as the benefits of the networking and information/resource sharing, the project partners also clearly identified the benefits of having good partnerships and group dynamics within the group, which is represented through the genuine respect and openness to work collaboratively to address a common goal. The links that were established between antenatal clinics and GPs as well as between hospital services and community based services was consistently identified as demonstrating good support systems. The good will in this partnership facilitated the smooth resolution of possible conflicts between partners.
Review of the relevance of the Action Plan initiatives
Review of the strength and effectiveness of the partnership

22.
Generally, the project was identified as meeting expectations. There was strong support for the opportunity and ability to identify and act on issues in a way which led to tangible results. Breastfeeding rates in Ballarat are currently increasing and the project appears to be gaining momentum. There was consensus amongst project partners that there is an ongoing role for the project, including extending it to engage policy makers directly.
In addition to meeting expected outcomes, there were several unexpected and mostly successful outcomes. For example, DEECD committed funds to provide 8 hours of training for MCH Nurses, and Council and the Best Start Project have also provided funds for training. Another unintended outcome was the range of available information that could be used in a positive way and which could be shared both between organisations and with other staff.
The opportunity to visit and explore breastfeeding “drop in” models was also identified as an unexpected success of the project. This specifically related to visits to the Dandenong Breastfeeding Centre and to the ABA Headquarters Resource Centre. This provided valuable background information to be able to consider options that may be relevant for Ballarat.
There were also some negative views given about the visual graphics on the pamphlet that was produced as part of the media and community awareness campaign. In addition, some negative comments were made about the emphasis and time given to the development of a Raphael Centre
in Ballarat (a peri-natal infant mental health facility providing intensive support for mothers, families and babies). However, it was also acknowledged that the efforts made in these discussions were in the context of establishing a breastfeeding ‘drop in’ facility, and that these two centres (the Raphael Centre and the ‘drop in’ facility) could be linked. Unfortunately, this was identified as not being an option when funding was specified.
Unexpected Outcomes

23.
There was strong and consistent agreement from project partners to continue to explore the opportunities for establishing a breastfeeding “drop in” centre that would support women who are breastfeeding. It was acknowledged that it would be ideal if a range of organisations could be represented, including universal and generalist services as well as specialist services, e.g. LC and MCH services as well as parenting and early childhood services and resources. This would support women in being able to access a range of services if they were required and provide an opportunity to be able to access a range of available information e.g. parenting information and resources. Several other Councils have developed breastfeeding “drop in” centres, including Carlton, Casey, Brimbank and Melton.
Considerations around recommendations for the breastfeeding “drop in” model were consistent. They indicated that it needed to be a separate location away from hospital services, representing the transition to, and engagement of, community based services. It was strongly recommended that whilst the birthing services required the intensive services within the hospital setting, the breastfeeding component should be strongly embedded in the community sector. Many options were proposed for the location of a breastfeeding “drop in” service, including Girrabanya, the Library, a Neighbourhood House or the Central Square shopping precinct. Anecdotal information from the Council/United Friendly Societies (UFS) MCH model indicates that some parents who access a “drop in” service may not attend other services and that these parents may then be linked with other mainstream services as an outcome of attending the “drop in” service.
When asked about appropriate times for the “drop in” centre, it was generally agreed that it should be available 6 days per week, where it could be used if there were no supports and/or the family had just moved to Ballarat/was visiting or if referrals were needed. The opportunity to provide services for 6 days per week also supports the role of the father in the breastfeeding process. It was identified that phone support was often effective, but that interventions achieved more effective outcomes where 1:1 attention was available. This would provide strong community based support in the first few weeks after birth, and would directly target additional resources to support breastfeeding during the first 2 weeks. This “drop in” centre concept also supported women learning from, and supporting each other in a professional setting.
Depending on the “drop in” centre model developed, staffing may or may not be identified as an issue. Many organisations are currently providing a support service which could be considered to be appropriately delivered within a “drop in” outreach model. The majority of project participants indicated that a “drop in” model would ideally be available for some period daily for 6 days per week (not a full time service, but open for a short/selected period each day). Key staffing would be recommended to include specialist LC and MCH staff, ABA volunteers and hospital outreach (including Domiciliary) services. Further work and negotiation between project partners is required to implement this.
Project partners indicated strong support to continue expansion of the Breastfeeding Charter. This was identified as an opportunity to promote community awareness of low breastfeeding rates and to promote locations and facilities where breastfeeding was positively supported.
Recommendations from partners

24.
Project partners also recommended further review of engagement with schools. This could be achieved through a coordinated/systematic approach within schools, and links with the School Nursing service. It was also identified that there were different needs in primary and secondary schools, where primary schools may be supported through the Breastfeeding Charter and where secondary schools may be supported through incorporating breastfeeding information into the curriculum.
There was strong support to continue engagement with GPs, including education and training for GPs and practitioners. This would also be extended to include pharmacists and pharmacy staff. This would be achieved through extending Professional Development opportunities for more participants, and support for practitioners who do work in the field, e.g. through recognition and public awareness. It is important to focus on breastfeeding and to keep other issues separate, for example, mental health or teenage pregnancy, and to be targeted about key messages to the community which are specifically about breastfeeding.
A further recommendation would be the establishment of a working group for data review and management. This group would have the responsibility of sourcing local data which could be used to inform local initiatives and planning within the constraints of current data systems and reporting requirements. This may also include reviewing opportunities that are available through the new MCH data system which has the capacity to generate different data and reports. This group would also seek commitment from partners to share data that is collected and how it is used collaboratively within the project.
It was also acknowledged that there needs to be an increased focus in the next phase of the project to provide information to culturally and linguistically diverse (CALD) groups. Through the Best Start project, there are opportunities to have formal meetings with different CALD groups to progress breastfeeding in a culturally sensitive, gendered approach.

25.
When asked about the motivation to join the Breastfeeding Charter, the majority of responses identified the theme of wanting to participate in increasing community awareness regarding the importance of breastfeeding. This included support for promoting breastfeeding as a community value through broad community support. There were many comments relating to concerns about the low breastfeeding rates in Ballarat and wanting to participate in raising community awareness to address this issue.
In August 2008 the City of Ballarat launched the Best Start Breastfeeding Charter in response to poor breastfeeding rates in Ballarat. The Charter calls on businesses, agencies and groups to look at ways they can support and promote breastfeeding.
The Charter provides a simple guide to the options available to support breastfeeding in our community.
Many comments were positive about efforts that encouraged breastfeeding. This included support for promoting the value and importance of breastfeeding within the community and being proactive in addressing low breastfeeding rates in Ballarat. More specifically, there was consistent support for providing public places and facilities where breastfeeding is welcomed and encouraged. This was supported as an opportunity to provide practical assistance in raising community awareness.
There were also many comments that indicated joining the Charter was specifically to support individual businesses, for example, ensuring that the space was inclusive for all young people (including young parents) and providing a welcoming environment for mothers and babies. For some businesses, supporting the family and children) was part of core business, and participating in the Charter was consistent with these values. There were also comments that indicated that the business had signed the Charter at the request of staff or in response to being able to directly support staff.
There are a number of options available for organisations which include displaying a Breastfeeding Welcome Here sticker, obtaining Breastfeeding Workplace Accreditation or developing Maternity Leave policies to include lactation breaks.
Charter signatories then have the option of being listed on the City of Ballarat website.
Joining the Charter also provided opportunities to encourage staff to discuss the issue and develop a better understanding of the needs of mothers/parents. In one business, it was identified that it helped to support staff to continue to breastfeed within the workplace. It also provided a good opportunity to connect with other local businesses that had a common view towards breastfeeding.
3. Outcomes from the Breastfeeding Charter survey
Motivation to join the Charter
Motivation to join the Charter
Good points about the Charter

26.
When asked if there were positive outcomes for staff, there were many comments that indicated that staff had an increased awareness of the importance of breastfeeding and how to support this in a practical way. There were also comments that joining the Charter acknowledged the importance of breastfeeding and provided an opportunity for open discussion. Some responses also indicated that the Charter supported staff to review facilities within the business, including making change tables and “Wet-Ones” available. If these facilities were not
When asked about the benefits to customers and clients, responses were equally divided. Many responses indicated that mothers were able to use the facility and that it provided an opportunity to breastfeed in a welcoming and supportive environment. There were comments that women often came back and used the facility again. Some businesses indicated that facilities were used occasionally, but that this was positive in promoting positive breastfeeding messages and awareness of breastfeeding.
Responses about whether joining the Charter has supported the business have been mixed. The majority of respondents indicated that there had been no specific or direct benefits, or that it has been hard to identify the benefits. However, there were several responses that indicated that there had been benefits, including promotion of
able to be incorporated, there were comments that other changes were made to support staff who wished to breastfeed, including review of policies and facilities.
In addition, some respondents indicated that the Charter had made neither a positive or negative impact. There were also some comments that there had been little change since the Charter had been implemented, rather that the Charter articulated and supported current work practices.
In contrast, many comments indicate that businesses have not seen benefits for customers and clients, with one comment articulating that clients may not bring young children to the business. This may be due to the type of business or may be because customers/clients do not know that it is a breastfeeding friendly business.
the business and being able to provide a service/opportunity that was consistent with the objectives of the business. Two respondents indicated that there had been little change for the business since joining the Charter as the principles and practice were already in place.
Positive outcomes or changes for staff
Benefit to your customer/client
Support for the business
The majority of other comments indicated that the Charter has been good at raising community awareness but needs continued support and continued promotion. The majority of respondents indicated positive support for the Charter and support for it to continue.
Other Comments

27.
This project involved the development of the City of Ballarat Infant Feeding Survey, which was developed to gauge the views of parents with young children about their infant feeding choices, for example, whether exclusively breastfeeding, bottle feeding expressed breast milk, bottle feeding with artificial infant formula or a combination of these. The project also aimed to identify influences which assisted parents to make these choices. For example, if the method of feeding changed, the reasons/influencing factors for changing. The survey also included some questions about consumer satisfaction or dissatisfaction with professional breastfeeding support services in Ballarat, including providing some information about their breastfeeding experiences in Ballarat.
The survey was delivered through local City of Ballarat Maternal & Child Health Centres (M&CH), the Ballarat Community Health “Providing Opportunities and Developing Services for Young Parents” (PODS) Project and the Ballarat Secondary College “Link Up” Program.
The full results for this survey are included as Appendix 2 in this report.
The City of Ballarat Infant Feeding Survey was designed in collaboration with the ‘Promoting Breastfeeding in Ballarat Project’ Reference Group, key stakeholders and with the assistance of an external consultant, Lynne Gleeson. A second consultant, Carly Wemyss, was then employed to deliver the survey.
Carly Wemyss visited each M&CH centre personally and delivered the surveys. The surveys were left in the waiting area of the M&CH Centres for clients to complete if they wished. Participation was entirely voluntary. The PODS and Link Up groups were given surveys personally by their respective workers, and the PODS surveys were returned via post. The M&CH Centre Nurse located at one site personally gave out and collected surveys.
Each centre was given 30 surveys, with an accompanying explanatory poster and drop boxes for completed surveys. The survey form included a short explanation of the City of Ballarat Infant Feeding Survey and the Promoting Breastfeeding Project.
The time period from delivery to collection was November 10th 2009 to January 8th 2010.
4. Outcomes from the Infant Feeding Survey (July 2010)
Survey Methodology

28.
In total there were 300 surveys delivered with 155 being completed, representing a 52% response rate. Completed surveys were obtained from the following locations:
Barkly Street M&CH centre: completed 100%Buninyong M&CH centre: completed 100%Mair Street M&CH centre: completed 0% PODS group: completed 100%Link Up group: completed 0%*.
*It should be noted that many of the young parents in the Link Up group also attend the PODS program. Parents may have completed the survey as part of the PODS group rather than the Link Up group.
The remaining 65 completed surveys (42% of total surveys returned) were received in equal proportions from the other four M&CH centres located in the City of Ballarat. These specific locations were Ballarat North, Mt Clear, Sebastopol and Wendouree/Cooinda centres.
The following is a snapshot of survey outcomes (NB Complete survey results included in Appendix 2)
“Breastfeeding only” was least likely to take place in the 15-19 year age group. •Women with their first baby are less likely to be breastfeeding only compared to women •having their second or subsequent baby. Breastfeeding only is more likely to occur when there are 2 adults in the family•When formula feeding only, the highest percentage of responses as to why they changed •from breastfeeding to other methods indicated that the decision was influenced by “baby issues” and by “other”.When the method of feeding changed, the highest percentage was recorded in babies •less than one month of age followed by 2-3 months. The highest percentage of respondents indicated that a change in the type of feeding •selected was made by difficulties with supply issues. The majority of respondents rated information provided about breastfeeding education •at school as either “poor” or “very poor”.
Other Comments
Other Comments

29.
Respondents were invited to provide additional comments which generally fell into four categories which included:
Lack of support returning to work - ‘regarding returning to work, maybe the facilities 1.could be outlined when maternity leave is processed as this may influence when you return to work’. ‘A lot of my friends had to change to the bottle when returning to work and not having time to feed naturally’.Lack of facilities and poor community attitudes - ‘I think we need more change/2.breastfeeding rooms made available’. ‘We need more clean, safe places to breastfeed when out and about’. ‘The general feeling I get is that breastfeeding is not acceptable in public, even when being discreet’.Lack of support, accurate information and education - ‘I think hospitals should have 3.staff dedicated to breastfeeding assistance. On both occasions I have received very conflicting advice which caused me stress and doubt. If someone was employed to offer consistent advice I think it would help breastfeeding rates a lot’. Information about breastfeeding is not consistent’.And those who spoke about their experiences positively - ‘my experience of breastfeeding 4.at home and in public was positive and I would encourage other mothers to give it a try’. ‘I feed anywhere!’

30.
Develop a set of protocols regarding breastfeeding information that is provided to parents at different stages
Develop strategies to influence “normalising” breastfeeding which is embedded in community attitudes
Review role of the project in schools, which may incorporate different approaches for the Charter as well as with primary and secondary schools
Provide education initiatives that assist in developing a shared understanding of the evidence base regarding artificial infant formula with pharmacists and pharmacy staff
Continue to review and negotiate the potential to establish a breastfeeding “drop in” service which is staffed collaboratively across project partners
All Midwives and MCH Nurses should have International Board Certified (IBC) LC qualifications or a specialist service should be established with Midwives/MCH staff with IBC LC qualifications
Establishment of a data working group to review how data is defined, consistency of data and establishment of effective data systems across services
Review IT and media practices within the CoB to establish guidelines that can support the promotion of breastfeeding in the community.
Promote engagement of the Ballarat ABA in the ongoing project
Extend the Breastfeeding Charter to include more signatories
Develop specific strategies to engage and support CALD groups
Develop specific strategies to engage and support Aboriginal and Torres Strait Islander groups
Develop specific strategies that can support Charter signatories in promoting community awareness
9. Summary of all Recommendations
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.

31.
Develop media promotions that recognise individual businesses that support the Charter
Develop specific materials/practical resources that assist businesses in promoting breastfeeding to their clients/customers
Develop strategies that assist businesses to gain positive and direct benefits from being a Charter signatory
Target breastfeeding promotion programs to parents in the younger age groups
Target breastfeeding promotion programs in the Sebastopol/Delacombe, Wendouree and Buninyong areas
Target breastfeeding promotion programs towards women who have their first baby
Target breastfeeding promotion programs towards single parents
Target breastfeeding promotion programs to parents in the baby’s first 3 months
Promote breastfeeding in education programs within schools
Promote breastfeeding awareness and consider breastfeeding needs in the development of community facilities
Promote breastfeeding awareness in community education programs
Support and recognise workplaces that promote breastfeeding
Support the development of breastfeeding friendly policies within Council, the partnership and community stakeholders
Promote adequate maternity leave and compliance with maternity leave and work place legislation and encourage the provision of appropriate workplace facilities for breastfeeding
Promote positive multicultural perceptions, beliefs and practices
Promote positive perceptions of breastfeeding, consistent information and challenge myths and misconceptions
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.

32.
Develop a publicity campaign to promote positive cultural attitudes to breastfeeding in public and raise awareness of available breastfeeding rooms
Provide a range of opportunities to extended family members to support mothers in learning and maintaining breastfeeding
Promote helpful attitudes and excellent knowledge levels of hospital staff and other health professionals
Ensure that all strategies include are appropriate to all levels of literacy and education
Ensure that all strategies are inclusive of all levels of socio-economic status
Encourage the development of community facilities that encourage breastfeeding
Support services that provide ongoing breastfeeding support, and ensure equitable access to such support
Ensure that breastfeeding becomes a standard part of the health education curriculum in schools, and that it is also an integral component in ante natal classes
Provide appropriate education and consistent advice on techniques for successful breastfeeding establishment in the first six weeks postpartum
Provide adequate and consistent advice on breastfeeding maintenance to 2 years and beyond, and on factors that are likely to limit breastfeeding success
Continue to undertake local research to ensure that local experiences as to the reasons why people do and don’t breastfeed in order to continually modify our Action Plan
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.

33.
BEST START BREASTFEEDING PROJECT - FIVE YEAR ACTION PLAN - EVALUATIONSeptember 2010
APPENDIX 1: Progress against the Ballarat Best Start Promoting Breastfeeding Action Plan
No BARRIER GOALS ACTIONS UPDATES 2004 - 2010
1 Lack of supportive policies and legislation (such as formal adoption of WHO Code on the marketing of breast milk substitutes, or the adoption of any code for retailers or for bottles and teats.)
Develop breastfeeding supportive policies and legislation
Recommendations:
Develop Memorandum of Understanding with MCH & UFS
Develop and implement breastfeeding education and training opportunities for Pharmacists and their staff
Support BHS to maintain their BFHI accreditation
Encourage and support St. John of God to seek BFHI accreditation
Develop promoting breastfeeding policies in partnership with DHS, which can be used in all early childhood centre’s
2005March - Council childcare centres all have Breastfeeding welcome here stickers and happy for someone from this group to present some info at a professional training / staff development session. Don’t have a specific breastfeeding policy, but would be happy for some guidance in writing one.
DHS doesn’t believe that any childcare / kinders have a breastfeeding policy and not a DHS requirement but happy for services to take this on though and happy to help. Will circulate through Snippets ( Newsletter that goes to all kinders /childcare centres)
2007 Council Kinders developed Breastfeeding policies and guidelines.
2008 Feb – “Caregivers Guide to B/Fed baby” and “Suggestions on Using an Electric Breastpump” flyers to Ballarat FDC providers
May - DHS-DEECD supporting policy for childcare centres, kindergartens and education as part of staff development.August – “Handling expressed breastmilk guidelines” provided to child care centres.
2010 April - Maternal & Child Health centres no longer seeing artificial infant formula reps and have adopted the Victorian M&CH Coordinators Group breastfeeding position statement & guidelines policy in line with WHO recommendations.
To challenge both hospitals to maintain / gain baby-friendly hospital initiative (BFHI) accreditation.
2010 June - Ballarat Health Services submitted application for BFHI and will be accredited in August 2010.St John of God does not meet the criteria for BFHI and will not be applying.

34.
No BARRIER GOALS ACTIONS UPDATES 2004 *
2 Inadequate maternity leave, and maternity leave and work place legislation*, and lack of appropriate workplace facilities for breastfeeding
Promote adequate maternity leave, and compliance with maternity leave and work place legislation and encourage the provision of appropriate workplace facilities for breastfeeding
Recommendations:
Ensure all Council Units implement the ongoing requirements of the BFWA (Breastfeeding Friendly Workplace Accreditation)
Publicly promote the Breastfeeding Room
Support other partner and community organisations to adopt breastfeeding friendly workplace policies
Support the public usage of the breastfeeding room at the City of Ballarat.
2006 - Breastfeeding room opened in the Phoenix Building for staff use only (including partners)
2007 - Discussions with HR re Breastfeeding room being open to public. Was not agreed to.
2008 - Discussions with HR re room being accessible for Council customers. Agreed that customers attending Council for meetings etc, would be able to use the room.
2009 - March - Breastfeeding room to move to Town Hall. Further discussions with HR re opening the room to the public who stated that access not possible due to security concerns in Town Hall.
2010 - March – Breastfeeding Welcome Here Stickers put up in council owned buildings (ongoing).April – City of Ballarat Breastfeeding Room ( in the Phoenix Building) open for public use.June – poster promotion of COB Breastfeeding Room through hospitals, pharmacies, M&CH, Division of GP’s, community health, Council childcare centres and COB.
Encourage the inclusion of positive life/work workplace clauses within the COB award negotiations.
2006 - Attended Enterprise Bargaining negotiations to lobby for and support the inclusion of family friendly and breastfeeding policies within the Award.
2007 - March - Workplace Flexible working and family friendly policy, which includes breastfeeding and lactation breaks, and supporting women returning to work and breastfeed implemented across Council
Develop and support employers / workplaces to adopt positive/best practice breastfeeding policies for employees and their families
2008 - April - City of Ballarat obtained Breastfeeding Friendly Workplace Accreditation. (BFWA). Paid for by Best Start.October – Council become “Healthy Facility” member of ABA and the Lactation Resource Centre, which enables staff to monthly breastfeeding magazines for all M & CH centres, as well as access to professional advice and research.
2009 - March – Toolbox (staff information paper) presentation on breastfeeding to Councils leadership team, and then rolled out to all staffMay – Negotiated with HR to take over budget for annual BFWA July - BFWA renewed, with agreement by HR to take on on-going responsibility. 2011 accreditation will involve a site visit by ABA.

35.
No BARRIER GOALS ACTIONS UPDATES 2004 *
3 Negative cultural perceptions, beliefs and practices in some ethnic groups
Promote positive multicultural perceptions, beliefs and practices
Recommendations:Explore the opportunities to provide culturally appropriate information and education regarding breastfeeding
Redevelop the multicultural pregnant and parenting library at BHS. (Ballarat Health Services)
2005 - BRMC, Council and the Central Highlands regional library updated the library at BHS.
2006 - Base Hospital employed a specific midwife to focus on indigenous women / families.
2007 - Maternity Unit purchased a software program that has all relevant information in a range of other languages.
Source appropriate information about BF in languages suitable for Ballarat’s CALD families.
2006 - Council staff trained in using the Interpreter Information service
2007 - M & CH sourced breastfeeding pamphlets in other languages.
2008 - Information made available on line via DEECD
Support women / families from other cultures to maintain their traditional practices
2006 - Participation in Multicultural / Harmony Week to provide breastfeeding information
2007 - Participation in Multicultural / Harmony Week to provide breastfeeding informationFunding request to Multicultural Council of Victoria to fund a mentor program to train women from a range of cultural groups in Ballarat about current breastfeeding (and broader child development and education issues), so they can support women from their communities (submission unsuccessful)
2008 - August – breastfeeding information session for CALD community.November – CALD Women’s Health seminar
2009 - Discussions with Councils Cultural Diversity Program to explore other avenues to develop a mentor program

36.
No BARRIER GOALS ACTIONS UPDATES 2004 *
4 Inaccurate and misleading community information / myths remaining unchallenged.
Promote positive perceptions, beliefs and practices and challenge myths
Recommendations:
Undertake a publicity campaign that relates current information about the positives of breastfeeding while challenging the myths
Develop set protocols across maternity care service providers that outline consistent, current and accurate information to be provided to parents.
Develop a community education pack that can be used across the project
2005 - March – A number of resources were purchased for the group from the Lactation Resource Catalogue. Resources were distributed to local GPs and the rest donated to the local branch of the ABA to update their library for public and training use.May - published the first Early Years Guide which include information about breastfeeding support services
2009 - June - breastfeeding component for BCHC ‘Little Baby Book’ a pregnancy, birth & postnatal resource for parents under 25 years of age.
Undertake a publicity campaign that relates current information about the positives of breastfeeding while challenging the myths
2007 - Worked with Councils Media department to develop a marketing plan. Whilst some articles appeared in Council publications, there was little commitment to launch a broader community campaign
2008 - May – ‘Oh My God’ postcard launched by Catherine King
2009 - November – Display” Blueprint for a Better World Millennium Development Exhibition’ which was held at St Patrick’s Cathedral and sponsored by Caritas Australia and Aus AID. November – information display at Maternity Coalition movie night.
2010 - February – promotional banner ‘breastfeeding facts’ challenging some of the myths around breastfeeding.March – information display at “Women After Dark Business Networking eventMarch – information display at Maternity Coalition movie night.June - information display at Maternity Coalition movie nightApril – May– Cardigan Village Playgroup, Sebastopol kindergarten, Our Lady Help of Christians Primary School and LINK UP & PODS young parents participated in art workshops to promote breastfeeding/nurturing. Exhibition of their works at Library and displayed for one month with Breastfeeding promotional banner.
Maintain a register of articles relating to breastfeeding in the local media outlets, respond to any negative articles and acknowledge positive ones.
2005 - Established a register of articles published in the Media and responded when appropriate.
37.
No BARRIER GOALS ACTIONS UPDATES 2004 *
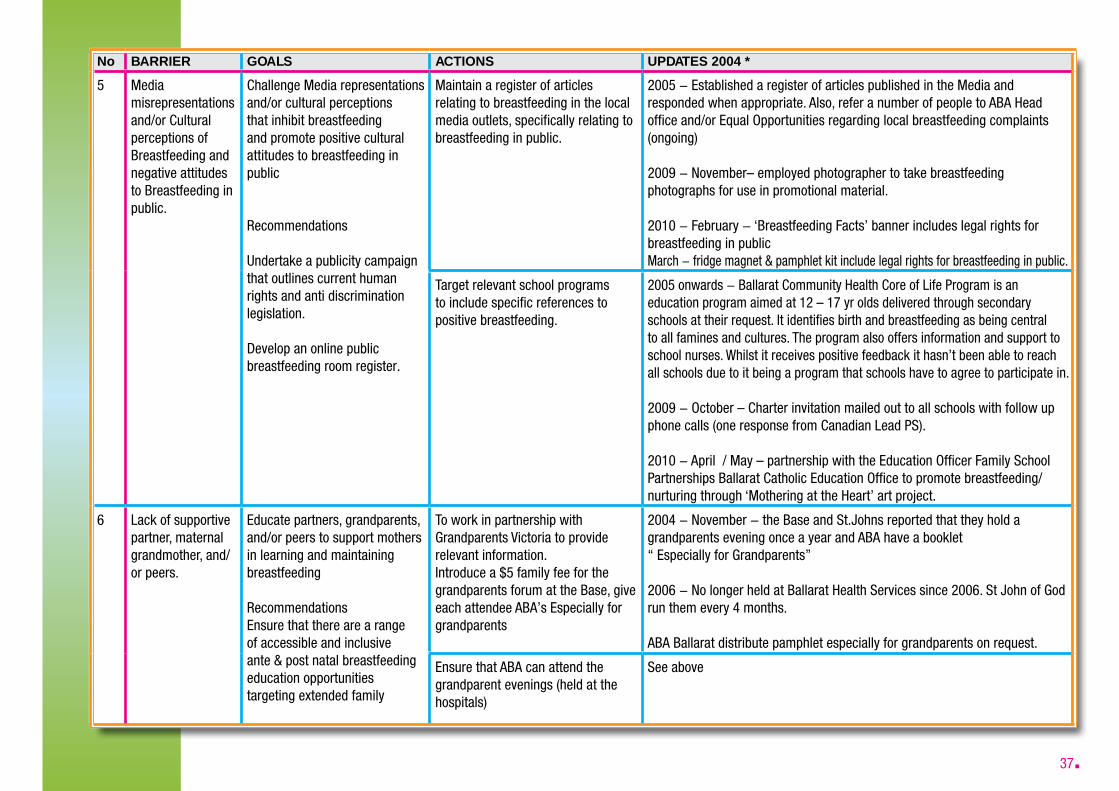
5 Media misrepresentations and/or Cultural perceptions of Breastfeeding and negative attitudes to Breastfeeding in public.
Challenge Media representations and/or cultural perceptions that inhibit breastfeeding and promote positive cultural attitudes to breastfeeding in public
Recommendations
Undertake a publicity campaign that outlines current human rights and anti discrimination legislation.
Develop an online public breastfeeding room register.
Maintain a register of articles relating to breastfeeding in the local media outlets, specifically relating to breastfeeding in public.
2005 - Established a register of articles published in the Media and responded when appropriate. Also, refer a number of people to ABA Head office and/or Equal Opportunities regarding local breastfeeding complaints (ongoing)
2009 - November– employed photographer to take breastfeeding photographs for use in promotional material.
2010 - February - ‘Breastfeeding Facts’ banner includes legal rights for breastfeeding in publicMarch - fridge magnet & pamphlet kit include legal rights for breastfeeding in public.
Target relevant school programs to include specific references to positive breastfeeding.
2005 onwards - Ballarat Community Health Core of Life Program is an education program aimed at 12 – 17 yr olds delivered through secondary schools at their request. It identifies birth and breastfeeding as being central to all famines and cultures. The program also offers information and support to school nurses. Whilst it receives positive feedback it hasn’t been able to reach all schools due to it being a program that schools have to agree to participate in.
2009 - October – Charter invitation mailed out to all schools with follow up phone calls (one response from Canadian Lead PS).
2010 - April / May – partnership with the Education Officer Family School Partnerships Ballarat Catholic Education Office to promote breastfeeding/nurturing through ‘Mothering at the Heart’ art project.
6 Lack of supportive partner, maternal grandmother, and/or peers.
Educate partners, grandparents, and/or peers to support mothers in learning and maintaining breastfeeding
Recommendations Ensure that there are a range of accessible and inclusive ante & post natal breastfeeding education opportunities targeting extended family
To work in partnership with Grandparents Victoria to provide relevant information.Introduce a $5 family fee for the grandparents forum at the Base, give each attendee ABA’s Especially for grandparents
2004 - November - the Base and St.Johns reported that they hold a grandparents evening once a year and ABA have a booklet “ Especially for Grandparents”
2006 - No longer held at Ballarat Health Services since 2006. St John of God run them every 4 months. ABA Ballarat distribute pamphlet especially for grandparents on request.
Ensure that ABA can attend the grandparent evenings (held at the hospitals)
See above

38.
No BARRIER GOALS ACTIONS UPDATES 2004 *
7 Unhelpful attitudes and inadequate knowledge levels of some hospital staff and other healthprofessionals.
Promote helpful attitudes and excellent knowledge levels of hospital staff and other health professionals
Recommendations
Provide a range of ongoing professional development opportunities targeting maternity service providers.
Develop set protocols across maternity care service providers that outline consistent, current and accurate information to be provided to parents.
Develop more collaborative responses between all maternity services in promoting and supporting each other.
Hold a conference aimed at both professionals and community members around “Breastfeeding for a Friendly Community”
2004 - November –Discussion re holding a breastfeeding conference next year to coincide with a breastfeeding week.
2005 - Best Start breastfeeding Conference “ Breastfeeding for a Healthy Community”
2007 - Based on the success of the first conference, worked with ABA to apply for Council Grant funding to run future conferences
2008 - May – ABA breastfeeding conference “Infant feeding – Risky Business”
2009 - May– ABA breastfeeding conference. “Breastfeeding Barriers”
Supporting current evidence based practice and knowledge and challenge practices that interfere with successful breastfeeding
2005 - Feb– Approached the GPs seminar group to ensure that breastfeeding could be included as a standard topic throughout the year of planned professional development.April – Seminar group have invited Rodney White , a Dr from Monash Drug Information, who has expertise in breastfeeding to speak at one of this year’s seminars. March - Breastfeeding welcome here stickers and current info re mastitis delivered to all GPs
2006 - Spoke to the School of Nursing at both Universities to ensure that their class text were current, which they were.
Information Pack bought for ABA to ensure that all counsellors had access to current information.
2010 - Purchase “Breastfeeding Management” latest edition for circulation to M & CH and reference group partners.
Seek baby friendly accreditation for both hospitals (BFHI)
See Question 1

39.
Provide opportunities for M&CH, ABA and the hospitals to work in partnership
2005 - July – discussion process began re: breastfeeding drop in support centre/parenting resource & information.
2007 - All parties agreed in principle to staff a collaborative drop in services. Resources were needed but unavailable at that time
2008 - July – discussion process began with a broader group (Primary Care Partnership – Family and Children’s Platform re: breastfeeding drop in support centre as part of a parenting resource & information hub. (On-going)
2009 - Reference Group members visit the community breastfeeding facility in Dandenong, and plan to visit the drop in service in Carlton.
(See Point 11)
Ensure that breastfeeding remains a current topic for staff/professional development
2005 - March - Breastfeeding welcome here stickers and current info re mastitis delivered to all GPs
2008 - August – “counselling the breastfeeding mother’ training at Ballarat Health services for M&CH, GP’s & Midwives
2009 - June– Lisa Amir seminar at BHS for M&CH, GP’s & Midwives.
( Also see information re conferences)
Provide all GPs and M & CH centres with a copy of the “Best practice guide to breastfeeding problems”
2008 - September – distribution of ‘Lact Facts’ $3 x 100 and ‘Best Practice Guidelines’ to Division of GP’s, Practice Nurses & M&CH.(Ongoing)
Encourage community health, GPs and others to undertake initiatives to create a health care environment where breastfeeding the norm and practices known to promote the health and well-being of babies/mothers (Based on the BFHI initiative)
2007 - Information from the reference group is disseminated through respective organizations for consideration and implementation of ideas.CAFS staff promote and hold a Trivia Night with funds raised donated to the Breast Feeding Project ( Approx $1700 raised)
2008 - Division of GPS undertaking training as part of their annual training of events calendar (ongoing)
2009 - Ballarat Community Health in the process of seeking Breastfeeding Friendly Workplace Accreditation2010 - All reference group partners are now Charter signatories

40.
No BARRIER GOALS ACTIONS UPDATES 2004 *
8 Low levels of education and/or literacy
Ensure that all strategies include all levels of education and/or literacy , or create strategies that target low levels of education or literacy if necessary
Recommendation
Promote the use of standard tools across all maternity services that are appropriate to all levels of education and literacy
Develop a set of cards that use accessible language and symbols to be used as part of the community education pack
2004 - April - Conducted parent surveys to provide feedback on the information packs parents receive prior to and after birth. Parents also asked what additional information they would like to receive. Specifically involved parents with low literacy skills, and delivered the survey differently ( ie/ with staff assistance where appropriate)
2009 - June – Worked with the Department of Health & Ageing, ‘Go for your Life’ focus groups to redevelop their breastfeeding fact sheet, to ensure that information was consistent and easy to understand.
2010April/May - ‘Mothering at the Heart’ art project specifically targeted some groups who may fit this category.
9 Low Socio Economic Status
Ensure that all strategies are inclusive of all levels of socioeconomic status
Recommendation:Ensure access to breastfeeding education, information and support through agencies working with financially vulnerable families.
Include financial benefits of breastfeeding in ante natal information/education.
Develop partnerships with specific agencies who already work with financially vulnerable families to ensure that the community education pack is accessible
2004 - April - Conducted parent surveys to provide feedback on the information packs parents receive prior to and after birth. Parents also asked what additional information they would like to receive. Parents accessing Ballarat Base Hospital, St John of God Hospital, The Little Clinic, Pinarc, Child and Maternal Health Services and The Day Stay Program were invited to participate.
2009 - June – Worked with BCHC in the development of their ‘Little Baby Book’ which is a pregnancy, birth & postnatal resource for parents under 25 years of age. It includes a breastfeeding component.
2010 - April/May - ‘Mothering at the Heart’ art project specifically targeted some groups who may fit this category.May – presentation to parents at Delacombe Community House on ‘Milk, Food & Your Baby’Developed partnership with PODS to ensure young parents participated in the infant feeding survey and art project

41.
No BARRIER GOALS ACTIONS UPDATES 2004 *
10 Lack of community facilities that encourage breastfeeding*
Encourage the development of community facilities that encourage breastfeeding
Recommendation:Publicly promote City of Ballarat Breastfeeding Room.
Extend Breastfeeding Charter and publicly recognise existing charter signatories.
Allow for public use of the City of Ballarat’s Breastfeeding room, and encourage them to act in a leadership role within the community to encourage additional facilities.
2005 - Initial discussion re the possibility of setting up a Breastfeeding room
2006 - Breastfeeding room opened in the Phoenix Building for staff use only (including partners)
2007 - Discussions with HR re Breastfeeding room being open to public. Was not agreed to.
2008 - Discussions with HR re room being accessible for Council customers. Agreed that customers attending Council for meetings etc, would be able to use the room.
2009 - March - Breastfeeding room to move to Town Hall. Further discussions with HR re opening the room to the public who stated that access not possible due to security concerns in Town Hall.
2010 - March – Breastfeeding Welcome Here Stickers put up in council owned buildings (ongoing).April – City of Ballarat Breastfeeding Room open for public use.June – promotional poster advertising City of Ballarat BF room distributed.July – Ballarat Courier ‘Parent 2010’ magazine breastfeeding room and Charter advertisement
Support agencies who meet breastfeeding-friendly criteria by giving them publicity i.e.“Breastfeeding Welcome Here” sticker and registering them on line
2008 - May – ‘Oh My God’ postcard launched by Catherine King.August - Launch of Breastfeeding Charter by Jaala Pulford MP. Charter signatories are listed on COB website as BF friendly.
2009 - September – Charter invitation mail out to businessesSeptember– Charter invitation mail out to corporationsOctober - Charter mail out to all schools
2010 - All Charter signatories mentioned on COB website and in various newspaper articles
Develop strategies that support all services, businesses and facilities to become breastfeeding friendly
2005 - May - The group agreed to develop a Ballarat Charter to assist with the development of Ballarat becoming a city that supports and encourages breastfeeding. The charter will be influenced by the Philippines’ baby friendly cities project.
2008 - May – ‘Oh My God’ postcard launched by Catherine King.August - Launch of BF Charter by Jaala Pulford MP. Charter signatories are listed on COB website as BF friendly.
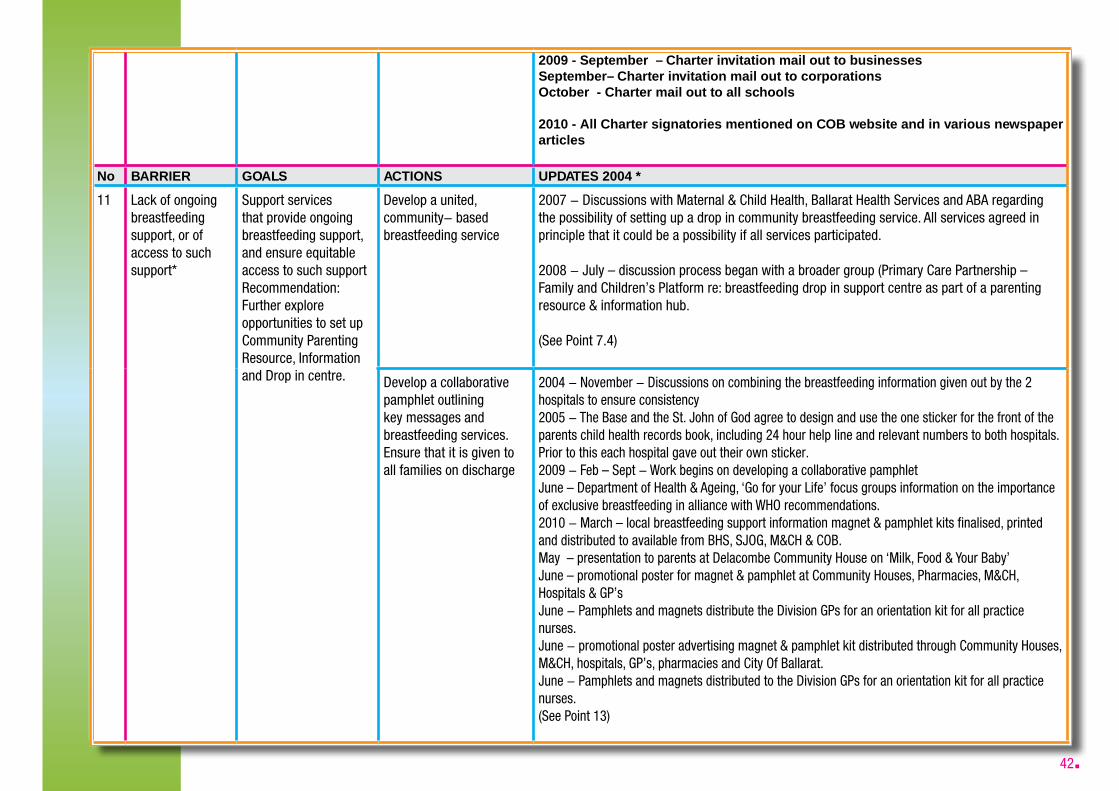
42.
2009 - September – Charter invitation mail out to businessesSeptember– Charter invitation mail out to corporationsOctober - Charter mail out to all schools
2010 - All Charter signatories mentioned on COB website and in various newspaper articles
No BARRIER GOALS ACTIONS UPDATES 2004 *
11 Lack of ongoing breastfeeding support, or of access to such support*
Support services that provide ongoing breastfeeding support, and ensure equitable access to such support Recommendation:Further explore opportunities to set up Community Parenting Resource, Information and Drop in centre.
Develop a united, community- based breastfeeding service
2007 - Discussions with Maternal & Child Health, Ballarat Health Services and ABA regarding the possibility of setting up a drop in community breastfeeding service. All services agreed in principle that it could be a possibility if all services participated.
2008 - July – discussion process began with a broader group (Primary Care Partnership – Family and Children’s Platform re: breastfeeding drop in support centre as part of a parenting resource & information hub.
(See Point 7.4)
Develop a collaborative pamphlet outlining key messages and breastfeeding services. Ensure that it is given to all families on discharge
2004 - November - Discussions on combining the breastfeeding information given out by the 2 hospitals to ensure consistency2005 - The Base and the St. John of God agree to design and use the one sticker for the front of the parents child health records book, including 24 hour help line and relevant numbers to both hospitals.Prior to this each hospital gave out their own sticker. 2009 - Feb – Sept - Work begins on developing a collaborative pamphletJune – Department of Health & Ageing, ‘Go for your Life’ focus groups information on the importance of exclusive breastfeeding in alliance with WHO recommendations.2010 - March – local breastfeeding support information magnet & pamphlet kits finalised, printed and distributed to available from BHS, SJOG, M&CH & COB.May – presentation to parents at Delacombe Community House on ‘Milk, Food & Your Baby’June – promotional poster for magnet & pamphlet at Community Houses, Pharmacies, M&CH, Hospitals & GP’sJune - Pamphlets and magnets distribute the Division GPs for an orientation kit for all practice nurses.June - promotional poster advertising magnet & pamphlet kit distributed through Community Houses, M&CH, hospitals, GP’s, pharmacies and City Of Ballarat.June - Pamphlets and magnets distributed to the Division GPs for an orientation kit for all practice nurses.(See Point 13)

43.
No BARRIER GOALS ACTIONS UPDATES 2004 *
12 Lack of appropriate education and information available prior to pregnancy and/or birth
Ensure that breastfeeding becomes a standard part of the health education curriculum in schools, and that it is also an integral component in ante natal classes.
Recommendations:Develop opportunities for breastfeeding to be integrated into the curriculum as a standard part of the health education in schools, beginning in Primary School.
Develop opportunities to include breastfeeding within existing courses, or services delivered within schools.
2004 - November - Approached childcare course to ensure information about breastfeeding was included in the curriculum. Relevant workers on the reference group offer to be guest speakers. ABA had reported that they had done a mail out to schools in 2003 offering to attend schools, but it didn’t get much response.November - Ballarat library very happy to put in for new updated books re breastfeeding in next financial year
2005 - March - DE&T don’t seem to have an overall health curriculum that would cover breastfeeding. Suggested that we ring individual schools.April - Group agreed that the resource folder should be held by the Breastfeeding Assoc to ensure that it continues to be used and circulated. Would be good if other groups borrowed the book for ante-natal classes, open days, new mums groups etc.April - Library updating books re breastfeeding. Group agreed that 2 x Breastfeeding Naturally and 2 x Breastfeeding with confidence (Sue Cox)Core of Life Program delivered to schools across Ballarat on request.
2006 - March – Discussion re purchasing information regarding breastfeeding to give out to all GPS to ensure that all information was current and consistent. Some felt that this is not a cost we should incur, but it was felt that this was the best strategy to ensure that it was rolled out.
2009 - July – invitation to participate in the development of the Department Health & Ageing National Breastfeeding Strategy which offers guidelines for BF education in schools and the importance of ante natal BF education.August –presentation to midwifery students at University of Ballarat.University, SMB and Aquinas students
13 Lack of appropriate education and ongoing advice on techniques for successful breastfeedingestablishment in the first six weeks postpartum.*
Provide appropriate education and consistent advice on techniques for successful breastfeeding establishment in the first six weeks postpartum
Develop a collaborative pamphlet outlining key messages and breastfeeding services that are available and ensure that it accessible to all families
2004 - November Discussions on combining the breastfeeding information given out by the 2 hospitals to ensure consistency
2005 - The Base and the St. John of God agree to design and use the one sticker for the front of the parents child health records book, including 24 hour help line and relevant numbers to both hospitals.Prior to this each hospital gave out their own sticker.
2009 - Feb – Sept - Work begins on developing a collaborative pamphletJune – Department of Health & Ageing, ‘Go for your Life’ focus groups information on the importance of exclusive breastfeeding in alliance with WHO recommendations.

44.
Recommendations:
Develop set protocols across maternity care service providers, in line with WHO & UNICEF recommendations, that outline consistent, current and accurate information for parents.
2010 - March – local breastfeeding support information magnet & pamphlet kits finalised, printed and distributed to available from BHS, SJOG, M&CH & COB.May – presentation to parents at Delacombe Community House on ‘Milk, Food & Your Baby’June – promotional poster for magnet & pamphlet at Community Houses, Pharmacies, M&CH, Hospitals & GP’sJune - Pamphlets and magnets distribute the Division GPs for an orientation kit for all practice nurses.June - promotional poster advertising magnet & pamphlet kit distributed through Community Houses, M&CH, hospitals, GP’s, pharmacies and City Of Ballarat.June - Pamphlets and magnets distributed to the Division GPs for an orientation kit for all practice nurses.
(See Point 11)
No BARRIER GOALS ACTIONS UPDATES 2004 *
14 Lack of adequate and consistent advice on breastfeeding maintenance, and on factors that arelikely to limit breastfeeding success (ABA five-year plan).*
Provide adequate and consistent advice on breastfeeding maintenance to 2 years and beyond, and on factors that are likely to limit breastfeeding success Recommendations:As in # 13
Develop a Memorandum of Understanding between all relevant services that endorse the key messages.
2009 - July – Department of Health & Ageing, National Breastfeeding Strategy information on the importance of health care providers and support services providing current, consistent advice and information for parents on breastfeeding issues in line with WHO recommendations.
2010 - March – breastfeeding support & information fridge magnet & pamphlet kit outline key messages as endorsed by all relevant services including WHO recommendations.
Incorporate the Memorandum of Understanding into all staff development and orientation.
All reference group services are Charter Signatories
15 Lack of access to local research
Undertake local research to ensure that local experiences as to the reasons why people do and don’t breastfeed in order to continually modify our Action Plan.
Develop a local research project
2004 - April - Conducted parent surveys to provide feedback on the information packs parents receive prior to and after birth. Parents also asked what additional information they would like to receive. Parents accessing Ballarat Base Hospital, St John of God Hospital, The Little Clinic, Pinarc, Child and Maternal Health Services and The Day Stay Program were invited to participate.June – Outcomes from the surveys led to changes being implemented in the 2 hospitals. It also led to the development of the Early Years guide which is now in its second edition and is seen as an on-going responsibility of the City of Ballarat.

45.
Recommendations:Continue to consult with parents about issues that inhibit and/or encourage their choices regarding breastfeeding
Develop an action plan and evaluation framework that assists in capturing local feedback and data
November -public meeting was held with support of the University of Ballarat and ABA Head Office to :
Brainstorm why Breastfeeding rates in Ballarat are decliningBrainstorm what services exist in Ballarat andBrainstorm what strategies we could undertakeOutcomes of the meeting provided the basis for the development of the Breastfeeding Action Plan
2005 - Looked at add on opportunities ie community educator at the Base interested in focusing on Asthma , could link in breastfeeding info or research?
2006 - June - John McDonald , Associate Professor School of Behavioural and Social Sciences and Humanities at the University of Ballarat attended to help the group formulate an Action Plan.
2007 - March – Had further discussions with University of Ballarat who would be happy to undertake some local research for us. We would require a specific funding allocation / budget for this to occur.
2009 - December – City of Ballarat in collaboration with Lynne Gleeson (private consultant) developed an Infant Feeding Survey. Rolled out to parents through M&CH centres by Carly Wemyss (Private consultant). Aim of survey was to gain an understanding of the concerns, issues, influencing factors that affected local women in their infant feeding choices.
2010 - January– Infant Feeding Surveys Collected and data analysis begun.June - Infant Feeding Survey completed with recommendations under review.

46.
Table 1: All respondents and type of feeding
Table 2: Type of Feeding and Mothers Age
Table 3: Mothers Age and Type of Feeding
Table 4: Postcode and Type of Feeding
Table 5: First Baby and Type of Feeding
Table 6: Family Composition and Type of Feeding
Table 7: Cultural Background and Type of Feeding
Table 8: Type of Birth and Type of Feeding
Table 9: Influences on decision and type of feeding selected
Table 10: Comments on influences on the decision to change feeding
47
48
48
49
50
51
53
54
56
58
Figure 1: Mothers Age
Figure 2: Postcode of respondents
Figure 3: Is this your first baby?
Figure 4: Family Composition
Figure 5: Cultural Identification
Figure 6: Type of Birth
Figure 7: Type of feeding (in the first six months)
Figure 8: Influences on type of feeding selected
Figure 9: Additional comments grouped by themes
Figure 10: Changing the method of feeding
Figure 11: Age of baby when method of feeding changed
Figure 12: Influence on decision to change method of feeding baby
Figure 13: Additional comments grouped by themes
Figure 14: Professional Support and Education
Figure 15: Professional Support and Education by Type of Feeding
Figure 16: Breastfeeding Education at School
Figure 17: Breastfeeding Education at School by Type of Feeding
Figure 18: Community Facilities and Attitudes
Figure 19: Community Facilities and Attitudes by Type of Feeding
Figure 20: Family Support
Figure 21: Family Support by Type of Feeding
Figure 22: Support at Work
Figure 23: Support at Work by Type of Feeding
Figure 24: Additional comments grouped by themes
47
49
50
51
52
53
55
56
57
58
59
60
61
63
64
65
65
66
67
68
69
70
70
72
List of Tables and Figures in Appendix
Appendix 2Results from the City of Ballarat Infant Feeding Survey (July 2010)

47.
Section I: Demographic Information
Appendix 2Results from the City of Ballarat Infant Feeding Survey (July 2010)
Table 1 (right) summarises the number of respondents and the type of feeding for the baby. This data indicates that there were 155 respondents in total and 90 (58%) were breastfeeding only (breastfeeding and expressed breastmilk feeding). In addition, a further 51 (33%) had a combination of breastfeeding and formula feeding. Fourteen respondents (9%) were formula feeding only.
Figure 1 above provides a summary of the age breakdown of survey respondents (n=155). Seventy six respondents (49%) were in the 27-35 age group. Fifteen respondents (10%) were in the 15-19 years category, and thirty one respondents (20%) were in the over 35 years category. Thirty three respondents (21%) were in the 20-26 year age group.
Table 1: All respondents and type of feeding
Figure 1: Mothers Age
Breastfed Only
Expressed Breastmilk Fed
Breastfed & Formula Fed
Formula Fed Only
Total
N
87
3
51
14
155
%
56%
2%
33%
9%
100%
TOTAL
10%
21%
49%
20%<15 - 1920 - 2627 - 35Over 35
Mothers Age

48.
Table 2 above summarises the data by type of feeding and mothers age. The results indicate that breastfeeding only was more likely to take place in the older age groups (54% in 27-35 age group and 25% in the 35+ age group). Breastfeeding only was least likely to take place in the 15-19 year age group. In addition, a higher percentage of women in the older age groups had a feeding pattern that included some breastfeeding. In contrast, the percentage of women who were formula feeding occurred consistently across all age groups. Formula feeding only was the most common type of feeding for the 15-19 year age group.
Table 3 above summarises the data broken down for each age group. This indicates that a combination of breastfeeding and formula feeding only was the most common form of feeding for the 15-19 year age group. In contrast, the older age groups (27-35 years and the over 35 years age group) had breastfeeding only as the most common type of feeding.
Table 2: Type of Feeding and Mothers Age
Table 3: Mothers Age and Type of Feeding
Recommendation 1: Target breastfeeding promotion programs to parents in the younger age groups.
Breastfed Only
Expressed Breastmilk Fed
Breastfed & Formula Fed
Formula Fed Only
<15 - 19 yrs 20 - 26 yrs 27 - 35 yrs >35 yrs Total
n
4
0
8
3
%
5%
0%
16%
23%
n
14
1
13
4
%
16%
50%
27%
31%
n
47
1
23
3
%
54%
50%
47%
23%
n
22
0
5
3
%
25%
0%
10%
23%
n
87
2
49
13
%
100%
100%
100%
100%
Breastfed Only
Expressed Breastmilk Fed
Breastfed & Formula Fed
Formula Fed Only
Total
<15 - 19 yrs 20 - 26 yrs 27 - 35 yrs >35 yrs
n
4
0
8
3
15
%
27%
0%
53%
20%
100%
n
14
1
13
4
32
%
44%
3%
41%
12%
100%
n
47
1
23
3
74
%
63%
1%
32%
4%
100%
n
22
0
5
3
30
%
73%
0%
17%
10%
100%

49.
Figure 2 above represents the postcodes of respondents. The majority of respondents were in the Ballarat area (65%). The smallest percentage of respondents was in the 3352 postcode area, which includes townships surrounding and outlying the Ballarat area (6%). Nine percent (9%) of respondents were from the Buninyong area, 12% were from Sebastopol/Delacombe and 8% from Wendouree.
Table 4 above summarises the type of feeding by postcode of respondents. The results indicate that Ballarat has the highest breastfeeding only rate, and the lowest formula feeding only rate.
Figure 2: Postcode of respondents
Table 4: Postcode and Type of Feeding
Recommendation 2: Target breastfeeding promotion programs in the Sebastopol/Delacombe, Wendouree and Buninyong areas.
Postcode
65% 12%
8%
6%
9%
Ballarat area
Sebastopol/ Delacombe
Wendouree
Ballarat surrounds
Buninyong
Breastfed Only
Expressed Breastmilk Fed
Breastfed & Formula Fed
Formula Fed Only
Total
Ballarat Sebas/Delacombe
BallaratSurroundsWendouree Buninyong
61
1
32
6
100
61%
1%
32%
6%
100%
8
1
6
1
16
50%
6%
38%
6%
100%
10
0
9
3
22
46%
0%
40%
14%
100%
0
0
0
3
3
0%
0%
0%
100%
100%
80%
0%
20%
0%
100%
8
0
2
0
10

50.
Figure 3 above summarises the information regarding first baby (n = 154). 53% of all respondents indicated that this was the first baby, and 47% indicated that the respondent had previously had a baby.
Table 5 above indicates the relationship between the first baby and the type of feeding. This indicates that women with their first baby are less likely to be breastfeeding only (49.5% compared to 66.5%). Women with their first baby are more likely to be using a combination of breastfeeding and formula feeding (38.5% compared to 26.5%) and more likely to be formula feeding only (10% compared to 7%).
Figure 3: Is this your first baby?
Table 5: First Baby and Type of Feeding
Recommendation 3: Target breastfeeding promotion programs towards women who have their first baby.
First Baby?
53%47%
YesNo
First Baby - Yes First Baby - No
Breastfed Only
Expressed Breastmilk Fed
Breastfed & Formula Fed
Formula Fed Only
Total
N
40
2
31
8
81
%
49.5%
2%
38.5%
10%
%100
N
46
0
18
5
69
%
66.5%
0%
26.5%
7%
100%

51.
Figure 4 above indicates the family composition of respondents. This indicates that 11% of all respondents were in single parent families, and 89% of respondents were in 2 adult families (n=150). The highest percentage of respondents was in a family that included 2 adults and 1 child (46%). The lowest percentage of respondents were in either the 1 adult and 3 children group (1%) or in the 1 adult and 2 children
group (3%). Seven percent of respondents were in the 1 adult and 1 child group.
Table 6 above summarises the relationship between the family composition and type of feeding. This indicates that breastfeeding only is more likely to occur when there are 2 adults in the family. Breastfeeding only is also more likely to occur in the sub-group which includes 1 adult and 3 children, although the numbers in the sample were small. In addition, a combination of breastfeeding and formula feeding is also more likely to occur when there are 2 adults in the family. In contrast, it appears that single parents are more likely to be formula feeding, although the sample size is small for this group.
Figure 4: Family Composition
Table 6: Family Composition and Type of Feeding
Recommendation 4: Target breastfeeding promotion programs towards single parents.
Family Composition7%
3%
1%
46%24%
19%
1 adult & 1 child
1 adult & 2children1 adult & 3+children2 adults & 1 child
2 adults & 2children2 adults & 3+children
1 adult & 1 child
Breastfed Only
Expressed Breastmilk Fed
Breastfed & Formula Fed
Formula Fed Only
Total
N
2
1
6
1
10
%
20%
10%
60%
10%
100%
1 adult & 2 children
N
2
0
0
2
4
%
50%
0%
0%
50%
100%
1 adult & 3 children
N
2
0
1
0
3
%
67%
0%
33%
0%
100%
2 adults & 1 child
N
37
1
23
7
68
%
54%
4%
34%
10%
100%
2 adults & 2 children
N
24
0
10
0
34
%
71%
0%
29%
0%
100%
2 adults & 3 children
N
18
0
5
3
26
%
69%
0%
19%
12%
100%
Total
N
85
2
45
13
145
%
59%
1%
31%
9%
100%

52.
Figure 5 above indicates the cultural identification of respondents. Six respondents (4%) indicated that they were from a culturally diverse background, with 4 respondents indicating they were from an ATSI background and 2 from a CALD background (3% and 1% of the total responses respectively). 96% (n=149) did not identify as being from a CALD background. The total number of responses was n=155. It should be noted that the survey was distributed only through the mainstream MCH program, and not through the Enhanced MCH program. Anecdotal information indicates that a higher percentage of respondents may identify as CALD or ATSI through the Enhanced MCH service.
Figure 5: Cultural Identification (Aboriginal /Torres Straight Islander / Non English Speaking Background)
Cultural Background
3%
1%
96%
Indigenous/TSICALDNo

53.
Table 7 (left) represents the CALD background and type of feeding. This data should be interpreted with caution due to the very low numbers of participants in the ATSI and CALD categories. It is interesting to note the high percentage (83%) of respondents from ATSI and CALD background who are breastfeeding
only. This is not consistent with other anecdotal evidence and may represent a bias in the sample. Please see note above regarding the Enhanced MCH service.
Figure 6 above indicates the type of birth of respondents. This indicates that the majority of respondents (63%, n=94) indicated that the baby had a normal vaginal birth. The second most common birth type (19%, n=29) was an emergency caesarean birth. The least common birth type was a vacuum birth (4%, n=7).
Table 7: Cultural Background and Type of Feeding
Figure 6: Type of Birth
ATSI
Breastfed Only
Expressed Breastmilk Fed
Breastfed & Formula Fed
Formula Fed Only
Total
N
3
1
4
%
75%
25%
100%
N
2
2
%
100%
100%
N
5
1
6
%
83%
17%
100%
CALD Total
Baby's Birth
010203040506070
%
VaginalBirth
VaccumBirth
ForcepsBirth
PlannedCaesarean
Birth
EmergencyCaesarean
Birth

54.
Table 8 above represents the type of birth and the type of feeding separated by type of birth subgroups. This indicates that breastfeeding only was the most common type of feeding following all types of births. In addition, the combination of breastfeeding and formula feeding was the second most common type of feeding following all births.
Current research has indicated that the use of Epidural Anaesthesia can have a direct impact on the establishment of breastfeeding. This question was not included in the survey, and therefore the results presented above in Table 8 need to be interpreted with some caution.
Table 8: Type of Birth and Type of Feeding
Vaginal
Breastfed Only
Expressed Breastmilk Fed
Breastfed & Formula Fed
Formula Fed Only
Total
N
49
2
32
11
94
%
52%
2%
34%
12%
100%
N
3
1
2
1
7
%
43%
14%
29%
14%
100%
N
8
0
2
1
11
%
73%
0%
18%
9%
100%
N
8
0
5
1
14
%
57%
0%
36%
7%
100%
N
19
0
10
0
29
%
66%
0%
34%
0%
100%
N
87
3
51
14
155
%
56%
2%
33%
9%
100%
Vacuum Forceps Planned Caesarean
EmergencyCaesarean Total

55.
Figure 7 above indicates the type of feeding for the first six months (n=151). This indicates a pattern which is very similar to the overall response presented in Table 1. Fifty eight percent (58%) of respondents indicated that they were breastfeeding only. Thirty two percent (32%) indicated that used a combination of both breastfeeding and formula feeding, and 1% indicated formula feeding only.
Figure 7: Type of feeding (in the first six months)
Feeding
58%
9%
1%
32%
Only breastfed
Only bottle fedwith breastmilk
Only bottle fedwith Formula
Fed bothbreastmilk andformula

56.
Figure 8 above represents the influences on the decision about the type of feeding that was selected. The respondents (n=145) could select more than one response in this question. The data indicates that the majority (21%) of women were influenced by other, closely followed by their partner (20%). Fifteen percent were influenced by the midwife/nurse and 14% by the mother. The father and the partner parents were identified the least number of times as having an influence on the decision about the type of feeding selected.
Figure 8: Influences on type of feeding selected
Table 9: Influences on decision and type of feeding selected
Breastfed Only
Partner
Mother
Father
Partner’s Parents
Midwife/Nurse
Doctor
Maternal & Child Health Nurse
Antenanatal/Breastfeeding Classes
Friend
Community Attitude
Other
Total
Expressed Breastmilk Fed
Breastfed &Formula Fed
Formula FedOnly
%
20%
17%
2%
2%
14%
3%
7%
9%
2%
4%
19%
100%
N
37
32
4
4
25
6
13
17
4
7
34
183
%
0%
25%
0%
0%
50%
0%
0%
0%
25%
0%
0%
100%
N
1
2
1
4
%
20%
8%
1%
2%
17%
3%
9%
9%
7%
7%
18%
100%
N
20
8
1
2
17
3
9
9
7
7
18
101
%
13%
0%
0%
0%
13%
13%
0%
0%
0%
7%
53%
100%
N
2
2
2
1
8
15

57.
Table 9 presents the data when separated by the type of feeding selected. For the decision to breastfeed only and selecting a combination of breastfeeding and formula feeding, the most common influence was the partner (20% in both groups). In addition, for the group of women who selected breastfeeding, 19% indicated that other influences were important in the decision, followed by the mother and the midwife/nurse. For women who selected a combination of breastfeeding and formula feeding, 18% indicated they were influenced by other factors, followed by 17% who reported the midwife/nurse was influential. For women who selected formula feeding, 53% indicated “other” as the most common influence on this decision.
Figure 9 above indicates that 82% of respondents indicated that the decision about the type of feeding selected was made by the woman herself, 6% indicated that there were difficulties with supply issues, 6% indicated baby issues and 6% indicated other influencing factors.
Self – decision made by woman herself, i.e. ‘past history of great difficulty breastfeeding. 1. I have attempted to breastfeed each of my six HEALTHY children’. ‘I just wanted to breastfeed’.Supply issues – low breastmilk volume, i.e. ‘I breastfed for 2 weeks, but never got my 2. milk supply’. Baby Issues – baby influenced decision, i.e. ‘very prem baby who was too sick to 3. breastfeed’. ‘ better for baby’.Work - mother returned to work. (no responses in this category)4. Other – any other influencing factors. i.e. ‘my mother in law fed two children until 2 5. years’. ‘they told me to give it a try and if it didn’t work to give formula’.
Figure 9: Additional comments grouped by themes

58.
Figure 10 above indicates the percentage of respondents who changed the method of feeding. Sixty two percent (n=91) indicated that they did not change the method of feeding, and 32% (n=57) indicated they did change the method of feeding. The total number of respondents was n=148.
Table 10 above provides additional information regarding the influences on the decision to change feeding types. For women who were breastfeeding only, 95% indicated that the decision was made by the woman herself. The decision being made by self was also reflected with other combinations of breastfeeding as well. In contrast, when formula feeding only, the highest percentage of responses indicated that the decision was influenced by “baby issues” and by “other”.
Figure 10: Changing the method of feeding
Table 10: Comments on influences on the decision to change feeding
Feeding Changes
38%
62%
YesNo
Breastfed Only
Self
Supply
Baby Issues
Work
Other
Total
Expressed Breastmilk Fed
Breastfed &Formula Fed
Formula FedOnly
%
95%
0%
0%
0%
5%
100%
N
40
0
0
0
2
42
%
50%
50%
0%
0%
0%
100%
N
1
1
0
0
0
2
%
72%
16%
8%
0%
4%
100%
N
18
4
2
0
1
25
%
55%
0%
27%
0%
18%
100%
N
6
0
3
0
2
11

59.
Figure 11 above indicates the age of the baby when the method of feeding changed. This question was answered only if the method of feeding changed, and was completed by 56 respondents. The highest percentage was at less than one month (32%), followed by 2-3 months (31%). After the baby reached 18 months, there were no respondents who changed the type of feeding.
Recommendation 5: Target breastfeeding promotion programs to parents in the baby’s first 3 months.
Figure 11: Age of baby when method of feeding changed

60.
Figure 12 above represents the influences on the decision to change the type of feeding that was selected. As above, respondents had to indicate that they had made a change in feeding method to be included in this question. As with the response represented in Figure 8 above, the respondents (N = 52) could select more than one response in this question. The data indicates that the majority (49%) were influenced by other factors. Ten percent of respondents were influenced by either their partner or their Doctor, 9% were influenced by the Midwife/Nurse and 7% were influenced by the Maternal and Child Health Nurse.
As above, respondents were invited to write additional qualitative comments following this question. Responses generally fell into 5 main categories, which have been grouped as follows:
Supply issues - ‘no one, I ran out of milk, ‘couldn’t keep up supply – single mother’.1. Self - ‘again, no one I decided myself, ‘self’.2. Baby Issues - ‘baby rejected breast so had to bottle feed’. ‘baby wasn’t gaining a lot 3. of weight’.Work - ‘returned to work’, ‘doing work placement so couldn’t continue’.4. Other - ‘went straight to formula as soon as expressing and blood started to come out. 5. Baby was much happier and so was I. My son had swollen breasts the whole time I breastfed him (a reaction). Was much happier on formula’.
Figure 12: Influence on decision to change method of feeding baby

61.
Figure 13 above summarises the comments for why women had made a change in the method of feeding. Forty seven comments were included. Forty percent of respondents indicated that a change in the type of feeding selected was made by difficulties with supply issues and 21% of comments related to decisions made by the woman herself. In addition, 18% indicated baby issues, and 7% indicated work issues. An additional 14% indicated other factors influenced the decision.
Figure 13: Additional comments grouped by themes

62.
Nine statements were included in the survey to gain information about how women perceived influences and attitudes regarding breastfeeding in Ballarat. Respondents were asked to rate each statement on a scale of “Very Good” to “Very Poor”. A “Not Applicable” response was also available. For this report, these statements were grouped into five key areas. The statements are summarised below:
Key Area: Professional Support and Education1. Quality of information provided prior to pregnancy and/or birth 2. Access to breastfeeding support services3. Access to good quality and consistent information about breastfeeding
Key Area: Breastfeeding Education at School4. Exposure to breastfeeding education during school years
Key Area: Community Facilities and Attitudes5. Ease and comfort of breastfeeding in public places6. Your experience of community attitudes to breastfeeding7. Availability of community facilities that support breastfeeding
Key Area: Family Support8. Support from family about breastfeeding practices
Key Area: Workplace Support9. Support for breastfeeding when returning to the workplace.
The summaries for each key area are presented below.
Section III: Experiences about breastfeeding in Ballarat

63.
Figure 14 above provides aggregate data and indicates that the majority of respondents (67%) rated professional support and education as either “very good” or good” (35% and 32% respectively). In contrast, 10% of respondents rated this area as “poor” or “very poor” (5% and 5% respectively).
As noted above, the following statements were included in this key area:1. Quality of information provided prior to pregnancy and/or birth 2. Access to breastfeeding support services3. Access to good quality and consistent information about breastfeeding
Key Area: Professional Support and Education
Figure 14: Professional Support and Education

64.
Figure 15 above provides data regarding perceptions of professional support and education, represented by the type of feeding method. The responses to each of the 3 statements have been added together, and are represented by numbers rather than percentages. The results indicate that the majority of women who are breastfeeding rated professional support and education as either “very good” or “good”. In contrast, very few respondents rated this area as “poor” or “very poor”.
As noted above, this key area is represented by a single statement only. The following statement is included in this key area:1. Exposure to breastfeeding education during school years
Key Area: Breastfeeding Education at School
Figure 15: Professional Support and Education by Type of Feeding

65.
Figure 16 above provides aggregate data and indicates that the majority of respondents (62%) rated information provided about breastfeeding education at school as either “poor” or “very poor” (30% and 32% respectively). In contrast, 13% of respondents rated this area as “very good” or “good” (2% and 11% respectively).
Figure 16: Breastfeeding Education at School
Figure 17: Breastfeeding Education at School by Type of Feeding
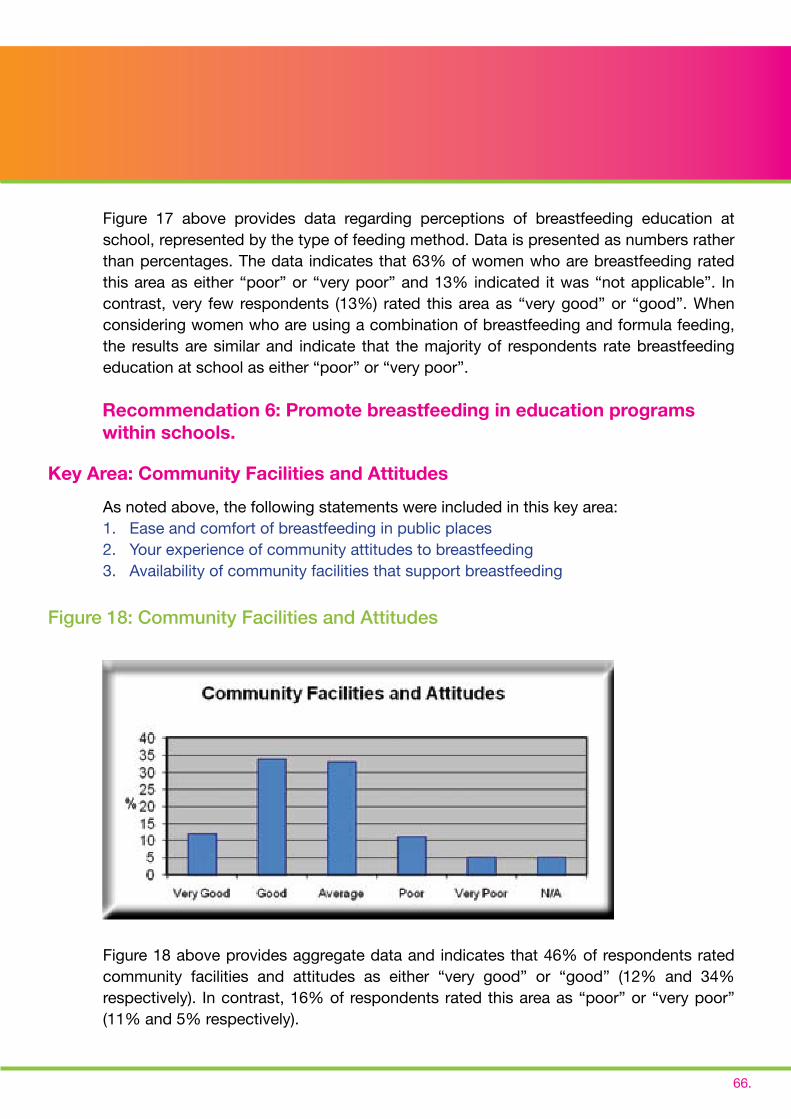
66.
Figure 17 above provides data regarding perceptions of breastfeeding education at school, represented by the type of feeding method. Data is presented as numbers rather than percentages. The data indicates that 63% of women who are breastfeeding rated this area as either “poor” or “very poor” and 13% indicated it was “not applicable”. In contrast, very few respondents (13%) rated this area as “very good” or “good”. When considering women who are using a combination of breastfeeding and formula feeding, the results are similar and indicate that the majority of respondents rate breastfeeding education at school as either “poor” or “very poor”.
As noted above, the following statements were included in this key area:1. Ease and comfort of breastfeeding in public places2. Your experience of community attitudes to breastfeeding3. Availability of community facilities that support breastfeeding
Figure 18 above provides aggregate data and indicates that 46% of respondents rated community facilities and attitudes as either “very good” or “good” (12% and 34% respectively). In contrast, 16% of respondents rated this area as “poor” or “very poor” (11% and 5% respectively).
Recommendation 6: Promote breastfeeding in education programs within schools.
Figure 18: Community Facilities and Attitudes
Key Area: Community Facilities and Attitudes

67.
Figure 19: Community Facilities and Attitudes by Type of Feeding
Figure 19 provides data regarding perceptions of community facilities and attitudes, represented by the type of feeding method. The responses to each of the 3 statements have been added together, and are represented by numbers rather than percentages. This indicates that the majority of women who are breastfeeding rated this area as either “good” or “average”. When considering women who are using a combination of breastfeeding and formula feeding, the perceptions are similar. Very few respondents rated the area as “poor” or “very poor”. For women who are formula feeding only, the highest number of responses rated the area as “average”.
Recommendation 7: Promote breastfeeding awareness and consider breastfeeding needs in the development of community facilities.
Recommendation 8: Promote breastfeeding awareness in community education programs.

68.
Key Area: Breastfeeding Education at School
Figure 20: Family Support
As noted above, this key area is represented by a single statement only. The following statement is included in this key area:1. Support from family about breastfeeding practices
Figure 20 above provides aggregate data and indicates that 82% of respondents rated family support as either “very good” or “good” (67% and 15% respectively). In contrast, 2% of respondents rated this area as “poor” or “very poor” (1% and 1% respectively).

69.
Figure 21: Family Support by Type of Feeding
Figure 21 above provides data regarding perceptions of family support represented by the type of feeding method. This key area is represented by a single question only, and data is included as numbers rather than percentages. The data indicates that the majority of women who are breastfeeding rated this area as either “very good” or “good”. In contrast, very few respondents rated this area as “poor” or “very poor”. For women who are using a combination of breastfeeding and formula feeding, the results are similar and indicate that the majority of respondents rate this area as either “very good” or “good”.
As noted above, this key area is represented by a single statement only. The following statement is included in this key area:1. Support for breastfeeding when returning to the workplace.
Key Area: Breastfeeding Education at School

70.
Figure 22: Support at Work
Figure 23: Support at Work by Type of Feeding
Figure 22 above provides aggregate data and indicates that the majority of respondents (52%) indicated that this question was “Not Applicable”. However, 29% of respondents rated support at work as either “very good” or “good” (16% and 13% respectively). In contrast, 11% of respondents rated support at work as “poor” or “very poor” (6% and 5% respectively).
Figure 23 above provides data regarding perceptions of support at work represented by the type of feeding method. Data is included as numbers rather than percentages, and the data indicates that the majority of women who are breastfeeding rate this area as either “Not Applicable”, or “very good” or “good”. When considering women who are using a combination of breastfeeding and formula feeding, the results are similar.
71.
Additional Comments
As above, respondents were again invited to write additional comments for this question. Responses generally fell into 4 main categories, which have been grouped as follows:
Lack of support returning to work - ‘regarding returning to work, maybe the facilities could 1. be outlined when maternity leave is processed as this may influence when you return to work’. ‘A lot of my friends had to change to the bottle when returning to work and not having time to feed naturally’. Lack of facilities and poor community attitudes - ‘I think we need more change/breastfeeding 2. rooms made available’. ‘We need more clean, safe places to breastfeed when out and about’. ‘The general feeling I get is that breastfeeding is not acceptable in public, even when being discreet’.Lack of support, accurate information and education - ‘I think hospitals should have staff 3. dedicated to breastfeeding assistance. On both occasions I have received very conflicting advice which caused me stress and doubt. If someone was employed to offer consistent advice I think it would help breastfeeding rates a lot’. Information about breastfeeding is not consistent’.And those who spoke about their experiences positively - ‘my experience of breastfeeding 4. at home and in public was positive and I would encourage other mothers to give it a try’. ‘I feed anywhere!’
Recommendation 9: Support and recognise workplaces that promote breastfeeding.

72.
Figure 24: Additional comments grouped by themes
Figure 24 above summarises the additional data provided in themes. Thirty two respondents included additional comments, with the majority of comments being in the area of lack of support, including accurate information and education (41%). The area with the least comments was regarding the lack of support in returning to work (7%). Thirty seven percent of respondents to this question included comments about the lack of facilities and community attitudes.