Project Report: Achieving Value for Money Abbotsford ... · Project Report: Achieving Value for...
42
Project Report: Achieving Value for Money Abbotsford Regional Hospital and Cancer Centre Project February 2005
Transcript of Project Report: Achieving Value for Money Abbotsford ... · Project Report: Achieving Value for...
Project Report:Achieving Value for Money
Abbotsford Regional Hospitaland Cancer Centre Project
February 2005

i
Purpose of this Document
Before entering into a public private partnership,Partnerships BC undertakes an analysis of the valuefor money achieved or expected over the life of thepartnership. Value for money is a broad term thatcaptures both quantitative factors, such as costs,and qualitative factors, such as service quality andprotection of public interests.
Value for money is one of six key principles guidingpublic sector capital asset management in BritishColumbia. The others are:
◗ sound fiscal and risk management;◗ strong accountability in a flexible and
streamlined process;◗ emphasis on service delivery;◗ serving the public interest; and◗ competition and transparency.
Since 2002, these principles have guided the B.C.public sector’s approach to acquiring and managingassets such as bridges, roads and health carefacilities. Ministries and other public bodies such ashealth authorities are encouraged to consider allavailable options for meeting their serviceobjectives. Under the Capital Asset ManagementFramework, options are analyzed and, afterconsidering the qualitative and quantitativeadvantages and disadvantages of each, the onethat overall best meets service delivery needs andmakes the best use of taxpayers’ dollars is chosen.
In some cases, the best option may be traditionalprocurement – where assets are purchased entirelywith taxpayer supported finance and operatedexclusively by the public sector. In other cases,agencies may find innovative ways to meet theirservice needs without acquiring capital assets. In all cases, agencies are publicly accountablethrough regular budgeting, auditing and reporting processes.
In all of its procurement processes, including publicprivate partnership agreements, the Province iscommitted to a high standard of public disclosure toensure accountability. This report describes therationale, objectives and processes that led to theuse of a public private partnership for theAbbotsford Regional Hospital and Cancer Centreproject, giving the public a clear sense of how andwhy the decision was reached to proceed with thatoption. It explains how value for money wasmeasured and how it was achieved in the context ofcurrent market conditions. Where applicable, it alsocompares key aspects of the final agreement toother options considered for the project.
For more on the Province’s Capital AssetManagement Framework, go tohttp://www.fin.gov.bc.ca/tbs/camf.htm
For more on public private partnerships in B.C., go to www.partnershipsbc.ca
Partnerships BC management is accountable for thecontents of this report, including the reasonablenessof the facts, assumptions, and professional opinionsthat have been presented.
Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Table of Contents
1. Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
2. Project Background, Rationale and Objectives . . . . . . . . . . . . . . . . . . . . . . .4
3. Competitive Selection Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
4. Changes in the Project . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
5. The Final Agreement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
6. Comparisons . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22
7. Ongoing Contract Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24
8. Best Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26
Appendix A: Developing and structuring the partnership approach . . . . . . . . . . . . . . . . . . .29
Appendix B: Comparison of the Net Present Value (NPV) of the public sector comparator with the final agreement . . . . . . . . . . . . . . . . .33
1
1. Executive Summary
Achieving Value for Money
The Abbotsford Regional Hospital and CancerCentre (AHCC) project is a long term agreementbetween the public sector and a private partner,wherein the public sector - the Fraser Health Authority(FHA) and the Provincial Health Services Authority(PHSA) - will provide clinical services to meet thecurrent and future health care needs of Fraser Valleyresidents. The private partner, Access HealthAbbotsford (AHA), has agreed to provide a highquality, well maintained hospital and cancer centreand facility management services includinghousekeeping, food, laundry and linen services tosupport effective health care delivery – in keeping withperformance standards set out in the agreement.
Partnerships BC is managing project procurementthrough to the commissioning of the completedhospital and cancer centre, with the objective ofdelivering value for money.
This report addresses project planning and deliveryup to finalization of the project agreement, whichoccurred on December 7, 2004. Value for moneydeterminations at this stage are based on a range ofanalyses, projections and comparisons to otherproject delivery options.
The ultimate success of the project will becontingent on the successful implementation of thenext stages of the project, which involve the detaileddesign, construction and commissioning of thehospital and cancer centre and, following that,provision of facility management services.
Partnerships BC’s assessment of the key attributesof the project is described below.
Health Service Delivery
The AHCC is designed to meet established and futurehealth service delivery needs in the Fraser Valley by:
◗ increasing capacity to meet the health serviceneeds of a growing population;
◗ providing health care services not currentlyavailable in the region;
◗ incorporating the flexibility needed toaccommodate future change; and
◗ responding to the project’s vision statement (seebox below)
Project Vision
Together we will create an innovativeenvironment that inspires caring and the pursuitof knowledge and excellence.
Guiding Principles
◗ Design care processes that optimize patient,client and family satisfaction
◗ Develop and apply integrated resources to enable: – seamless and sustainable care and
support for patients and families – effective exchange of information – sharing of technology and services – ongoing learning and the development of
new knowledge ◗ Develop and maintain a healing and
aesthetically pleasing environment that issensitive to diversity
◗ Foster a safe, comfortable and productivework environment that promotes providerrecruitment, retention and satisfaction
◗ Create a flexible and adaptable design toaccommodate future structures, processes,care delivery systems and technological needs
◗ Build and promote partnerships that improveeffectiveness and efficiency
◗ Maximize cost effectiveness and the use ofavailable resources
◗ Use technologies as a tool to improve costeffectiveness, integration of services and health outcomes
◗ Maintain the individual identities of the FHAand PHSA/BCCA while sharing resourcesand providing seamless services
◗ Minimize impact on the natural and physicalenvironment
2 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Cost
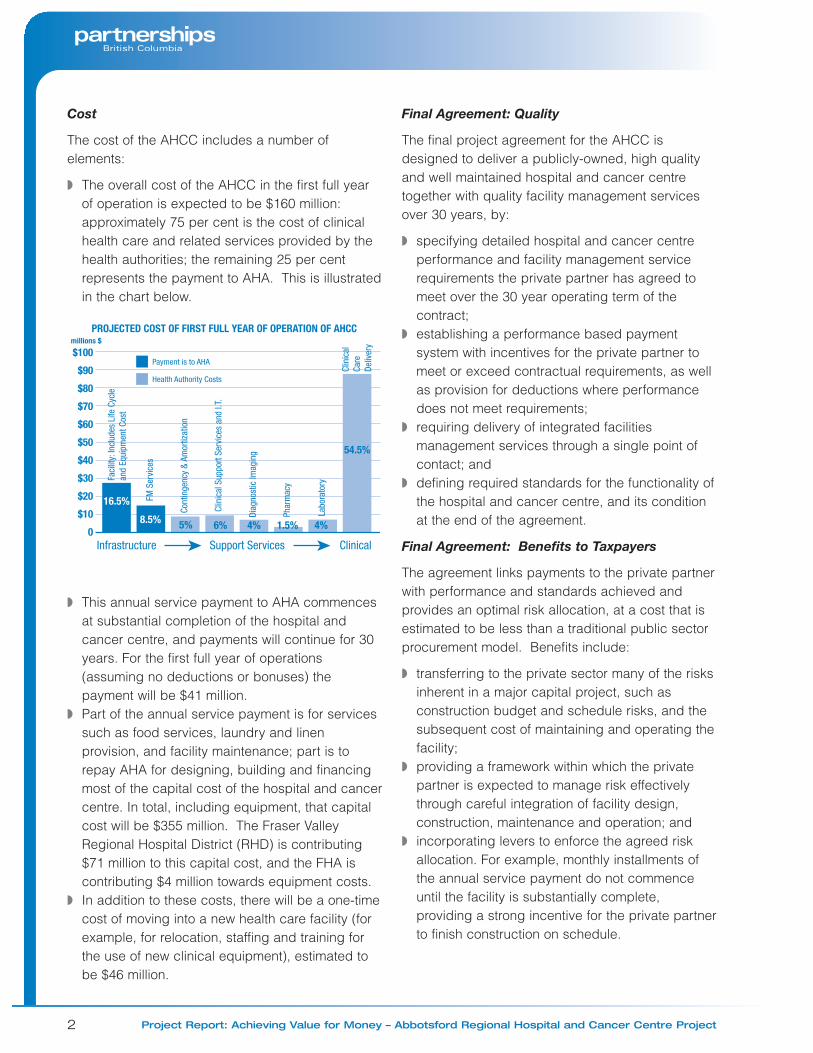
The cost of the AHCC includes a number ofelements:
◗ The overall cost of the AHCC in the first full yearof operation is expected to be $160 million:approximately 75 per cent is the cost of clinicalhealth care and related services provided by thehealth authorities; the remaining 25 per centrepresents the payment to AHA. This is illustratedin the chart below.
◗ This annual service payment to AHA commencesat substantial completion of the hospital andcancer centre, and payments will continue for 30years. For the first full year of operations(assuming no deductions or bonuses) thepayment will be $41 million.
◗ Part of the annual service payment is for servicessuch as food services, laundry and linenprovision, and facility maintenance; part is torepay AHA for designing, building and financingmost of the capital cost of the hospital and cancercentre. In total, including equipment, that capitalcost will be $355 million. The Fraser ValleyRegional Hospital District (RHD) is contributing$71 million to this capital cost, and the FHA iscontributing $4 million towards equipment costs.
◗ In addition to these costs, there will be a one-timecost of moving into a new health care facility (forexample, for relocation, staffing and training forthe use of new clinical equipment), estimated tobe $46 million.
Final Agreement: Quality
The final project agreement for the AHCC isdesigned to deliver a publicly-owned, high qualityand well maintained hospital and cancer centretogether with quality facility management servicesover 30 years, by:
◗ specifying detailed hospital and cancer centreperformance and facility management servicerequirements the private partner has agreed tomeet over the 30 year operating term of thecontract;
◗ establishing a performance based paymentsystem with incentives for the private partner tomeet or exceed contractual requirements, as wellas provision for deductions where performancedoes not meet requirements;
◗ requiring delivery of integrated facilitiesmanagement services through a single point ofcontact; and
◗ defining required standards for the functionality ofthe hospital and cancer centre, and its conditionat the end of the agreement.
Final Agreement: Benefits to Taxpayers
The agreement links payments to the private partnerwith performance and standards achieved andprovides an optimal risk allocation, at a cost that isestimated to be less than a traditional public sectorprocurement model. Benefits include:
◗ transferring to the private sector many of the risksinherent in a major capital project, such asconstruction budget and schedule risks, and thesubsequent cost of maintaining and operating thefacility;
◗ providing a framework within which the privatepartner is expected to manage risk effectivelythrough careful integration of facility design,construction, maintenance and operation; and
◗ incorporating levers to enforce the agreed riskallocation. For example, monthly installments ofthe annual service payment do not commenceuntil the facility is substantially complete,providing a strong incentive for the private partnerto finish construction on schedule.

3
Partnerships BC has analyzed the net present valueof the final agreement compared to a conventionalpublic sector project, including the estimated valueof risk transfer. According to this analysis, aneconomic benefit is expected in the order of $39million over the term of the agreement. That is, thenet present value of the payments to AHA over thelife of the contract (assuming no bonuses ordeductions) is estimated to be $424 million, whilethe net present value of the cost of, hypothetically,building and operating a similar hospital fully withinthe public sector, over the same period, (the publicsector comparator) is projected to be $463 million.This analysis is sensitive to a number of variables,including assumptions around the cost of capitalover time and adjustments for risk (amounts areexpressed in 2004 dollars).
Fair and Open Competitive Selection
A fair and open selection process has resulted in acontract with a partner that combines the expertiseof a number of well qualified, experiencedorganizations. The process included:
◗ incorporating extensive due diligence in thedevelopment and implementation of a relativelynew procurement process for B.C.;
◗ directly engaging the Ministry of Health Services(MHS), the health authorities and the RHD instructuring the project and defining procurementobjectives; and
◗ maintaining competitive pressure while assessinga single proposal, through the use of aconfidential cost benchmark (the public sectorcomparator or PSC), and by only committing to acontract when the full evaluation and negotiationprocesses were complete.
Ongoing Contract Monitoring
The project agreement includes arrangementsdesigned to ensure that each phase of theagreement is implemented as intended, and thepublic sector is implementing arrangements toeffectively monitor this:
◗ a collaborative detailed design developmentprocess between the private partner’s architects, constructors and facilitiesmanagement service providers and project teamand health authority user groups is designed toensure the hospital and cancer centre meetsclinical functionality needs;
◗ during construction, the public sector projectteam will monitor AHA’s progress closely, and an independent certifier will confirm milestones are met;
◗ during the operations phase of the project, theadministration of the agreement will focus onconfirming that performance standards are beingmet by AHA; as part of this, quality satisfactionsurveys will be used to solicit feedback frompatients, visitors, medical staff and healthauthority staff; and
◗ Partnerships BC will work with the MHS and thehealth authorities to undertake higher level, overallreviews of the project at intervals such as five and10 years to establish whether the agreement isfunctioning as intended and the expectedbenefits have been realized.
Best Practices
The Abbotsford Regional Hospital and CancerCentre is the first B.C. hospital to be procured as apublic private partnership. This offers an opportunityto build on experience and develop best practicesfor B.C. Partnerships BC has identified bestpractices at each stage of project development, andis already drawing upon these for future projects.

4 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Public Private Partnerships inHealth Care
Public private partnerships have been used formany years to build health facilities around theworld. In B.C., they are consistent with thegovernment’s vision for modernizing health care, asset out in the December 2002 “Picture of Health”document. The document encouraged healthauthorities to explore public private partnershipswhere they can enhance patient care, deliver valuefor money and serve the public interest, consistentwith the Canada Health Act.
In such partnerships, the private sector typicallyfinances, designs, builds, maintains and operates abuilding to meet detailed performance standards.The Province and/or health authorities provide theclinical (patient health care) services and pay for thefacility and facility services over time. Payments aretied to the agreed-upon performance standards.These include the standard of the building andservices to be provided, and specified time periodsto rectify performance that does not meet theagreed standards.
The partnership model is designed to capture thestrengths of both the public and private sectors,recognizing that private companies have alwaysplayed a part in delivering public infrastructure suchas bridges, highways and hospitals. Partnershipagreements build on that history and clearlydelineate areas of responsibility for both sectorsover the life of a long-term agreement. Keydifferences between the public private partnershipapproach and traditional project procurement arethe inclusion of performance based payment, andthe transfer of many of the risks inherent in capitalprojects to the private sector.
Public private partnerships are part of the Province’splan to provide affordable infrastructure that meetspublic needs. As health care demands continue tomount, this procurement model has the potential tomaximize the value of taxpayers’ investments in newhealth facilities.
Project Background & Rationale
The need for a new health care facility has beenrecognized for more than 15 years
The existing 202-bed Matsqui-Abbotsford-Sumas(MSA) Hospital was built in 1953 and last renovatedin 1980. The decision to replace the hospitalreflects a combination of various factors.
◗ The relative age and condition of the hospitalwould prevent it from being cost-effectivelyupgraded or expanded. This has been borne outby studies conducted in the late 1980s.
◗ The existing hospital lacks the capacity needed toprovide health care to the regional population. Itsnumber of beds has remained constant since1980 while the population of Abbotsford has morethan doubled. The region’s population isexpected to continue growing by between 1.5and two per cent per year, which is greater thanthe general B.C. population growth rate, until atleast 2015, driving increased demand for allhealth care specialties, especially obstetrics,pediatrics, psychiatry and surgery.
◗ The existing hospital is unable to support theoutpatient and ambulatory programs, or providethe advanced medical technology, that areincreasingly important in the delivery of effectivehealth care.
◗ The FHA is committed to increasing theproportion of care provided to the region’sresidents by the region’s hospitals. In recentyears as many as 20 per cent of Fraser Valleyresidents have been treated in Vancouver.
◗ There is an established need to provide a cancercentre in the Fraser Valley. The design andconstruction of a new hospital offered theopportunity to incorporate a cancer centre.
2. Project Background, Rationale and Objectives
5
The AHCC is designed to meet the growingneeds of the region’s population
The FHA’s Strategic Plan confirms the future role ofthe hospital as a regional referral centre. It willserve the core community care needs of Abbotsfordresidents, as well as the secondary acute careneeds of residents of Fraser East (Hope, Chilliwack,Abbotsford, Mission and Agassiz/Harrison).
Specifically, the AHCC will provide the followingprograms and services:
◗ referral centre services for pediatrics (medicaland surgical cases requiring hospital stays oflonger than 48 hours), obstetrics, special carenursery, vascular, nephrology and oncologyservices;
◗ new outpatient programs such as renal dialysis,MRI (Magnetic Resonance Imaging) and nuclearmedicine;
◗ enhanced services related to trauma and morecomplex critical care cases requiring surgical andmedical resources;
◗ a regional role in inpatient acute medical andsurgical oncology for Fraser East residents, inconcert with the cancer centre;
◗ regional services in psychiatry, including six childand adolescent psychiatry beds and a four-bedintensive observation and treatment unit;
◗ acute patient palliative care and symptommanagement services; and
◗ a variety of ambulatory (outpatient) care programs.
The cancer centre will form part of the BC CancerAgency’s Lower Mainland network of services.Patients from the Fraser Valley will no longer need totravel to cancer centres in Vancouver or Surrey fortreatment. This will be an important improvement,given the expected growth in cancer cases in theFraser region. Over the next 10 years, the numberof new cases is expected to grow by about 3.5 percent per year, compared to growth of about threeper cent in the Lower Mainland.
The cancer centre will support the followingprograms and services:
◗ multi-disciplinary consultation and care planningfor new patients;
◗ chemotherapy;◗ access to national and international clinical trials;◗ radiation therapy and enhanced brachytherapy
services;◗ supportive care and pain/symptom management;◗ nutritional consultation and rehabilitation support;◗ patient and community education in cancer
prevention;◗ hereditary cancer program;◗ breast health program in collaboration with the
FHA; and ◗ professional education/liaison for community
based cancer control programs.
The AHCC is also expected to become a centre forlearning, incorporating resources such as a jointhospital/cancer centre library and learning centre,along with facilities to enable the development ofpartnerships with nursing and medical schools.
Project Objectives and Scope
The primary objectives of the AHCC project are:
◗ to deliver a new facility and services that meet allthe expectations of the project’s vision andguiding principles; and
◗ to deliver a competitively-priced hospital andcancer centre better in design, construction andoperation than would have been provided througha traditional procurement process.
The scope includes the financing, design,development, construction, building maintenanceand facilities management services for a completefacility, and the procurement of certain medical andother equipment. The facility and services mustmeet specified performance standards as describedin the project’s output specifications, which weredeveloped in consultation with the health authorities.

6 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
The private partner will provide the followingfacilities management services:
◗ general management services (includingmanagement and administration of all otherfacility management services provided by theprivate partner, including functions such ashuman resources and quality monitoring);
◗ helpdesk services (provision of a single point ofaccess to all facility management services);
◗ food services (patient and non-patient);◗ housekeeping services;◗ laundry/linen services;◗ materiel services (management of goods
and supplies);◗ plant services (including facility maintenance,
repair and replacement);◗ protection services (security and safety);◗ patient portering;◗ utilities management; and◗ parking services.
The health authorities will provide all clinical anddiagnostic services, as well as facilitiesmanagement services not listed above.
Project Procurement Planning andOptions Analysis
The AHCC procurement followed extensiveprovincial and regional planning
Planning for replacement of the MSA Hospital hasbeen underway since the late 1980s, with thedecision to build a new hospital first announced in1990. Plans were developed, including full workingdrawings ready for tender; however, the project wasput on hold in 1997. It was reviewed again threeyears later and a proposal was developed tointegrate a cancer centre. A business case forprocuring the project as a traditional capital projectwas approved by the Province in spring 2001.
Later that year, the Province requested anotherreview of the project plan – this time, to focus on thepossibility of increasing private sector involvementto help reduce public sector costs and risks whilemaintaining or improving quality. This reviewreflected the policy goals of improving the capitalproject planning process and promoting soundfiscal management, public accountability andachievement of better value for taxpayers’ dollars.
The Finance-Design-Build-Operate-MaintainModel demonstrated the greatest potential toprovide value for money
Consistent with the requirements of the CapitalAsset Management Framework, the project teamconsidered traditional procurement and three publicprivate partnership procurement options:
◗ Traditional Capital Project, wherein the publicsector owns, finances, operates and maintains thefacility, with private partners engaged in designand construction under separate contracts.
◗ Design-Build-Maintain, wherein the public sectorowns, operates and finances the project butengages a private partner to design, constructand maintain the facility for a specified period of time.
◗ Design-Build-Operate-Maintain, wherein thepublic sector owns and finances the project butengages a private partner to design, construct,operate selected facility management servicesand maintain the facility for a specific period of time.
◗ Finance-Design-Build-Operate-Maintain, whereinthe private partner owns, finances, designs,constructs, operates selected facilitymanagement services and maintains the facility.
Each of the public private partnership options wasassessed against the traditional capital procurementmodel. While the total project costs of all theoptions were estimated to be financially similar, theproject team’s analysis concluded that the Finance-Design-Build-Operate-Maintain model offered thebest potential to deliver value for money throughinnovation, timely delivery and the most effective risktransfer to the private sector. This model was lateradapted to retain public sector ownership of theland and hospital and cancer centre.
7
Expected Benefits of the Preferred Option
In November 2002, the Province approved theFinance-Design-Build-Operate-Maintain model onthe basis of the following expected benefits:
◗ expedited construction and commissioning fromthe time of contract finalization;
◗ high levels of patient satisfaction;◗ a shift in the way health facilities and related
services are planned, financed and delivered,placing greater emphasis on performancestandards and outcomes and improved costeffectiveness. This was viewed as beingimportant for the future of health care in B.C.;
◗ the transfer to the private sector of risks that somepublic sector organizations have had difficulty inmanaging over time, such as construction risk,the risk of cost overruns, and operating risks, forexample with regard to facility maintenance andfunctionality; and
◗ increased financial discipline: experience in otherjurisdictions has demonstrated that privatepartners with at-risk capital invested in projectshave a greater stake in ensuring that facilitiesoperate fully, reliably and efficiently.
Project Implementation
A governance and management structure was put inplace to guide project development, procurementand implementation. It included a project team anda company – Abbotsford Hospital and CancerCentre Inc (AHCC Inc) – established under the B.C.Company Act as a formal decision making andcontractual vehicle. For further details on the stepstaken to structure the project, see Appendix A.
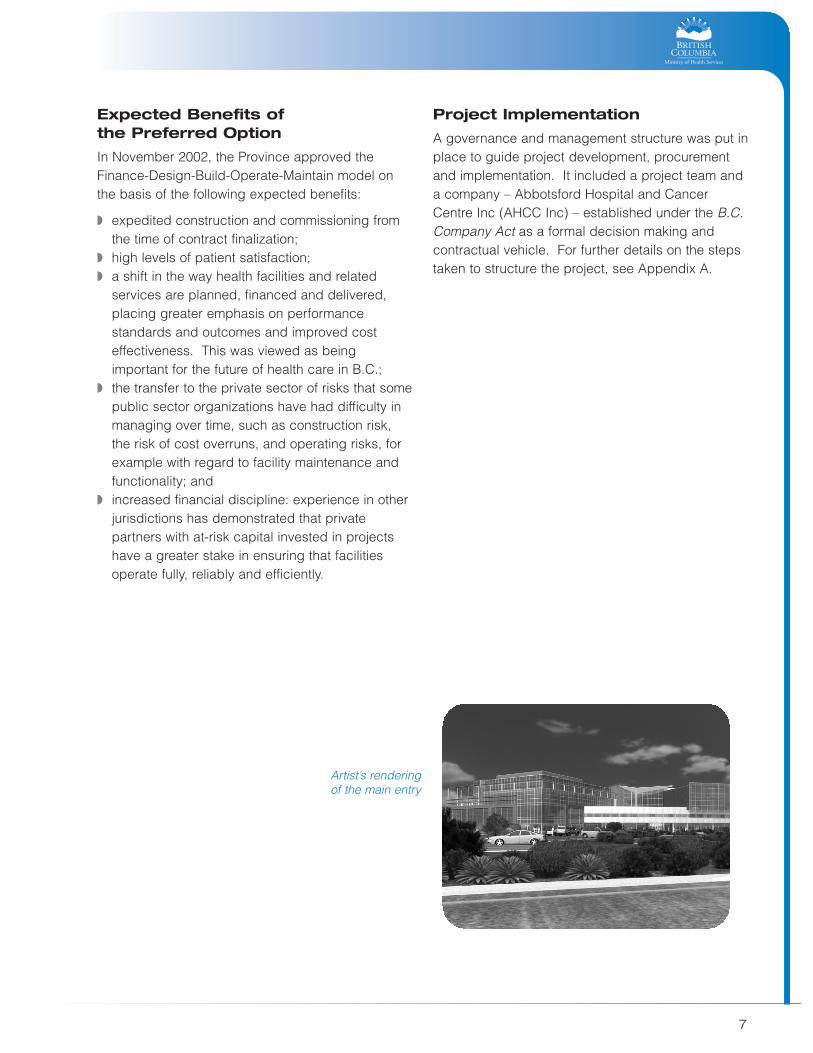
Artist’s rendering of the main entry
8 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Objectives
The competitive selection process had the following key objectives:
◗ select a qualified, experienced partner to finance, design, build, maintain and operate facilities managementservices for the AHCC;
◗ implement a fair, timely and competitive procurement process, and◗ achieve value for money.
Procurement Process and Timetable
3. Competitive Selection Process
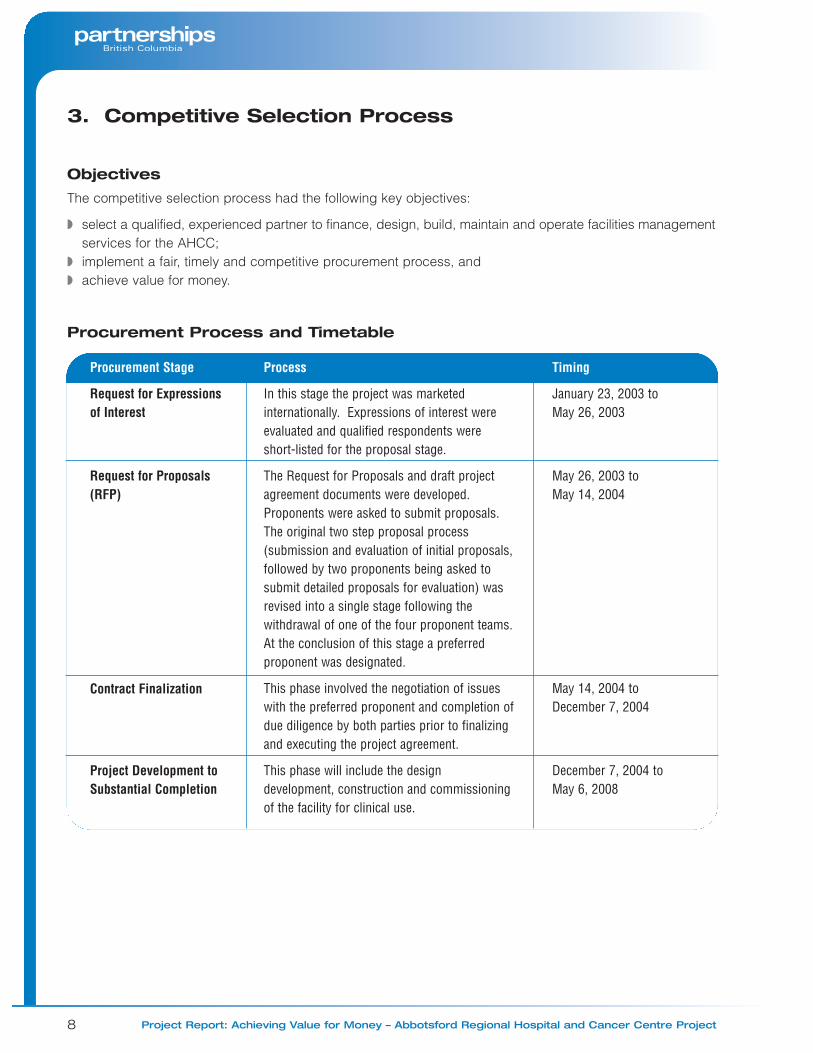
Procurement Stage
Request for Expressionsof Interest
Request for Proposals(RFP)
Contract Finalization
Project Development toSubstantial Completion
Process
In this stage the project was marketedinternationally. Expressions of interest wereevaluated and qualified respondents wereshort-listed for the proposal stage.
The Request for Proposals and draft projectagreement documents were developed.Proponents were asked to submit proposals.The original two step proposal process(submission and evaluation of initial proposals,followed by two proponents being asked tosubmit detailed proposals for evaluation) wasrevised into a single stage following thewithdrawal of one of the four proponent teams.At the conclusion of this stage a preferredproponent was designated.
This phase involved the negotiation of issueswith the preferred proponent and completion ofdue diligence by both parties prior to finalizingand executing the project agreement.
This phase will include the designdevelopment, construction and commissioningof the facility for clinical use.
Timing
January 23, 2003 toMay 26, 2003
May 26, 2003 to May 14, 2004
May 14, 2004 toDecember 7, 2004
December 7, 2004 to May 6, 2008
9
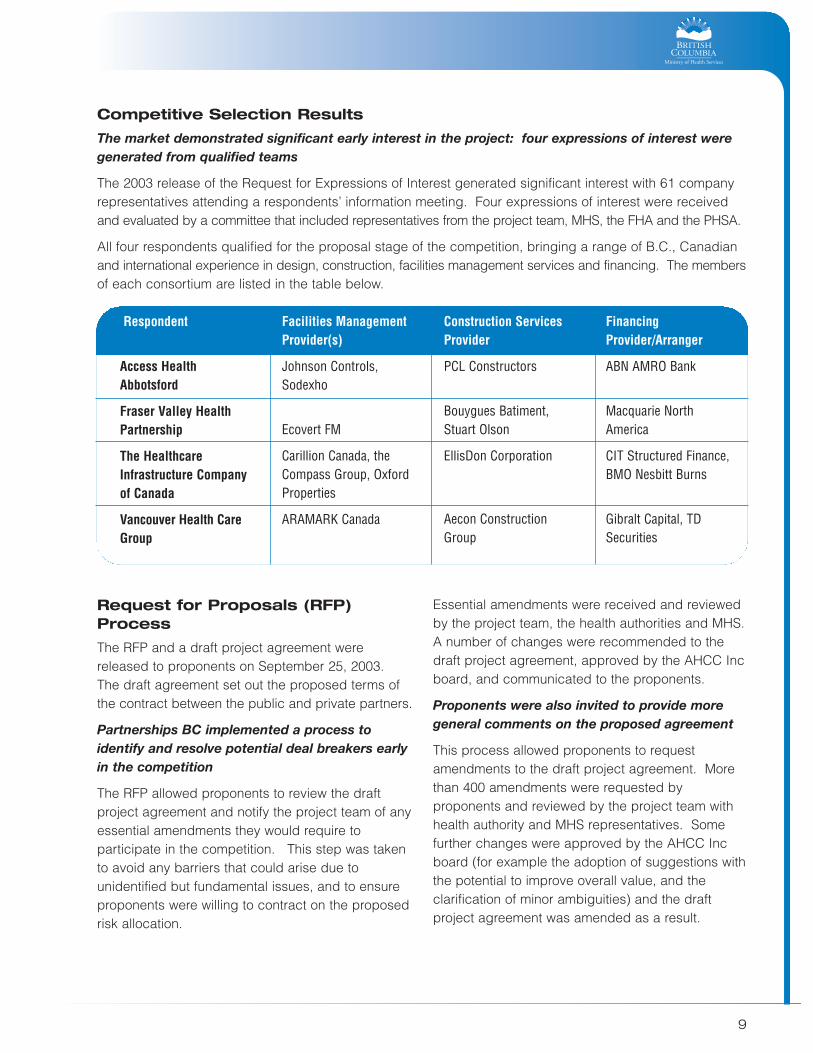
Competitive Selection Results
The market demonstrated significant early interest in the project: four expressions of interest weregenerated from qualified teams
The 2003 release of the Request for Expressions of Interest generated significant interest with 61 companyrepresentatives attending a respondents’ information meeting. Four expressions of interest were receivedand evaluated by a committee that included representatives from the project team, MHS, the FHA and the PHSA.
All four respondents qualified for the proposal stage of the competition, bringing a range of B.C., Canadianand international experience in design, construction, facilities management services and financing. The membersof each consortium are listed in the table below.
Respondent
Access HealthAbbotsford
Fraser Valley HealthPartnership
The HealthcareInfrastructure Companyof Canada
Vancouver Health CareGroup
Facilities ManagementProvider(s)
Johnson Controls,Sodexho
Ecovert FM
Carillion Canada, theCompass Group, OxfordProperties
ARAMARK Canada
Construction ServicesProvider
PCL Constructors
Bouygues Batiment,Stuart Olson
EllisDon Corporation
Aecon ConstructionGroup
FinancingProvider/Arranger
ABN AMRO Bank
Macquarie NorthAmerica
CIT Structured Finance,BMO Nesbitt Burns
Gibralt Capital, TDSecurities
Request for Proposals (RFP)Process
The RFP and a draft project agreement werereleased to proponents on September 25, 2003.The draft agreement set out the proposed terms ofthe contract between the public and private partners.
Partnerships BC implemented a process toidentify and resolve potential deal breakers earlyin the competition
The RFP allowed proponents to review the draftproject agreement and notify the project team of anyessential amendments they would require toparticipate in the competition. This step was takento avoid any barriers that could arise due tounidentified but fundamental issues, and to ensureproponents were willing to contract on the proposedrisk allocation.
Essential amendments were received and reviewedby the project team, the health authorities and MHS.A number of changes were recommended to thedraft project agreement, approved by the AHCC Incboard, and communicated to the proponents.
Proponents were also invited to provide moregeneral comments on the proposed agreement
This process allowed proponents to requestamendments to the draft project agreement. Morethan 400 amendments were requested byproponents and reviewed by the project team withhealth authority and MHS representatives. Somefurther changes were approved by the AHCC Incboard (for example the adoption of suggestions withthe potential to improve overall value, and theclarification of minor ambiguities) and the draftproject agreement was amended as a result.

10 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Participation in the competition was confirmed ina Proposal Competition Agreement
On November 19, 2003 two of the four proponentssigned the Proposal Competition Agreement andprovided AHCC Inc with letters of credit confirmingtheir participation in the proposal competition. TheProposal Competition Agreement also madeprovision for partial payment to unsuccessfulproponents that completed a proposal to offsetsome of the cost of proposal development, and tosecure intellectual property rights to material fromunsuccessful proposals.
The two confirmed proponents were Access HealthAbbotsford (AHA) and The HealthCare InfrastructureCompany of Canada.
Partnerships BC implemented an effectiverequest for information and bilateral process
Recognizing the need for controlled information flowbetween proponents and the project team duringproposal development, the RFP established aninquiries and communication process, including arequest for information process and a series of fulland partial team bilateral meetings. The bilateralmeetings provided comments and feedback on thegeneral acceptability of proponents’ ideas and wereattended by project team members, technical andcommercial advisers, and health authoritystakeholders.
Between October 2003 and April 2004, the projectteam responded to 118 requests for information andissued 14 addenda to the RFP document.
Partnerships BC responded to the singleproponent situation by retaining the RFPframework but strengthening evaluation
In January 2004, during proposal development, oneof the two confirmed proponents, The HealthCareInfrastructure Company of Canada, withdrew fromthe competition.
Partnerships BC reviewed procedural options in lightof the single proponent situation, and decided toretain the established RFP process because itprovided a rigorous framework of proponentrequirements, and a comprehensive evaluation
process that needed to be satisfied before a finalagreement could be negotiated. The evaluationprocess was strengthened by increasing thereliance upon and weighting of the public sectorcomparator (PSC) as the primary financialbenchmark. The PSC was kept strictly confidentialto help maintain competitive pressure.Confidentiality was also maintained around theproject team’s estimates for the value of risks.
AHA submitted a proposal on April 16, 2004.
Evaluation of AHA’s Proposal
PBC completed a comprehensive and rigorousevaluation process
Proposal evaluation was undertaken in two stages:
◗ Preliminary review and initial affordabilityconfirmation: The proposal was checked forcompleteness, clarifications were requested, andthe cost of the total service payment in the first fullyear of operations was confirmed.
◗ Detailed review: The proposal was evaluated indetail against the evaluation criteria set out in theRFP in each of the following categories:– clinical operations, efficiency and design– facilities management services and human
resources– construction– financial – partnering relationship and team integration
and delivery– risk transfer and commercial considerations.
Sub-panels evaluated the proposal’s strengths andweaknesses in each of these categories and maderecommendations to the proposal evaluationcommittee, which included representatives of theproject team, MHS and the health authorities. Thecommittee made an overall assessment of theproposal and determined whether requirements ofthe RFP had been satisfied.

11
Following this process, the evaluation committeerecommended that contractual negotiations shouldbe entered with AHA. This was confirmed by theAHCC Inc board in mid-May 2004, subject to thesatisfactory resolution of issues in the proposal thatrequired negotiation.
The project’s process monitor concluded that thecompetitive selection process was fair
Partnerships BC engaged a process monitor toadvise the project team on the development ofdocuments and processes during the competition.The process monitor was mandated to act as anindependent observer during both the bilateralprocess and the evaluation process. The monitorconcluded that both the Request for Expressions ofInterest and the RFP stages of the competitioncomplied fully with the Province’s policy for fairness,transparency and accountability, and wereconducted in accordance with best practices forgovernment procurement in Canada.
Contract Finalization andContractual Close
Partnerships BC established a team to negotiate afirm contract with AHA, and a process to ensure thathealth authorities and MHS were aware of progressand consulted on key operational issues.Negotiations proceeded steadily from mid-Maythrough July 2004, when the detailed terms of theagreement were established. Final negotiations anddue diligence were completed between July andDecember 2004.
Competitive Selection Costs
The AHCC is the first major hospital procured inB.C. as a public private partnership, and a highlevel of diligence was needed to effectivelyimplement this new procurement approach.Procurement costs, including the costs oftransaction and legal advisors, were $14.5 million tofinancial close. This represents approximately 3.4per cent of the project’s net present value, or 4.1 percent of the construction capital cost of the facilityand equipment.
More than half of these costs represent aninvestment in establishing best practices that will beapplied to, and help reduce procurement costs forfuture public private partnership projects. In fact,the form of project agreement developed for theAHCC has already been used as the starting pointfor another public private partnership project (theBritannia Mine Water Treatment Plant).
The treatment of these and other public sectorprocurement costs is further addressed inAppendix B.
Artist’s rendering of the exterior of the building
12 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
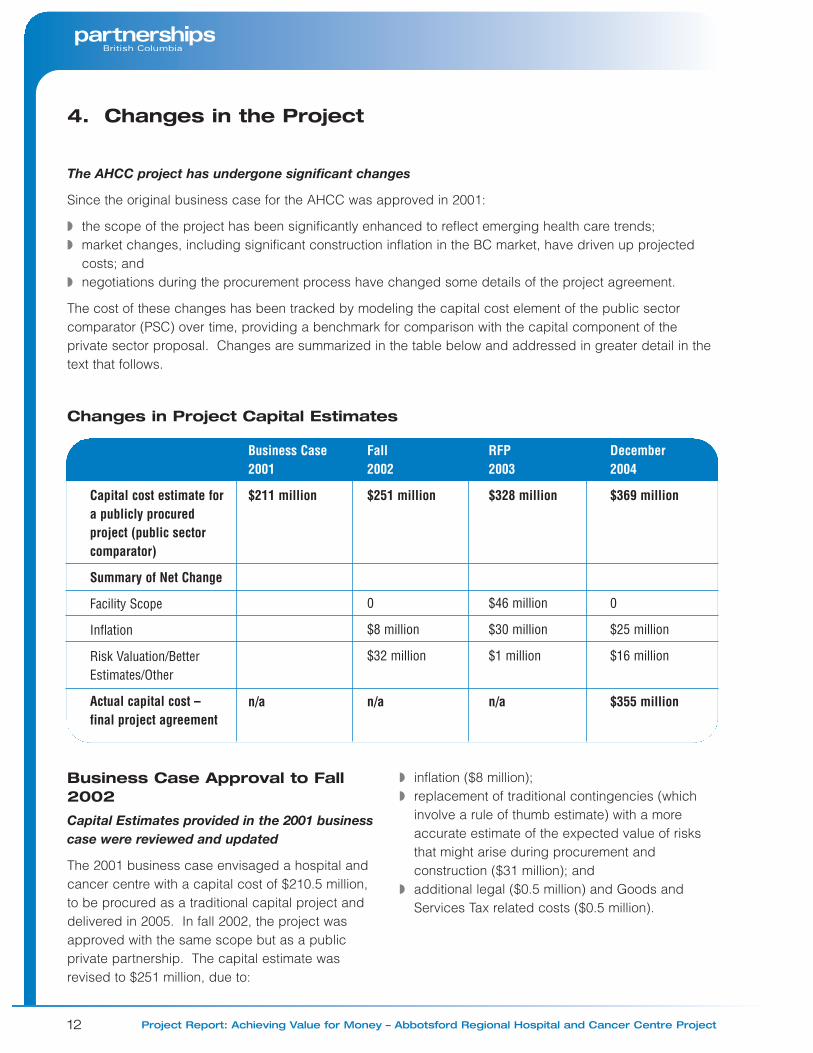
The AHCC project has undergone significant changes
Since the original business case for the AHCC was approved in 2001:
◗ the scope of the project has been significantly enhanced to reflect emerging health care trends;◗ market changes, including significant construction inflation in the BC market, have driven up projected
costs; and◗ negotiations during the procurement process have changed some details of the project agreement.
The cost of these changes has been tracked by modeling the capital cost element of the public sectorcomparator (PSC) over time, providing a benchmark for comparison with the capital component of theprivate sector proposal. Changes are summarized in the table below and addressed in greater detail in thetext that follows.
Changes in Project Capital Estimates
4. Changes in the Project
Capital cost estimate fora publicly procuredproject (public sectorcomparator)
Summary of Net Change
Facility Scope
Inflation
Risk Valuation/BetterEstimates/Other
Actual capital cost –final project agreement
Business Case2001
$211 million
n/a
Fall2002
$251 million
0
$8 million
$32 million
n/a
RFP 2003
$328 million
$46 million
$30 million
$1 million
n/a
December2004
$369 million
0
$25 million
$16 million
$355 million
Business Case Approval to Fall2002
Capital Estimates provided in the 2001 businesscase were reviewed and updated
The 2001 business case envisaged a hospital andcancer centre with a capital cost of $210.5 million,to be procured as a traditional capital project anddelivered in 2005. In fall 2002, the project wasapproved with the same scope but as a publicprivate partnership. The capital estimate wasrevised to $251 million, due to:
◗ inflation ($8 million);◗ replacement of traditional contingencies (which
involve a rule of thumb estimate) with a moreaccurate estimate of the expected value of risksthat might arise during procurement andconstruction ($31 million); and
◗ additional legal ($0.5 million) and Goods andServices Tax related costs ($0.5 million).
13
Fall 2002 to RFP Release(September 2003)
Significant enhancements were made to thehospital and cancer centre scope
Heath care is a fast developing area, significantlyaffected by a series of emerging trends. Thesecurrently include increasing moves towards short-stayand outpatient care, increased use of proceduressuch as MRI and nuclear medicine, and new clinicalchallenges such as the SARS (Severe AcuteRespiratory Syndrome) virus.
In light of this changing landscape, a clinical bestpractices review was undertaken in 2002 toreassess the hospital and cancer centre programdeveloped in 2000 and ensure that the AHCC couldfulfill its role as one of three FHA regional referralcentres. The process included literature reviews,visits and discussions with medical centres ofexcellence, interviews and discussions withphysicians, nurses and other professionals fromeach program area, and input from experiencedclinical programming consultants.
The project team, the health authorities and theirprofessional staff then developed a final clinicalprogram and detailed output specifications for theproject. Changes in scope at that stage includedthe following.
◗ Clinical best practices improvements– more space for education/academic activities;– changes related to infection control (for
example, four-bed rooms became private orsemi-private and the number of isolation roomswas increased to 50, driving significantincreases in equipment requirements);
– equipment enhancements, for example indiagnostic imaging:
– intensive care and coronary care units wereseparated; and
– a rehabilitation room was added to thesurgical floor.
◗ Increased capacity for digital applications in thehospital and cancer centre– the potential to accommodate electronic
administration and records; and – two of the eight operating rooms will be high
technology digital operating rooms, equippedwith what is referred to as “OR1” technology,including video and teleconferencing facilities.
◗ Facility and environmental improvements– separate entrances for ambulatory/cancer and
emergency care;– changes in building design to meet LEED
(Leadership in Energy and EnvironmentalDesign) Silver standards, setting a positiveenvironmental example and improving energyefficiency.
◗ Cancer centre enhancements– increased areas for radiation therapy; and – new breast and hereditary cancer programs to
improve screening and treatment.
As a result of these changes the building size wasincreased by 10 per cent and the overall estimate ofcapital cost, including equipment, increased byapproximately $46 million.
The scope of facilities management services wasmodified
Following a review of alternative service deliveryoptions, a list of non-clinical facilities managementservices, some of which were optional, wasproposed in the Request for Expressions of Interest.This list was refined for the RFP to reflect marketresponse and decisions by the project team (see thenext page). Services removed from the scope of theagreement will be performed by the public sector.
Market changes further affected estimates ofproject cost
In addition to the increased facility scope, risingconstruction costs and general inflation furtherincreased the capital cost estimate. When the RFPwas released, the PSC capital estimate for thefacility was $328 million, with an expected first yearannual service payment of $40 million.
14 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
RFP (September 2003) to Financial Close (December 2004)
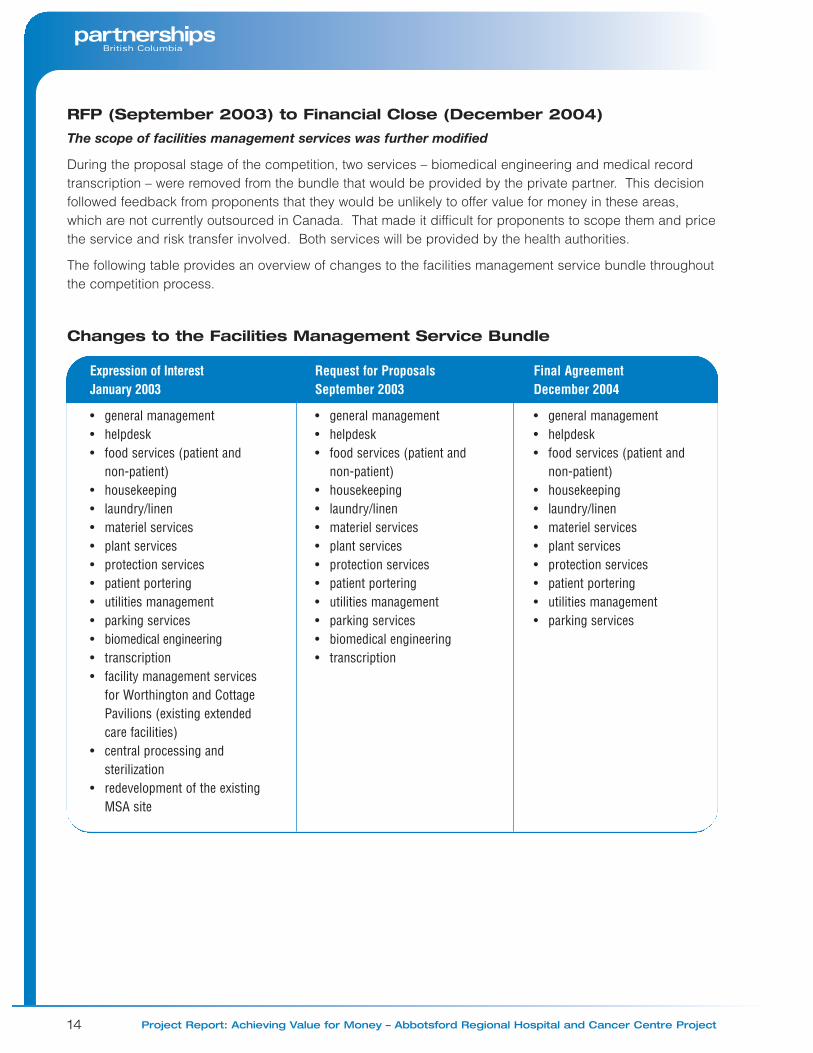
The scope of facilities management services was further modified
During the proposal stage of the competition, two services – biomedical engineering and medical recordtranscription – were removed from the bundle that would be provided by the private partner. This decisionfollowed feedback from proponents that they would be unlikely to offer value for money in these areas,which are not currently outsourced in Canada. That made it difficult for proponents to scope them and pricethe service and risk transfer involved. Both services will be provided by the health authorities.
The following table provides an overview of changes to the facilities management service bundle throughoutthe competition process.
Changes to the Facilities Management Service Bundle
Expression of Interest January 2003
• general management• helpdesk• food services (patient and
non-patient)• housekeeping• laundry/linen• materiel services• plant services• protection services• patient portering • utilities management• parking services• biomedical engineering• transcription• facility management services
for Worthington and CottagePavilions (existing extendedcare facilities)
• central processing andsterilization
• redevelopment of the existingMSA site
Request for Proposals September 2003
• general management• helpdesk• food services (patient and
non-patient)• housekeeping• laundry/linen• materiel services• plant services• protection services• patient portering • utilities management• parking services• biomedical engineering• transcription
Final AgreementDecember 2004
• general management• helpdesk• food services (patient and
non-patient)• housekeeping • laundry/linen • materiel services• plant services• protection services• patient portering• utilities management • parking services
15
Market conditions changed dramatically
Between the release of the RFP and the pricing ofthe proposal, construction cost inflation in the B.C.market increased dramatically, due to a buildingboom fueled by housing growth as well as theprospect of major projects related to the 2010Olympic Games, the Richmond/Airport/Vancouver(RAV) rapid transit project and the VancouverConvention Centre.
Project estimates of 2.5 per cent inflation werereplaced with actual and forecast inflation ratesranging from three to seven per cent to 2008. The project’s cost consultant concluded thatconstruction inflation would add approximately $25 million to estimated costs.
Additional items were added to the budget
Prior to receipt of the proposal, Partnerships BCidentified a number of items that had not beenincluded in the original PSC capital estimate, butneeded to be added to allow the PSC to becompared to the public private partnership. Theseitems included public sector management costs,which had not previously been taken into account(estimated to be around $8 million in a publiclyprocured project); the cost of facilities managementservices equipment (approximately $6 million); andthe cost of the equipment procurement team(approximately $1 million).
Further costs not recognized in PSC calculationswere identified during evaluation of AHA’s detailedproposal. For example, the proponent identifiedadditional costs around off-site hydro requirements(approximately $2 million), municipal levies(approximately $1.5 million) and soil survey costs(approximately $2 million), and demonstrated thatthe cost of achieving a LEED Silver standardbuilding would be higher than previously estimated(approximately $1 million more). These additionalcosts were also added to the PSC capital estimateso that the two estimates could be compared.
These increases in the PSC capital estimates afterthe release of the RFP (totaling approximately $25million) were partially offset by a reduction in thevaluation of risk (by approximately $9 million) overthe same period, reflecting ongoing review andevaluation of risk values as the project developed.
The final estimate of the PSC capital cost for theproject was approximately $369 million.
Final Cost Estimates and Actual Costs
The AHA proposal exceeded the RFP target forcapital costs. However, a review by a third-partycost consultant concluded that the proposal pricingwas consistent with current market conditions.
Following negotiations, the agreed-upon cost of thecapital construction and equipment component ofAHA’s contract was $355 million.
Project Affordability
Capital costs represent a relatively small proportionof the long term cost of a project like the AHCC;good decisions made during the design of such ahospital and cancer centre may increase capitalcosts, but can also increase efficiency and reduceoperating costs (both for the provision of clinicalhealth care services and facility managementservices) over the longer term.
To recognize this, overall project affordability, andoften project related decision-making, is based onprojected total annual operating costs. The mostsignificant of these are the health authorities’ clinicalcare and related costs; the other major cost is theannual payment to the private partner, whichreflects repayment of most of the facility’s capitalcosts, as well as maintenance and facilitymanagement services.
16 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
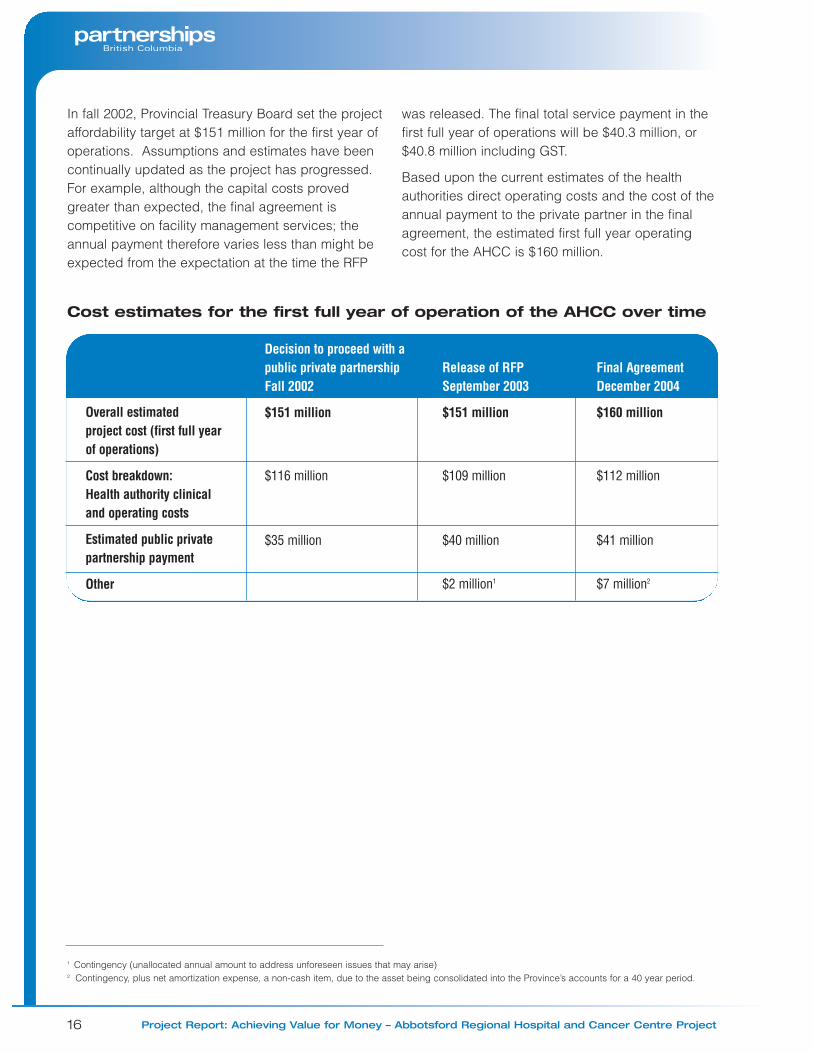
In fall 2002, Provincial Treasury Board set the projectaffordability target at $151 million for the first year ofoperations. Assumptions and estimates have beencontinually updated as the project has progressed.For example, although the capital costs provedgreater than expected, the final agreement iscompetitive on facility management services; theannual payment therefore varies less than might beexpected from the expectation at the time the RFP
was released. The final total service payment in thefirst full year of operations will be $40.3 million, or$40.8 million including GST.
Based upon the current estimates of the healthauthorities direct operating costs and the cost of theannual payment to the private partner in the finalagreement, the estimated first full year operatingcost for the AHCC is $160 million.
Overall estimatedproject cost (first full yearof operations)
Cost breakdown:Health authority clinicaland operating costs
Estimated public privatepartnership payment
Other
Decision to proceed with apublic private partnershipFall 2002
$151 million
$116 million
$35 million
Release of RFPSeptember 2003
$151 million
$109 million
$40 million
$2 million1
Final AgreementDecember 2004
$160 million
$112 million
$41 million
$7 million2
Cost estimates for the first full year of operation of the AHCC over time
1 Contingency (unallocated annual amount to address unforeseen issues that may arise)2 Contingency, plus net amortization expense, a non-cash item, due to the asset being consolidated into the Province’s accounts for a 40 year period.
17
Profile of the Private Partner
Access Health Abbotsford (AHA) combines theexpertise of a number of specialist organizations.
◗ Design: The facility design team includes SilverThomas Hanley, an Australian architecture firmwith extensive health care experience, includingin the design of cancer care facilities, andMusson Cattell Mackey, a well-establishedVancouver-based architecture firm.
◗ Construction: PCL Constructors Westcoast is amember of the PCL family of companies. PCL isa major Canadian construction contractor and hasextensive experience in North America on healthrelated facilities. PCL is building, or has built,health care facilities in eight provinces and allthree territories. Examples of recent projectsinclude the Ambulatory Care Expansion atWomen’s and Children’s Hospital in Vancouverand the Health Sciences Centre in Winnipeg. Equipment Planning Associates, a Canadian firmwith expertise in medical equipment planning andexperience, will support PCL in procuringequipment for the facility and will coordinatetechnical design and construction with equipmentrequirements.
◗ Facility management services: Propertymanagement services, including facility andphysical asset maintenance, will be provided byJohnson Controls. Johnson Controls has wideexperience in the development, integration andinstallation of building systems and controls. Itsrecent experience includes projects at RoyalInland Hospital in Kamloops and St. JohnsRehabilitation Hospital in Toronto. Facility management services including helpdesk, housekeeping, materiels, patient portering,laundry and linen, food services and parking willbe provided by Sodexho, a company withextensive experience in the provision of healthcare support services, supported by other wellqualified facility management service providers;for example, parking services will be providedby Intercon.
◗ Project development and financing: ABN AMROis one of the world’s largest financial institutionsand has operated in Canada’s wholesale bankingmarket for over 50 years. ABN has been involvedin structuring and underwriting more than 35public private partnership agreements in variousglobal markets.
Key Terms of the ProjectAgreement
Facility and Facility Management ServiceProvision and Standards
AHA will deliver a 300-bed (with 261 planned toopen in May 2008), 60,000 square metre hospitaland cancer centre at a new site on Marshall Road inAbbotsford, and will provide facilities managementservices for the new facility. Specifically, AHA will:
◗ design and construct the AHCC facility to anagreed-upon standard;
◗ finance the capital cost of the facility over theterm of the project (with the exception of thecapital contribution made by the Fraser ValleyRegional Hospital District (RHD));
◗ manage and operate the facility to agreedperformance standards with respect to:– general management;– helpdesk;– food services (patient and non-patient);– housekeeping;– laundry/linen services;– materiel services;– plant services (including facility maintenance);– protection services;– patient portering;– utilities management;– parking services; and
◗ maintain the hospital and cancer centre to anagreed-upon performance-based standard overthe term of the agreement, including therectification of defects or deficiencies that arisein the facility.
5. The Final Agreement
18 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Benchmarking and market testing
Under the agreement, every five years the cost ofservices such as food services and laundry andlinen supply will be compared against the generalmarket cost of the same services. Provided that AHA’sperformance in the preceding five years have metrequirements, its pricing for each service would bebenchmarked against comparable service providers.Should AHA prove to no longer be competitive, or iftheir satisfaction ratings do not meet requirements,AHCC would have the option of proceeding to fullmarket testing. This would involve re-tendering thespecific service, and could potentially result in achange of the sub-contractor within the AHA agreement.Any upward or downward change in the cost of specificservices following benchmarking or market testingwould be reflected in the annual payment to AHA.
Legal and Commercial Structure
Ownership of the site and hospital and cancer centreremains with the public sector. AHA is granted anon-exclusive licence to construct, manage andoperate the facility from the date of the projectagreement to the end of the project term. In addition,AHA has rights to provide patient entertainment andtwo areas of retail space, and may in future proposeother commercial opportunities (subject to AHCCInc approval).
The contract term is 33 years and five months.This includes a construction period and 30 years ofoperations from the expected date of substantialcompletion. The condition of the hospital andcancer centre at the end of the term is specified inthe agreement.
Public Interest Considerations
The project agreement is designed to protect thepublic interest through performance standards foroperations and maintenance. These are supportedthrough performance payments. AHCC Inc also hasremedies available to address any deficiencies orbreaches of the agreement. For example, it has theright to perform work itself where AHA fails to do soand offset related costs against payments to AHA.
The agreement also stipulates that service providersretained by AHA must be consented to by AHCC Inc,and that AHA will not provide health care servicesto patients.
The agreement includes a dispute resolutionmechanism to deal with any difference in interpretationor other disagreement relating to the projectagreement. The mechanism comprises processesto resolve disputes and obtain binding decisions.
Termination provisions are in place in the event thateither AHCC Inc or AHA fails to meet its obligationsunder the project agreement.
Design
AHA has drawn from health care facilities around theworld to produce a preliminary design expected tobe clinically functional and efficient, and to create ahealing environment that will reflect the projectvision. The AHA design team continues to workclosely with health care professionals on detaileddesign to ensure the facility meets the needs ofpatients, care providers and other users.
Features of the new facility include:
◗ a preliminary design that meets or exceedsrequirements for clinical functionality, operationalefficiency and design objectives. For example,maternity and the maternity operating room arelocated adjacent to the operating suite, providingflexibility in operating room use, improvingmaternity patient safety (due to the proximity ofthe operating suite), and improving efficiency byco-locating all operating rooms;
◗ site utilization that maximizes the preservation ofnatural features and is compact, allowing room forfuture expansion and additional commercial useson the site;
◗ a design that includes the flexibility to adapt tofuture health authority needs, and is capable ofboth horizontal and vertical expansion if requiredat a later date;
◗ a design that is aesthetically pleasing, creating ahealing environment. For example the use ofnatural light is maximized. Most patient rooms aresingle occupancy with direct access to windows,and support departments (such as the pharmacy)are located on upper floors with access to daylight;
19
◗ a design that is planned to meet LEED Silverstandards of environmental design and energyefficiency. The AHCC will be the first hospital inCanada to do so; and
◗ access to the outdoors for patients, families andstaff through a series of indoor and outdoorcourtyards and a roof deck.
Integrated facility management services
The project agreement provides for integratedfacility management services. A single help deskwill manage facility management service deliveryand provide a system for monitoring and reportingquality. Health care professionals and other userswill be able to contact all service areas, fromhousekeeping through to security, through a singlepoint of access. This is a much simplerarrangement than exists in any other B.C. hospital.
Financial Summary
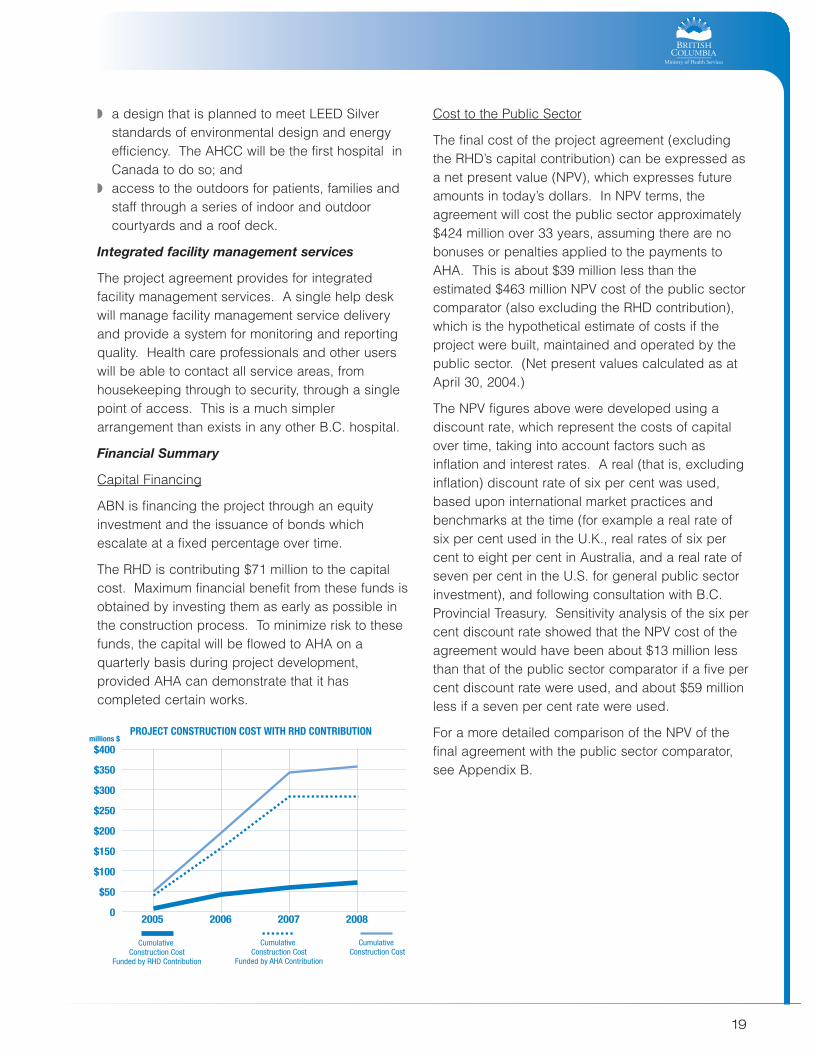
Capital Financing
ABN is financing the project through an equityinvestment and the issuance of bonds whichescalate at a fixed percentage over time.
The RHD is contributing $71 million to the capitalcost. Maximum financial benefit from these funds isobtained by investing them as early as possible inthe construction process. To minimize risk to thesefunds, the capital will be flowed to AHA on aquarterly basis during project development,provided AHA can demonstrate that it hascompleted certain works.
Cost to the Public Sector
The final cost of the project agreement (excludingthe RHD’s capital contribution) can be expressed asa net present value (NPV), which expresses futureamounts in today’s dollars. In NPV terms, theagreement will cost the public sector approximately$424 million over 33 years, assuming there are nobonuses or penalties applied to the payments toAHA. This is about $39 million less than theestimated $463 million NPV cost of the public sectorcomparator (also excluding the RHD contribution),which is the hypothetical estimate of costs if theproject were built, maintained and operated by thepublic sector. (Net present values calculated as atApril 30, 2004.)
The NPV figures above were developed using adiscount rate, which represent the costs of capitalover time, taking into account factors such asinflation and interest rates. A real (that is, excludinginflation) discount rate of six per cent was used,based upon international market practices andbenchmarks at the time (for example a real rate ofsix per cent used in the U.K., real rates of six percent to eight per cent in Australia, and a real rate ofseven per cent in the U.S. for general public sectorinvestment), and following consultation with B.C.Provincial Treasury. Sensitivity analysis of the six percent discount rate showed that the NPV cost of theagreement would have been about $13 million lessthan that of the public sector comparator if a five percent discount rate were used, and about $59 millionless if a seven per cent rate were used.
For a more detailed comparison of the NPV of thefinal agreement with the public sector comparator,see Appendix B.
20 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
While these net present value differences arerelatively modest, the final agreement is expected toprovide additional value for money by:
◗ shifting risk away from the public sector andmaking risk management substantially theresponsibility of the private partner;
◗ providing the public sector with greater certaintyaround the availability and ongoing standard ofthe hospital and cancer centre it will receive; and
◗ providing other qualitative benefits not captured inthe present value calculations (see Chapter 6:Comparisons for further detail).
Risk Allocation Summary
Risks have been allocated to the partner best ableto cost-effectively manage them. For example, thepublic sector is better able to determine whetherhospital and cancer centre design will meet healthauthorities’ clinical functionality needs. Similarly, theprivate partner will be better able to ensure thedesign will be cost effective from an operational andmaintenance perspective over the facility’s lifecycle.
Some risks are shared. For example, for utilityusage, both partners will share additional costsassociated with inefficiencies, and both will benefitfrom energy efficiency. For every shared risk theproject agreement stipulates how the risk will beallocated; for example, by providing thresholds foreach party’s responsibility for a certain risk. In theevent of any difference in interpretation of the riskallocation, the dispute resolution mechanism would apply.
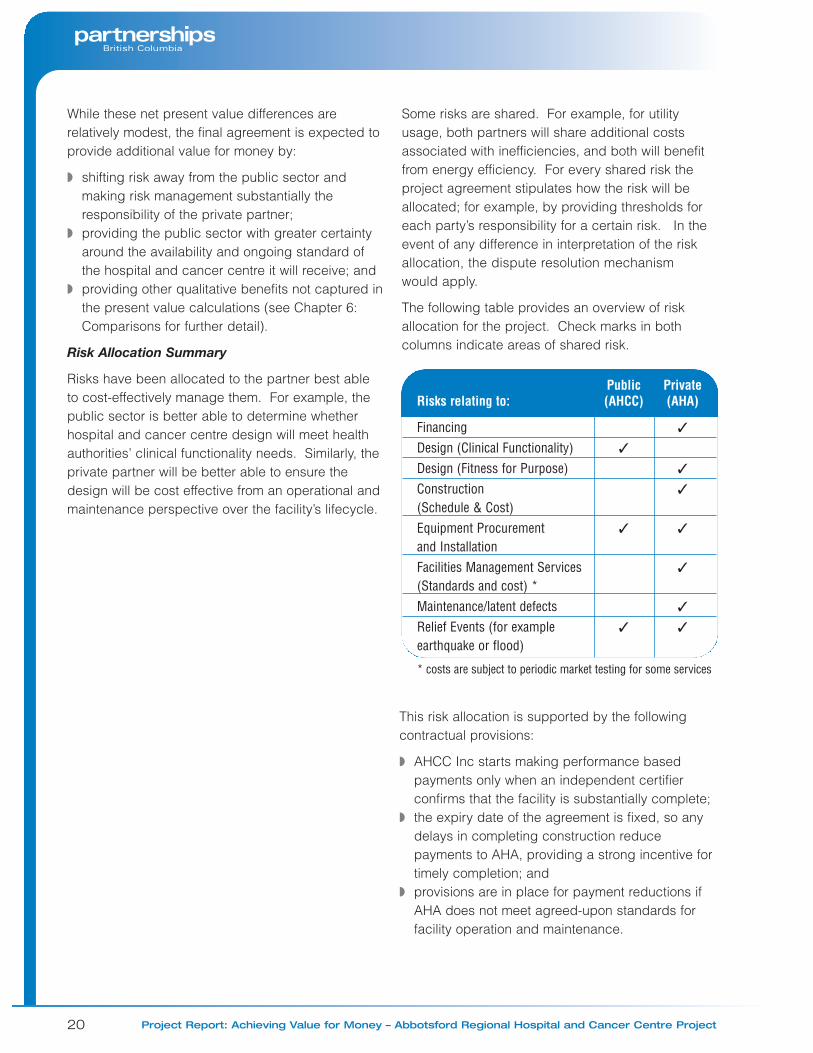
The following table provides an overview of riskallocation for the project. Check marks in bothcolumns indicate areas of shared risk.
Public Private Risks relating to: (AHCC) (AHA)
Financing ✓
Design (Clinical Functionality) ✓
Design (Fitness for Purpose) ✓
Construction ✓
(Schedule & Cost)Equipment Procurement ✓ ✓
and InstallationFacilities Management Services ✓
(Standards and cost) *Maintenance/latent defects ✓
Relief Events (for example ✓ ✓
earthquake or flood)
* costs are subject to periodic market testing for some services
This risk allocation is supported by the followingcontractual provisions:
◗ AHCC Inc starts making performance basedpayments only when an independent certifierconfirms that the facility is substantially complete;
◗ the expiry date of the agreement is fixed, so anydelays in completing construction reducepayments to AHA, providing a strong incentive fortimely completion; and
◗ provisions are in place for payment reductions ifAHA does not meet agreed-upon standards forfacility operation and maintenance.
21
Performance Payments
When the hospital and cancer centre is ready foroccupancy, AHCC Inc will commence performance-based payments to AHA for the facility, itsmaintenance and facilities management servicesover the term of the contract.
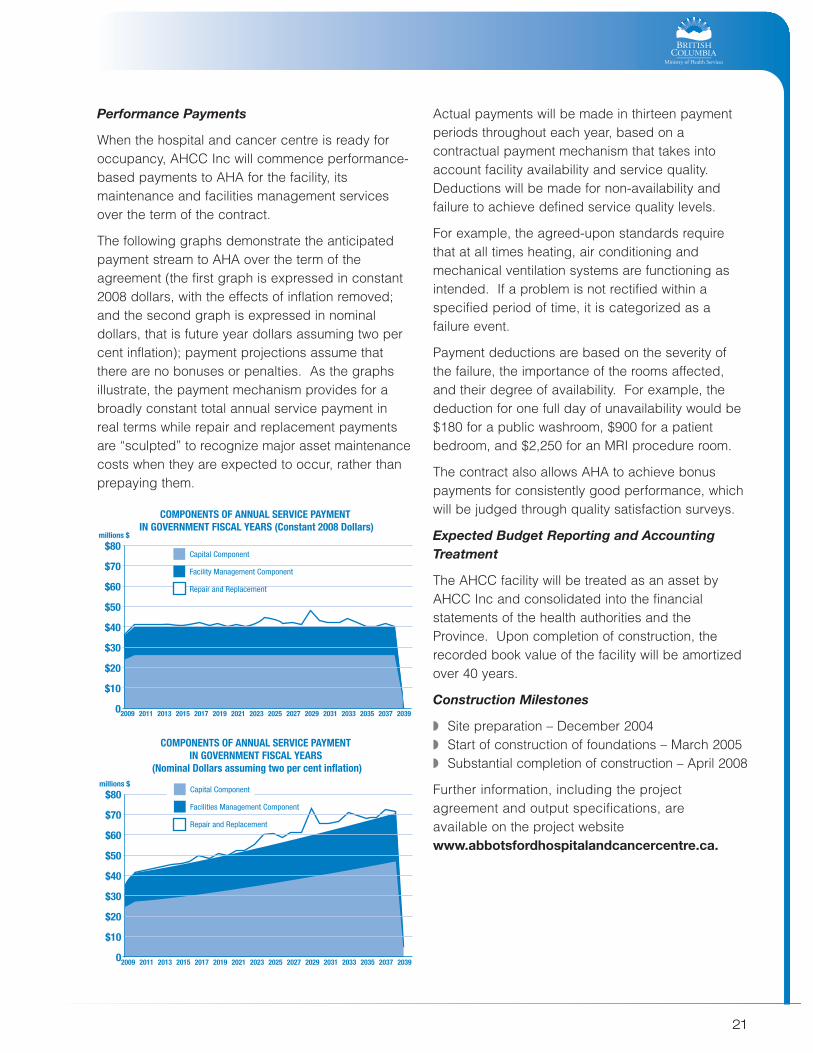
The following graphs demonstrate the anticipatedpayment stream to AHA over the term of theagreement (the first graph is expressed in constant2008 dollars, with the effects of inflation removed;and the second graph is expressed in nominaldollars, that is future year dollars assuming two percent inflation); payment projections assume thatthere are no bonuses or penalties. As the graphsillustrate, the payment mechanism provides for abroadly constant total annual service payment inreal terms while repair and replacement paymentsare “sculpted” to recognize major asset maintenancecosts when they are expected to occur, rather thanprepaying them.
Actual payments will be made in thirteen paymentperiods throughout each year, based on acontractual payment mechanism that takes intoaccount facility availability and service quality.Deductions will be made for non-availability andfailure to achieve defined service quality levels.
For example, the agreed-upon standards requirethat at all times heating, air conditioning andmechanical ventilation systems are functioning asintended. If a problem is not rectified within aspecified period of time, it is categorized as afailure event.
Payment deductions are based on the severity ofthe failure, the importance of the rooms affected,and their degree of availability. For example, thededuction for one full day of unavailability would be$180 for a public washroom, $900 for a patientbedroom, and $2,250 for an MRI procedure room.
The contract also allows AHA to achieve bonuspayments for consistently good performance, whichwill be judged through quality satisfaction surveys.
Expected Budget Reporting and AccountingTreatment
The AHCC facility will be treated as an asset byAHCC Inc and consolidated into the financialstatements of the health authorities and theProvince. Upon completion of construction, therecorded book value of the facility will be amortizedover 40 years.
Construction Milestones
◗ Site preparation – December 2004◗ Start of construction of foundations – March 2005◗ Substantial completion of construction – April 2008
Further information, including the projectagreement and output specifications, are available on the project websitewww.abbotsfordhospitalandcancercentre.ca.
22 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Value for money is a broad term that captures bothquantitative factors, such as costs, and qualitativefactors such as service quality. Partnerships BClooks at a broad range of factors in determiningwhether a project offers value for money totaxpayers, including comparison of the finalagreement to other benchmarks – in this case, theexpected results of a hypothetical traditional publicsector delivery model, and the expected results of ahypothetical public private partnership model,assessed prior to the procurement process.
Operational efficiency and clinicalfunctionality
◗ Traditional public sector delivery can achieve verygood results in designing a new health carefacility through careful scope definition and closecooperation between clinical planners, healthauthority users and architects. The partnershipapproach was expected to add to the traditionalapproach, which can be more prescriptive, byencouraging the private sector to focus onoutcomes and bring forward new ideas formeeting hospital and cancer performancerequirements.
◗ AHA provided a strong preliminary design.During negotiations, AHA’s clinical plannerworked with AHCC’s project team and healthauthority planners to further develop the design,and the results to date have been well receivedby the health authorities.
Design and Construction
◗ The public private partnership model is expectedto deliver the standards required as costeffectively as possible. The integrated nature ofthe project agreement is expected to balanceshort term design and construction with the needto consider the future costs of facility managementservice provision, maintenance and repair.
◗ Discipline will be brought to the process bylenders who will pay close attention to meetingthe construction budget and schedule as well aslonger term costs.
◗ The final agreement incorporates design andtechnical solutions that are new in B.C. Forexample, most B.C. hospitals include horizontalinterstitial spaces (spaces between floors) indiagnostic and treatment areas to allowmaintenance to take place without disruptingclinical services; the AHCC will include verticalinterstitial spaces in these areas, which need lessspace, are less expensive, and provide flexibilityin the hospital and cancer centre.
Equipment
◗ Early market sounding indicated there waspotential to bundle a significant proportion offacility equipment with the contract, drivinginnovation and reducing costs. During proposaldevelopment, it became apparent that additionalvalue for money would not be achieved this way,and AHCC Inc decided to deliver most equipmentthrough a cash allowance, retaining the risk oftechnology and price changes in these areas. Anadvantage of this is the ability to make equipmentselections as late as possible, thus procuring thelatest medical technology available.
◗ A benefit of the final agreement is that AHA willbe responsible for the procurement andinstallation of the equipment, and associated risks– such as ensuring that the equipment is installedwhen the hospital and cancer centre is ready toopen, and that service outlets are correctly locatedin rooms to meet equipment needs.
6. Comparisons
23
Facilities management services
◗ An expected benefit of the partnership model isthe introduction of a linkage between detailedperformance standards and payment. This hasnot previously been available in public sectorfacilities management delivery, although recentoutsourcing contracts have similar provisions.
◗ Partnerships BC believes that AHA’s integratedfacilities management solution, and the provisionof all services through a single help desk, willprove to be a significant benefit, simplifying healthprofessionals’ access to these services.
Delivery time
◗ Partnerships BC assumed that traditionalprocurement, with separate contracts for designand construction, would involve a 50 monthdelivery period from contract signing tocommissioning. The expected public privatepartnership delivery time was 36 months. Thefinal agreement is based on 41 months.
Financial
◗ When the project was approved as a publicprivate partnership, the cost was expected to besimilar to a traditional approach. Based upon thecurrent financial analysis, both the net presentvalue of the hypothetical traditional and publicprivate partnership models would be $463 million.
◗ The final agreement has a net present value of$424 million, demonstrating modest expectedpresent value savings of $39 million over thebenchmark estimates.
Risk transfer
◗ In traditional projects, design, construction,operations and maintenance are rarely integratedand the public sector retains significant risk.
◗ Expected risk transfer was reflected in theproject’s request for proposals; AHA proposedslightly less transfer of risk but at a lower cost,resulting in a more optimal final risk allocationthan had been expected.
◗ The level of investor capital (debt and equity) atrisk also provides a high level of comfort that AHAwill meet its contractual responsibilities.
Artist’s rendering of thebuilding exterior
24 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Partnerships BC is implementing a project management structure tailored to the needs of thedevelopment phase of the project
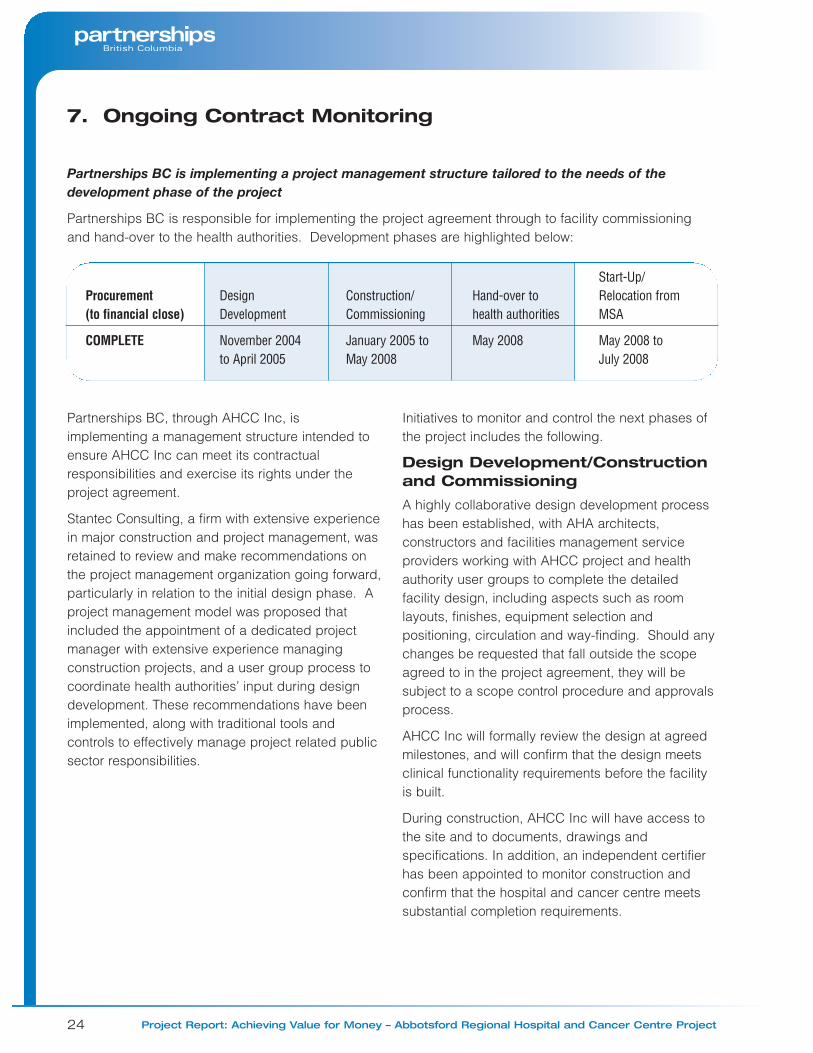
Partnerships BC is responsible for implementing the project agreement through to facility commissioningand hand-over to the health authorities. Development phases are highlighted below:
7. Ongoing Contract Monitoring
Procurement(to financial close)
COMPLETE
DesignDevelopment
November 2004to April 2005
Construction/Commissioning
January 2005 toMay 2008
Hand-over tohealth authorities
May 2008
Start-Up/Relocation fromMSA
May 2008 to July 2008
Partnerships BC, through AHCC Inc, isimplementing a management structure intended toensure AHCC Inc can meet its contractualresponsibilities and exercise its rights under theproject agreement.
Stantec Consulting, a firm with extensive experiencein major construction and project management, wasretained to review and make recommendations onthe project management organization going forward,particularly in relation to the initial design phase. Aproject management model was proposed thatincluded the appointment of a dedicated projectmanager with extensive experience managingconstruction projects, and a user group process tocoordinate health authorities’ input during designdevelopment. These recommendations have beenimplemented, along with traditional tools andcontrols to effectively manage project related publicsector responsibilities.
Initiatives to monitor and control the next phases ofthe project includes the following.
Design Development/Constructionand Commissioning
A highly collaborative design development processhas been established, with AHA architects,constructors and facilities management serviceproviders working with AHCC project and healthauthority user groups to complete the detailedfacility design, including aspects such as roomlayouts, finishes, equipment selection andpositioning, circulation and way-finding. Should anychanges be requested that fall outside the scopeagreed to in the project agreement, they will besubject to a scope control procedure and approvalsprocess.
AHCC Inc will formally review the design at agreedmilestones, and will confirm that the design meetsclinical functionality requirements before the facilityis built.
During construction, AHCC Inc will have access tothe site and to documents, drawings andspecifications. In addition, an independent certifierhas been appointed to monitor construction andconfirm that the hospital and cancer centre meetssubstantial completion requirements.
25
AHCC Inc will receive monthly inspection andprogress reports from AHA, and will be able toaddress any issues that arise at a joint projectmanagement oversight committee that meets atleast once per month. AHCC and AHA have agreedto a master schedule for design and constructionand will work together to identify and resolve anyissues that may put this at risk.
Start-Up, Relocation and HealthAuthority Commissioning
Partnerships BC is working with the healthauthorities to plan for the clinical start-up activitiesrequired for a new health facility. These includeclinical services redesign (for example, traininghealth professionals in the use of new IT devicesand equipment), clinical commissioning (such as thecalibration of radiotherapy equipment), relocationfrom the MSA Hospital, and organization of healthauthority policies and procedures for administeringthe project agreement during operations.
These activities would be required regardless ofwhether a traditional or public private partnershipprocurement model had been used for the project.They are related to, but not part of, the projectagreement and do not involve AHA. Typically,moving into a new health facility costs in the regionof half a year’s operating costs. Preliminaryestimates of the cost of start-up activities areapproximately $46 million.
Operations
After commissioning, the health authorities will takeownership of AHCC Inc and will be responsible foradministering the project agreement. Resources(three full time health authority employees) havebeen identified in the health authorities’ operatingestimates to perform these functions. The specificadministrative structure and procedures have yet tobe finalized, but key functions will be to ensure thatAHA is meeting performance standards through theimplementation of a contractually requiredperformance monitoring program (which will includequality satisfaction surveys of patients, visitors,health authority staff and medical staff).
Long Term Contract Review
Partnerships BC will work with MHS and the healthauthorities to design a process for reviewing theproject at appropriate intervals such as five, 10 or15 years from the start of operations. This reviewprocess will enable Partnerships BC to establishwhether the project agreement is functioning asintended, and whether the expected benefits havebeen realized.
26 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Partnerships BC has determinedsome best practices for publicprivate partnerships through theAHCC project
The AHCC is the first major B.C. hospital to beprocured through a public private partnershipmodel. As such, it has provided an importantopportunity to build on experience and develop bestpractices for future projects. As discussed below,best practices have been identified at each stage ofproject development.
Preparing the business case
Clarity around the project vision, success criteriaand cost estimates are essential.
◗ The AHCC business case was underpinned by avision and guiding principles. This provedcritical in defining success criteria, informingdecisions and providing a foundation for theevaluation process.
◗ Clearly defined contractual outcomes (in particularoutput specifications that are at least 80 per centcomplete) are important for the creation of reliablecapital and operating cost estimates.
◗ The public private partnership budgeting processcreated a clear understanding of all project-related cost elements, particularly with respect torisk and lifecycle cost elements such as ongoingmaintenance. Traditional capital budgeting tendsto be less specific, applying broad contingencyfigures for risk and rarely identifying lifecycle costs.
Approaching and developing the market
The emerging Canadian partnership market isbeing developed and nurtured to maximizecompetition.
◗ The number of participants in the North Americapartnership market is currently relatively small.Partnerships BC marketed the AHCC projectglobally prior to starting the competitive process,so as to maximize competition by encouragingcompanies with the required experience,expertise and capacity to participate.
◗ Ongoing market sounding proved to be animportant tool for ensuring a clear understandingof the level of interest in aspects of the project.
◗ When designing the competitive process, in orderto attract and maintain interest in the project it isimportant to consider pursuit costs for potentialproponents. These costs are driven by thenumber of stages in the process, the level of detailrequired in proposals, and the availability of partialcompensation for unsuccessful proponents.
◗ Through the AHCC and other projects,Partnerships BC has developed a thoroughunderstanding of international and Canadiandevelopers, sub-contractors, lenders andadvisors and is working with this community tofurther develop the B.C. market (and by extensionthe Canadian market). The broader and moreexperienced the B.C. and Canadian marketsbecome, the greater the participation andcompetition on future B.C. projects will be.
8. Best Practices
27
Structuring the proposedagreement
The project agreement between AHCC Inc andAHA will form a benchmark for the developmentof future partnership projects.
◗ The Canadian market has accepted the project’scontractual structure and the paymentmechanism, and these will be utilized as the basisof future partnership agreements.
◗ In moving to an output and outcome basedcontract, Partnerships BC has identified a numberof factors that contribute to sound contractdevelopment practices:– extensive input by the eventual hospital and
cancer centre users is required throughout theproject development process. In the case ofAHCC, the Fraser Health Authority andProvincial Health Services Authority made theproject a priority and provided significant support;
– the template for output specifications, togetherwith instructions on wording, should bedeveloped by the project’s legal adviser (thismitigates the risk of forming unintendedobligations, and assists in harmonizingspecification and contract language); and
– the market will price a “premium” for anyparticular service provision that is not welldefined or understood. For example,biomedical engineering and health recordstranscription fell into this category, andultimately were not included in the finalagreement so as to avoid such a premium.These services will be provided by the healthauthorities, as is currently the case.
Designing the procurementprocess
Good planning, organization and clarity willcontribute to a successful procurement process.
◗ The concurrent release of the draft projectagreement and the RFP gave proponents clearinformation on project requirements – such as theproposed risk allocation, evaluation criteria andsubmission requirements.
◗ The essential amendment process for identifyingpotential “deal breakers” significantly reduced thelength of negotiations. In future, with a precedentagreement available, the essential amendmentphase may not be required.
◗ Partnerships BC developed a well-organizedprocess for providing information andclarification to proponents during the proposaldevelopment process that should be applicablefor future projects.
◗ As on the AHCC project, evaluation teams shouldactively engage key project stakeholder groups,and be organized and well briefed prior to thecommencement of evaluation activities.
◗ It is critical that lenders have a strong involvementearly in the process. In the AHCC project, earlylender involvement resulted in financial closeseven months following the designation of thepreferred proponent; in the UK, similar projectswithout strong lender input have taken as long as18 months to reach financial close.
Increasing standardization
Standardization of documentation and processesis fundamental to increasing the efficiency of thepartnership procurement process in B.C.
◗ Market participants have encouragedPartnerships BC to standardize projectagreements, procurement documentation andprocurement processes where appropriate.
◗ The AHCC project involved legal and internationaltransaction advisers in structuring the project,developing procurement documents andmanaging negotiations. As the advisorycommunity gains experience with B.C. precedentdocumentation and identified best practices, theprocess of standardization will accelerate. Theform of project agreement used for the AHCC hasalready been applied to another B.C. publicprivate partnership project, the Britannia MineWater Treatment Plant project.
28 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Implementing governance andproject management
An effective and efficient governance modelrequires the project team to make decisions inan organized way; allows for reflection and theuse of second opinions; and enables the projectteam to focus on external issues.
◗ Partnership projects typically involve severalpublic sector stakeholders, which necessitates anaccountable, organized and consultativegovernance structure. The governance model forthe AHCC project was developed and streamlinedas the project developed and requirementschanged; the resulting use of an overall projectboard (AHCC Inc) as a single point of decisionmaking and contracting was very effective andthis structure could have applicability for otherprojects, particularly those involving a number ofgovernment stakeholders.
◗ Partnerships BC found that stakeholderconsultation was most effective when it focusedon principles, rather than specific drafting issues.
◗ U.K. experience has highlighted the need toapply appropriate resources to projectmanagement after financial close, to ensure thatall contractual commitments are effectivelyimplemented. Partnerships BC has implementeda project management structure and controls forthe AHCC project to maintain health authority andtechnical adviser input in the process; mitigate thoserisks retained by the public sector; oversee theperformance of the private sector; and thoroughlyand effectively implement the project agreement.
Artist’s rendering ofthe interior atrium

29
Project Governance
Partnerships BC is managing procurement of theAHCC project as an agent for the Ministry of HealthServices (MHS) and the Province. Partnerships BChas worked with MHS, the Fraser Health Authority(FHA) and the Provincial Health Services Authority(PHSA) to develop a consultative governancemodel, illustrated in the chart below. This model willbe used through to facility commissioning.
AHCC Project GovernanceStructure
Abbotsford Hospital and Cancer Centre Inc(AHCC Inc) was established under the CompanyAct as a formal decision making and contractualvehicle for purposes of the partnership. The originalboard comprised three directors representing MHSand Partnerships BC.
Following the release of the Request for Proposals inSeptember 2003, health authority representativesattended board meetings as observers. After thefinancial close of the project agreement, theyjoined as directors, while representatives of theFraser Valley Regional Hospital District (RHD),which is making a significant capital contribution to the project, attend board meetings in anobserver capacity.
Following construction, all shares of AHCC Inc willbe transferred from Partnerships BC to the FHA andPHSA for the operations phase of the project.
The Project Advisory Committee was establishedto oversee the project’s development and progressand to ensure that clinical and service needs weretaken into account. Committee members includedrepresentatives of MHS, FHA, the PHSA and theRHD. This committee had a significant role inshaping the project and supported the developmentof detailed consultation processes for specificaspects of project procurement to provide aneffective interface with the health authorities. Thecommittee discontinued meeting after August 2004.
A Hospital Construction Committee has been inplace since May 2003. Members are local MLAsand representatives of the RHD. The committeeprovides a valuable channel of communication withthe community, providing updates on projectprogress and keeping the project team advised oflocal issues and concerns affecting projectdecision making.
Appendix A:Developing and Structuring the Partnership Approach
Ministry of HealthServices
Approval of projectscope and budget
Ministry of Finance
Approval of Funding
HospitalConstructionCommitteeInput fromCommunity
Stakeholders
AHCC IncBoard of Directors
Decision making
Project AdvisoryCommittee
(disbanded at financial close)
Advice andRecommendations
Partnership BCProject Team
Project Delivery
30 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
The Project Team includes a chief project officer, aproject financial officer and project leadersresponsible for commercial, procurement andtechnical services. Key team members wereseconded to Partnerships BC from FHA, bringingwith them knowledge of previous planningprocesses and health authority facility requirements.Health authority representatives also work closelywith the project team and advise on clinical andfacility management related issues. During theproject structuring, competitive selection andnegotiations, the project team included personnelwith international transaction and legal expertise.
The project team has used a range of classicproject management techniques such as schedulingand scope control, following the strategy outlined inthe project procurement plan covering the period tofinancial close. That plan is being succeeded by aproject management plan to completion ofconstruction and commissioning, which focuses onhow the public sector will implement its part of theproject agreement.
Project Structure and Design
Partnerships BC has searched for and utilizedbest practices in structuring the project
Best practices can be defined as the set ofprocesses, techniques or management methodshaving either a demonstrable record of success orrepresenting the approach most likely to achievesignificant improvements in terms of cost, quality,schedule or other specified criteria.
Since public private partnership procurement is stillrelatively new in B.C., Partnerships BC learned fromthe considerable experience of other jurisdictionssuch as the U.K. and Australia. Partnerships BChas drawn on this experience and assimilated bestpractices into the structure of the AHCC project,paying particular attention to the successes andlessons learned during the development of the U.K.Private Finance Initiative model. This is the mostdeveloped partnership model in the world in termsof delivering health infrastructure and non-clinicalsupport services.
Partnerships BC adapted the UK partnershipmodel for BC conditions
The U.K. model for partnership delivery wasadopted as a general baseline with adaptations forB.C. and Canadian circumstances. It is based on astandard form of project agreement – an output-basedcontract, rather than the prescriptive arrangementtypically seen in traditional procurement projects –along with a performance-based paymentmechanism. Several aspects of the U.K. modelwere modified for use in B.C.
Under most U.K. public private partnerships, theprivate party owns the facility until the end of thecontract term. Partnerships BC modified thisapproach to increase protection of the publicinterest, using instead a licence structure that keptfacility ownership in public sector hands andprovided superior tax efficiency, simplicity andflexibility. The licence gives the private partnerrights, such as access to the site, to perform itsobligations. The U.K. is increasingly shifting to thiscontractual model in its agreements.
Comprehensive output specifications define theprivate party’s deliverables in the project agreement.Developing these was a major focus for the projectteam in close consultation with health authorityrepresentatives and project advisors. The outputspecifications were developed as follows:
◗ Clinical/non-clinical: Output specificationsdescribe the clinical (e.g. emergency andambulatory) and non-clinical (e.g. informationmanagement and learning centre) programs thatwill take place in the facility, along withinformation such as required adjacencies androom sizes. These specifications are the basisupon which the private partner designs thefacility. The U.K. model for specificationdevelopment was adapted to reflect the AHCCfacility program and Canadian health carepractices and requirements.
◗ Design and Technical: Output specificationswere developed specifically for the project, takinginto account Canadian standards, building codesand other codes required in B.C.

31
◗ Facilities Management: The starting point for thefacilities management output specifications wasthe U.K. standard model, which was thenmodified to reflect Canadian terminology and B.C.hospital operation practices. These specificationsdefine the requirements and performancestandards for each service. For example, theprivate partner is required to provide laundry andlinen services 24 hours per day, 365 days peryear, and, among other requirements, there mustbe sufficient clean linens and uniforms at alltimes. A quality monitoring system will bedeveloped to identify whether performanceindicators are met.
Following a review of alternative service deliveryoptions, a list of facilities management services wasrecommended for consideration as part of theprocurement package. This package was reviewedand amended over time to arrive at the final facilitiesmanagement services package. For further detail,see Chapter 4: Changes in the Project.
Equipment represents about one third of the capitalelement of the project. The initial equipment strategywas to transfer as much risk as possible to theprivate partner where cost effective, maximizingclinical input by choosing specific equipment itemsas late as possible to provide a balance betweenchanging technology and construction/installationrisks, and to maximize the use of existing procurementcontracts where they represent best value. Theequipment strategy was modified over time to reflectmarket response (for more details see page 22).
Risk analysis is required in all capital projects, but ismuch more significant in a partnership project whererisks must be categorized, valued and considered inlight of whether they would be more appropriatelymanaged by the public or private sector. Theproject team developed an extensive risk matrix,which was reviewed and endorsed by the project’stransaction advisors and formed the basis of thevaluation of risk, and the initial allocation presentedin the project agreement.
The payment mechanism is critical for effectivedelivery of the project agreement. It defines muchof the risk transfer and establishes incentives for the
private partner to offer continuous services toagreed-upon performance standards. The standardU.K. payment mechanism model was used as astarting point, with the following modifications:
◗ the mechanism was simplified to improve ease ofadministration;
◗ provisions were made for surveys to ensure thatuser satisfaction is reflected; and
◗ a bonus system was included to encourageconsistently good service, and to help foster apositive working partnership.
Development of the Public SectorComparator (PSC) as a benchmark
Under the partnership model, the private sectorpartner will finance, design, build, equip, maintainand provide facility management services for theAHCC for a total annual service paymentcommencing after construction. The PSCrepresents a hypothetical, risk adjusted estimate ofpublic sector costs to procure the same scope ofwork though a traditional model, and serves as abenchmark for assessing the value for moneypotential of different options.
The AHCC PSC was modified as project plansevolved, and was approved as a benchmark by theAHCC Inc board prior to the receipt of AHA’sproposal. As new information was received,assumptions in the model were changed to reflectactual conditions. Changes to the PSC werereviewed and approved by the AHCC Inc board,documented, and reviewed and reconciled by Ernstand Young.
Procurement Strategy andProcess Design
A four-stage procurement process - Request forExpressions of Interest; Request for Proposals(RFP); Contract Finalization and Close; and ProjectDevelopment - was designed with extensive inputfrom the project’s legal counsel and process monitorwith the aim of achieving a competitive, rigorous, fairand transparent process.

32 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
Partnerships BC incorporated steps to make theprocess productive and efficient
These steps included:
◗ concurrent release of the RFP and a draft form ofproject agreement;
◗ a process to identify and, if possible, resolvepotential deal breakers early;
◗ provision of partial payment to offset some pursuitcosts for unsuccessful proponents, and inconsideration for the right to use aspects ofunsuccessful proposals;
◗ a well organized and managed bilateral andinformation process to assist proponents indeveloping their proposals; and
◗ guidance to proponents on an affordabilitythreshold for the project.
The process was also supported by ongoingconsultation with stakeholders (including MHS,health authorities, the RHD and governmentagencies) and third parties.
Advisors from Partnerships UK, Bevan Brittan (U.K.),Clayton Utz (Australia) and InfrastructureProcurement Partners (Australia) provided advice onthe RFP and the draft project agreement to ensureconsistency with best practices worldwide. CIBCWorld Markets reviewed the draft project agreementand confirmed prior to its release with the RFP thatthe proposed terms and conditions represented afeasible basis on which to approach proponents.The project’s financial model, PSC and risk matrixwere all reviewed by Ernst & Young, who confirmedthe reasonableness of the assumptions andcalculations either by independent verification ofmodel outcomes or by comparison of outcomeswith similar projects.
Artist’s rendering of thebuilding exterior

33
The bar charts below compare the make-up of thepublic sector comparator (PSC) relative to the finalproject agreement with Access Health Abbotsford.
Explanatory Notes
◗ The annual service payments that will be paid toAHA can be compared with the capital costs,facility management operating costs, repair andreplacement costs and transferable risk costs inthe PSC.
◗ The NPV charts refer to four categories of risk:– Transferable Operating Risk. Events that might
occur during the operating period (followingcommissioning) for which responsibility andconsequence could reasonably be transferredto the private sector in a public privatepartnership arrangement.
– Retained Operating Risk. Events that mightoccur during the operating period for whichresponsibility and consequence likely wouldnot be transferred to the private sector in apublic private partnership arrangement.
– Transferable Development Risk. Events thatmight occur during the development period forwhich responsibility and consequence couldreasonably be transferred to the private sectorin a public private partnership arrangement.
– Retained Development Risk. Events that mightoccur during the development period for whichresponsibility and consequence likely wouldnot be transferred to the private sector in apublic private partnership arrangement.
Appendix B:Comparison of the Net Present Value (NPV) of thePublic Sector Comparator with the Final Agreement

34 Project Report: Achieving Value for Money – Abbotsford Regional Hospital and Cancer Centre Project
◗ Public sector management costs reflect estimatedcosts through to commissioning. – Total public sector management costs for the
project, up to the time when the hospital beginsoperation, are projected to be $24.5 million. Ofthat, $19 million ($16 million present value) wasincluded in the public private partnership NPV.This figure reflects the project’s expectedprocurement costs excluding a portion of costsexpected to provide benefits to future projects(including one-time costs related tointernational advisers, legal costs and taxadvice). The procurement costs include theestablishment of a dedicated project team andthe cost of performing extensive due diligencearound the hospital and cancer centre programand the development of detailed outputspecifications.
– The PSC analysis assumes procurement costsfor a traditionally procured project of the samescope as the final agreement would beapproximately $8 million present value.Normally this type of project would be run by ahealth authority rather than a dedicated projectteam. The PSC procurement cost figureincludes direct costs such as salaries, legalfees and work related to clinical best practices,but assumes lower overheads, as well assubstantially lower costs relating to thedevelopment of the clinical program, thedevelopment of output specifications andrelated contractual documents and thecompetitive process.
◗ The Fraser Health Authority is making acontribution towards equipment in the newhospital. Normally equipment in an existinghospital would be transferred to a new hospital.This is not the case in this project, and insteadthe FHA is making a contribution of $4 milliontowards equipment.
◗ The present value of costs funded by the capitalcontribution made by the Fraser Valley RegionalHospital District (RHD) has been included in thegraph for completeness ($71 million, or $61 millionpresent value). These costs are provincialcommitments under the final agreement, but sincethey are funded by the contribution they are notgenerally included in the discussion elsewhere inthe document of the net present value cost of thePSC and final agreement to the province. Theeconomic analysis of the PSC and the finalagreement are affected in the same way by thisaccounting for the contribution and so thecomparison of the PSC to the final agreement isunaffected by this treatment.