Overview of male circumcision research in Uganda - Presented ...

Progress in male circumcision scale-up:
country implementation and research update
June 2010

List of Abbreviations ACHAP AfricaComprehensiveHIV/AIDSProgramme
AIDS AcquiredImmunodeficiencySyndrome
BLM BanjaLaMtsogolo
BOTUSA Botswana-USApartnership
CDC CentresforDiseaseControl
CHAM ChristianHealthAssociationofMalawi
CIDRZ CentreforInfectiousDiseasesResearchZambia
DHS DemographicandHealthSurvey
DMPPT DecisionMakersProgrammePlanningTool
FHI FamilyHealthInternational
FLAS FamilyLifeAssociationofSwaziland
GFATM GlobalFundforAIDS,TBandMalaria
HCP HealthCommunicationPartnership
HIV HumanImmunodeficiencyVirus
HMIS HealthManagementInformationSystem
IEC InformationEducationandCommunication
IMC InternationalMedicalCorps
Jhpiego JohnHopkinsProgramforInternationalEducationinGynaecologyandObstetrics
KAP Knowledge,AttitudesandPractice
M&E MonitoringandEvaluation
MC MaleCircumcision
MCC MaleCircumcisionConsortium
MOH MinistryofHealth
MOH&CW MinistryofHealthandChildWelfare
MOH&SW MinistryofHealthandSocialWelfare
MOVE ModelsforOptimisingtheVolumeandEfficiencyofMCservices
MSI MarieStopesInternational
NAC NationalAIDSCouncil/Commission
NGO NonGovernmentalOrganization
OR OperationsResearch
PEPFAR TheUSPresident’sEmergencyPlanforAIDSRelief
PSI PopulationServicesInternational
VCT VoluntaryCounsellingandTesting
QA Qualityassurance
QI QualityImprovement
RCT RandomizedControlTrial
RHRU ReproductiveHealthandHIVResearchUnit
SANAC SouthernAfricanNationalAIDSCouncil
SRH SexualandReproductiveHealth
TOT TrainingofTrainers
TRACPlus TreatmentResearchAIDS,TBandMalariaandotherepidemics
UNAIDS JointUnitedProgrammeonHIV/AIDS
UNFPA UnitedNationsPopulationFund
UNICEF UnitedNationsChildren’sFund
USAID UnitedStatesAgencyforInternationalDevelopment
USG UnitedStatesGovernment
UTH UniversityTeachingHospital
WHO WorldHealthOrganization
ZNFPC ZimbabweNationalFamilyPlanningCouncil
IntroductionIn2007,WHO/UNAIDSrecommendedthatmale
circumcisionbeincludedintheHIVpreventionpackage.
ThirteenSouthernandEasternAfricancountrieswith
highHIVprevalence,lowlevelsofmalecircumcisionand
generalizedheterosexualepidemicshavebeenidentified
asprioritycountriesformalecircumcisionscale-up,these
are:Botswana,Kenya,Lesotho,Malawi,Mozambique,
Namibia,Rwanda,SouthAfrica,Swaziland,Tanzania,
Uganda,ZambiaandZimbabwe.Thesecountrieshavebeen
engagedindevelopingprogrammesformalecircumcision
implementationandareatvariousstagesofprogramme
scale-up.
Tenkeyelementshavebeenidentifiedascriticaltomale
circumcisionprogrammescale-up,theseinclude:leadership
andpartnerships;situationanalysis;advocacy;enabling
policyandregulatoryenvironment;strategyandoperational
planfornationalimplementation;qualityassuranceand
improvement;humanresourcedevelopment;commodity
security;socialchangecommunicationandmonitoringand
evaluation.TheseareoutlinedinfullintheOperational
guidanceforscalingupmalecircumcisionservicesfor
HIVprevention,WHOandUNAIDS,2008whichcanbe
accessedathttp://www.who.int/hiv/pub/malecircumcision/
op_guidance/en/index.html.
Thisreportprovidesanoverviewofprogressinmale
circumcisionprogrammescale-upinallthethirteenpriority
countriesaccordingtothekeyelements.Informationfor
eachcountryhasbeencontributedbyfocalpersonsfrom
MinistryofHealth,UNAgencieswithincountries,PEPFAR
programmesincludingU.S.CentersforDiseaseControl,
USAID,andotherimplementingagenciesthroughregular
progressreports,collaborativeconsultations,meetingsand
discussions.Servicedeliverystatisticshavebeenprovidedas
muchaspossiblefromMinistryofHealthreports,however,
somestatisticswereprovidedbysupportingagencies.Most
oftheinformationhasbeencollectedduringthemonthof
May2010.
Thisreportalsocontainsasectiononplannedandongoing
researchinthefieldofmalecircumcisionforHIVprevention.
Wewouldliketoacknowledgethecontributionsofallthe
studysponsors,investigators,fundersandreviewers.
Anyfurtherupdates,revisionsorcorrectionscanbesent
tothemalecircumcisionforHIVpreventionClearinghouse
Botswana
Kenya
Lesotho
Malawi
Mozambique
Namibia
Rwanda
South Africa
Swaziland
Tanzania
Uganda
Zambia
Zimbabwe


SECTION ONECountry
implementation update
1
Botswana Statistics:• Population:1.8m
• HIVPrevalence:17.6%
• MCPrevalence:11.2%
Leadership, partnerships & advocacy1. Leadership:MOHleadingtheprogramme.Dedicated
MCcoordinatorappointedanddistrictandfacilitylevel
focalpersonsassigned.SafeMCreferencegroupisin
placeforadvisory,policyissues;chairedbyDirectorof
DepartmentofHIV/AIDSPreventionandCare.Technical
workinggroupinplacewithallpartnersrepresented,
STIunitisthesecretariat.NACsupportsresource
mobilization.
2. Partnerships:WHO,UNAIDS,ACHAP,CDC/BOTUSA,
I-Tech,Jhpiego,PSI.Partnersprovidefinancial,human
andtechnicalsupportresources.
3. Advocacy:FormerPresidentFestusMogaeis
chairpersonofNACandaleadingfigureinthe‘African
championsforHIVpreventioninitiative’.Heled
adoptionofMCasadditionalHIVpreventionstrategy
inBotswana.Sensitizationofpolitical(Cabinet,MPs)
andsocialleaders,media,civilsocietyorganizations,
privatepractitioners,healthcareproviders,medicalaid
schemesandpublicdonein2009.
Situation analysisRapidsituationanalysisofhealthfacilitiesconducted
bygovernmentandpartnersin2007.Resultsinformed
thedevelopmentofthenationalsafemalecircumcision
additionalstrategyforpreventionofHIV/AIDS.
In-depthneedsassessmentof51publicandprivate
facilitiesabilitytoexpandandstrengthensafeMCservices
conductedin2008/9whichinformedthedevelopment
ofthenationaloperationalplanforscalingupsafemale
circumcisioninBotswana:2011–2015.Situationanalysis
oftraditionalhealersalsoconducted.
Policy and regulatory frameworkMChasbeenincorporatedintoexistingHIVprevention
policy,approvedbycabinet.
Strategy and operational planStrategyapprovedbygovernment.Phasedscale-up
plantoreachMCprevalencerateof80%amongHIV-ve
males0-49yearsoldby2016.Sixfacilitiesselectedto
bestrengthenedascentersofexcellence.DMPPTused
toderivecostingandimpactdata.MCincludedinGFATM
application.
TrainingSafeMCtrainingcurriculumhasbeendevelopedwhich
includesavideo.
ByApril2010,90healthworkerstrained(medicalofficers
andnurses/socialworkers).Teamofmastertrainersfrom
I-TECHtrainedbyMOH.Currentlydecentralizedtraining
beingconductedinthecentersofexcellence.
TraditionalhealersHIVtrainingcurriculumhasbeen
developedwithsafeMC.
Quality AssuranceQAframeworkhasbeendeveloped,strategybeing
developed.WHOMCQAguideandtoolkithavebeen
adaptedandthestandardsadopted.TeamofQAfacilitators
weretrainedataWHOworkshopinSeptember2009.
Twentyeightfocalpersonsincentersofexcellencetrained
onQA.Externalqualityassessmentsconductedatfour
centersofexcellenceinFebruary2010.InternalQA
assessmentsongoing.
Service deliveryScalingupofservicedeliverystartedinApril2009withMC
servicesintegratedintoexistingHIVpreventionservices.
ThirtyfivepublichealthfacilitiesareperformingMC
includingthesixcentersofexcellence,sevenpublicclinics
andafewprivates.
CDC/ACHAP/WHOsupportedtheMOHtoprovidemassMC
servicesinJuly2009forinitiatesintheKgatlengdistrict.
1321initiateswerecounseledandofferedHIVtesting;
88.5%weretested,96.2%circumcised,3.8%excluded
with2%mildtomoderateadverseevents.Allinitiateswere
reviewed24-48hrspost-MC.
Servicedeliverystatistics:
MCsdonefromJanuary2009-March2010=6,180.
CommunicationAshort-termcommunicationstrategyhasbeendeveloped
toguideimplementationandaddressimmediatepublic
informationneeds.FirstphaseofstrategylaunchedinApril
2009asasix-monthmultimediacampaign;30billboards
erectedcountry-wideand32minibusesbranded.TV
messages,radiospots,newspapermessageswereaired.
BO
TS
WA
NA

2
KenyaStatistics: • Population:37.5m
• HIVPrevalence:7%forthecountry.
15.3%forNyanzaprovince.
• MCPrevalence:85%forthecountry.
40%forNyanzaprovince
Leadership, partnerships & advocacy1. Leadership:Leadership:MOHcontinuestoprovide
overalltechnicalleadership.Programmenow
mainstreamedintoMOHannualplanningprocess.A
nationalandprovincialtaskforceareoperational.Focal
MCpersonsatnationalanddistrictlevels.JointMC
inter-ministerialtaskforceworkingwell.
2. Partnerships:TheMCC(FHI,UniversityofIllinoisat
ChicagoandEngenderHealth),NyanzaReproductive
HealthSociety,ImpactResearchandDevelopment,
MSI,IMC,APHIA(EngenderHealth,PATH,PSI),UNICEF.
PEPFAR,WHO/UNAIDS,Gatescontinuetobekey
partners.WorldBankisnewpartnersinceJanuary
2010.
3. Advocacy:MinistryofMedicalServicescalledfor
continuedscaleupatrecentstakeholdermeeting.He
joinsvoicesfromPrimeMinisterMr.RailaOdingawho
hasendorsedthescaleupofMCandin2009metwith
thecouncilofLuoelderstopromoteMC.
Situation analysis SituationanalysiscompletedforNyanza,Teso,Turkanaand
Nairobiprovinces.
Policy & regulatory framework MCpolicyisinplace,called‘NationalguidanceforMC’to
enhanceacceptanceassomegroupsfeltthataformal
policywouldsuggestamandateofMCforallmen.
DMPPTtrainingdone,datacollectionbeingfinalizedand
reportavailablesoon.
Strategy and operational plan ThevoluntarymaleMCstrategicplanfornext5yearswas
publishedinApril2010;tobepostedonMCClearinghouse.
Keytarget:allprovincestohaveMCprevalenceof80%by
2013.Thetargetgroupsare15-49yearoldsandnewborns.
Aphasedapproachtoservicedeliveryunderway,with
initialprogammeinNyanza;NairobiProvincenowadding
activities;preparatoryactivitiesinWesternProvince.
Training
Nearly800providersofvariouscadreshavebeentrained.
Quality assurance Aqualityimprovementteamhasbeenestablished.Atthe
nationalleveltheM&EteamisinchargeofQI/QAinthe
healthsectorandMCisintegratedinthis.
WHOMCQAtoolkitisbeingused.Localadaptation
underway.
QAstrategyisinthestrategicplan.WHOsupportedQI
national/provincialtrainingApril2010.
Service delivery ServicedeliveryscaledupinNyanzaandstartedinNairobi.
MCservicesbeingofferedinprisons.
Servicedeliverystatistics:
MCsSept2008-April2010=110,000.
WorldBankfundingforpilotof5000MCinTesoarea.
Communication Communicationstrategypublished.Nationalharmonized
IECmaterialsdevelopedandbeingusedinfield.
Monitoring & evaluationM&Eframeworkinplace.M&Esystemandformstomonitor
MCuptakeandadverseeventsdevelopedandformsbeing
distributed.
M&EindicatorsdevelopedinlinewithWHO/PEPFAR
recommendations.
MCincorporatedintoroutineKenyaAIDSInformation
system.
KE
NY
A

Botswana
3
LesothoStatistics: • Population:2m
• HIVPrevalence:23.2%
• MCPrevalence:48%
Leadership, partnerships & advocacy1. Leadership:MOHisleadingtheprogramme.MCTask
Forcewithtwosub-committeeshavebeencreated:the
ClinicalandtheAdvocacyandCommunicationsSub-
committee.MCFocalpersonhasbeenidentifiedinthe
MOH.
2. Partnerships:PSI,PEPFAR,WHO,UNAIDS,UNICEF,
UNFPA.
3. Advocacy:Extensiveadvocacyhasbeendonewith
traditionalleaders.TraditionaltaskteamonMCformed.
Situation analysis Situationanalysisinformalhealthsectorhasbeen
completed.Finalreportprintedandreadytodisseminate.
Policy & regulatory frameworkMCPolicyhasbeenapprovedbyMoH&SocialWelfare
minister.Policysummarizedintoabrief,translatedin
Sesothoandreadytobedisseminated.MCscaleupwillbe
implementedaspartofacomprehensiveHIVHealthSector
Preventionstrategywithinthehealthsector;thispolicyis
alsoreadyfordissemination.
Regulationsdonotallowcertaintaskshiftingtonurses.
Areviewisplannedofregulationsandprocessesoftask
shiftinginLesothoandothercountries.
Strategy and operational planStrategyandoperationalplanapproved;awaitingaformal
launch.
GuidelinesoncomprehensiveHIVpreventionservicewith
MCasonecomponenthavebeenelaboratedandare
nowunderreview.Exploringwaysofhowtoworkwith
traditionalproviders.
Training Currentlytrainingplansnotyetdeveloped.
Quality assuranceQAactivitieshavenotbeenstarted.Supervisionguidelines
arebeingadapted.
Service deliveryFormalscale-uphasnotstarted.Districtassessmenton
comprehensiveHIVpreventionserviceistobeconducted;
findingstoinformplanningfortheseservices.Public-private
partnershipsbeingreinforcedasNGOsareinvolvedand
workinginlinewiththenationalguidelines.
CommunicationDevelopmentofIECmaterialsforHIVpreventionservices
includingMCisongoingwithinthehealthsector.
Monitoring and evaluation M&Eframeworkhasnotyetbeendeveloped.Planstobe
developedforoperationsresearch.
LE
SO
TH
O

Botswana
4
Malawi Statistics: • Population:13.2m
• HIVPrevalence:12%
• MCPrevalence:21%
Leadership, partnerships & advocacy1. Leadership:TheMOHisheadingtheMC
subgroupconsistingofnational,multilateral&NGO
representatives.AfocalpersonforMChasnotyetbeen
appointed.Highlevelleadershipisstillneeded.
2. Partnerships:WHO,UNAIDS,UNICEF,UNFPA,CHAM,
CDC,PSI,BLM.
3. Advocacy:Planningtoidentifyalocalchampionfor
MC.Advocacyisstillneededatvariouspoliticaland
healthproviderlevels.Advocacymeetingsheldin
2007;stakeholdersmeetingheldinAugust2009.
Situation analysis Datacollectionforsituationanalysiscompleted.Findings
anddraftreportpresentedtostakeholders;finalversion
withrecommendationsawaitingapprovalbythePermanent
Secretary.Mainfindings:conduciveenvironmentexistsfor
establishmentoffocusedMCprogramme.
Policy & regulatory framework Nopolicyorregulatoryframeworkexistsyet.
Strategy and operational plan Nostrategyoroperationalplanexistsyet.
TrainingTrainingactivitiesnotyetdeveloped;awaitinggovernment
policyandstrategy.
Quality assurance QAactivitieshavenotbeenstarted.
Service delivery Formalscale-uphasnotstarted.
AlocalNGO,BLMisprovidingMCservicesintheirclinics.
Servicedeliverystatistics:
MCsdoneDecember2009-May2010=1,200
Communication Acommunicationplanhasnotbeendeveloped.
Monitoring & evaluationM&Eframeworknotyetdeveloped.Operationsresearch
planstobedeveloped.
MA
LA
WI

5
MozambiqueStatistics: • Population:21m
• HIVPrevalence:16%
• MCPrevalence:56%
Leadership, partnerships & advocacy1. Leadership:MOHleadingtheprogramme.Anational
taskforceisinplace.MCfocalpersonidentifiedinMOH
(asurgeonworkinginthenationalreferralhospital).
2. Partnerships:PEPFAR,PSI,USG,WHO,UNAIDS,
UNICEF,JHPIEGO.
3. Advocacy:Formerpresidentsinvolvedin‘African
championsforHIVpreventioninitiative’visited
MozambiqueinJune2009.Afollowupplanofaction
includingcontinuousadvocacyforscalingupaccessto
MCserviceshasbeendiscussedwiththegovernmentof
Mozambique.
Situation analysis Ahealthfacilityreadinessassessment(facilityrapid
assessment)hasbeencompletedbyJhpiego.AKAPsurvey
isplannedfor2010.
Policy & regulatory framework NoformalMCPolicydeveloped.Anationalstrategyfor
intensifyingHIVpreventionactivitieswasadoptedand
launchedbythePresidentofMozambiqueinDecember
2008.
Strategy and operational plan AnoperationalplanforHIVpreventionhasbeendeveloped
whichincludesMC.Fivepilotsiteshavebeenselected.
Scale-uptobeinitiatedin2010.
TrainingAfewseniorstaffoftheMOHhavebeentrainedonMC.
Trainingplansandmaterialsarebeingdevelopedwiththe
supportofWHO,UNAIDSandJhpiego.
A‘trainingoftrainers’workshopisplannedfor2010which
willbefollowedbyacascadetrainingofstaffinall11
provincesin2010-2011.
Trainingmaterialsfortraditionalcircumcisersarebeing
developedbytheNationalTaskForce,tobefinalizedand
testedin2010.
Quality assurance QAtrainingmaterialsandmethodologyarebeing
developedbytheMCnationaltaskforce.Thematerialwill
betranslatedintoPortugueseandadaptedtothenational
contextin2010.FieldtestingandimplementationoftheQA
programisplannedforlate2010.
Service delivery Noformalscaleuphasstarted.MCservicesareprovided
ondemandandaspartofroutineminorsurgeryservices.
MCservicesaredeliveredmainlyingovernmenthospitals.
ThereisnoknownprivateproviderofMCservicesin
Mozambique.
Servicedeliverystatistics:
MCsdoneNovember2009toMay2010:853
Communication Acommunicationstrategyisbeingdevelopedwiththe
supportoftheNationaltaskforceandPSI.
Monitoring & evaluationM&EframeworkforMChasbeendeveloped.NinecoreMC
indicatorshavebeenselectedandvalidated.
Anoperationsresearchagendaisbeingdevelopedbythe
nationaltaskforce.
MO
ZA
MB
IQ
UE

6
NamibiaStatistics: • Population:2m
• HIVPrevalence:18%
• MCPrevalence:21%
Leadership, partnerships & advocacy1. Leadership:MOHleadingtheprogramme.ANational
TaskForceisinplace.MCfocalpersonidentifiedin
MOHandMCCoordinatorhired.
2. Partnerships:WHO,UNAIDS,PEPFAR(IntraHealth,
I-Tech,PSI),CDC.
3. Advocacy:The‘AfricanChampionsforHIVPrevention
Initiative’visitedinJune2009.Advocacydonefor
healthworkers;advocacywithtraditionalleadersis
required.
Situation analysis Situationanalysisreportnowavailable.
Situationanalysisneededintermsofunderstanding
traditionalcircumcisers’practices.Workshopwithtraditional
healersisbeingplanned.
Policy & regulatory framework ReviseddraftpolicysubmittedtoMOHManagement;
includestaskshiftingofsurgicaltaskstonurses.
Thisdraftpolicyavailableandguidingpilotingprogramme.
Strategy and operational plan Strategyhasbeendevelopedandbeingrolledoutina
limitednumberofpilotsites;plansunderdevelopment.
Costingandimpactdataforthenationalstrategywas
derivedbyusingtheDMPPT,butDMPPTtoberedonegiven
newinformation.
TrainingTaskForcedevelopedMCtrainingcurriculum&addingto
VCTcurriculum.TwoMCtrainingshavebeenconductedin
2009;1in2010.Pilotinginselectedhealthfacilities.Also
MCprojectmanagementcoursewithhospitalmanagement
staffatpilotsites.
Quality assurance QAtrainingwillbeincludedinthepilotprogrammethatis
underway;trainersfollowuptrainees.
Service delivery Formalscale-upnotyetstartedbutatpilotsitesservice
deliveryunderway.
Fivepilotsiteshavebeenidentified.Threesitesarein
operation.ThreededicatedMCteams(MD,Nurse)hired
tomitigateHRconstraints.Assessmentoffivefacilities
todeterminefeasibilityofintroductionofvolunteer
programmedone.
Servicedeliverystatistics:
MCsdoneAugust2009toMay2010=340.
Communication Communicationstrategyatfinalstageofapproval.
MCcommunicationmaterialsarebeingproduced.Concerns
aboutmatchingriseindemandwithsupply
Monitoring & evaluationM&Esystem,databaseandtoolsdeveloped,appliedand
revisedbasedonpilotsiteexperience.
Noplansinplaceyetforoperationsresearch.
NA
MI
BI
A

7
RwandaStatistics: • Population:9.3m
• HIVPrevalence:3%
• MCPrevalence:12%
Leadership, partnerships & advocacy1. Leadership:NAC(CNLS)coordinatesandleadsmulti-
sectoralapproach;MOHresponsibleforMCasasurgical
interventioninhealthfacilities&ensurenormsand
standards.TRACplusresponsibleforMCwithinHIV.
TechnicalWorkingGroup(TWG)since2008aspartof
NationalHIVpreventionTWG;withsubgroupsoncost
andimpact.MCfocalpersonappointedandislocatedin
TRACplus&CNLS.
2. Partnerships:WHO,UNAIDS,UNICEF.USG,Jhpiego,
civilsocietyorganizationsespeciallyyouth.
3. Advocacy:Symposiumoncosteffectivenessof
paediatricMCin2007.Nationaladvocacycampaign
conductedinSeptember/October2008.
Situation analysis Facilityreadinessassessmentcompleted.Dataisbeing
analysed,reportexpectedDecember2009.
KAPsurveyongoing-toinformstrategyplandevelopment.
Onechallengeisthemobilityofhumanresources
Policy & regulatory framework MCintegratedinNationalHIVpreventionpolicy;MC
specificpolicyunderdiscussion.DMPPTmeetingplanned
Strategy and operational plan MCdraftnationalstrategyawaitingfinalapproval;MC
includedinNationalStrategicPlan.Formalimplementation
strategynotyetavailable.Nationalguidelines(normsand
standards)forimplementationdeveloped;awaitingfinal
approval.
DMPPT:Guidelinesintheprocessofdevelopmentfrom
decisionmakersbasedonpolicyscenariosthatconsider
resourcescurrentlyavailableforMCortheprevention
keyresultintheNationalStrategicPlan;onescenarioto
beselectedandnextstepsforoperationalplanstobe
developed.
Onechallengeisthedevelopmentofascaleupplan.
TrainingTwoprogrammemanagerstrained;sixNationaltrainers;
sitestafftrained:69nurse/counsellors,17providers.
Trainingandcapacitybuildingofhealthworkersfromarmy
healthservicesinKanombeandKaduhaconductedin
September2009.
Quality assurance QAframeworkandstructurenotyetdeveloped.
Service delivery FoursitessupportedbyJhpiego.Ongoingimplementation
ofservicedeliveryinmilitaryfacilities.
JointMCimplementationplannedin2districtswithUNICEF,
WHOUNAIDS.
Servicedeliverystatistics:
MCsdoneOctoberthroughtoMay2010=542.
Communication CommunicationthroughRwandaHealthCommunication
Centre.TRACPlushastargetedall30districtmayorsto
includeMCintheirHIV/AIDScontrolplans.
OnechallengeisthemisconceptionsaboutMCinthe
generalpopulation.
Monitoring & evaluationNationalM&EplanforHIV/AIDS(2009-2012)ongoing.
RW
AN
DA
8
South AfricaStatistics: • Population:48.5m
• HIVPrevalence:18.1%
• MCPrevalence:35%
Leadership, partnerships & advocacy1. Leadership:MOHisleadingwithSANACand
ProgrammeImplementingCommittee;Deputy
PresidentisChairofSANACandthereisaMCfocal
personinMOH.Anationalmulti-sectoraltaskforceon
MMC,chairedbytheChiefDirectorofHIVandAIDS,
willbeconstitutedandserveasthetechnicaland
advisorybody.ProvincialanddistrictMMCTaskforces,
undertheleadershipoftheProvincialheadsofhealth,
willbeformedtospearheadandcoordinatethesafe
malecircumcisionroll-outinprovinces.
2. Partnerships:RHRU,Jhpiego,UNAIDS,UNICEF,WHO,
FuturesGroup,CDC/PEPFAR,SFH.
Thepolicywillbeimplementedinpartnershipwith
traditionalleaders;faithbasedorganizations,thepublic
andprivatehealthsectorsandothercivilsocietysectors
thatshouldpromoteMCaspartoftheircomprehensive
HIVpreventionresponse.
3. Advocacy:AdvocacywithdifferentSANACgroups
(men,women).Researchtaskteaminvolvedin
advocacy.
Situation analysis Anationwidesituationalanalysisandareviewofthe
existingMMCresearch&servicesinSouthAfricaarein
progress.Operationallessonscontinuetobelearntfrom
theMMCProjectunderwayinOrangeFarm,asafollow-up
totheOrangeFarmRCT.
Policy & regulatory framework The“MalecircumcisionpolicyforHIVpreventioninSouth
Africa”providestheframeworkforpolicymakersand
implementersofsafemalecircumcisionactivities;inthe
processoffinalization.Prioritizesmale15-49yearsold.
Priorityprovinces:Kwa-ZuluNatal,Mpumlanga,Northern
Cape.MMCtobeprovidedpredominantlyatPHCfacility
inlinewithpolicyofdecentralizationofallpublichealth
services.PolicyalsorespectstraditionalMCandwillprovide
forstrengtheningofqualityoftraditionalMCaspartofpublic
healthinterventiontoreduceadverseevents.
Strategy and operational plan Draftstrategyinplaceandimplementationguidelines
developed.DMPPTdone.Planisthatallprovincesshould
havesufficientcapacityandresourcestoroll-outMMC
accordingtonationalguidelines.Forcepsguidedmethodis
primarymethodforMMC.
TrainingTwotrainingcentresforMMCwhichusetheOrangeFarm
modelhavebeenestablishedinPietermaritzburg(Kwa-
ZuluNatal):EastBoomCommunityHealthCentreandthe
Districthospital.
Quality assurance Routineprogramevaluationshallbeacomponentofmale
circumcisionservicesforqualitycontrolandtoguidethe
planningofservices.
Service delivery National/ProvincialworkshoponMMC,March2010,
includingdevelopmentandimplementingpartners.MMC
guideline&othersupportingdocumentshavebeen
finalized.Kwa-ZuluNatalprovinceistorolloutMMCin11
districts.MpumalangaandNorthernCapeprovincesare
beingassistedtodevelopplans.
Thelinkbetweenthepublicandprivatesectorwillbe
improvedtoprovidequalityservicescollaborativelyand
efficiently.
Servicedeliverystatistics:
MCsthroughApril2010=18,100.
Communication TheSANACcommunicationstechnicaltaskteamhas
developedacommunicationframeworkforMMCthatforms
thebasisforthedevelopmentofanationalcommunication
strategyformalecircumcision.Keymessageshavebeen
developedandpostershavebeenprinted.
Monitoring & evaluationOperationsresearchwillbeconductedtostrengthen
malecircumcisionservicesandtoimplementeffective,
comprehensiveHIVpreventionprogrammesinthecontext
ofsexualandreproductivehealth.
SO
UT
H
AF
RI
CA
9
SwazilandStatistics: • Population:1m
• HIVPrevalence:26%
• MCPrevalence:8%
Leadership, partnerships & advocacy1. Leadership:MOHleadingtheprogramme.National
taskforceincludesallpartnerswhoareworkingon
MC.DeputydirectorclinicalservicesistheMCfocal
personandchairoftheMCtaskforce.AdedicatedMC
coordinatornowinplaceinMOH.
2. Partnerships:Supportingpartners:WHO,UNICEF,
UNAIDS,PEPFAR,FLAS,MCpartnership(PSI,Jhpiego,
MSI,PopulationCouncil).
3. Advocacy:CurrentPrimeMinisterisstrongsupporter
ofMC.
Situation analysis Partsofsituationanalysisdonetoinformpolicy
development.
Policy & regulatory framework FinalizedpolicyonsafemalecircumcisionforHIV
preventionadoptedbycabinet,officiallaunchpending;
postedonmalecircumcisionClearinghousewebsite.
Strategy and operational plan StrategyandImplementationPlanforScalingupSafeMale
CircumcisionforHIVPreventioninSwazilandfinalizedand
printed.PostedonthemalecircumcisionClearinghouse
website.
TrainingTrainingisongoing.Jhpiego/PSIhavedonefivetrainingsin
2010.Atotalof79providers,20doctorsand59nurses
havebeentrained.
Quality assurance In2010WHOandJhpiegoQA/QItoolsmergedandareto
beimplementedinallhealthfacilities.
Service delivery Additionalgovernmentsites(nowtotalsix)identified
toprovideintegratedMCservices.TheMCTaskForce
CoordinatorensurestheworkplansofNGOimplementers
aresharedwiththeMOH.CabinetapprovedMOH
AcceleratedSaturationInitiative.MCservicedeliverymodel
pilotedusingvolunteerphysiciansfromAmericanUrological
Association,April-May2010.Fourvolunteerphysicianswere
placedathealthfacilities.
Servicedeliverystatistics:
MCsdone2006-March2010=9,309.
Communication TheMCProgrammeCoordinatorisincreasingawareness
inothersectorsandhasbegungivingpresentationsto
theMinistryofEducation,faith-basedorganizations,and
privatesectors.FromFebruary2010,amediacampaign
aboutMCoccurredthatincludedweeklynewspaperarticles
andnationalradiospots.HPIfacilitateddialoguewith
parliamentariansonMC.MOHworkedwithbothHouses
ofParliamentwhoadoptedaResolutiontocommitto“the
objective,missionandvisionofMaleCircumcisionforHIV
Prevention”inSwaziland.
Monitoring & evaluationM&Eframeworkisindraftform.
MCtaskforceSub-ResearchCommitteewhichconsists
ofprogrammeplanners,seniorgovernmentofficialsand
higherinstitutionsoflearningwillbeoverseeingongoing
research.
SW
AZ
IL
AN
D

10
TanzaniaStatistics: • Population:40m
• HIVPrevalence:5.7%
• MCPrevalence:70%
Leadership, partnerships & advocacy1. Leadership:MOHleadingtheprogramme.MCTask
ForcewasformedinOctober2007with25members.
MCresponsibilityaddedtoIECHeadwithinNational
AIDSControlProgrammeintheMOH&SW
2. Partnerships:NIMR,WHO,CDC,UNICEF,USAID,
Jhpiego,AssociationofPrivateHospitals.
3. Advocacy:MChasbeenwidelypracticedinregionsfor
traditionalandreligiouspurposes.Thereisnoevidence
ofoppositiontoMC.
Situation analysis Situationanalysishasbeencompleted.Finalreport
available.
Traditionalprovidersstudycompleted.Reportavailable.
Policy & regulatory framework DevelopmentofspecificMCpolicystillbeingdiscussed.
Strategy and operational plan Draftnationalstrategyawaitingfinalapprovalofthe
government.MCincludedinthe5yearnationalmulti-
sectoralHIV/AIDSstrategicframework2008-2012andthe
healthsectorHIV/AIDSstrategy2008-2012.
TrainingAdaptationoftheWHOManualforMaleCircumcisionfor
HIVPreventionunderLocalAnesthesiaandtheTraining
Manual:CounselingforMaleCircumcision;itisbeing
utilizedindemonstrationsites.
Total49MCproviderstrained(additional45tobetrainedin
May2010).
Quality assurance Standardsforservicesprovidingmalecircumcision
underlocalanesthesia,asitestart-upguide,a3-day
facilityorientationandoperationsguidedevelopedfor
demonstrationsites;tobeadaptedforcountryuse.
Service delivery AnadditionaldemonstrationsiteprovidingMCservicesset
up(totalfour).
MOVEgraduallybeingintroducedatthesefoursites.
Servicedeliverystatistics:
MCsdoneOctober2009throughMarch2010=3,148.
Communication Clienteducationmaterials(flipchart,brochure,poster,
flyer)developed;demandcreationmaterialsstillindraft
butwilltargetmen,adolescentsandtheirguardians,
femalepartners.
Monitoring & evaluationM&Etoolsformalecircumcisionhavebeendevelopedfor
demonstrationsites;tobeadaptedforcountryuse.
TA
NZ
AN
IA

11
UgandaStatistics: • Population:32m
• HIVPrevalence:6.4%
• MCPrevalence:25%
Leadership, partnerships & advocacy1. Leadership:NationalTaskForceforMCisinplace.
2. Partnerships:Supportingpartners:WHO,UNAIDS,
UNICEF,UNFPA,PEPFAR(USAIDandCDC),FHIand
MakerereUniversitySchoolofPublicHealth.Multiple
developmentpartnersavailablebutawaitingfirmplans
tobecomeactive.
3. Advocacy:Nolocalchampionsidentified.Thereis
increasingacceptanceforMCforHIVpreventionbut
advocacystillneededwithparliamentmembers.
Situation analysis Situationalanalysistodeterminetheacceptabilityand
feasibilityofmedicalMCpromotioninUgandahasbeen
completedanddisseminated.Mappingsurveyofmedical
MCservicescompleted.
Policy & regulatory framework PolicyapprovedinMarch2010.
Strategy and operational plan Planningforstrategydevelopment.Consultationsongoing
onwhichMCsurgicaltechniquetoadoptandwhichcadres
todosurgery.ResultsofDMPPTunderdiscussiontoinform
targetgroupinstrategy.
TrainingNationwidetrainingnotyetinitiated.Healthworkersfroma
selectednumberoffacilitiesarebeingtrainedattheRakai
HealthSciencesResearchProject.
Quality assurance QAactivitieshavenotyetinitiated.
Service delivery Formalscale-upnotyetstarted.Scaleupexpectedafter
thelaunchofthePolicyin2010.
Militarywillingtoofferservices.
Communication Communicationsstrategyapproved,May2010.MC
awarenesscampaignsongoing.IECmaterialsdeveloped.
Monitoring & evaluationMonitoringandevaluationframeworkhasnotyetbeen
developed.Operationsresearchisongoinginspecificsites.
UG
AN
DA

12
ZambiaStatistics: • Population:12m
• HIVPrevalence:14.3%
• MCPrevalence:13.1%
Leadership, partnerships & advocacy1. Leadership:MOHleadingtheprogramme.National
TaskForceinplace.AdedicatedNationalMC
Coordinatorhasbeenappointed.
2. Partnerships:Supportingpartners:UTH,MC
Partnership(PSI,Jhpiego,MSI,PopulationCouncil)and
CIDRZ.
3. Advocacy:Ongoingadvocacy.HighlevelmeetingJuly
2009.
Situation analysis Situationalanalysisincludingacceptabilityandhealth
facilityreadinessassessmenthasbeencompleted;dueto
beprinted.
Policy & regulatory framework CabinetmemoincorporatingMCinHIVpreventionhasbeen
approved.Theagreementisnottohaveastandalonepolicy
butratherpartofcomprehensiveHIVpolicy.
Lookingattaskshiftingandworkingwithtraditional
providers.
Strategy and operational plan DisseminationofthenationalMCstrategyand
implementationplan2010-2020toalldistrictsinNorth
Western,CopperBeltandEasternProvinces.
DMPPTdatacollectioncompletedanddueforanalysis.
TrainingPartnershipwithJhpiegoandUTHfortraining.
Approximately350providerstrained.
Trainingofprovidersongoing.MCtrainingmanuals
adapted;nationalMOHMCtrainingmanualsfinalised.
Quality assurance QAstrategyinplace.QIteampresentatnationallevel.
WHOQAguideandtoolkittobeimplemented.
MChealthworkercertificationframeworkdevelopedwith
MedicalCouncilofZambia.
Service delivery ServicedeliverysitesadoptingMOVEprinciples
Servicedeliverystatistics:
MCstoJanuary2010=20,779:
Public-10,476
NGO-9,566
Private-737.
Communication Communicationactivitiesbeingimplemented.Media
programmesincorporatingMC;men’shealthkit.
Monitoring & evaluationReportingtoolsandsystemputinplacetoallowMC
implementerstoreporttoMOH.
Provincialanddistrictdisaggregatedannualtargetsmade
andprovidedtoprovincialmedicalofficers
OngoingORthroughuniversityteachinghospital.
ZA
MB
IA

13
ZimbabweStatistics: • Population:12m
• HIVPrevalence:13.6%
• MCPrevalence:10%
Leadership, partnerships & advocacy1. Leadership:MinistryofHealthandChildWelfareis
providingleadershipwithanappointedFocalPerson
leadingtheMCprogramme.MCTaskForcewith
subcommitteesformed.SteeringCommitteeandthree
TechnicalWorkingGroupsareinplace.TheMinistry
continueshavingMCSteeringCommitteemeetings
comprisingofdifferentpartners.FocalpersonforMC
andcondomprogrammingidentifiedintheMOH&CW.
2. Partnerships:Supportingpartners:ZNFPC,WHO,
UNFPA,PSI,churchorganizations.
3. Advocacy:Ongoingsensitizationandinvolvement
oftraditionalcircumcisers,medicalpractitioners,
provincialhealthteamsandcommunitystakeholders.
AonedayworkshopwasconductedinFebruary2010
withProvincialMedicalDirectorstoadvocateforthe
servicedeliverymodelsfortherolloutphaseofmale
circumcision.
Twostakeholdersmeetingswereheldtosensitizethe
keystakeholdersintwoprovinces.
Situation analysis MCsituationanalysisconductedandresultsdisseminated
tostakeholders.
Policy & regulatory framework MCpolicyfinalizedinOctober2009.LaunchedinNovember
2009.
Strategy and operational plan Thecountryisintheprocessofdevelopingamale
circumcision5-yearStrategyandImplementationPlan.The
StrategyisexpectedtobecompletebyJune2010.
TheDMPPTisinprogressandexpectedtobecompletedby
endMay2010.
TrainingNotrainingsundertakeninthisquarter.Establishedcentral
leveltrainingsiteatZNFPCHarare&2othertrainingsites
havebeensetup.NationalTOTwasconductedpreviously
for18nationaltrainersconsistingofsurgeons,nursesand
counselors.Onehundredandfournursesanddoctors
trained.TrainingmaterialshavebeenadaptedfromWHO
trainingguidelines.
Quality assurance DevelopedaqualityassuranceMCcounsellingtoolto
improvethequalityofMCservices.
Service delivery Servicedeliverystatistics:
MCsdonetoMarch2010=4,361.
Communication Developed10billboardstoincreaseawarenessandvisibility
ofMCservices.Developedflyerstargetingyouth,parents
andguardianinanefforttoincreaseawarenessofthe
servicestoyouthandparents.
Monitoring & evaluationEvaluationofthepilotphaseofMCwasconductedandthis
willinformthestrategy.
ZI
MB
AB
WE

14
SECT
ION
TW
OPl
anne
d an
d on
goin
g re
sear
ch o
n m
ale
circ
umci
sion
for H
IV p
reve
ntio
n
16
16
Intr
oduc
tion:
Sincethethreerandomizedcontrolledtrialsdemonstratedreduced
riskoffemale-to-maletransmissionofHIV,avarietyofresearchhas
beenundertakenorisplanned,tocontinuetoinformthescale-up
ofmalecircumcisionservices.Thissectionprovidesasummary
ofresearchrelatedtomalecircumcisionasofJune2010.The
contributionsofallthestudysponsors,investigators,fundersand
reviewersofthisoverviewaregratefullyacknowledged.

17
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Beha
viou
r, kn
owle
dge/
attit
udes
/bel
iefs
Aprospectivestudy
ofbehavioralrisk
compensationrelated
tomalecircumcision
(MC)asanHIV
preventionmethod
KisumuEast,
KisumuWest
andNyando
Districts,
Kenya
UniversityofIllinois
atChicago&Nyanza
ReproductiveHealth
Society(TheBill
andMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Observational
prospectivestudy.
Followupat6,
12,18,and24
monthsafter
circumcision/
enrolment.
Evaluatesexualriskbehaviour1a)changes
insexualriskbehaviourb)sexualfunction
andsatisfactionc)perceptionofHIVrisk;
2)evaluateperceptionsofcircumcisionin
long-termfemalepartnersofcircumcised
participants.
1600Circumcisedand1600
matcheduncircumcisedmales
aged>18years;long-term
femalepartnersofcircumcised
males
Recruitment
completed.Follow-
upongoing
Impactofmale
circumcisiononsexual
riskbehaviours
Kisumu
Municipality,
Kenya
UniversityofIllinois
atChicago&Nyanza
ReproductiveHealth
Society(TheBill
andMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Seriesof3cross-
sectionalrandom-
householdstudies
conductedevery2
years
Changesinperceptions,knowledgeand
beliefsaboutmalecircumcisionandHIV
overtime.HIVandmalecircumcision
prevalencefollowingintroductionofmale
circumcisionservicesingeneralpopulation
overtime.
Menandwomenaged15-49
yrs,1,000maleand1,000female
participantsineachstudycycle
(totaln=6,000)
Baselinesurvey
completed
Prospectivestudy
ofbehavioralrisk
compensationpost
malecircumcision
Zambia
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
Observational
prospectivestudy
atbaseline,6,12
and24months
postenrollment.
Evaluate:a)changesinsexualriskbehavior
overtimeamongmenandwomenb)
changesinageanduseofcondomsat
firstsexc)changesinwomen'sabiltyto
negotiatesafesex.
Randomsampleof1750males
and1650females15-29years;
oversampleofmales15-24years
andfemales15-19yearswillbe
obtainedtoassesschangesin
riskbehavioramongyoungadults
specifically.Qualitativesamples
of30maleandfemalestudy
participants.
RecruitmentJuly/
Aug2010
Evaluationofthetiming
oftheresumptionof
sexualactivitypost-
malecircumcision
Zambia
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
Observational:
Baselineand6
weekspost-male
circumcision
Measuretheprevalenceofunprotected
sexualbehaviorduringthehealingperiod
post-malecircumcision.
225meninterviewedimmediately
priortomalecircumcisionand6
weekspostmalecircumcision;
validationofreportingofsexual
activitywithmaritalpartnersof
maleparticipants
RecruitmentJune/
July2010
Evaluatingmethodsfor
improvingoutcomes
forwomenofmale
circumcisionclients
whoareHIV+or
clientswhorefuseHIV
VCT
Zambia
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
Observational
formative
assessment
Toreducewomen’sHIVriskfromHIV+
menwhohaverecentlyhaveundergone
malecircumcisionby1)assessingand
improvingknowledgeofHIVrisk2)
improvingadherencetosexualabstinence
amongpartnersofmalecircumcisionclients
duringpost-operativehealingperiodand3)
evaluatemethodsforimprovingHIVVCT
amongmalecircumcisionclients.
Malecircumcisionclientsandtheir
sexualpartners
Protocolunder
development

18
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Information,
CircumcisionandHIV
Prevention
70Villagesin
Kuntamanji,
Malawi
UniversityofMichigan
withtheUniversityof
MalawiChancellors
College.
Randomized
controlledtrial
Estimatebehaviouralresponsesto
informationaboutmalecircumcision
protectiveeffectandHIV.
1,200circumcisedand
uncircumcisedmen
Ongoing
Com
mun
icat
ions
Textmessagingto
improveadherence
topostoperative
clinicappointments
andreduceearly
resumptionofsexual
intercourse
KisumuEast,
KisumuWest
andSiaya,
Kenya
Universityof
Washington,Fogarty
throughUniversity
ofIllinoisChicago&
NyanzaReproductive
HealthSociety
Randomized
controlledtrial
Assesstheefficacyoftextmessages
forincreasingadherenceto7daypost
surgicalfollowupvisitandforreducingthe
proportionofmenwhoresumesexbefore
42dayspost-operatively.
Menaged18years+whoget
circumcisedatanyoffourstudy
clinics
Submittedto
Institutional
ReviewBoards
(IRBs)
SMSmessagingto
Improveadherence
topostoperative
clinicappointments
andtoreduceearly
resumptionofsexual
intercourseaftermale
circumcision
Zambia
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
Randomizationto
differentdosesof
SMSmessaging,
includingtosexual
partners
Assesstheefficacyoftextmessagesfor
increasingadherencetothe7daypost-
surgicalfollow-upvisitandforreducingthe
proportionofmenwhoresumesexbefore
42dayspost-op.
Malecircumcisionclientsandtheir
sexualpartners
Protocolunder
development
Communicatingpartial
protectionofmale
circumcision
Kisumu
Eastand
KisumuWest
districts
inNyanza
Province,
Kenya
FamilyHealth
International(TheBill
andMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Phase1:formative
qualitativein-
depthinterviews
Phase2:
qualitative
interviews/focus
groupstotest
andrefineinitial
messages
Phase3:
quantitative
messagetesting
usingpost-test
onlyrandomized
design
1)Insightintomen'sandwomen's
understandingofpartialprotectionof
voluntarymedicalmalecircumcision
2)Messagesthateffectivelycommunicate
partialprotectivenessofvoluntarymedical
malecircumcisionthatcanbeincorporated
intomalecircumcisioncommunication
strategiesinNyanzaProvince,Kenya.
-circumcisedanduncircumcised
menaged18-39years
-womenofreproductiveage
18-39years
Underway,
completion
December2010
19
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Com
mun
ity im
pact
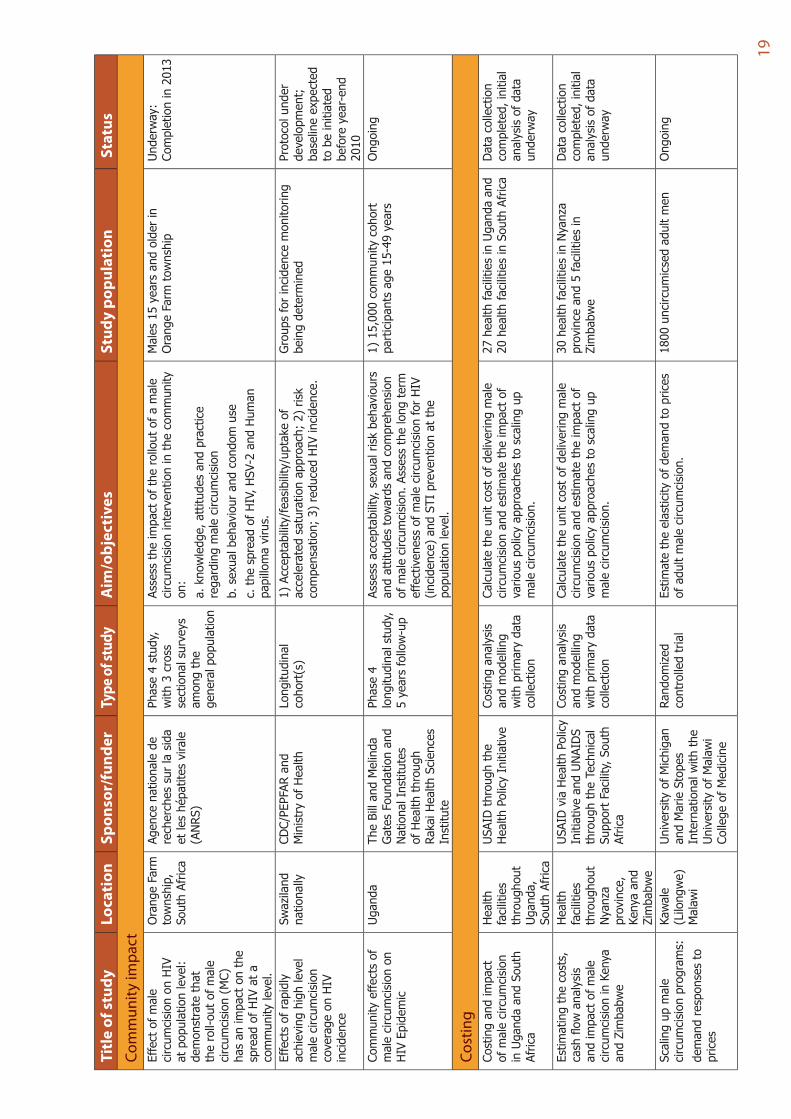
Effectofmale
circumcisiononHIV
atpopulationlevel:
demonstratethat
theroll-outofmale
circumcision(MC)
hasanimpactonthe
spreadofHIVata
communitylevel.
OrangeFarm
township,
SouthAfrica
Agencenationalede
recherchessurlasida
etleshépatitesvirale
(ANRS)
Phase4study,
with3cross
sectionalsurveys
amongthe
generalpopulation
Assesstheimpactoftherolloutofamale
circumcisioninterventioninthecommunity
on:
a.knowledge,attitudesandpractice
regardingmalecircumcision
b.sexualbehaviourandcondomuse
c.thespreadofHIV,HSV-2andHuman
papillomavirus.
Males15yearsandolderin
OrangeFarmtownship
Underway:
Completionin2013
Effectsofrapidly
achievinghighlevel
malecircumcision
coverageonHIV
incidence
Swaziland
nationally
CDC/PEPFARand
MinistryofHealth
Longitudinal
cohort(s)
1)Acceptability/feasibility/uptakeof
acceleratedsaturationapproach;2)risk
compensation;3)reducedHIVincidence.
Groupsforincidencemonitoring
beingdetermined
Protocolunder
development;
baselineexpected
tobeinitiated
beforeyear-end
2010
Communityeffectsof
malecircumcisionon
HIVEpidemic
Uganda
TheBillandMelinda
GatesFoundationand
NationalInstitutes
ofHealththrough
RakaiHealthSciences
Institute
Phase4
longitudinalstudy,
5yearsfollow-up
Assessacceptability,sexualriskbehaviours
andattitudestowardsandcomprehension
ofmalecircumcision.Assessthelongterm
effectivenessofmalecircumcisionforHIV
(incidence)andSTIpreventionatthe
populationlevel.
1)15,000communitycohort
participantsage15-49years
Ongoing
Cost
ing
Costingandimpact
ofmalecircumcision
inUgandaandSouth
Africa
Health
facilities
throughout
Uganda,
SouthAfrica
USAIDthroughthe
HealthPolicyInitiative
Costinganalysis
andmodelling
withprimarydata
collection
Calculatetheunitcostofdeliveringmale
circumcisionandestimatetheimpactof
variouspolicyapproachestoscalingup
malecircumcision.
27healthfacilitiesinUgandaand
20healthfacilitiesinSouthAfrica
Datacollection
completed,initial
analysisofdata
underway
Estimatingthecosts,
cashflowanalysis
andimpactofmale
circumcisioninKenya
andZimbabwe
Health
facilities
throughout
Nyanza
province,
Kenyaand
Zimbabwe
USAIDviaHealthPolicy
InitiativeandUNAIDS
throughtheTechnical
SupportFacility,South
Africa
Costinganalysis
andmodelling
withprimarydata
collection
Calculatetheunitcostofdeliveringmale
circumcisionandestimatetheimpactof
variouspolicyapproachestoscalingup
malecircumcision.
30healthfacilitiesinNyanza
provinceand5facilitiesin
Zimbabwe
Datacollection
completed,initial
analysisofdata
underway
Scalingupmale
circumcisionprograms:
demandresponsesto
prices
Kawale
(Lilongwe)
Malawi
UniversityofMichigan
andMarieStopes
Internationalwiththe
UniversityofMalawi
CollegeofMedicine
Randomized
controlledtrial
Estimatetheelasticityofdemandtoprices
ofadultmalecircumcision.
1800uncircumicsedadultmen
Ongoing

20
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Dev
ices
TheShangRing:A
novelmalecircumcision
deviceforHIV
prevention
HomaBay
District
Hospital,
Kenya
EngenderHealthand
WeillCornellMedical
College;Kenya
NationalAIDSControl
Programmeand
MinistryofHealth.
Non-comparative
pilotstudy
1)Assesssafety&efficacyoftheShang
RingforadultmalecircumcisioninKenyan
mentodetermineifsafeforuseinlarger
studiesinAfrica;2)assessacceptability
amongprovidersandsatisfactionamong
menbeingcircumcised.
40HIV-negativemenaged
18to54yearsseekingmale
circumcision
Completed.
Dataanalysis&
manuscriptwriting
areunderway
TheShangRing:
Evaluationofhealing
atthreetimeintervals
andpotential
forspontaneous
detachment
HomaBay
District
Hospital,
Kenya
Bill&Melinda
GatesFoundation
throughFHIwith
EngenderHealthand
WeillCornellMedical
College,University
TeachingHospital,
Lusaka,Kenya
NationalAIDSControl
Programmeand
MinistryofHealth.
Non-comparative
safetyand
acceptabilitystudy
1)Assesshealingafterremovalofthe
ShangRingatthreedifferenttimepoints,7,
14and21days;2)determinewhetherthe
devicewillspontaneouslydetachifremoval
isdelayedforlongerthanthecurrently
recommendedtimeof7-10days,uptoa
maximumof21days.
50HIV-negativemenaged
18to54yearsseekingmale
circumcision
SubmittedforIRB
review.
Comparisonofthe
ShangRingwith
conventionalsurgical
methods
1)Zambia:
Lusaka,
University
Teaching
Hospital
/Society
forFamily
Health,
2)Kenya:
HomaBay
District
Hospital,
Kenya
Bill&MelindaGates
Foundationthrough
FamilyHealth
Internationalwith
EngenderHealthand
WeillCornellMedical
College;University
TeachingHospital,
Lusaka,Kenya
NationalAIDSControl
Programmeand
MinistryofHealth.
Randomized
controlledtrial
1)Comparethepainandacceptabilityof
theShangRingprocedurewiththeforceps
guidedsurgicalcircumcisiontechnique
(Kenya)andthedorsalslittechnique
(Zambia);
2)comparethesafetyandthecourse
ofwoundhealing,includingthetimeto
completehealing,betweentheShangRing
adultmalecircumcisionprocedureandthe
standardsurgicalcircumcisionprocedures;
3)comparetheeaseoftheShangRing
methodversusstandardcircumcision
surgicalprocedures.
400HIV-negativemenaged
18to54yearsseekingmale
circumcision:200ShangRingand
200standardsurgicalprocedures
SubmittedforIRB
review.
Shangring
Uganda
NationalInstitutesof
Health
Safetyand
acceptability
ToassessShangRingsafetyand
acceptabilitycomparedwithdorsalslit.
250HIV-negativemen,15-49
yearsold
Planned
21
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Form
ativ
e re
sear
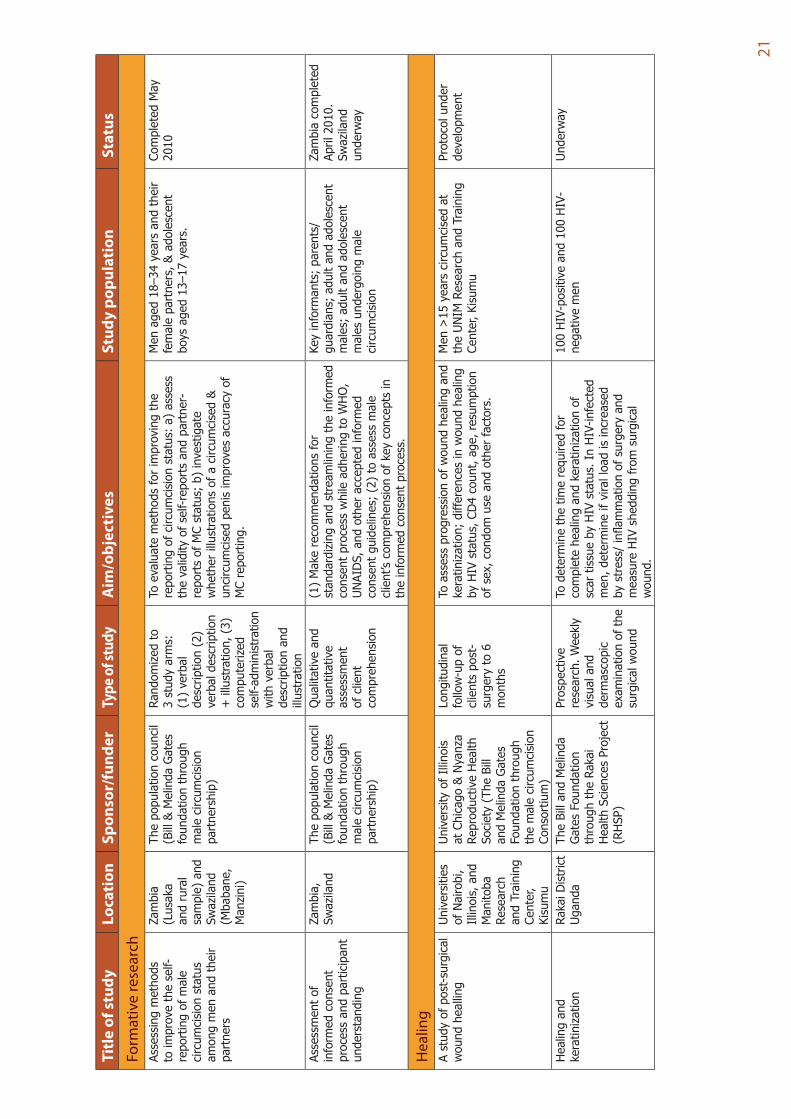
chAssessingmethods
toimprovetheself-
reportingofmale
circumcisionstatus
amongmenandtheir
partners
Zambia
(Lusaka
andrural
sample)and
Swaziland
(Mbabane,
Manzini)
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
Randomizedto
3studyarms:
(1)verbal
description(2)
verbaldescription
+illustration,(3)
computerized
self-administration
withverbal
descriptionand
illustration
Toevaluatemethodsforimprovingthe
reportingofcircumcisionstatus:a)assess
thevalidityofself-reportsandpartner-
reportsofMCstatus;b)investigate
whetherillustrationsofacircumcised&
uncircumcisedpenisimprovesaccuracyof
MCreporting.
Menaged18–34yearsandtheir
femalepartners,&adolescent
boysaged13–17years.
CompletedMay
2010
Assessmentof
informedconsent
processandparticipant
understanding
Zambia,
Swaziland
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
Qualitativeand
quantitative
assessment
ofclient
comprehension
(1)Makerecommendationsfor
standardizingandstreamliningtheinformed
consentprocesswhileadheringtoWHO,
UNAIDS,andotheracceptedinformed
consentguidelines;(2)toassessmale
client’scomprehensionofkeyconceptsin
theinformedconsentprocess.
Keyinformants;parents/
guardians;adultandadolescent
males;adultandadolescent
malesundergoingmale
circumcision
Zambiacompleted
April2010.
Swaziland
underway
Hea
ling
Astudyofpost-surgical
woundhealling
Universities
ofNairobi,
Il linois,and
Manitoba
Research
andTraining
Center,
Kisumu
UniversityofIllinois
atChicago&Nyanza
ReproductiveHealth
Society(TheBill
andMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Longitudinal
follow-upof
clientspost-
surgeryto6
months
Toassessprogressionofwoundhealingand
keratinization;differencesinwoundhealing
byHIVstatus,CD4count,age,resumption
ofsex,condomuseandotherfactors.
Men>15yearscircumcisedat
theUNIMResearchandTraining
Center,Kisumu
Protocolunder
development
Healingand
keratinization
RakaiDistrict
Uganda
TheBillandMelinda
GatesFoundation
throughtheRakai
HealthSciencesProject
(RHSP)
Prospective
research.W
eekly
visualand
dermascopic
examinationofthe
surgicalwound
Todeterminethetimerequiredfor
completehealingandkeratinizationof
scartissuebyHIVstatus.InHIV-infected
men,determineifviralloadisincreased
bystress/inflammationofsurgeryand
measureHIVsheddingfromsurgical
wound.
100HIV-positiveand100HIV-
negativemen
Underway

22
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Hum
an re
sour
ces
Respondingtothe
humanresource
capacitydevelopment
andtrainingneeds
HomaBay,
Rachuonyo,
Rongoand
Nyando
distirctsin
Nyanza,
Kenya
EngenderHealth(The
BillandMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Deskreview;
facility
assessments;in-
depthinterviews
withkey
informants;focus
groupdiscussions
withsexualand
reproductive
healthand
HIVprogram
managers&
healthworkers
1)Determinegapsinhumancapacity
andtrainingneedsrelatedtomale
circumcision;2)identifyhumanresource
andtrainingbarriers/facilitatingfactorsto
introducingmalecircumcisionservices;
3)recommendationsregardingstrategies
toaddresscurrenthumanresourceand
traininggapstosupportmalecircumcision
roll-out.
NotApplicable
Finalizingstudy
report.
Privatesectorhealth
providersassessment
Nyanza
Province,
Kenya
FamilyHealth
International(TheBill
andMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Cross-sectional
study
1)Descriptionandclearunderstanding
ofcostsassociatedwithbringingfacilities
andemployeestominimumstandardsfor
malecircumcisionprovision;2)actualcosts
associatedwithprovidingmalecircumcision
servicesaccordingtoWHOminimum
package;3)recommendationsforstrategies
tointegrateprivatemalecircumcision
serviceprovisionwithMOHservices.
Surveyandobservations
ofprivate-for-profit,non-
governmentalandfaith-based
organizationhealthfacilities
Completed
Assessmentofnon-
physicianclinicians
performingmale
circumcision
HomaBay,
Rachuonyo,
Rongoand
Nyando
distirctsi n
Nyanza,
Kenya
EngenderHealth(The
BillandMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Prospectivestudy
1)Malecircumcisionsurgicalandpost-
operativeproceduresperformedbytrained
non-physiciancliniciansatregularfacilities
workplace;2)malecircumcisionsurgical
outcomesat7-daysand60-dayspost-
surgery;3)patientsatisfactionwithmale
circumcisionservicesprovidedbynon-
physiciancliniciansat7-daysand60-days
post-surgery;
4)costsassociatedwithprovidingmale
circumcisionbynon-clinicianphysicians.
2,530malecircumcision
procedures-malesaged13-54
years
Underway,
completion
September2010
Assessmentoftraining
Uganda
PEPFAR
Observational
study
Processassessmentwithpreandpost
trainingevaluationsandmonitored
surgeries.
Trainees
Ongoing(280
completed)
Assessmentof
physiciansandclinical
officers
Uganda
Centerfor
Communication
Programs/USAID
Observational
study
Safetyandtimerequiredforsurgery.
Men15-49yearsold
Ongoing

23
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Infa
nt m
ale
circ
umci
sion
Infantmale
circumcisionin
Gaborone,Botswana,
andsurroundingareas:
Feasibility,safetyand
acceptability
Gaborone,
Mochudiand
Molepolole,
Botswana
PEPFAR/Centers
forDisease
ControlBotswana-USA
Partnership(BOTUSA)
Prospective
randomizedtrial
oftwomethods
forinfantmale
circumcision.
Ascertain:1)actualuptake/acceptance
ofinfantmalecircumcisionanddetermine
parentalfactorsassociatedwithuptake;
2)feasibility(includingcost)andsafetyof
infantmalecircumcisionusingMogenclamp
versusPlastibell;3)parentalsatisfaction
withtheresultsofcircumcision.
300maleinfants(150ineach
arm)inBotswana
Enrollingwith
approximately190
ofthe300infants
enrolled.
Evaluationofsafe
voluntaryinfant
medicalmale
circumcisioninselected
facilitiesinNyanza
Province,Kenya(The
MtotoMsafiProject)
KisumuEast,
KisumuWest
andSiaya
districts
inNyanza
Province,
Kenya
UniversityofIllinois
atChicago&Nyanza
ReproductiveHealth
Society(TheBill
andMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Casecontrolstudy1)Comparebeliefsandattitudesabout
circumcisionbetweenparentschoosing
infantmalecircumcisionandthose
decliningtheprocedure;2)identify
facilitatorsandbarrierstouptakeofinfant
malecircumcision;3)measureadverse
eventratesassociatedwithinfantmale
circumcision.
Consentingparentsinselected
healthfacilities.Recruiting300
parentsacceptinginfantmale
circumcisionand300parents
declininginfantmalecircumcision
Underway
Evaluationofsafety
andacceptabilityof
neonatalcircumcision
usingGomco,Plastibell,
andMogenmethods
Lusaka,
Zambia
CentersforDisease
Control,Centrefor
InfectiousDisease
ResearchinZambia
andtheUniversity
TeachingHospital
DepartmentofUrology
Prospective
randomizedtrial
TotestthehypothesisthattheGomcoand
Mogenclampsmethodswillbesaferthan
thePlastibellmethodinZambia.
600neonates(450fromthe
UniversityTeachingHospital,
Lusakaand150fromaMatero
referenceclinic)
Underway
Mol
ecul
ar m
icro
biol
ogy,
imm
unol
ogy
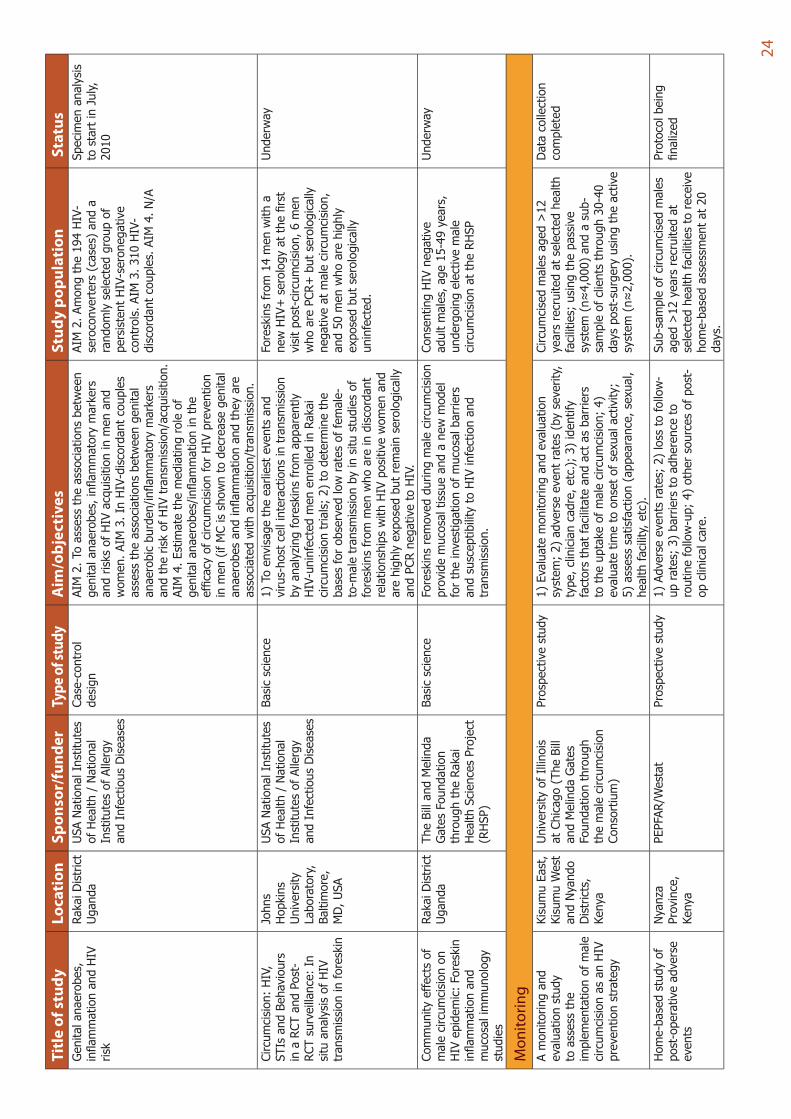
Genitalanaerobes,
inflammationandHIV
risk
RakaiDistrict
Uganda
USANationalInstitutes
ofHealth/National
InstitutesofAllergy
andInfectiousDiseases
Molecular
microbiology,
immunologyand
epidemiologic
observational
study
AIM1.Toassessthecorrelationbetween
theburdenofgenitalanaerobesand
inflammatorymarkersinHIV-uninfected
menandtheirfemalepartners.
100HIV-negativemarriedmenin
theinterventionarmwhoreceived
circumcisionatenrollmentand
100meninthecontrolarmwho
receivedcircumcisiondelayed
for24months,andtheirlinked
femalepartners(n=200)
Specimenanalysis
tostartinJuly,
2010
24
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Genitalanaerobes,
inflammationandHIV
risk
RakaiDistrict
Uganda
USANationalInstitutes
ofHealth/National
InstitutesofAllergy
andInfectiousDiseases
Case-control
design
AIM2.Toassesstheassociationsbetween
genitalanaerobes,inflammatorymarkers
andrisksofHIVacquisitioninmenand
women.AIM3.InHIV-discordantcouples
assesstheassociationsbetweengenital
anaerobicburden/inflammatorymarkers
andtheriskofHIVtransmission/acquisition.
AIM4.Estimatethemediatingroleof
genitalanaerobes/inflammationinthe
efficacyofcircumcisionforHIVprevention
inmen(ifMCisshowntodecreasegenital
anaerobesandinflammationandtheyare
associatedwithacquisition/transmission.
AIM2.Amongthe194HIV-
seroconverters(cases)anda
randomlyselectedgroupof
persistentHIV-seronegative
controls.AIM3.310HIV-
discordantcouples.AIM4.N/A
Specimenanalysis
tostartinJuly,
2010
Circumcision:HIV,
STIsandBehaviours
inaRCTandPost-
RCTsurveillance:In
situanalysisofHIV
transmissioninforeskin
Johns
Hopkins
University
Laboratory,
Baltimore,
MD,USA
USANationalInstitutes
ofHealth/National
InstitutesofAllergy
andInfectiousDiseases
Basicscience
1)Toenvisagetheearliesteventsand
virus-hostcellinteractionsintransmission
byanalyzingforeskinsfromapparently
HIV-uninfectedmenenrolledinRakai
circumcisiontrials;2)todeterminethe
basesforobservedlowratesoffemale-
to-maletransmissionbyinsitustudiesof
foreskinsfrommenwhoareindiscordant
relationshipswithHIVpositivewomenand
arehighlyexposedbutremainserologically
andPCRnegativetoHIV.
Foreskinsfrom14menwitha
newHIV+serologyatthefirst
visitpost-circumcision,6men
whoarePCR+butserologically
negativeatmalecircumcision,
and50menwhoarehighly
exposedbutserologically
uninfected.
Underway
Communityeffectsof
malecircumcisionon
HIVepidemic:Foreskin
inflammationand
mucosalimmunology
studies
RakaiDistrict
Uganda
TheBillandMelinda
GatesFoundation
throughtheRakai
HealthSciencesProject
(RHSP)
Basicscience
Foreskinsremovedduringmalecircumcision
providemucosaltissueandanewmodel
fortheinvestigationofmucosalbarriers
andsusceptibilitytoHIVinfectionand
transmission.
ConsentingHIVnegative
adultmales,age15-49years,
undergoingelectivemale
circumcisionattheRHSP
Underway
Mon
itorin
g Amonitoringand
evaluationstudy
toassessthe
implementationofmale
circumcisionasanHIV
preventionstrategy
KisumuEast,
KisumuWest
andNyando
Districts,
Kenya
UniversityofIllinois
atChicago(TheBill
andMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Prospectivestudy
1)Evaluatemonitoringandevaluation
system;2)adverseeventrates(byseverity,
type,cliniciancadre,etc.);3)identify
factorsthatfacilitateandactasbarriers
totheuptakeofmalecircumcision;4)
evaluatetimetoonsetofsexualactivity;
5)assesssatisfaction(appearance,sexual,
healthfacility,etc).
Circumcisedmalesaged>12
yearsrecruitedatselectedhealth
facilities;usingthepassive
system(n≈4,000)andasub-
sampleofclientsthrough30-40
dayspost-surgeryusingtheactive
system(n≈2,000).
Datacollection
completed
Home-basedstudyof
post-operativeadverse
events
Nyanza
Province,
Kenya
PEPFAR/Westat
Prospectivestudy
1)Adverseeventsrates;2)losstofollow-
uprates;3)barrierstoadherenceto
routinefollow-up;4)othersourcesofpost-
opclinicalcare.
Sub-sampleofcircumcisedmales
aged>12yearsrecruitedat
selectedhealthfacilitiestoreceive
home-basedassessmentat20
days.
Protocolbeing
finalized
25
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Serv
ice
deliv
ery
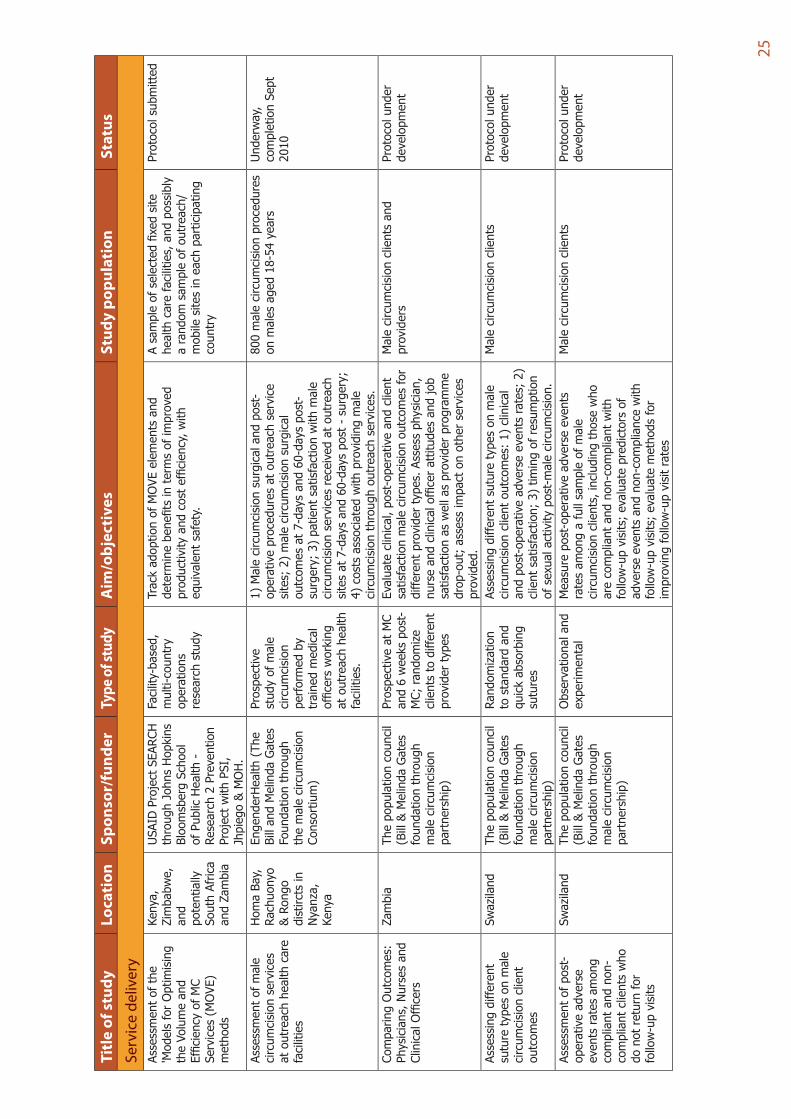
Assessmentofthe
'ModelsforOptimising
theVolumeand
EfficiencyofMC
Services(MOVE)
methods
Kenya,
Zimbabwe,
and
potentially
SouthAfrica
andZambia
USAIDProjectSEARCH
throughJohnsHopkins
BloomsbergSchool
ofPublicHealth-
Research2Prevention
ProjectwithPSI,
Jhpiego&MOH.
Facility-based,
multi-country
operations
researchstudy
TrackadoptionofMOVEelementsand
determinebenefitsintermsofimproved
productivityandcostefficiency,with
equivalentsafety.
Asampleofselectedfixedsite
healthcarefacilities,andpossibly
arandomsampleofoutreach/
mobilesitesineachparticipating
country
Protocolsubmitted
Assessmentofmale
circumcisionservices
atoutreachhealthcare
facilities
HomaBay,
Rachuonyo
&Rongo
distirctsin
Nyanza,
Kenya
EngenderHealth(The
BillandMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Prospective
studyofmale
circumcision
performedby
trainedmedical
officersworking
atoutreachhealth
facilities.
1)Malecircumcisionsurgicalandpost-
operativeproceduresatoutreachservice
sites;2)malecircumcisionsurgical
outcomesat7-daysand60-dayspost-
surgery;3)patientsatisfactionwithmale
circumcisionservicesreceivedatoutreach
sitesat7-daysand60-dayspost-surgery;
4)costsassociatedwithprovidingmale
circumcisionthroughoutreachservices.
800malecircumcisionprocedures
onmalesaged18-54years
Underway,
completionSept
2010
ComparingOutcomes:
Physicians,Nursesand
ClinicalOfficers
Zambia
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
ProspectiveatMC
and6weekspost-
MC;randomize
clientstodifferent
providertypes
Evaluateclinical,post-operativeandclient
satisfactionmalecircumcisionoutcomesfor
differentprovidertypes.Assessphysician,
nurseandclinicalofficerattitudesandjob
satisfactionaswellasproviderprogramme
drop-out;assessimpactonotherservices
provided.
Malecircumcisionclientsand
providers
Protocolunder
development
Assessingdifferent
suturetypesonmale
circumcisionclient
outcomes
Swaziland
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
Randomization
tostandardand
quickabsorbing
sutures
Assessingdifferentsuturetypesonmale
circumcisionclientoutcomes:1)clinical
andpost-operativeadverseeventsrates;2)
clientsatisfaction;3)timingofresumption
ofsexualactivitypost-malecircumcision.
Malecircumcisionclients
Protocolunder
development
Assessmentofpost-
operativeadverse
eventsratesamong
compliantandnon-
compliantclientswho
donotreturnfor
follow-upvisits
Swaziland
Thepopulationcouncil
(Bill&MelindaGates
foundationthrough
malecircumcision
partnership)
Observationaland
experimental
Measurepost-operativeadverseevents
ratesamongafullsampleofmale
circumcisionclients,includingthosewho
arecompliantandnon-compliantwith
follow-upvisits;evaluatepredictorsof
adverseeventsandnon-compliancewith
follow-upvisits;evaluatemethodsfor
improvingf ollow-upvisitrates
Malecircumcisionclients
Protocolunder
development

26
Titl
e of
stu
dyLo
cati
onSp
onso
r/fu
nder
Type
of s
tudy
Aim
/obj
ecti
ves
Stud
y po
pula
tion
Sta
tus
Sexu
ally
tran
smitt
ed in
fect
ions
and
repr
oduc
tive
trac
t inf
ectio
nsHIVandSTIIncidence
Kisumu,
Kenya
UniversityofIllinois-
ChicagoandNyanza
ReproductiveHealth
Society(TheBill
andMelindaGates
Foundationthrough
themalecircumcision
Consortium)
Cohortstudy,
post-RCT
EstimatethedifferencesinHIVandother
STIincidencebetweencircumcisedand
uncircumcisedmen.
Menages18-34years
Continuingfollow-
up
Malecircumcision:HIV,
STIsandbehaviorsin
aRCTandpost-RCT
Surveillance;Human
papillomavirus(HPV)
testing
RakaiDistrict
Uganda
andJohns
Hopkins
University
Laboratory,
Baltimore,
MD,USA
USANationalInstitutes
ofHealth/National
InstitutesofAllergy
andInfectiousDiseases
Randomized
clinicaltrialwith6,
12and24month
followupvisits.
1)Assesstheefficacyofmalecircumcision
forhighriskHPVpreventionandto
determinetheprevalence,incidenceand
clearanceofHPV;2)assesstheefficacy
ofcircumcisionforreductionofgenital
highrisk-HPVinfectionsinfemalepartners
ofHIV-infectedanduninfectedmaletrial
participantsbycomparingHPVprevalence
andincidenceinfemalepartnersof
circumcisedanduncircumcisedmarried
men.
Samplesfrom609HIV-negative
and530HIV-positivemen,and
femalepartners
Underway
Circumcision:HIV,
STIsandbehaviorsin
aRCTandpost-RCT
Surveillance
RakaiDistrict
Uganda
USANationalInstitutes
ofHealth/National
InstitutesofAllergy
andInfectiousDiseases
PhaseI V,post-
trialsurveillance
studyofmale
circumcision
effectiveness
1)ConductSTIassaysonstoredsamples
todeterminetheefficacyofcircumcision
inpreventingselectedSTIs;2)assessthe
long-termeffectivenessofcircumcisionfor
HIV/STIprevention,andeffectsonsexual
riskbehaviors,byconductinganadditional
5yearsofannualfollowupamongmen
whohadenrolledintheNIHtrial.
5,000menaged15-49years
originallyenrolledinthemale
circumcisiontrial.
Underway