Program of Medicine Studies MODULE SENSATION AND PERCEPTION modul… · · 2012-11-30Program of...
45
EUROPOS SĄJUNGA Europos Socialinis Fondas Program of Medicine Studies MODULE SENSATION AND PERCEPTION Third Year Fifth Semester Faculty of Medicine Kaunas University of Medicine
Transcript of Program of Medicine Studies MODULE SENSATION AND PERCEPTION modul… · · 2012-11-30Program of...

EUROPOS SĄJUNGAEuropos Socialinis Fondas
Program of Medicine Studies
MODULE
SENSATION AND PERCEPTION
Third YearFifth Semester
Faculty of MedicineKaunas University of Medicine

Contents
1. General information .................................................................................................... 4 2. General content of the module ................................................................................... 4 3. Aim and objectives of the module .............................................................................. 4 4. Tutorials ........................................................................................................................ 6
4.1. Case 1. Strange senses (Mr. Ache) ...................................................................... 6 4.2. Case 2. Unobservant basketball player (Mr. Overlook Junior) ........................... 7 4.3. Case 3. Dizziness attacks (Mr. Vertigo) ............................................................. 9 4.4. Case 4. A drowsy librarian (Miss Slumber) ...................................................... 11 4.5. Case 5. Transposed words (Mr. Silent) ............................................................ 13 4.6. Case 6. A forgotten car (Mr. Scatterbrain) ........................................................ 14
5. Lectures ....................................................................................................................... 17 5.1. Histology of sensory receptors ......................................................................... 17 5.2. Anatomy of the general and chemical senses: receptors, pathways and centers
........................................................................................................................... 17 5.3. Physiology and pathophysiology of the somatosensory system and
chemoreception .................................................................................................. 17 5.4. Opioid and nonopioid (antipyretic) analgesics. Local anesthetics .................... 17 5.5. Local anesthesia ................................................................................................ 17 5.6. Anatomy of vision: structure of the eye, visual pathways and location of
centers ................................................................................................................ 18 5.7. The structure of the organ of vision. Retinal histology .................................... 18 5.8. Physiology and pathology of the visual system ................................................ 18 5.9. Processing of the sensory information in the structures of the visual cortex .... 18 5.10. Sense of hearing and balance: structure of the ear, auditory and vestibular
pathways and centers. Relation of vestibular organ and cerebellum ................. 18 5.11. Histology of the auditory and vestibular organ .............................................. 19 5.12. Physiology and pathological physiology of the hearing and equilibrium
systems ............................................................................................................... 19 5.13. Reticular formation of the brain stem ............................................................. 19 5.14. Sleep and wakefulness .................................................................................... 19 5.15. Neurotransmitters and their metabolism ......................................................... 19 5.16. Hypnotic and general anesthesia inducing drugs. Antiepileptic drugs ........... 19 5.17. Morphofunctional organization of the telencephalon and cerebrovascular
system ............................................................................................................... 20 5.18. Architectonics of the cerebral cortex. Structural module of the cerebral cortex
........................................................................................................................... 20 5.19. Physiological basis of the language function .................................................. 20 5.20. Brain stroke. Tumors of the nervous system and coverings ........................... 20 5.21. Anatomy of the limbic system ........................................................................ 20 5.22. Learning and memory. Emotions and behavior .............................................. 20 5.23. Pathogenetic importance of reactive nitrogen and oxygen species ................ 21 5.24. Psychostimulants. Antidepressants. Anxiolytics. Antipsychotic drugs.
Medicines improving memory ........................................................................... 21 6. Practicals .................................................................................................................... 22
6.1. Sensation of touch and esthesiometry. Smell and taste ..................................... 22 6.2. Drug used in pain: opioid analgesics and antipyretics. Local anesthetics ......... 22 6.3. Types of local anesthesia. Techniques and complications ................................ 23
2

6.4. Anatomy of the eyeball and accessory structures ............................................. 23 6.5. Histology of organ of vision. The structure of the retina ................................. 23 6.6. Accommodation, visual acuity and peripheral vision. Binocular vision and
illusions ............................................................................................................. 24 6.7. Anatomy of the temporal bone and external, middle and internal ear. Relation
of vestibular organ and cerebellum .................................................................... 24 6.8. Vestibular and auditory organ. The internal ear. The spiral organ of Corti ...... 25 6.9. Tonal liminal audiometry. Kinetosis ................................................................ 25 6.10. Electroencephalogram (EEG) and evoked potentials ..................................... 26 6.11. Drugs inducing sleep and general anesthesia. Antiepileptic drugs ................. 26 6.12. Morphofunctional organization of the telencephalon and cerebrovascular
system ................................................................................................................ 27 6.13. Architectonics of the cerebral cortex and its structural modulus .................... 27 6.14. Brain stroke. Tumors of the nervous system and coverings ........................... 28 6.15. Psychostimulants. Antidepressants. Anxiolytics. Antipsychotic drugs.
Medicines improving memory ........................................................................... 29 7. Seminars ...................................................................................................................... 30
7.1. Molecular mechanisms of light signal transduction .......................................... 30 7.2. Significance and anatomical peculiarities of the reticular formation ................ 30
8. Module examination program ................................................................................. 31 8.1. Biology .............................................................................................................. 31 8.2. Anatomy ............................................................................................................ 31 8.3. Histology ........................................................................................................... 31 8.4. Physiology and pathophysiology ...................................................................... 31 8.5. Biochemistry .................................................................................................... 32 8.6. Pharmacology .................................................................................................... 32 8.7. General surgery ................................................................................................ 33 8.8. Pathological anatomy ........................................................................................ 33
9. Appendix ..................................................................................................................... 34 9.1. Sensation of touch ............................................................................................. 34 9.2. Sensation of taste ............................................................................................... 35 9.3. Accommodation and the visual acuity .............................................................. 36 9.4. Visual field ....................................................................................................... 38 9.5. Tonal liminal audiometry .................................................................................. 40 9.6. Kinetosis ............................................................................................................ 42 9.7. Electroencephalogram (EEG) ............................................................................ 44
3

1. General information
Supervisor of the module: Assoc. Prof. Rimvydas Miliauskas, Department of Physiology Coordinator of the module: Lector Alė Laukevičienė, Department of Physiology
Departments: 1.Institute of Biology2.Institute of Anatomy3.Department of Histology and Embryology 4.Department of Physiology 5.Department of Biochemistry6.Department of Basic and Clinical Pharmacology7.Clinic of General Surgery8.Clinic of Pathological Anatomy
Subjects:1. Biology 2. Human anatomy 3. Human histology and embryology 4. Physiology 5. Pathophysiology 6. Biochemistry 7. Pharmacology 8. General surgery 9. Pathological anatomy
2. General content of the moduleBy analyzing the problems of this module students gain new knowledge and apply it to the following domains:
• Structure and function of the sensory nervous system;• Some basic knowledge of the neurological examination;• Symptoms and syndromes of the nervous system disorders;• Topographic basis of the syndromes;• Neuroanatomy and neurochemistry of neuronal circuits of the higher functions
of the central nervous system; • Higher functions of the nervous system (emotions, behavior, sleep and
wakefulness, learning and memory) and their disorders; • Organization of the CNS associated with the higher functions of the brain; • Pharmacological basis of treatment of neurological disorders of the CNS.
3. Aim and objectives of the moduleAfter having studied this module students should know how to define, analyze, explain and relate phenomena in the cases analyzed in the module. By attaining this aim, students should gain knowledge about the system structure, function,
4

mechanisms of disorders and principles of their examination and treatment:
• Hierarchical structure of the nervous system; • Organization of the nervous system at different levels; • Phenomena associated with excitation of the nervous system, impairment of its
functions, release from the higher control; • General functions of the nerve cells and their response to the lesions; • Phenomena of excitation and inhibition in the CNS; • Cerebral circulation and the blood-brain barrier; • Elementary knowledge about the tumors of the CNS; • Localization of the higher functions and the dominance of the cerebral
hemispheres; • Topographical and functional anatomy of the brain: frontal lobes, the limbic
system and memory circuits; • Characteristics of the higher functions of the CNS: emotions, behavior,
memory, consciousness, cognitive functions and their disorders (apraxias and agnosias);
• Neurotransmitters of the CNS and their receptors: dopamine, noradrenalin, serotonin, GABA etc.;
• Main classes of psychotropic substances (antidepressants, antipsychotic and anxiolytic agents) and substances producing addiction.
5

4. Tutorials
4.1. Case 1. Strange senses (Mr. Ache)
Mr. Ache is 60 years old. He arrived to the doctor since he feels a strong pain appearing irregularly during the last several weeks. The pain starts from the neck and spreads to the left shoulder and further down to the thumb. In addition, the patient noted that he has a difficulty in estimating the position of the left leg. Therefore he stumbled across the border of the sidewalk and fell down several times. When answering to the doctor’s questions he recalled that it became more difficult for him to evaluate water temperature in the bathtub with the right hand than with the left one. Moreover, he noted some weakness of the left arm.
Examination of the sensibility showed a hypoesthesia and dysesthesia on the left side of the body in the region of dermatome C5. In addition, there was a decrease of the touch sensitivity in the left arm and anterior and radial side of the forearm, the left side of the trunk and the left leg. The patient makes errors when the doctor asks him to tell the position of the toes of the left foot with the eyes closed. The ability to appreciate vibrations applied to the left ankle is less in comparison with the vibrations applied to the right ankle. On the contrary, the senses of temperature and pain are normal on the left side, but they are reduced on the right side, except the shoulder and the face where they are normal.
Where do you expect the lesion to be located?
Concept of the problem: structural and functional organization of the somatosensory systemClinical symptoms: disorder and dissociation of senses
Aim To know and understand the general organization of the sensory system, the modality, the general structure of receptors, the receptor potential, the receptors for touch, vibration, temperature and pain, the organization of the sensory pathways, the action of analgesics; the chemical senses.
Learning objectives and contents
To complete the analysis of this problem the students should know:
• Histology of sensory receptorsSubject: HistologyDepartment of HistologyReferences: Junqueira L.C., Carneiro J.. Basic Histology. Text & Atlas. 11th ed.
McGraw-Hill. 2005. p. 27-29, 42-47, 71, 158-160.
• General structure of organization of the somatosensory system.• Pathways of the somatosensory system.• Structure of the olfactory and taste organs.• Pathways of the olfactory and gustatory systems.
Subject: Human anatomy Institute of Anatomy References:
6

Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh, Kahle W., Frotscher M. Nervous system and sensory organs. Thieme. Stuttgart-New York, 2003, p. 312-331, 228.
• Physiology of the somatosensory system and chemoreception• Tactile (touch) senses, taste and smell senses• Pain • Disorders of the senses Subjects: Physiology and pathophysiology Department of Physiology
References:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch.7 (p. 138-147), Ch. 10 (p. 185-191).Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia:
Elsevier Saunders; 2006, Ch. 46 (p. 573-577), Ch. 47 (p. 585-597), Ch. 48 (p. 598-609).
• Drug used for pain control (opioid analgesics and antipyretics, local anesthetics).Subject: PharmacologyDepartment of Basic and Clinical PharmacologyReferences:Katzung B.G. Basic and Clinical Pharmacology. Appleton and Lange, 1998, p.
425-434, 496-516, 578-588.Supplementary readings:Howland R. D., Mycek M. J. Lippincotts Illustrated Review: Pharmacology. 3rd
Ed. Lippincott Williams and Wilkins. Philadelphia, 2006, p. 157-169, 495-515.
• Ways and methods of anesthesia. • Local anesthesia, development, indications and contraindications. • Local anesthetics, clinical features, dosage.
Subject: General surgeryClinic of General surgeryReferences:Oxford handbook of anaesthesia. 2nd ed. Ed. KG. Allman. Oxford Medical
Publications, 2006.
4.2. Case 2. Unobservant basketball player (Mr. Overlook Junior)Mr. Overlook Junior is a secondary school graduate. He is a tall (195 cm.) and still growing youngster. He desires to become a good basketball player and attends the training sessions regularly. His coach reproached him recently for overlooking the balls passed him from the sides, and bumping against the neighboring players. Then Junior told that he often suffered from headaches. Then the coach suggested going to a doctor.
After asking about his complaints and examining him carefully, the family doctor decided to send him to an ophthalmologist and neurologist. The ophthalmologist found certain changes in the visual fields of both eyes. The neurologist suggested taking CT scan of the head. The CT scan showed changes in the region of the Turkish saddle (sella turcica).
7

What could be the reason for such clinical symptoms?How can you explain the complaints in the light of the results of investigations?
Concept of the problem: structural and functional organization of the retina, optic nerves, tracts and visual cortex.
Clinical symptoms: changes in the visual fields
Aim
To know and understand the role of the structures of the eye for the visual function, the functional connections of the cells in the retina, the receptive fields of the ganglion cells, the visual pathways, projections to subcortical and cortical structures, the feature extraction of the object, the principles of the color vision and the control of the eye movements.
Learning objectives and contents
To complete the analysis of this problem the students should know:
• Structure of the eyeball.• The central visual pathway.• Accessory visual structures.• Innervation of the eye.• Vascular supply of the eye.
Subject: Human anatomy Institute of Anatomy References: Drake R. l., Vogl W., Mitchell A. W. M. Gray's anatomy for students. Elsevier.
Philadelphia, 2005, 830-853. Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, p. 155-159, 103-105.Kahle W., Frotscher M., Nervous system and sensory organs. Thieme. Stuttgart-
New York, 2003, p. 338-359.Supplementary readings:Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley &
Belfus. Philadelphia, 2004, plates 89 - 91, 94 - 104.Moses K. P., Banks J. C., Nava P. B., Petersen D., Atlas of clinical gross anatomy.
Elsevier, 2005, p. 58-71.
• Histology of organ of vision.• The structure of the retina.• Ultrastructure of visual cells.
Subject: HistologyDepartment of HistologyJunqueira L.C., Carneiro J. Basic Histology. Text &Atlas. 11th ed. McGraw-Hill.
Medical Publishing Division, 2005, p. 456-468Sadler T.W. Langman’s Medical Embryology. 10th edition. Lippincott Williams
&Wilkins, 2006, p. 325-333.Supplementary readings:Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley &
Belfus. Philadelphia, 2004, plates 92, 93.
8

• Molecular mechanism of light signal transduction.Subject – BiochemistryDepartment of BiochemistryReferences Berg J.M., Tymoczko J.L., Stryer L. Biochemistry. 5th ed. W.H. Freeman, New
York, 2002, p.903-913.Cox D.N., Nelson M.M.. Lehninger Principles of Biochemistry. 3rd ed., Worth
Publishers, New York, 2000, p.458-462.
• The optical system of the eye, optical defects and their corrections. Accommodation. Papillary reflex.
• Signal transduction in the retina. Receptive fields. Visual acuity.• Adaptation. Color vision.• Visual fields. Visual pathways and their lesions.• Functional organization of the visual cortex. Binocular vision.• Movements of the eye.
Subjects: Physiology and pathophysiology Department of PhysiologyReferences:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch.8 (p. 148-170).Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia:
Elsevier Saunders; 2006, Ch. 49 (p. 613-625), Ch. 50 (p. 626-639), Ch. 51 (p. 640-650).
• Processing of sensory information in the visual cortex. Subject – BiologyInstitute of BiologyReferences http://webvision.med.utah.edu/VisualCortex.htmlhttp://hubel.med.harvard.edu/b23.htmhttp://www.physpharm.fmd.uwo.ca/undergrad/sensesweb/
4.3. Case 3. Dizziness attacks (Mr. Vertigo)
Mr. Vertigo, now 48 years old, has always felt fine. However, last autumn he noted sudden decreasing hearing at the left ear. After several hours the hearing impairment disappeared. This spring he had the first dizziness attack with the nausea and vomiting. During the attack, hearing impairment on the left ear repeated again. After eight hours the dizziness and decreased hearing passed away. Later on, similar attacks with dizziness and hearing loss repeated many times. The patient is anxious about hearing impairment and especially about dizziness, which makes him invalid and gives troubles in social communication. The patient does not dare to leave his house, since he is afraid of dizziness and vomiting in public. Some days ago he had a new attack and decided to go to the hospital immediately.
When he arrived, the attack still continued. The doctor noted that the patient drifted to the left when going. He also noted the rightward horizontal nystagmus. Vestibular tests showed the deficiency of function on the left side. Rinne (F. H. Rinne) and Weber (E. H. Weber) tests showed a decrease in hearing at the left ear. The potentials
9

evoked by the suprathreshold sound level were equal on both sides. The attack lasted for several hours. At the end of the attack the leftward drift disappeared, the tests of vestibular function and hearing thresholds became normal.
How can you explain these temporary disorders of equilibrium and hearing?
Concept of the problem: structural and functional organization of the hearing and equilibrium systemsClinical symptoms: vertigo and impairment of hearing
Aim
To know and understand the structure of the external, middle and inner ear, the general mechanisms of the signal transduction in the inner ear and the two different sensory functions of the inner ear: the sense of hearing and the sense of equilibrium.
Learning objectives and contents
To complete the analysis of this problem the students should know:• Structure of the temporal bone and external, middle and inner ear.• Auditory pathway.• Vestibular pathways and their connections with the cerebellum.• Innervation of the ear.• Vascular supply of the ear.
Subject: Human anatomy Institute of Anatomy References: Drake R. l., Vogl W., Mitchell A. W. M. Gray's anatomy for students. Elsevier.
Philadelphia, 2005, 854-871. Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, p. 109-111, 115-121.Kahle W., Frotscher M., Nervous system and sensory organs. Thieme. Stuttgart-
New York, 2003, p. 362-383.Supplementary readings:Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley &
Belfus. Philadelphia, 2004, plates 63 - 68, 73 - 74, 77.Moses K. P., Banks J. C., Nava P. B., Petersen D. Atlas of clinical gross anatomy.
Elsevier, 2005, p. 72-81.
• Histology of the vestibular auditory organ. The structure of crista ampullaris and maculae. The structure of cochlear duct, the structure of organ of Corti.
• Formation of the auditory and vestibular organ.Subject: histology and embryology Department of Histology and EmbryologyReferences:Junqueira L.C., Carneiro J.. Basic Histology. Text &Atlas.11 th edition. McGraw-
Hill. Medical Publishing Division. 469-474.Sadler T.W. Langman’s medical Embryology. 10th edition. Lippincott Williams
& Wilkins, 2006, p.317-324.Supplementary readings:Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley &
Belfus. Philadelphia, 2004, plates 69 - 72, 75 - 76.
• The directional sensitivity of the hair cells of the vestibular organ.
10

• The detection of the head position, linear and angular acceleration.• Vestibulo-spinal and vestibulo-ocular reflexes. Nystagmus. Motion sickness
(kinetosis). • Transmission of the sound signal to the inner ear. Transduction of the signal in the
Corti organ.• Encoding of the sound frequency and intensity. The range of the audible
frequencies.• Organization of the central auditory pathways. Binaural hearing.Subjects: Physiology and pathophysiology Department of Physiology
References:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch. 9 (p. 171-184).Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia:
Elsevier Saunders; 2006. Ch. 52 (p. 651-662), Ch. 55 (p. 692-697).
4.4. Case 4. A drowsy librarian (Miss Slumber)
Miss Slumber is a 25-year old librarian. She came to the doctor, since she was frightened of falling asleep when she was driving to work at 10 o’clock in the morning despite she had good sleep last night. She was anxious about increasing sleepiness progressively during the last three years. Her sleep rhythm is regular: she goes to bed at 22:30 and gets up at 7:00. She does not use any sedatives or alcohol. She does not complain about her night sleep. She does not snore and has no sense of restless legs. She has refreshing night sleep and gets up easily in the morning. However, she feels sleepy during the day and has to take a nap for 2-3 hours. Sometimes she feels an irresistible sleepiness and can fall asleep anywhere.
In addition, she noted that when she falls asleep she has hallucinations (visual, auditory, or somatesthetic). On waking up or falling asleep, she sometimes feels herself totally paralyzed for a few seconds. She also noted during the last year that she feels weakness in her knees during strong emotions, e.g. when she bursts out laughing. However, she does not lose consciousness and does not have any convulsions. During the interview it became clear that her mother and a cousin on the maternal side also have complaints about strong somnolence during the daytime.
Neurological examination did not show any pathologic symptoms. However, polygraphic recording of her night sleep showed that the first state of sleep she enters when she falls asleep is the REM sleep. The following sleep structure was normal. Another investigation performed five times per day every two hours showed that the patient goes directly from waking into a REM phase of sleep. The mean latency time was 4.5 minutes.
How can you explain such kind of sleepiness and how to treat the patient?
Concept of the problem: sleep phases, stages and cycles.Clinical symptoms: a peculiar case of sleep-wakefulness sequence disorder.
Aim
To study and understand the generation of summated electrical activity of the brain, the electroencephalogram (EEG); to analyze the main kinds of brain waves and to relate their changes with the functional state of the brain; to distinguish different
11

phases and stages of sleep on the basis of changes in the EEG and other physiological variables; to investigate some disorders of cyclical sequence of sleep and wakefulness.
Learning objectives and contents
To complete the analysis of this problem the students should know:• Principal structure, localization and importance of the reticular formation.• Nuclei of the reticular formation and features of their neurons.
Subject: human anatomyInstitute of AnatomyReferences:Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, p. 87-99, 123-128.Kahle W., Frotscher M., Nervous system and sensory organs. Thieme. Stuttgart-
New York, 2003, p. 146-149.Supplementary readings:Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley &
Belfus. Philadelphia, 2004, plates 22-23, 29, 130-135, 142-144.
• The generation of summated electrical activity of the brain, the electroencephalogram (EEG) and evoked potentials.
• The main waves of the human EEG, their changes and relations to the general state of the brain. Some pathological changes in the EEG, e.g. during the epileptic seizure.
• The differentiation of sleep phases and stages according to changes in the EEG, electromyogram (EMG) and electrooculogram (EOG). Changes in functioning of other organs and systems during the sleep.
• Circadian rhythm and sleep cycles. Certain disorders of alternation of sleeping and waking. Explanation of sleep mechanisms.
Subjects: Physiology and pathophysiology Department of Physiology
References:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch. 11 (p. 192-201).Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia:
Elsevier Saunders; 2006. Ch. 59 (p. 739-745).
• Synthesis, inactivation and action mechanisms of neurotransmitters.Subject – Biochemistry Department of BiochemistryReferences: Smith C., Marks A.D., Lieberman M. Mark’s Basic Medical Biochemistry. A
Clinical Approach. 2nd ed., Lippincott Williams&Wilkins, Philadelphia. 2005, p.886-899.
• Drugs inducing sleep and general anesthesia. Antiepileptic drugs.Subject – pharmacologyDepartment of Basic and Clinical PharmacologyReferences:
12

Katzung B.G. Basic and Clinical Pharmacology. Appleton and Lange, 1998, p. 354-372, 386-409, 409-425.
Supplementary readings: Howland R.D., Mycek M.J. Lippincotts Illustrated Review: Pharmacology. 3rd
Ed. Lippincott Williams and Wilkins. Philadelphia, 2006, p. 103-115, 125-139, 169-180.
4.5. Case 5. Transposed words (Mr. Silent)
Mr. Silent is 45-years old office employee. He came to the doctor at the request of his wife. She has noted that he became a completely different man during last several months. He became apathetic and inactive. He spends most of his time watching television. He is indifferent to and cannot concentrate on anything. His colleagues noted his slowing behavior. He often forgets the meetings and cannot concentrate on planning and organizing his work. He became emotionally distant from his friends and family, and sometimes is irritable. The doctor decided to treat his condition with antidepressant drugs.
Despite four month’s treatment his conditions did not improve. Moreover, the patient recently noted that he dropped the things he kept in his right hand. During examination the doctor found a slight amimia and some strange behavior. The patient was well oriented but confused the chronology of the past events. His linguistic expression was unimpaired, but the articulation was difficult and unclear. He could hardly choose correct consonants. He spoke slowly and had difficulties in finding correct words. He sometimes used one term instead of another. He had problems with his writing by transposing the neighboring letters and forgetting some letters at all. He had an uncontrolled wish to move pencils and other objects on the table in front of him.
Neurological examination showed slowing of the saccadic eye movements to the right. The doctor noticed a slight central paresis of the right side of the patient face and paresis of the extensor muscles of his right hand fingers. During the test of extended arms, the right arm of the patient dropped down. The doctor decided to make magnetic resonance imaging (MRI) of the brain and Doppler ultrasonography for the vertebro-basilar blood flow.
What kind of disorder could be in this case?Which brain areas could be involved?
Concept of the problem: physiological and anatomical basis of the language function.Clinical symptoms: difficulties in speaking and writing and some disorders in behavior.
Aim
To relate association areas of the cerebral cortex with the higher functions of the brain, to reveal the neurophysiological basis of motivation, emotions and behavior.
Learning objectives and contents
To complete the analysis of this problem the students should know:• External and internal structure of the telencephalon.• Functional organization of the cerebral cortex. Sensory and motor cortex. • Arterial blood supply of the brain.
13

• Venous drainage of the brain.• Cerebrospinal fluid spaces and features of cerebrospinal fluid flow.
Subject: human anatomyInstitute of AnatomyReferences:Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, 129-153.Drake R. l., Vogl W., Mitchell A. W. M. Gray's anatomy for students. Elsevier.
Philadelphia, 2005, 782-799.Kahle W., Frotscher M., Nervous system and sensory organs. Thieme. Stuttgart-
New York, 2003, p. 208-289.Supplementary readings:Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley &
Belfus. Philadelphia, 2004, plates 24, 26, 30, 32-36, 40-42.
• The functions of the association areas of the cerebral cortex• Asymmetry of the brain. The differences in function of the right and left
hemispheres. • The language areas of the cerebral cortex. • Kinds of aphasias: disorders of speech.• Motivation, emotions and behavior. Subjects: Physiology and pathophysiology Department of Physiology
References:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch. 16 (p. 272-277).Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia:
Elsevier Saunders; 2006. Ch. 57 (p. 714-722).• Disorders of cerebral circulation and tumors.
Subject: pathological anatomy Clinic of Pathological AnatomyReferences:Kumar V., Abbas A. K., Fausto N.. Robbins and Cotran Pathologic Basis of
Disease, 7th Edition, Elsevier Saunders 2005, 1361-1369, 1401-1414.
4.6. Case 6. A forgotten car (Mr. Scatterbrain)
Mr. Scatterbrain is 68-year old pensioner. He is an old car mechanic and lives with his wife in a small flat. His wife is anxious about him for a long time since he has not as much energy as before. He became dull and can sit in his armchair passively without doing anything for hours. He does not take care of himself and has a shave only rarely. Finally, his wife complains that he is “in the clouds” and she has to tell him the same things again and again until he responds. When she asks him to go shopping, he often buys only half of that what she asked. He went sopping by car several times, but came back on foot, since he could not remember where he parked the car. More and more often he does not switch off the cooker after preparing the meal. It seems to his wife that she should always take care of him, but when she gives a hint about that, it upsets him and makes him angry.
14

At last, at repeated requests of his wife, he agreed to see a doctor. According to the doctor’s opinion, his physical health is good. Clinical findings are normal, except slight hypertension (150/90 mm Hg). During the conversation, the doctor noticed that the patient could recall the events of the last days only loosely. Nevertheless, he can repeat a list of several written or spoken words immediately. However it is difficult for him to repeat it after 5 or 10 minutes. The patient knows his age and remembers, with some inaccuracy, the events associated with his family and his professional life. The patient told to the doctor that he was deeply involved in constructing small models. Unfortunately, he had to drop his hobby recently, because he felt he could not do this with the necessary precision. This upsets him quite much. The doctor noticed that the patient couldn’t find simple words to express his thoughts. He even used the word “boat” instead of “boot”. He had a strange tendency to repeat the last words of the person with whom he is speaking.
The doctor leaned from the wife of the patient that he does not use any sedatives or alcohol. The doctor decided to make a full blood analysis and Doppler ultrasonography for the vertebro-basilar blood flow. The magnetic resonance imaging (MRI) of the brain showed a slight increase of the sulci in the cerebral cortex.
How can you interpret the symptoms and condition of the patient?What treatment can you suggest?
Concept of the problem: the physiological basis of learning and memory functions.Clinical symptoms: difficulties in speaking and writing and some disorders in behavior.
Aim
To distinguish different kinds of learning, to explain mechanisms of learning and memory at the systemic and cellular level, to study some cases of memory disorders.
Learning objectives and contents
To complete the analysis of this problem the students should know:• Structure of the limbic system.• Connections of the limbic system structures.
Subject: human anatomyInstitute of AnatomyReferences:Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, 161-167.Kahle W., Frotscher M. Nervous system and sensory organs. Thieme. Stuttgart-
New York, 2003, p. 332-335.Supplementary readings:Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd ed. Hanley &
Belfus. Philadelphia, 2004, plates 43-47, 119-124.• Architectonics of the neocortex. Structural module of the cortex.
Subject: histology and embryologyDepartment of Histology and EmbryologyReferences:Junqueira L.C., Carneiro J. Basic histology. Text & Atlas.11th edition. McGraw-
Hill. Medical Publishing Division. p. 163-166; 168. Supplementary readings:Sadler T.W. Langman’s medical embryology. 10th edition. Lippincott Williams &
15

Wilkins, 2006. p.285-310.
• Non-associative and associative learning (conditioning). • Mechanisms of learning and memory. Subjects: Physiology and pathophysiology Department of Physiology
References:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch. 16 (p. 266-272).Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia:
Elsevier Saunders; 2006. Ch. 57 (p. 723-727), Ch. 58 (p. 728-738), Ch. 59 (p. 745-747).
• The main molecular mechanisms related to brain cell damage and death in Alzheimer disease.
Subject: biochemistryDepartment of BiochemistryReferences:Smith C.M., Marks A.D., Lieberman M. Basic medical biochemistry. A clinical
approach. Lippincot Williams and Wilkins, Philadelphia. 2005, p. 439-457. Champe P.C., Harvey R.A., Ferrier D.R. Biochemistry. Lippincott’s illustrated
reviews. Lippincot Williams and Wilkins, Philadelphia. 2004, p.21.Karp G. Cell and molecular biology. 4th ed. John Wiley&Sons, 2005, p.66-69. http://en.wikipedia.org/wiki/Alzheimer_disease#Biochemical_characteristics
• Psychostimulants. Antidepressants. Anxiolytic agents. Antipsychotic drugs. Medicines improving memory (cognitive function).
Subject: pharmacologyDepartment of Basic and Clinical PharmacologyReferences:Katzung B.G. Basic and Clinical Pharmacology. Appleton and Lange, 1998, p.
100-103, 354-372, 483-496,521-531.Supplementary readings: Howland R.D., Mycek M.J. Lippincotts Illustrated Review: Pharmacology. 3rd
Ed. Lippincott Williams and Wilkins. Philadelphia, 2006, p. 43-55, 115-125, 139-157.
16

5. Lectures
5.1. Histology of sensory receptorsDepartment of Histology and EmbryologyClassification of receptors. Groups of sensitive nerve endings. Free and non-free nerve endings. Terminal nerve cell corpuscles and their classification. Not encapsulated tactile bodies. Encapsulated nerve corpuscles: encapsuleted tactile corpuscle (Meissner‘s corpuscle), flat corpuscles (Pacini corpuscle) and some others.Peculiarities of receptor cells, centrioles, microtubules, cilia and flagellum structures. Structure of sensory receptors: rod and cone epitheliocytes, crista ampullaris and maculae, sensory (hair) cells, gustatory cells.
5.2. Anatomy of the general and chemical senses: receptors, pathways and centers
Institute of Anatomy
Structure and classification of receptors, peculiarities of their distribution, neuroanatomical description of the receptive field. Location of the first order somatosensory neurons and projection of their central and peripheral processes. Somatosensory nuclei in the spinal cord and brain stem. Somatosensory tracts in the spinal cord and brain stem, subcortical centers and projections into brain cortex.
Olfactory system: anatomy of olfactory organ, pathways and centers. Gustatory system: anatomy of the gustatory organ, pathways and centers.
5.3. Physiology and pathophysiology of the somatosensory system and chemoreception
Department of Physiology
Classification of sensations. Receptor potential. Adaptation. Tonic and phasic receptors. Encoding of the modality and intensity of the stimulus. Receptive field and lateral inhibition. Somatosensory system. Mechanical skin senses. Senses of temperature and pain. Kinds of pain. Endogenic pain-suppressing system. Two somatosensory pathways. Lesions of pathways. Brown-Séquard syndrome. Somatotopic organization of the cerebral cortex. Sensory transduction in taste and smell systems.
5.4. Opioid and nonopioid (antipyretic) analgesics. Local anestheticsDepartment of Basic and Clinical PharmacologyGeneral characteristic of the drug groups. Classification and names of the medicines. Pharmacodynamics (mode of action) and pharmacokinetics. Pharmacological effects. Adverse effects.
5.5. Local anesthesiaClinic of General Surgery
Ways and methods of anesthesia. Local anesthesia, development, indications and contraindications. Local anesthetics, clinical features and dosage.
17

5.6. Anatomy of vision: structure of the eye, visual pathways and location of centers
Institute of AnatomyStructure of the eye. Coats of the eyeball: fibrous, vascular and inner layers. Macula and optic disc. Ocular refractive media: cornea, aqueous humor, lens and vitreous body. Visual pathways, subcortical and cortical visual centers. Accessory structures of the eye: muscles of the eyeball, eyelids, conjuctiva, lacrimal apparatus, orbit. Innervation of the eye. Vascular supply of the eye.
5.7. The structure of the organ of vision. Retinal histologyDepartment of Histology and Embryology
Internal structure of the eye: fibrous, vascular and internal layers of the eye. Structure of sclera and retina. Structure of ciliary body and iris. Composition of retina. Histology of neuron chains: external (photoreceptor), medial (associative) and internal (ganglionic). The course of light rays in the retina. Ultrastructure of visual cells. The content of the eyeball: the lens and the vitreous. Accessory organs of the eye: the eyelid and lacrimal duct. Formation of the organ of vision.
5.8. Physiology and pathology of the visual systemDepartment of Physiology
The optical system of the eye. Optical defects and their correction. Accommodation. Pupillary reflex. Signal transduction in the retina. Receptive fields of ganglion cells. Visual acuity. Adaptation. Color vision. Visual field. Visual pathways and their lesions. Binocular vision. Eye movement.
5.9. Processing of the sensory information in the structures of the visual cortex
Institute of Biology
The light reflected from surfaces carries information on various properties of objects, like shape, size, color, texture, position, tilt angle, movement direction, speed, and others. The main goal of the investigations on visual perception is to explain the information flow processing at different levels of the visual system and to understand the principles of synthesis of unite sensory image from various object features. More than a third part of the brain cortex is involved into the visual information processing, e.g. occipital, parietal, temporal, frontal regions and associative centers.
5.10.Sense of hearing and balance: structure of the ear, auditory and vestibular pathways and centers. Relation of vestibular organ and cerebellum
Institute of Anatomy
The ear: organ of hearing and balance. External ear: auricle, outer ear canal, tympanic membrane. Middle ear: tympanic cavity, auditory ossicles and auditory tube. Internal ear: bony and membranous labyrinths, perilymph and endolymph. Sense of hearing, auditory pathways and centers. Sense of balance, vestibular pathways and centers. Connections of vestibular nuclei with the cerebellum. Innervation of the ear. Vascular supply of the ear.
18

5.11. Histology of the auditory and vestibular organDepartment of Histology and EmbryologyHistology of the vestibular and auditory organ: external, medial and internal ear. The organ of vestibular: the structure of crista ampullaris and maculae. The structure of auditory organ. Make up of the cochlear duct, the structure of organ of Corti. Histophysiology of the auditory organ. Formation of the auditory and vestibular organ.
5.12.Physiology and pathological physiology of the hearing and equilibrium systems
Department of Physiology
Directional sensitivity of the hair cells. The detection of the head position, the linear and angular acceleration. Vestibulospinal and vestibulo-ocular reflexes. Nystagmus. Kinetosis. Sound transmission through the middle air. Signal transduction in the Corti organ. Encoding the frequency and intensity of the sound stimulus. The range of the audible frequencies. The organization of the central auditory pathways. Binaural hearing.
5.13.Reticular formation of the brain stemInstitute of Anatomy
Anatomy of the reticular formation, morphological and neurochemical characterization of the reticular formation neurons, specific reticular nuclei, efferent and afferent connections. Vital centers of the reticular formation.
5.14.Sleep and wakefulnessDepartment of Physiology
Alternation of sleeping and waking. Circadian rhythms. Sleep phases: slow wave sleep and rapid eye movement (REM) sleep. Sleep stages and cycles. Functional changes in the body organs and systems during the sleep. The transmitter systems of the brain responsible for the sleep and sequence of sleep stages.
5.15.Neurotransmitters and their metabolismDepartment of BiochemistrySynthesis and inactivation of catecholamine and indolamine neurotransmitters, histamine, acetylcholine and GABA. Amino acids as neurotransmitters. Pain mediators: glutamate, kinins, catecholamines. Enkephalins and endorphins.
5.16.Hypnotic and general anesthesia inducing drugs. Antiepileptic drugs
Department of Basic and Clinical PharmacologyGeneral characteristic of the drug groups. Classification and names of the medicines. Pharmacodynamics (mode of action). Pharmacokinetics and method of adminsitration. Therapeutic use. Adverse effects.
19

5.17.Morphofunctional organization of the telencephalon and cerebrovascular system
Institute of Anatomy
Surfaces of the cerebrum. Brodmann's areas of the cortex. Functional organization of the cortex: sensory, motor and association cortex. Asymmetry of the cerebral hemispheres and speech area.
Peculiarities of the blood supply of the brain and anatomy of the blood-brain barrier. Arterial supply, basilar artery and circle of Willis. Venous drainage, superficial and deep cerebral veins, venous dural sinuses. Ventricular system of the brain, choroid plexus and cerebrospinal fluid.
5.18. Architectonics of the cerebral cortex. Structural module of the cerebral cortex
Department of Histology and Embryology
The cerebrum (the brain). The neocortical layers of the brain. Cytoarchitectonics. Brodman areas. Types of cortical cells and their connections. Myeloarchitectonics. Columnar structure of the cerebral cortex: functional and morphological module.
5.19.Physiological basis of the language functionDepartment of Physiology
Functions of association cortex. Dominant and non-dominant hemisphere. Language areas (Broca and Wernicke). Apraxia and agnosia. Split brain phenomenon. Neglect syndrome.
5.20.Brain stroke. Tumors of the nervous system and coveringsClinic of Pathological Anatomy
Conception of the brain stroke. Ischemic and hemorrhagic brain stroke, its causes, mechanisms of developing, morphological peculiarities and outcomes. Classification of tumors of the nervous system, morphological peculiarities of most common tumors, lacal and general complications and causes of death.
5.21.Anatomy of the limbic systemInstitute of Anatomy
Paleocortex, archicortex and neocortex: subdivision and functional significance. Subdivisions and pathways of the limbic system: amygdala, septum, hippocampal formation and cingulate gyrus. The interconnections between associative neocortical regions and the component parts of the limbic system. Neurochemical types of the neurons and their connections.
5.22.Learning and memory. Emotions and behaviorDepartment of Physiology
Motivation and behavior. Reward and punishment systems of the brain. Emotions and the limbic system. Non-associative and associative learning. Formation of the memory.
20

5.23.Pathogenetic importance of reactive nitrogen and oxygen species Department of BiochemistryMechanisms of reactive nitrogen and oxygen species induced brain-cell death. Role of neuroglia. Mechanisms of formation of beta amyloid and other proteins typical for Alzheimer disease.
5.24.Psychostimulants. Antidepressants. Anxiolytics. Antipsychotic drugs. Medicines improving memory
Department of Basic and Clinical PharmacologyGeneral characteristic of the drug groups. Classification and representatives (names of the medicines). Pharmacodynamics (mode of action). Pharmacokinetics and method of administration. Therapeutic use. Adverse effects. Acute and chronic toxicity, overdosing.
21

6. Practicals
6.1. Sensation of touch and esthesiometry. Smell and tasteDepartment of Physiology
Print Appendix 9.1 and 9.2 for laboratory works
Part 1. Touch sensation and esthesiometry.Aim: To define the spatial threshold of the skin on different parts of the arm and hand
using the method of esthesiometry. Instrumentation: Esthesiometer.
Using the esthesiometer, determine the minimal distance between two points which are perceived as two, not as one. Compare the spatial threshold of the skin of the shoulder, forearm, hand and finger tips.
Part 2. Sensation of taste and smell. Aim: To determine taste perception threshold and relations between sensations of
taste and smell. Laboratory equipment: The solutions with different concentrations of sugar, NaCl,
quinine sulfate and acetic acid. Slices of an onion and potato.
Give the subject to taste solutions with different taste starting from the lowest concentrations. Mark the lowest perceivable concentration as the threshold. Clamp the nose and put a slice of onion or potato on the tongue. Check if the subject can perceive the taste.
References:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch.7 (p. 138-142), Ch. 10 (p. 185-191).Ghai CL. A textbook of practical physiology, 1989. p. 288-289, 309-310.Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia: Elsevier
Saunders; 2006, Ch. 46 (p. 573-578), Ch. 47 (p. 585-597), Ch. 53 (p. 663-670).
6.2. Drug used in pain: opioid analgesics and antipyretics. Local anesthetics
Department of Basic and Clinical PharmacologyGeneral characteristic of the groups in relation with its clinical use. Classification and representatives of the groups. Mode of action. Effects on pain. Pharmacokinetic characteristics and method of administration. Systemic and local effects. Adverse effects. Overdosing, prevention and treatment of the overdosing.
References:Katzung B. G. Basic and Clinical Pharmacology. Appleton and Lange, 1998, p.
425-434, 496-516, 578-588.Supplementary readings: Howland R. D., Mycek M. J. Lippincotts Illustrated Review: Pharmacology. 3rd Ed.
Lippincott Williams and Wilkins. Philadelphia, 2006, p. 157-169, 495-515.
22

6.3. Types of local anesthesia. Techniques and complicationsClinic of General Surgery
Superficial, infiltrative and intravenous regional anesthesia. Peripheral and central nerve blocks, technique, complications, prevention of complications and first aid.
References:Oxford handbook of anaesthesia. Second edition. Ed. Keith G. Allman. Oxford Medical Publications, 2006.
Supplementary readings:Oxford handbook of anaesthesia. Second edition. Edited by Keith G. Allman. Oxford
Medical Publications. 2006
6.4. Anatomy of the eyeball and accessory structuresInstitute of Anatomy
Anatomy of the orbit. Structure of the eyeball: fibrous, vascular and inner layers. Anatomy of the fundus of the eye: macula, optic disc and blood vessels of the retina. Ocular refractive media: cornea, aqueous humor, lens and vitreous body. Anatomy of the visual pathway, subcortical and cortical visual centres. Accessory structures of the eye: muscles of the eyeball, eyelids, conjuctiva, lacrimal apparatus, orbit. Innervation of the eye. Vascular supply of the eye.
References:Drake R. l., Vogl W., Mitchell A. W. M. Gray's anatomy for students. Elsevier.
Philadelphia, 2005, 830-853. Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, p. 155-159, 103-105.Kahle W., Frotscher M., Nervous system and sensory organs. Thieme. Stuttgart-
New York, 2003, p. 338-359.Supplementary readings:
Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley & Belfus. Philadelphia, 2004, plates 89 - 91, 94 - 104.
Moses K. P., Banks J. C., Nava P. B., Petersen D., Atlas of clinical gross anatomy. Elsevier, 2005, p. 58-71.
6.5. Histology of organ of vision. The structure of the retinaDepartment of Histology and EmbryologyDescription of histological slides:
1. Optical calix, calix opticus (H-E). On a section of the embryo’s head, try to identify the calix using low microscopic magnification. Under high magnification, examine the structure of separate parts of the developing organ of vision and make an attempt to explicate the origin of development of each part of the eye, focusing on the peculiarities of development of the retina. Make a drawing of the structure of the developing eyeball.
2. The eyeball, bulbus oculi (H-E). Under low microscopic magnification, try to find the coating of the posterior part of the eyeball: the retina, the choroidea, the sclera.
3. Retina, retina, (H-E). On examining retinal structures under high microscopic magnification, investigate and draw the following layers of the visual retina: stratum pigmentosum, stratum nervosum, stratum limitans externa, stratum nucleare
23

externum, stratum plexiforme externum, stratum nucleare internum, stratum plexiforme internum, stratum ganglionicum, stratum neurofibrorum, and stratum limitans internum. Pay attention to the changes in the stratum pigmentosum when the visual retina is in the dark and in the day light. Make efforts to keep in mind the histological structure of different layers.
References:Valančiūtė A., Vitkus A. Laboratory works. II semester. KMU, 1993, p. 3-4
6.6. Accommodation, visual acuity and peripheral vision. Binocular vision and illusions
Department of Physiology
Print Appendix 9.3 and 9.4 for laboratory works
Aim: (1) To define accommodation range (the distance between far and near point) and amplitude (difference in refractive power at rest and in full accommodation); to define visual acuity; to examine peripheral color vision (white, blue, red, green). (2) To define Panum area of the visual system; to measure the intensity of geometric illusion by changing one parameter of the image.
Laboratory equipment: (1) Optic bench, two movable pins, a perforated disk, a table of optotytpes, a set of lenses; perimeter, colored pencils and leaflets, calipers and a ruler. (2) Computerized technique and the software for of the visual psycho-physiological experiment.
(1) Define the near and the far point for the sharp vision. Calculate the range and amplitude of the accommodation. Define the visual acuity for a subject using the tables. Assess the influence of the refraction upon the visual acuity by using lenses (+1 dpt and –1 dpt). Recognize the relation between refraction and accommodation.
Study the peripheral vision by fixing the subject’s eye at the center of the perimeter. Approach the color stimulus from the periphery. Mark the maximal distance on the graph (every 30°) when the stimulus is detected. Compare the visual field for different colors. Analyze the visual field defects due to the lesions of the visual pathways.
(2) Fix the chin at the convenient height and choose the appropriate distance of the flag in order to see the left side of the screen with the left eye only and the right side of the screen with the right eye only. Select the figures and increase or decrease their size checking when they seem double. Assess the visual mistakes due to illusions by comparing and changing the parameters of the figures.
References:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch. 8 (p. 148-170).
Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia: Elsevier
Saunders; 2006, Ch. 49 (p. 613-625), Ch. 50 (p. 626-639), Ch. 51 (p. 640-650).
6.7. Anatomy of the temporal bone and external, middle and internal ear. Relation of vestibular organ and cerebellum
Institute of Anatomy
Anatomy of the temporal bone. External ear: auricle, outer ear canal, tympanic
24

membrane. Middle ear: tympanic cavity, walls of the tympanic cavity, auditory tube, auditory ossicles and muscles of auditory ossicles. Internal ear: bony and membranous labyrinths. Vestibulocochlear nerve. Anatomy of the auditory and vestibular pathways and centers. Connections of vestibular nuclei with the cerebellum. Nerves of the ear. Blood vessels of the ear.
References:Drake R. l., Vogl W., Mitchell A. W. M. Gray's anatomy for students. Elsevier.
Philadelphia, 2005, 854-871. Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, p. 109-111, 115-121.Kahle W., Frotscher M., Nervous system and sensory organs. Thieme. Stuttgart-
New York, 2003, p. 362-383.Supplementary readings:
Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley & Belfus. Philadelphia, 2004, plates 64 - 68, 73 - 74, 77.
Moses K. P., Banks J. C., Nava P. B., Petersen D., Atlas of clinical gross anatomy. Elsevier, 2005, p. 72-81.
6.8. Vestibular and auditory organ. The internal ear. The spiral organ of Corti
Department of Histology and Embryology
Description of histological slides:
1. Cochlea (H-E) (cross section). It is a spiral cochlear duct twisted two and half times having a bony cochlear spiral formation, modiolus. Using lower magnification, make an attempt to identify the section of labyrinthus osseus. Indicate the triangular form of ductus cochlearis, the scala vestibiuli, and the scala tympani. Under high magnification, point out the membrana basalis with organum spirale located on it. Find ciliary epitheliocytus piliaris, the internal and external ciliary, epitheliocytus sensorius pilosus and epitheliocytus phalangeus. Take into account the composition of membrana tectoria, and ligamentum spirale cochleae. Make a drawing of all these structures.
References:Valančiūtė A., Vitkus A. Laboratory works. II semester. KMU, 1993, p. 2-3.
6.9. Tonal liminal audiometry. Kinetosis Department of Physiology
Print Appendix 9.5 and 9.6 for laboratory works
Aim: (1) To define hearing thresholds at various tone frequencies conducted by air; (2) To model kinetosis (motion sickness) and to explain pathogenesis of the symptoms.
Laboratory equipment: (1) Audiometer with the headphones; (2) Bárány chair.
(1) Define hearing thresholds at various tone frequencies by increasing the sound intensity from 0 dB up to the lowest level the subject can hear. Check the left and right ear separately using the headphones. Draw the threshold audiograms for air conduction. Explore examples of audiograms with hearing pathology.
25

(2) Investigate the effect of rotation on some body functions. Count the pulse rate and measure the arterial blood pressure before the test. Turn the subject sitting on the Bárány chair at 10 revolutions per 20 seconds. Stop suddenly the chair and check the pulse rate and blood pressure of the subject as soon as possible. Observe the movement of the eyeballs at the same time and define the kind of the nystagmus. Fill in the table of results. Review the video record of the kinetosis evoked in guinea pig by putting some drops of chloroform into the external auditory canal.
References: Civinskienė G., Kėvelaitis E., Korotkich I. ir kt. Fiziologijos praktikos darbai. Kaunas, 2006, p. 77-80.
Lažauskas R., Laukevičienė A., Korotkich I., Senikienė Ž., Bulatov A. Fiziologijos praktikos darbai. I dalis. KMU leidykla, Kaunas, 2000. p. 47-53.
Porth C.M. Pathophysiology. 7th ed. Lippincott Williams & Wilkins. Baltimore, 2005. p. 1344-1351.
http://en.wikipedia.org/wiki/Motion_sickness
6.10.Electroencephalogram (EEG) and evoked potentials Department of Physiology
Print Appendix 9.7 for laboratory work
Aim: To estimate the waves of the electroencephalogram (EEG) and the evoked potentials.
Laboratory equipment: A computer program with real recordings of the EEG and evoked potentials.
Distinguish the EEG from interfering physiological signals. Describe the EEG waves of different frequencies. Define the alpha waves and the mechanism of their production. Recognize and define the mechanism of the reaction of EEG desynchronization. Define the wave characteristic of the epileptic seizure. Distinguish the sleep stages according to the EEG waves. Conceive the principle of isolation of the evoked potentials. Describe the visual evoked potential.
References:Ganong WF. Review of medical physiology. 22nd ed. New York: Lange Medical
Books / McGraw-Hill; 2005. Ch. 11 (p. 192-201).
Supplementary readings:Guyton AC, Hall JE. Textbook of medical physiology. 11th ed. Philadelphia: Elsevier
Saunders; 2006, Ch. 59 (p. 739-745).
6.11.Drugs inducing sleep and general anesthesia. Antiepileptic drugsDepartment of Basic and Clinical PharmacologyGeneral characteristic of the groups in relation with its clinical use. Classification and representatives of the groups. Mode of action. Effects on sleep, on conscious. Pharmacology of antiseizure action. Pharmacokinetic characteristics and method of administration. Systemic and local effects. Adverse effects. Teratogenic and mutagenic effect of antiepileptics. Dependence and tolerance. Interaction with another drugs.
References:Katzung B. G. Basic and Clinical Pharmacology. Appleton and Lange, 1998, p.
354-372, 386-425.
26

Supplementary readings: Howland R. D., Mycek M. J. Lippincotts Illustrated Review: Pharmacology. 3rd Ed.
Lippincott Williams and Wilkins. Philadelphia, 2006, p. 103-115, 125-139, 169-180.
6.12.Morphofunctional organization of the telencephalon and cerebrovascular system
Institute of Anatomy
Surfaces of the cerebrum. Brodmann's areas of the cortex. Arterial supply: pools of the vertebral and internal carotid arteries, basilar artery and circle of Willis. Venous drainage, superficial and deep cerebral veins, venous dural sinuses. Ventricular system of the brain, choroid plexus and cerebrospinal fluid spaces.
References:Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, 129-153.Drake R. l., Vogl W., Mitchell A. W. M. Gray's anatomy for students.
Elsevier. Philadelphia, 2005, 782-799.Kahle W., Frotscher M., Nervous system and sensory organs. Thieme.
Stuttgart-New York, 2003, p. 208-289.Supplementary readings:Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed.
Hanley & Belfus. Philadelphia, 2004, plates 24, 26, 30, 32-36, 40-42.
6.13.Architectonics of the cerebral cortex and its structural modulusDepartment of Histology and Embryology
Description of histological slides:
1. Cerebral vesicles, vesiculae cerebrales (H-E). Under lesser magnification, find three cerebral vesicles. Make a drawing and point out the ratio of cerebral vesicles to the entire body of the embryo. It is necessary to find and mark the spinal cord and the spinal ganglion.
2. The cortex of the cerebrum, cortex cerebralis |(impregnation). Using lesser microscopic magnification, find out the gray and white mater of the hemisphere. Using high magnification find and draw the following layers of the cerebral cortex: I - stratum moleculare, II- stratum granulare externum, III - stratum neurium pyramidalium externum, IV - stratum granulare internum, V –stratum neurium pyramidalium internum, VI – stratum neurium fusiformium. You also have to mark the structure and form of neuroglial cells and neurons of the cerebral cortex. Pay attention to the form and direction of dendrities and neurites. Recall everything you know about interneural relations of the cerebral cortex.
3. Choroid plexus, plexus chorioideus. Under lesser microscopic magnification, try to identify the transverse section of the choroid plexus of the cerebral ventricle. Using high magnification, make attempts to draw the choroidal tissue, tela choroidea. At this place the wall of the choroid plexus is covered by a layer of cuboid or low columnar epithelium containing a network of blood vessels.
References:
27

Valančiūtė A., Vitkus A. Laboratory works. II semester. KMU, 1993, p. 2-3.
6.14.Brain stroke. Tumors of the nervous system and coveringsClinic of pathological anatomy
By studying macro- and micropreparations, select and evaluate preparations illustrating causes of the brain stroke, morphological peculiarities and causes of death. Identify individual tumors of the brain and brain coverings in macropreparations, Evaluate peculiarities of their morphology and progress. Solve the modeled morphological diagnostic tasks.
Glioblastoma (spongioblastoma) multiforme. Histological slide (H+E). Find a tumor composed of glial cells of various sizes and shapes. Pay attention to the hemorrhages and foci of necrosis in the tumor.
Macropreparations 1. Atherosclerosis a.a. cerebri (stenosis >75%)2. Thrombus obturatotius arteriae3. Necrosis (infarctus) colliguativa (ramolitio) cerebri4. Cystis post ramollitionem cerebri5. Haemorrhagia cerebri6. Haemosiderosis cerebri7. Carcinoma metastaticum cerebri8. Meningioma (arachnoidendothelioma) durae matris9. Astrocystoma10. Glioblastoma (spongioblastoma) multiforme11. Medulloblastoma cerebelli12. Phlebotrhrombosis cruris13. Embolia thrombica a. pulmonalis14. Bronchopneumonia
Questions for self-study 1. What means the conception of “brain stroke”?2. What are causes and peculiarities of the development of brain infarctions?3. What is the difference in development of ischemic and hemorrhagic infarctions?4. What is morphology of the brain infarction?5. What is the outcome and functional significance of the brain infarctions?6. What is the classification of tumors of the nervous system?7. Why do all tumors of the nervous system have a malignant course?8. How the benign and malignant tumors of the nervous system are classified
according to the degree of their differentiation and maturity?9. How and where do the tumors of the nervous system spread?10. What is the glioblastoma multiforme and medulloblastoma?11. What meningeal tumors do you know?12. What are the causes of death due to tumors of the nervous system?13. What tumors of the autonomic nervous system do you know?14. What are the tumors of the peripheral nervous system?15. What are causes of death due to pheochromocytoma?
ReferencesKumar V, Abbas AK, Fausto KN, editiors. Robbins and Cotran pathologic basis of
disease. 7th ed. Philadelphia; Elsevier Saunders; 2005. p.1361-1367, 1401-1410.
28

6.15.Psychostimulants. Antidepressants. Anxiolytics. Antipsychotic drugs. Medicines improving memory
Department of Basic and Clinical Pharmacology
Understanding of emotions, thinking, memory and cognitive disorders. General characteristic of the groups in relation with its clinical use. Classification and representatives of the groups. Mode of action and pharmacological effects. Changes of the brain neurotransmitters using these medicines. Pharmacokinetic characteristics and method of administration. Adverse effects. Acute and chronic toxocity. Prevention of the overdosing.
References:Katzung B. G. Basic and Clinical Pharmacology. Appleton and Lange, 1998, p.
100-103, 354-372, 483-496, 521-531.Supplementary readings: Howland R.D., Mycek M.J. Lippincotts Illustrated Review: Pharmacology. 3rd Ed.
Lippincott Williams and Wilkins. Philadelphia, 2006, p. 43-55, 115-125, 139-157.
29

7. Seminars
7.1. Molecular mechanisms of light signal transductionDepartment of BiochemistryAim: To get acquainted with structural features and mechanisms of action of the main compounds implicated in light signal transduction.Objectives1. To get acquainted with structural features of light-sensitive pigments and their
interaction with specific proteins in photoreceptors of retina.2. To discuss about structural alterations as well as function of rhodopsin and its
component 11-cis retinal under light signal transduction.3. To get acquainted with stages of light signal transmission and respective changes
of photoreceptors as well as light-sensitive pigments.4. The influence of vitamin A deficiency on the visual function.References:Berg J.M., Tymoczko J.L., Stryer L.. Biochemistry, 5th ed. W.H. Freeman, New
York, 2002, p.903-913.Cox D.N.and Nelson M.M.. Lehninger Principles of Biochemistry. 3rd ed., Worth
Publishers, New York, 2000, p.458-462.http://en.wikipedia.org/wiki/Rhodopsinhttp://depts.washington.edu/biowww/faculty/saari.html
7.2. Significance and anatomical peculiarities of the reticular formation
Institute of Anatomy
Anatomy of the reticular formation of the brainstem, morphological and neurochemical characterization of the reticular formation neurons, specific reticular nuclei. Location of the reticular formation. Significance of the reticular formation.
References:Crossman A. R., Neary D. Neuroanatomy. Churchill Livingstone. Edinburgh,
2005, p. 87-99, 123-128.Kahle W., Frotscher M., Nervous system and sensory organs. Thieme. Stuttgart-
New York, 2003, p. 146-149.Supplementary readings:
Poritsky R., Freeman B. K. Neuroanatomy: To color and study. 2nd Ed. Hanley & Belfus. Philadelphia, 2004, plates 29, 142-144.
30

8. Module examination program
8.1. Biology1. Morphological and functional projections of the retina to the primary visual
cortex.2. Types of receptive fields of the primary visual cortex.3. Modular structure of the primary visual cortex.4. Functional peculiarities of the higher visual cortices. 5. Conception of the sensory information-processing channel.
8.2. Anatomy1. Pathway of the epicritic sensibility.2. Pathway of the protopathic sensibility.3. Structure, pathways and centers of the olfactory organ.4. Gustatory organ - structure, innervation, pathways and centres. 5. Structural parts of the eyeball.6. Optic nerve, optic tract and centers.7. Muscles of the eyeball, their innervation.8. Organs of the eyeball protection, lacrimal apparatus.9. Anatomy of the external and middle ear.10. Anatomy of the inner ear.11. Auditory pathway and centers.12. Vestibular pathways and centers.13. Reticular formation: location, structure, neurochemical characteristic and
significance.14. External structure and morphofunctional characteristic of the telencephalon.15. Limbic system: subdivision, location, connections with other brain parts and
significance.16. Brain blood supply.
8.3. Histology1. Histology of sensory receptors.2. Histophysiology of the retina.3. The ultrastructure of the retinal cells, their importance in vision. The yellow and
blind spot of the retina.4. Histophysiology of the vestibular organ.5. Structure of the cochlea.6. Histophysiology of the Corti organ.7. Cyto-myeloarchitectonics of the cerebral cortex.8. Cyto-myeloarchitectonics of the cortex of the cerebellum.9. Structural module of the cerebral cortex.
8.4. Physiology and pathophysiology1. Primary and secondary sensory cells. Receptor potential. Adaptation. Tonic and
phasic receptors. 2. Mechanoreception in the skin. Encoding of the modality, intensity and location.
Receptive field and lateral inhibition.
31

3. Receptors for tyemperature and pain. Pain substances (mediators). Kinds of pain. 4. Two somatosensory pathways transmitting information up to the cortex. Effects of
lesions. 5. Central mechanisms controlling pain.6. Optical system of the eye. Optical defects and their correction. Accommodationan
its control. 7. Response of the pupil to the light. Pupillary reflex arc. Clinical significance of
disorders.8. Functional organization of the retina. Receptive fields of the ganglion cells. 9. Visual pathways. Projections to the cortex. P and M channels of visual
information. 10. Dark adaptation. Color vision and its disorders. 11. Function of the outer and middle ear. Ear and bone conduction. Disorders of
conduction. 12. The traveling wave of the basilar membrane of the cochlea. Transduction of the
sound signal in the hair cells of Corti organ. 13. Encoding of the sound frequency and intensity. Central auditory pathways.
Detection of sound source direction. 14. Directional sensitivity of the hair cells in the vestibular organ. Sensation of body
position, linear and angular acceleration. Disorders of the balance and equilibrium.
15. Transduction of signals in the taste sensory cells and the central transmission pathways.
16. The functional organization of the smell system. 17. Functions of association cortex. Language areas. Aphasias. 18. Non-associative and associative learning. Mechanisms of learning and memory.
Disorders of memory. 19. Motivation and behavior. Emotions and the limbic system. 20. Sleep phases, stages and cycles defined by EEG, EMG and EOG. Changes of
functions of the other organs and systems. The role of the reticular system. Sleep disorders.
8.5. Biochemistry 1. Synthesis and inactivation of catecholamine and indolamine neurotransmitters.2. Biochemical functions of rhodopsin and 11-cis retinal in light signal transduction.3. Reactive nitrogen and oxygen species: formation and pathogenetic importance.
8.6. Pharmacology1. Describe the mode of action of opioid receptors agonists, antagonists and mixed
(agonists–antagonists) acting drugs. Pharmacological effects on CNS and peripheral organs. Clinical use of these medicines.
2. Describe the opioid analgesics used for pain relief, cough suppress and diarrhea. Denote the most common adverse effect.
3. Describe the mechanism of action, pharmacological effects and adverse effects of the non-opioid analgesics.
4. Indicate the main groups, representatives of local anesthetics. Describe adverse effects.
5. Describe the mechanism of action ir main pharmacological properties of inhaled and intravenous anesthetics.
6. Identify the classification, mechanism of action and main pharmacological effects
32

of anxiolytic and hypnotic drugs.7. Describe the clinical use and adverse effects of benzodiazepines, barbiturates and
other (newer) anxiolytics and hypnotics. Indicate how to avoid tolerance, dependence and withdrawal syndrome of anxiolytics and hypnotics.
8. Identify the pharmacological effects and dose effect relationship (show graphically) of benzodiazepines and barbiturates. Compare the dose effect relationship between benzodiazepines and barbiturates.
9. Indicate the classification of antiepileptic drug according to mechanism of action. Name the most popular representatives and describe the most common adverse effects.
10. Indicate the antiepileptic drugs used to treat partial, generalized seizures, absence, myoclonus and epileptic state. Describe the most common adverse effects.
11. Identify classification of antidepressant drugs. Name the most common representatives and their mechanism of action.
12. Identify the pharmacodynamic and pharmacokinetic properties and their clinical use of the main antidepressant groups.
13. Describe the most common adverse effects of antidepressant drugs in relation with effects on different classes of receptors (adrenergic, cholinergic, serotoninergic and histaminergic).
14. Describe the classification of antipsychotic drugs (neuroleptics). Name the main representatives and their pharmacological effects depending on action on the different localization of dopamine receptors.
15. Indicate the pharmacodynamic and pharmacokinetic properties of antipsychotic drugs (neuroleptics) and their clinical use (therapeutic indications).
16. Describe the most common adverse effects of antipsychotic drugs (neuroleptics) in relationship to their action on different brain structures and organs (e.g. parkinsonism, dyskinesias, endocrine and metabolic effects, antiadrenergic, antihistaminergic and antimuscarinic effects etc.).
17. Indicate the main groups of drugs used to treat memory (cognitive) disturbances, name the main representatives and adverse effects.
18. Describe the most common adverse effects of drugs used to treat memory (cognitive) disturbances.
8.7. General surgery 1. Superficial and infiltrative anesthesia, indications for surgery, contraindications,
technique and anesthetics.2. Intravenous regional anesthesia, indications, technique, anesthetics and
complications.3. Peripheral and central nerve blocks.
8.8. Pathological anatomy1. Etiology, mechanisms of development and morphological picture of the brain
infarction.2. Classification of the tumors of nervous system and its coverings.3. Morphological peculiarities and complications of the tumors of central nervous
system.
33

Name …………...……….…………………… Group ..………. Date .………………..
9. Appendix
9.1. Sensation of touch
The receptor surface of the sensory skin system is enormous and varies from 1.4 to 2.1 m2. A spatial differentiation of a skin surface, i.e. the capacity of a human subject to perceive separately the touching of two neighboring points of the skin, varies widely in its different parts. The double-point threshold of spatial differentiation of the tongue mucus membrane is equal to 0.5 mm and on the skin of the back to more than 60 mm. These differences are mainly associated with various sizes of skin receptive fields (from 0.5 mm2 to 3 cm2) and with the degree of their overlapping.
The procedure:
1. The eyes of the subject should be closed throughout this exercise. The esthesiometer is a pair of dividers with a scale indicating the distance between the legs in millimeters. To determine how closely the two points of the esthesiometer can be brought together and yet be felt as two points the observer should touch the subject in a random manner with either one point or with two points of the esthesiometer to prevent guessing.
2. Measure (in mm) how closely the two points of the esthesiometer can be brought together and yet be felt as two points when applied to the skin on the ventral surface of the thumb. Make each determination three times. Average the results.
Repeat the experiment on the palm and back of the hand, ventral and dorsal surface of the forearm, and fingertips. Record all values in the table.
ResultsFill the results of the esthesiometry in the following table.
Localization in the body Threshold of touch sensationyours partner’s
Ventral surface of the thumb
The hand – ventral surface
The hand – dorsal surface
The forearm – ventral surface
The forearm – dorsal surface
The fingertips
34
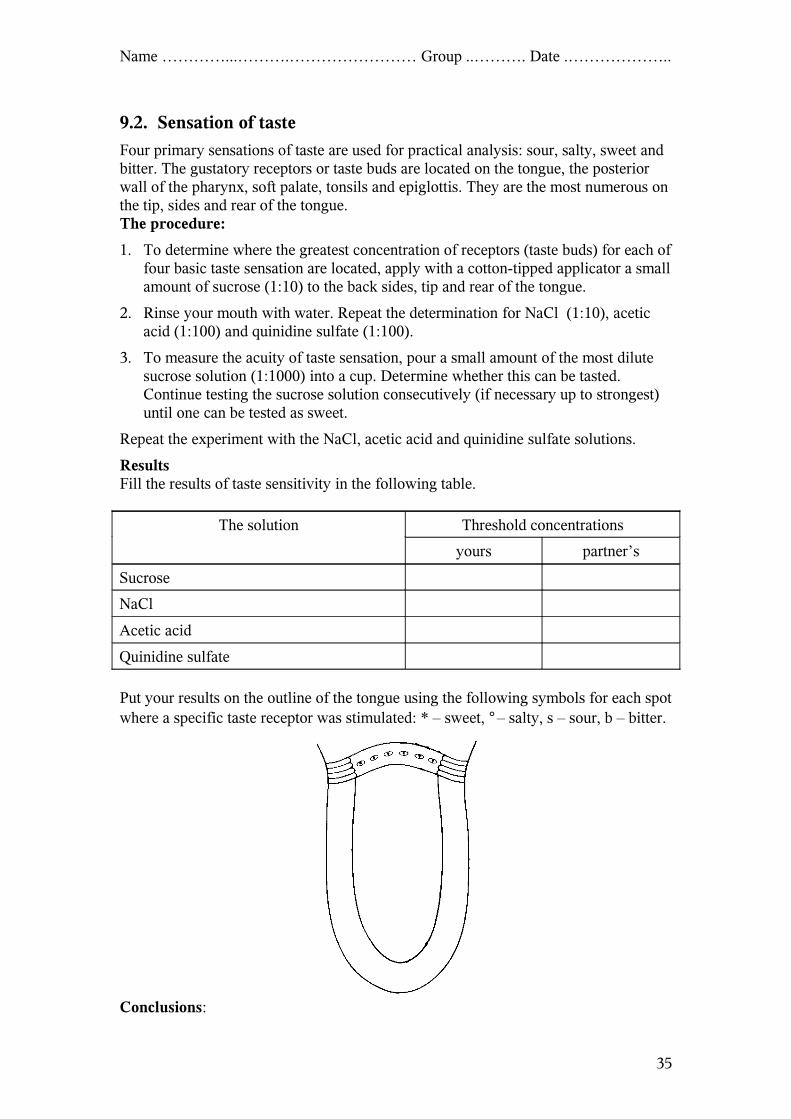
Name …………...……….…………………… Group ..………. Date .………………..
9.2. Sensation of taste
Four primary sensations of taste are used for practical analysis: sour, salty, sweet and bitter. The gustatory receptors or taste buds are located on the tongue, the posterior wall of the pharynx, soft palate, tonsils and epiglottis. They are the most numerous on the tip, sides and rear of the tongue.The procedure:
1. To determine where the greatest concentration of receptors (taste buds) for each of four basic taste sensation are located, apply with a cotton-tipped applicator a small amount of sucrose (1:10) to the back sides, tip and rear of the tongue.
2. Rinse your mouth with water. Repeat the determination for NaCl (1:10), acetic acid (1:100) and quinidine sulfate (1:100).
3. To measure the acuity of taste sensation, pour a small amount of the most dilute sucrose solution (1:1000) into a cup. Determine whether this can be tasted. Continue testing the sucrose solution consecutively (if necessary up to strongest) until one can be tested as sweet.
Repeat the experiment with the NaCl, acetic acid and quinidine sulfate solutions.
ResultsFill the results of taste sensitivity in the following table.
The solution Threshold concentrations
yours partner’s
Sucrose
NaCl
Acetic acid
Quinidine sulfate
Put your results on the outline of the tongue using the following symbols for each spot where a specific taste receptor was stimulated: * – sweet, ° – salty, s – sour, b – bitter.
Conclusions:
35

Name …………...……….…………………… Group ..………. Date .………………..
9.3. Accommodation and the visual acuity
Adjustment of the eye to sharp vision of objects at different distances is called accommodation. The mechanism of accommodation consists of contraction of the ciliary muscles, which alter the convexity of the lens. The ciliary muscles are innervated by the parasympathetic fibers of the oculomotor nerve. Stimulation of the parasympathetic fibers contracts the ciliary muscle, which relaxes the lens ligaments and increases the curvature of the lens and, consequently, its refractive power. With an increased refractive power, the eye is capable of focusing on near objects. The eye is considered to be normal, or emmetropic, if parallel light rays from the distant objects are in sharp focus on the retina, when the ciliary muscle is completely relaxed. This means that the emmetropic eye can see all distant objects clearly; with its ciliary muscle relaxed. To focus the objects at a close range the ciliary muscle must contract and thereby provide various degrees of accommodation.
There are two principal anomalies of light refraction in the eye: (1) hypermetropia or “far-sightedness” and (2) myopia or “near-sightedness”. Hypermetropia is usually due either to an eyeball that is too short or occasionally to a lens system that is too weak when the ciliary muscle is relaxed. In this condition the parallel light rays from the object converge behind the retina. This defect of refraction can be corrected by an effort of accommodation, i.e. by increasing the convexity of the lens. In hypermetropic persons the near point of vision is farther from the eye than in persons with normal vision, and efforts of accommodation when examining near objects proves insufficient. That is why the hypermetropic persons have to wear convex glasses for reading which increase the refraction.
In myopia, when the ciliary muscle is completely relaxed the light rays coming from distant objects are focused in front of the retina. This is usually due to a too long eyeball, but it can occasionally result from too much refractive power of the lens system of the eye. No mechanism exists by which the eye can decrease the strength of its lens to less than that, which exists when the ciliary muscle is completely relaxed. However, as an object comes nearer to the eye, it finally comes near enough that its image will focus. Myopia is corrected by placing a concave lens in front of the eye, which diverges the rays.
With increasing age, the lens becomes less elastic, partly because of progressive denaturation of lens proteins. Therefore, the ability of the lens to change its shape progressively decreases, and the power of accommodation also decreases. This condition is called presbyopia and that is why old people correct the errors of accommodation with the help of convex glasses.
The procedure:
Detection of punctum proximum: 1. Put one pin on the optical bench about 15 cm and another pin about 1 m in front of
your eyes.2. Look through the holes in the disk K (a distance between the holes s and d is less
than diameter of the pupil) and focus on the near pin (P) (see Figure). Note whether the pin (nearer P or farther R) appears double or single.
3. Now focus on the distant pin (R) and note whether the pin appears double or single (see Figure).
4. Put a pin on the optical bench in front of one eye (the other being closed) at arm’s length. Gradually bring the pin nearer to the eye by drawing it along the optical
36

Name …………...……….…………………… Group ..………. Date .………………..
bench. When the pin appears to be double, the item is closer than the near point and your eye can no longer accommodate for it. Move the pin away to the point where it appears single again. This is your near point of vision (punctum proximum). If glasses are worn, determine the near point without glasses. Determine the near point for each eye in centimeters and compare with that of your partner.
Assessment of visual acuity:1. For the assessment of visual acuity the distant vision of the subject should be
tested with the Snellen’s test chart. While the subject stands 5 meters from the Snellen chart, the observer stands near the Snellen chart, which should be well illuminated.
2. The subject should then cover one eye with a card, but should not close the eye. The observer indicates the lines to be read and the subject should read the letters from above downwards (the distance for each line in meters is given on the chart).
3. Test each eye separately without glasses and with convex lens (+1D) and concave lens (–1D). Express the results as:
V=d/D, 4. where: V – visual acuity, d – the distance at which certain letters can be read by
the subject, D – the distance at which the same letters can be read by the normal eye.
5. If the subject usually wears glasses the test should be repeated with the glasses on.6. Compare the results without and with glasses or with lens (+1D and –1D).
Results:
Parameters Right eye Left eyeyours partner’s yours partner’s
Punctum proximum
Vis
ual a
cuity Without glasses
With +1D lensWith –1D lensWith glasses (if indicated)
37

Name …………...……….…………………… Group ..………. Date .………………..
Conclusions:
9.4. Visual field
Space seen by the eye when gaze is steadily fixed on one point is called the visual field. The process of charting the visual field is known as perimetry. The area seen to the medial side is called the nasal visual field, and the area seen to the lateral side is called the temporal visual field. The boundaries of the normal visual field for colorless objects are about 90° on the temporal side, about 60° on the nasal side, about 50° upward and about 35° downward. The peripheral visual field is maximum for white objects, and smaller for blue, red and green in that order. The subject should be able to distinguish the color with certainty.
Destruction of an entire optic nerve obviously causes blindness of the respective eye. Destruction of the optic chiasm prevents the passage of impulses from the nasal halves of the two retinas to the opposite optic tracts. Therefore, the nasal halves are both blinded, which means that the person is blind in both temporal visual fields. This condition is called bitemporal hemianopsia. Such lesions frequently result from tumors of the adenohyphophysis pressing upward on the optic chiasm. Interruption of an optic tract denervates the corresponding half of each retina on the same side as the lesion, and, as a result, neither eye can see objects on the opposite side. This condition is known as homonymous hemianopsia. Lesion of the optic radiation or the visual cortex of one side also causes homonymous hemianopsia. In all perimetry charts, a blind spot caused by lack of rods and cones in the retina over the optic disc is found approximately 15° laterally to the central point of vision. Occasionally blind spots are found in portions of the visual field other than the optic disc area. Such blind spots are called scotomata. They frequently result from allergic reactions in the retina or from toxic conditions, such as lead poisoning or excessive use of tobacco.
The procedure:
1. The subject should be seated on a stool in front of the perimeter that consists of a broad metal rotatable arc and adjustable chin rest mounted on a pillar. Adjust the height of the chin rest so that the eye (for example right eye) is at the level of the arc. Instruct the subject not to move his eye but keep looking at the center of the arc.
2. Fix a test object (a white spot) in the carrier and take it to the end of the arc.3. Start on the temporal side in the horizontal meridian. Tell the subject to raise his
hand or say “yes” as soon as the object comes into view. Bring the test object inwards and as soon as the subject raises his hand record this point in the chart.
4. Move the arc downwards by 30° gradually bring the object inwards from the end of the arc once again.
5. Repeat the procedure until the arc returns back to the original position (i.e. through 360°). Joint all points in the chart paper with a pen. This is the peripheral visual field.
6. Chart the peripheral visual field with test objects of green color. Compare the visual field with that of your partner.
Conclusions:
38

Name …………...……….…………………… Group ..………. Date .………………..
Results of perimetry
Visual pathways and visual fields. Lesions of the visual pathways a, b, c and d are shown on the left. Shade in the corresponding visual field defects in figures A, B, C and D on the right. (N – nasal, T – temporal side of the visual field).
39

Name …………...……….…………………… Group ..………. Date .………………..
9.5. Tonal liminal audiometry
Tonal liminal audiometry is used to evaluate the acuity of hearing for sounds of different height. The value of hearing threshold in decibels (dB) is marked on the Y-axis of the graph, called audiogram, where the X-axis is the tone frequency in hertz (Hz). During the measurement, sound conductivities by air and by bone tissue are studied.
AimDetermination of the hearing thresholds {of the sound conductivities by air and
by bone} for the tones of different frequency.
EquipmentAudiometer with headphones.
ProcedureMeasurement of sound conductivity by air.1. Put on the headphones: with red mark - on the right ear, with blue - on the left.2. Press the “Left” key on the control panel of audiometer to start testing of the left
ear.3. Press the “Tone Interrupter” key. The indicator pointer must be fixed in the
rightmost position. If it does not occur, press the key again.4. Using the “Frequency” switch, choose the necessary frequency of the tone (250,
500, 1000, 2000, 6000 or 8000 Hz).5. With the “Hearing” switch, set the tone intensity higher than minimal so, that the
examined person could hear it distinctively. Using the same switch, set the tone intensity to zero, and then start increasing it by 5 dB each time. When the examined person begins to hear the tone again, abort the increase. Repeat the measurement 2 - 3 times to determine minimal threshold intensity. Mark its value for chosen frequency on the audiogram.
6. Using the “Frequency” switch, change the tone height and repeat the measurement (step 5) until you obtain values of threshold intensity for all other frequencies. Remember, that during measurements the pointer of indicator always must be in the rightmost position. To fix it there, press the "Tone Interrupter" key if necessary.
7. Press the “Right” key on the control panel of audiometer, and repeat steps 3 – 6 for the right ear.
8. Connect the points on the audiograms with a continuous line.
Measurement of the sound conductivity by the bone tissue.1. Place the smaller headphone on the processus mastoideus from the left side so,
that it would not touch the auricle.2. Press the "Bone" key.3. Perform the measurement as described in the previous section (steps 3 - 6) and
repeat it from the right side.4. Connect the points on the audiograms with a dotted line.
After the measurement turn off the audiometer by pressing the "Battery Switch" key.
40

Name …………...……….…………………… Group ..………. Date .………………..
Left ear
250 500 1000 2000 4000 6000 8000 Hz
50
60
70
80
90
100
110
120 dB
Right ear
250 500 1000 2000 4000 6000 8000 Hz
50
60
70
80
90
100
110
120 dB
-10
0
10
20
30
40
-10
0
10
20
30
40
41

Name …………...……….…………………… Group ..………. Date .………………..
9.6. Kinetosis
A complex of organism reactions, which occur under the influence of acceleration, lateral or torsion swing and repeated thrust, is called kinetosis. Acceleration can be:- linear (positive or negative) ,- centripetal - acceleration of the thrust - angular
The main pathogenetical mechanisms of kinetosis :- stimulation of mechanoreceptors of equilibrium (or balance ) organ;- stimulation of proprioreceptors in the skin, muscles, tendons, articulations,
visceral organs;- stimulation of vision receptors, induced by changing movements of the objects in
the space; - signalization from receptors of mucous membranes and serosal covers to nuclei of
autonomic nervous system.
Characteristic features of kinetosis are:weakness, paleness, bradycardia, decrease of arterial blood pressure, nausea. Stimulation of n. vagus causes vomiting and sweating.
Nystagmus is one of the features of acceleration action. Nystagmus is an involuntary rapid oscillation of the eyeballs in a horizontal, vertical, or rotary direction. Nystagmus on extreme lateral gaze that fatigues quickly usually is physiologic. Opticokinetic nystagmus is physiologic as well. It is the eyeball movement induced by looking at a rapidly repeated pattern (e.g., when looking at passing telegraph poles from the window of a moving train).
Nystagmus can be rotatory, vertical or horizontal. The direction of the nystagmus is determined by the direction of the quick component because it is easier to see. However, the slow component is the more fundamental response to vestibular stimulation, while the quick component is compensatory. The slow component moves in the direction of the movement of the endolymph. The hallucination of movement of environment is in direction of endolymphatic flow, and the hallucination of movement of subject is in the opposite direction.
Patients with vertigo, difficulty with balance, or a sensorineural hearing loss of unknown etiology should have vestibular function tested by electronystagmography (ENG) with caloric test. Caloric stimulation is produced by irrigating the ears with warm and cool water, which causes convection currents within endolymph. These currents cause movement of the cupula in the ampulla of the horizontal semicircular canal. The movement is in one direction during cooling and in the opposite direction during warming. The duration of the nystagmus and the velocity of slow component or the frequency of nystagmus may be measured. Canal paresis, a unilateral reduction or absence of sensitivity and directional preponderance, a relative exaggeration of the nystagmic response in one direction, can be demonstrated.
Nystagmus should be described in regard to- the direction of fast and slow component;- its character: regular, irregular or rotatory;- the degree of involvement of either eye.
42

Name …………...……….…………………… Group ..………. Date .………………..
Rotation testSelect a student for examination; register his pulse rate and arterial blood pressure and make sure that he has no spontaneous nystagmus before the rotation. Leave the cuff on the arm and start twisting the student in Bárány chair. Ask him to make his head inclined 30° forward to examine the horizontal semicircular canal (or 90° forward for examination of frontal semicircular canal, or to bend his head to one of the shoulders to examine the respective sagittal canal). Twist the chair around 10 times per 20 sec, then stop rotation abruptly and examine the eyeballs. At the same time take his pulse (per 10 s) and arterial blood pressure several times until they normalize.
Describe the changes in pulse rate and arterial blood pressure and note the time of normalization. Record the values of pulse rate and arterial blood pressure in the table and display them graphically.
When is the nystagmus observed: before or after the rotation?Describe the changes in pulse and blood pressure noting the time of normalization.Explain the mechanism of the observed changes.
Results: Fill in the table and draw a graph:
Variable Before Time after rotationrotation …….s …….s …….s …….s …….s
Pulse rate (beats/min)Systolic blood pressure (mm Hg)Diastolic blood pressure (mm Hg)
Results
40
60
80
100
120
140
160
180
Time (s)
Pu
lse
rate
/ B
loo
d p
ress
ure
Pulse rate
Systolic BP
Diastolic BP
Conclusions:
43

Name …………...……….…………………… Group ..………. Date .………………..
9.7. Electroencephalogram (EEG)
Direction: Make measurements on the screen and fill in the tables.
F1 ELECTROENCEPHALOGRAPHY
A Calibration.
B Non-EEG signals, superimposed on the EEG: eye movements.
TraceNo.
Lead (derivation):
F, C, P, O
Amplitude of the eye movement potentials
(µV)1.2.3.4.
C Non-EEG signals, superimposed on the EEG: electromyogram (EMG).
D α-waves: frequency and amplitude E β-waves: frequency
ExampleNo.
Amplitude (µV)
Frequency (Hz)
Example No.
Frequency (Hz)
1. 1.2. 2.3. 3.4. Sum
Sum MeanMean
F, G, H Desynchronization Choose one kind of desynchronization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Choose the lead (derivation) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
EEG pattern Amplitude (µV)
Frequency (Hz)
SychronizedDesychronized
I Habituation. After how many repetitions the habituation is evident? . . . . . .
J EpilepsyPattern of seizure activity
Amplitude (µV)
Duration of complex (s)
Frequency of complex (Hz)
Frequency band(α, β, δ, θ)
Spike-and-wave complexNote. Calculate the frequency from the duration of the complex!
44

Name …………...……….…………………… Group ..………. Date .………………..
K, L, M, N Sleep
EEG pattern Amplitude (µV)
Duration of the wave
Frequency (Hz)
Frequency band (α, β, δ, θ)
K WakefulnessFalling asleep
L "Vertex" waveM SpindlesN K-complexNote. Do not fill the shaded cells!
F2 EVOKED POTENTIALS
A Principle of averaging
B Visual evoked potential
The lead (derivation)
Largest positive waveamplitude
(µV)latency
(ms)
CONCLUSIONS:
45