Prognostic Implications of Type 2 Diabetes Mellitus in Ischemic and Nonischemic Heart ... ·...
13
Prognostic Implications of Type 2 Diabetes Mellitus in Ischemic and Nonischemic Heart Failure Isabelle Johansson, MD, PHDFELLOW, a Ulf Dahlström, MD, PHD, b Magnus Edner, MD, PHD, a Per Näsman, PHD, c Lars Rydén, MD, PHD, a Anna Norhammar, MD, PHD a ABSTRACT BACKGROUND Heart failure (HF) is a common and serious complication in type 2 diabetes mellitus (T2DM). The prognosis of ischemic HF and impact of revascularization in such patients have not been investigated fully in a patient population representing everyday practice. OBJECTIVES This study examined the impact of ischemic versus nonischemic HF and previous revascularization on long-term prognosis in an unselected population of patients with and without T2DM. METHODS Patients stratified by diabetes status and ischemic or nonischemic HF and history of revascularization in the Swedish Heart Failure Registry (SwedeHF) from 2003 to 2011 were followed up for mortality predictors and longevity. A propensity score analysis was applied to evaluate the impact of previous revascularization. RESULTS Among 35,163 HF patients, those with T2DM were younger, and 90% had 1 or more associated comorbidities. Ischemic heart disease (IHD) occurred in 62% of patients with T2DM and 47% of those without T2DM, of whom 53% and 48%, respectively, had previously undergone revascularization. T2DM predicted mortality regardless of the presence of IHD, with adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) of 1.40 (1.33 to 1.46) and 1.30 (1.22 to 1.39) in those with and without IHD, respectively. Patients with both T2DM and IHD had the highest mortality, which was further accentuated by the absence of previous revascularization (adjusted HR: 0.82 in favor of such treatment; 95% CI: 0.75 to 0.91). Propensity score adjustment did not change these results (HR: 0.87; 95% CI: 0.78 to 0.96). Revascularization did not abolish the impact of T2DM, which predicted mortality in those with (HR: 1.36; 95% CI: 1.24 to 1.48) and without (HR: 1.45; 95% CI: 1.33 to 1.56) a history of revascularization. CONCLUSIONS Ninety percent of HF patients with T2DM have preventable comorbidities. IHD in patients with T2DM had an especially negative influence on mortality, an impact that was beneficially influenced by previous revascularization. (J Am Coll Cardiol 2016;68:1404–16) © 2016 by the American College of Cardiology Foundation. From the a Cardiology Unit, Department of Medicine K2, Karolinska Institutet, Stockholm, Sweden; b Department of Cardiology and Department of Medical and Health Sciences, Linköping University, Linköping, Sweden; and the c Center for Safety Research, KTH Royal Institute of Technology, Stockholm, Sweden. This work was supported by unrestricted grants from the Swedish Heart- Lung Foundation and the Regional Agreement on Medical Training and Clinical Research (ALF) between Stockholm County Council and the Karolinska Institute. Dr. Dahlström has received research grants from Linkoping University and AstraZeneca Inc.; and honoraria from expert group participation organized by different pharmaceutical companies, none of which were directly related to the present publication. Dr. Rydén has received research grants from the Swedish Heart-Lung Foundation, AFA Insurance, and the Swedish Diabetes Foundation; honoraria from expert group participation; and personal fees for delivering educational lectures organized by pharmaceutical and societal organizations, none of which were directly related to this publication. Dr. Norhammar has received funding from the Swedish Heart-Lung Foundation and the Swedish Diabetes Foundation for the present report; and has received honoraria for advisory boards and lectures from Eli Lilly, AstraZeneca, MSD, and Boehringer Ingelheim. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received May 20, 2016; revised manuscript received June 17, 2016, accepted June 21, 2016. Listen to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Valentin Fuster. JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 68, NO. 13, 2016 ª 2016 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION PUBLISHED BY ELSEVIER ISSN 0735-1097/$36.00 http://dx.doi.org/10.1016/j.jacc.2016.06.061
Transcript of Prognostic Implications of Type 2 Diabetes Mellitus in Ischemic and Nonischemic Heart ... ·...

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y VO L . 6 8 , N O . 1 3 , 2 0 1 6
ª 2 0 1 6 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 0 6 . 0 6 1
Prognostic Implications ofType 2 Diabetes Mellitus inIschemic and Nonischemic Heart Failure
Isabelle Johansson, MD, PHD FELLOW,a Ulf Dahlström, MD, PHD,b Magnus Edner, MD, PHD,a Per Näsman, PHD,cLars Rydén, MD, PHD,a Anna Norhammar, MD, PHDa
ABSTRACT
Fro
De
Ro
Lu
Co
Inc
dir
AF
de
thi
Fo
an
to
Ma
BACKGROUND Heart failure (HF) is a common and serious complication in type 2 diabetes mellitus (T2DM). The
prognosis of ischemic HF and impact of revascularization in such patients have not been investigated fully in a patient
population representing everyday practice.
OBJECTIVES This study examined the impact of ischemic versus nonischemic HF and previous revascularization on
long-term prognosis in an unselected population of patients with and without T2DM.
METHODS Patients stratified by diabetes status and ischemic or nonischemic HF and history of revascularization in the
Swedish Heart Failure Registry (SwedeHF) from 2003 to 2011 were followed up for mortality predictors and longevity.
A propensity score analysis was applied to evaluate the impact of previous revascularization.
RESULTS Among 35,163 HF patients, those with T2DM were younger, and 90% had 1 or more associated comorbidities.
Ischemic heart disease (IHD) occurred in 62% of patients with T2DM and 47% of those without T2DM, of whom 53% and
48%, respectively, had previously undergone revascularization. T2DM predicted mortality regardless of the presence of
IHD, with adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) of 1.40 (1.33 to 1.46) and 1.30 (1.22 to 1.39) in
those with and without IHD, respectively. Patients with both T2DM and IHD had the highest mortality, which was further
accentuated by the absence of previous revascularization (adjusted HR: 0.82 in favor of such treatment; 95% CI: 0.75 to
0.91). Propensity score adjustment did not change these results (HR: 0.87; 95% CI: 0.78 to 0.96). Revascularization did
not abolish the impact of T2DM, which predicted mortality in those with (HR: 1.36; 95% CI: 1.24 to 1.48) and without
(HR: 1.45; 95% CI: 1.33 to 1.56) a history of revascularization.
CONCLUSIONS Ninety percent of HF patients with T2DM have preventable comorbidities. IHD in patients with
T2DM had an especially negative influence on mortality, an impact that was beneficially influenced by previous
revascularization. (J Am Coll Cardiol 2016;68:1404–16) © 2016 by the American College of Cardiology Foundation.
m the aCardiology Unit, Department of Medicine K2, Karolinska Institutet, Stockholm, Sweden; bDepartment of Cardiology and
partment of Medical and Health Sciences, Linköping University, Linköping, Sweden; and the cCenter for Safety Research, KTH
yal Institute of Technology, Stockholm, Sweden. This work was supported by unrestricted grants from the Swedish Heart-
ng Foundation and the Regional Agreement on Medical Training and Clinical Research (ALF) between Stockholm County
uncil and the Karolinska Institute. Dr. Dahlström has received research grants from Linkoping University and AstraZeneca
.; and honoraria from expert group participation organized by different pharmaceutical companies, none of which were
ectly related to the present publication. Dr. Rydén has received research grants from the Swedish Heart-Lung Foundation,
A Insurance, and the Swedish Diabetes Foundation; honoraria from expert group participation; and personal fees for
livering educational lectures organized by pharmaceutical and societal organizations, none of which were directly related to
s publication. Dr. Norhammar has received funding from the Swedish Heart-Lung Foundation and the Swedish Diabetes
undation for the present report; and has received honoraria for advisory boards and lectures from Eli Lilly, AstraZeneca, MSD,
d Boehringer Ingelheim. All other authors have reported that they have no relationships relevant to the contents of this paper
disclose.
nuscript received May 20, 2016; revised manuscript received June 17, 2016, accepted June 21, 2016.

AB BR E V I A T I O N S
AND ACRONYM S
CABG = coronary artery
bypass surgery
CI = confidence interval
CKD = chronic kidney disease
eGFR = estimated glomerular
filtration rate
HF = heart failure
HR = hazard ratio
IHD = ischemic heart disease
LVEF = left ventricular
ejection fraction
MI = myocardial infarction
NYHA = New York Heart
Association
PCI = percutaneous coronary
intervention
SwedeHF = Swedish Heart
Failure Registry
T2DM = type 2 diabetes
mellitus
J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6 Johansson et al.S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6 Diabetes, Heart Failure, and Ischemic Heart Disease
1405
D iabetes mellitus, predominantly type 2(T2DM), affects 390 million people globally,a number expected to increase to 600
million in 2030 (1). Cardiovascular disease is themost common complication and mortality causerelated to T2DM. Recent evidence favors increasinglife expectancy in patients with T2DM becauseof improved risk factor management and post–myocardial infarction (MI) survival (2,3). Unfortu-nately, these improvements are expected to increasethe prevalence of chronic complications, includingheart failure (HF) (4). Besides enhancing the risk ofHF, T2DM has an adverse impact on the prognosis ofHF (5). Consequently, an increasing proportion of pa-tients with T2DM are expected to develop ischemicHF in the future. Diabetes is over-represented in HFpopulations, even in the absence of ischemic heartdisease (IHD). The presence of a specific diabetes-induced cardiomyopathy unrelated to hypertensionor IHD but rather caused by deranged myocardialmetabolism has been proposed as an explanation(6). However, the actual prevalence and role of thiscondition in terms of morbidity and mortality remainto be fully understood (7–9). Moreover, existing evi-dence related to the true impact of T2DM on HF sur-vival, often based on subgroup analyses of eitherclinical trials or registry reports, is conflicting. Studieshave indicated better (9), equal (7,8), and compro-mised (9) survival in ischemic and nonischemic HF(10,11). These discrepant results probably reflect therecruitment of different and selected patient popula-tions and often vaguely defined glucometabolicstates.
SEE PAGE 1417
The aim of this study was to investigate the prev-alence and impact of ischemic and nonischemic HFand the role of previous revascularization in patientswith T2DM in a contemporary unselected HF popu-lation that reflects everyday clinical practice.
METHODS
DATA SOURCE. The Swedish Heart Failure Registry(SwedeHF), introduced throughout Sweden in 2003,has been described in detail elsewhere (12). Registryinformation is available on the SwedHF website (13).Participating centers (65 hospitals, 113 outpatientclinics) report to the registry, which contained infor-mation on 47,000 patients in 2011. The primary in-clusion criterion is a physician-judged diagnosis ofHF; 76 variables are recorded via an Internet-basedcase report form at hospital discharge or outpatientvisits. Data are entered into a database managed by
the Uppsala Clinical Research Center(Uppsala, Sweden) and run monthly againstthe Swedish Population Registry.
STUDY POPULATION AND DESIGN. BetweenJanuary 2003 and September 2011, 36,595patients with HF managed in a specialistsetting were included in SwedeHF. The pre-sent cohort of 35,163 patients (68% fromhospitals, 32% from outpatient clinics) wasestablished after the exclusion of patientswith no information on sex or glucometabolicstate (n ¼ 123) or who had type 1 diabetesmellitus (n ¼ 198) or IHD (n ¼ 1,111). The dateof the first registration was assigned as theindex date, and all descriptive data in thepresent analysis were extracted from thissingle occasion. The primary endpoint wasall-cause mortality, acquired by merging theSwedeHF database with the Swedish Popu-lation Registry using the unique 10-digitpersonal identification number of Swedishcitizens. Follow-up ended on September
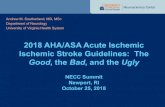
13, 2011.DEFINITIONS. Definitions are based on the pre-defined definitions used in SwedeHF (OnlineAppendix). HF was diagnosed by the attendingphysician based on guideline recommendations at thetime of inclusion. New York Heart Association (NYHA)functional classes I to IV were used to define HFseverity. An adapted definition was used for IHD,defined as present or absent based on the case historyfrom patient records. Patients reported as withoutIHD but with a confirmed coronary revascularizationprocedure (n ¼ 739) or a history of previous MI(n ¼ 218) were reclassified as having IHD (Figure 1).Revascularization was defined in SwedeHF as a his-tory of coronary artery bypass surgery (CABG) orpercutaneous coronary intervention (PCI). This pro-cedure is freely available in Sweden, and patients aregenerally offered this treatment according to thecurrent European guidelines (14). MI was based oninformation from patient records. T2DM was definedas a confirmed history of this diagnosis or the pre-scription of glucose-lowering drugs. Comorbiditieswere defined as the presence of any or several of thefollowing: hypertension, atrial fibrillation, pulmonarydisease, valvular heart disease, or idiopathic dilatedcardiomyopathy, all of which were classified as “yes”or “no” based on patient records. Left ventricularejection fraction (LVEF) was the most recently esti-mated, grouped into 4 classes: $50%, 40% to 50%,30% to 39% and <30%. Estimated glomerular filtrationrate (eGFR) was calculated with the MDRD formula,

FIGURE 1 Redefinition of IHD
IHD No IHD
Total cohortn = 35 163
Original
Modified IHD
Final IHD variable
IHD, verified by corain = 5 977
IHD, not verified bycorai
n = 10 957
No IHDn = 18 229
IHDn = 16 934
No/missing IHDbut
revascularizedn = 739
IHDn = 17 673
No IHDn = 17 490
No/missing IHD,no/missing revascularization
butPrevious MI
n = 218
IHDn = 17 891
No IHDn = 17 272
To avoid misclassification, an adapted definition was used for ischemic heart disease (IHD), defined as present or absent based on the case history
from hospital records. Patients reported as being without IHD but with a confirmed coronary revascularization procedure (n ¼ 739) or history of
previous myocardial infarction (MI) (n ¼ 218) were reclassified as having IHD, which yielded 17,891 patients (51%) with IHD and 17,272 (49%) without.
corai ¼ coronary angiography.
Johansson et al. J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6
Diabetes, Heart Failure, and Ischemic Heart Disease S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6
1406
and an eGFR <60 ml/min1/1.73 m2 was considered thecutoff for chronic kidney disease (CKD).
STATISTICAL ANALYSIS. Statistical comparisons ofdifferences between independent groups were per-formed with the Student t test for continuous vari-ables. Quantitative normally distributed variables arepresented as the mean (standard deviation) and 95%confidence intervals (CIs) or, when appropriate, me-dian, range, and 95% CI. Natriuretic peptides werelogarithmically transformed before Student t testing.Categorical variables were compared by chi-squaretests and are presented as counts and proportions(%). Analyses of differences between those with andwithout T2DM were performed in subgroups by IHDstatus and further in the IHD population in those withand without previous revascularization. Statisticaldifferences for all-cause mortality by T2DM, IHDstatus, and revascularization were estimated withCox proportional hazard regression and depicted ascrude and age-adjusted estimated survival curves.
Univariate and multivariate models were used toevaluate the predictive value of T2DM, as well asrevascularization, in all-cause mortality. Adjustmentsfor potentially important covariates were performedin 2 models. Model 1 included age, sex, HF duration,level of care, weight, systolic and diastolic bloodpressure, LVEF class, eGFR class, hemoglobin class,T2DM, hypertension, atrial fibrillation, pulmonarydisease, and use of angiotensin-converting enzymeinhibitors, angiotensin receptor II blockers, betablockers, mineralocorticoid receptor antagonists,diuretic agents, digitalis, nitrates, statins, andantithrombotic agents. Model 2 included the samevariables as model 1 plus 2 additional variables (heartrate and NYHA functional class) that were excludedfrom model 1 because of a large number of missingvalues. In addition, because of the observationalcharacter of the investigation, a propensity scoremodel was applied to avoid potential bias regardingthe impact of previous revascularization on all-causemortality. The propensity score, which expressed the

J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6 Johansson et al.S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6 Diabetes, Heart Failure, and Ischemic Heart Disease
1407
probability of an assigned treatment, in this caserevascularization, given a set of known baselinecharacteristics, was used to balance the study popu-lation with regard to a chosen dependent variable(15). Logistic regression was used to estimate indi-vidual propensity scores for the history of revascu-larization in patients with IHD and T2DM (n ¼ 5,182)with a good fit (Hosmer and Lemeshow test; p ¼ 0.27[p > 0.05 is considered a good fit] and c-statistic of0.7) based on 26 baseline variables (including de-mographics, medical history, and reported pharma-cological treatment) (15). The selected variables werethose that affected all-cause mortality in univariatelogistic regression given they had a reasonably lowamount of missing data. An individual propensityscore was estimated for 3,467 patients with completeinformation on all variables. The impact of previousrevascularization on all-cause mortality was there-after determined by means of Cox regression adjustedfor the propensity score.
A 2-sided probability value of p < 0.05 wasconsidered significant and is reported with 95% CI.Analyses were performed with SAS statistical soft-ware (version 9.4).
ETHICAL CONSIDERATIONS. The Swedish NationalBoard of Health and Welfare and the Swedish DataInspection Board approved the establishment ofSwedeHF and subsequent patient registration anddata analyses. The registry and this study conform tothe Declaration of Helsinki. Individual patient con-sent was not required or obtained, but patients wereinformed about registry entry with permission to optout. The Regional Ethical Review Board at LinköpingUniversity approved the merging of SwedeHF withthe Swedish Population Registry.
RESULTS
Important clinical characteristics are presented inTable 1. Among 35,163 patients, IHD was reported in51%. The proportion of IHD in the T2DM cohort was62% compared with 47% in those without T2DM, ofwhom 53% and 48%, respectively, had undergoneprevious revascularization.
PATIENTS WITH T2DM WITH AND WITHOUT IHD.
When we compared T2DM patients with and withoutIHD, the former were slightly older (75 years vs. 74years), more often men (66% vs. 57%), and morefrequently had reduced LVEF (<50%: 83% vs. 69%)and CKD (63% vs. 55%). Smoking (current/former)was more common in T2DM patients with IHD (62%vs. 53%), whereas associated comorbidities were lesscommon: atrial fibrillation (40% vs. 51%), idiopathic
dilated cardiomyopathy (7% vs. 12%), hypertension(59% vs. 60%), and pulmonary disease (18% vs. 20%).Eighty-eight percent of the patients with T2DMwithout IHD had at least 1 comorbidity. Thisincreased to 90% when idiopathic dilated cardiomy-opathy was added (Table 2). Patients with andwithout IHD underwent similar pharmacologicaltreatment except for a more frequent use of statinsand acetylsalicylic acid among those with IHD.
PATIENTS WITH IHD IN RELATION TO REVASCULARIZATION.
Baseline data for patients with IHD according to pre-vious revascularization and the presence or absenceof T2DM are outlined in Table 3. When we focused onpatients with T2DM and compared those with andwithout previous revascularization, the latter wereolder (mean age 77 years vs. 73 years) and more oftenwomen (43% vs. 26%). Comorbidities, such as atrialfibrillation and pulmonary disease and preservedLVEF (16% vs. 19%), were less common in T2DMpatients who had been revascularized than inthose who had not. Patients without previous revas-cularization were more often prescribed diureticagents and digitalis but less often given renin-angiotensin-aldosterone system inhibitors, betablockers, and statins.
A corresponding comparison of baseline data be-tween patients without T2DM revealed a similarpattern, although in slightly different proportionsfrom the T2DM cohort.
PATIENTS WITH AND WITHOUT T2DM. Among pa-tients with IHD (Table 1), those with T2DM wereyounger (75 years vs. 77 years) and had a higherprevalence of hypertension (59% vs. 45%) and CKD(63% vs. 56%). The proportion with preserved LVEF($50%) was similar in both groups (17% vs. 18%),but the IHD patients with T2DM were more symp-tomatic (NYHA functional class III or IV; 54% vs.46%). In general, patients with T2DM had moreextensive pharmacological treatment with renin-angiotensin-aldosterone system inhibitors (84% vs.79%), diuretic agents (88% vs. 79%), and statins(67 vs. 59%). About 50% of the IHD patients had ahistory of revascularization, which was more com-mon in patients with T2DM than without (53% vs.48%).
In patients without IHD (Table 1), the mean age was73 years regardless of T2DM state. The comorbiditypattern between those with and without T2DM cor-responded with that in patients with IHD, except thatpreserved LVEF ($50%) was more common in pa-tients without IHD than among those with this dis-ease and more common in those with T2DM than inthose without (31% vs. 26%).

TABLE 1 Baseline Characteristics by Presence of T2DM and by Reported History of Ischemic/Nonischemic Heart Disease
Nonischemic Heart Disease Ischemic Heart Disease
No T2DM(n ¼ 14,029; 81%)
T2DM(n ¼ 3,243; 19%) p Value
No T2DM(n ¼ 12,574; 70%)
T2DM(n ¼ 5,317; 30%) p Value
Demographics
Age, yrs 73.4 � 14 73.7 � 11 0.10 77.2 � 11 74.8 � 10 <0.0001
Age group, yrs <0.0001 <0.0001
#65 3,814 (27) 755 (23) 1,833 (15) 924 (17)
66–80 4,897 (35) 1,475 (45) 5,170 (41) 2,739 (52)
>80 5,318 (38) 1,013 (31) 5,571 (44) 1,654 (31)
Male 7,787 (56) 1,852 (57) 0.10 8,173 (65) 3,509 (66) 0.20
Level of care (hospital/outpatient visit) 65/32 73/27 <0.0001 68/32 74/26 <0.0001
Weight, kg 76 � 19 86 � 21 <0.0001 75 � 16 83 � 18 <0.0001
BMI, kg/m2 26 � 6 29 � 6 <0.0001 26 � 5 28 � 6 <0.0001
Smoking habit (never/former/current) 49/37/14 47/40/13 0.009 41/47/12 38/50/12 0.007
Alcohol consumption (never/ordinary/problematic) 11/77/12 13/74/12 0.01 11/82/7 14/78/9 0.0002
Duration of heart failure (</>6 months) 59/41 51/49 <0.0001 46/54 39/61 <0.0001
NYHA functional class <0.0001 <0.0001
I 1,440 (14) 211 (9) 977 (11) 284 (8)
II 5,049 (48) 1,010 (44) 3,939 (44) 1,478 (39)
III 3,603 (34) 963 (41) 3,563 (40) 1,725 (46)
IV 418 (4) 138 (6) 508 (6) 283 (8)
Heart rate, beats/min 77 � 17 77 � 17 0.13 73 � 15 74 � 15 <0.0001
Blood pressure, mm Hg
Systolic 128 � 22 131 � 22 <0.0001 126 � 21 129 � 22 <0.0001
Diastolic 74.4 � 13 73.8 � 13 0.005 72 � 12 72 � 12 0.19
Pulse pressure, mm Hg 53 � 18 57 � 19 <0.0001 55 � 18 58 � 19 <0.0001
Mean arterial pressure, mm Hg 92 � 14 93 � 14 0.03 90 � 13 91 � 13 0.0003
Previous or present disease
Hypertension 5,587 (41) 1,929 (60) <0.0001 5,508 (45) 3,022 (59) <0.0001
Atrial fibrillation 7,635 (55) 1,652 (51) 0.0004 5,320 (43) 2,116 (40) 0.003
Pulmonary disease 2,336 (17) 640 (20) <0.0001 2,206 (18) 939 (18) 0.52
Valvular heart disease 3,010 (22) 561 (18) <0.0001 2,449 (21) 894 (18) <0.0001
Idiopathic dilated cardiomyopathy 2,138 (16) 379 (12) <0.0001 820 (7) 336 (7) 0.69
Previous interventions
Revascularization (CABG/PCI) . . . 5,871 (48) 2,768 (53) <0.0001
Valvular surgery 737 (5) 140 (4) 0.03 727 (6) 297 (6) 0.64
Left ventricular function (echocardiography) <0.0001 0.15
EF $50% 3,028 (26) 817 (31) 1,890 (18) 797 (17)
EF 40%–49% 2,373 (20) 516 (19) 2,438 (23) 1,006 (22)
EF 30%–39% 2,816 (24) 564 (21) 3,353 (31) 1,422 (31)
EF <30% 3,564 (30) 761 (29) 3,092 (29) 1,415 (31)
Continued on the next page
Johansson et al. J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6
Diabetes, Heart Failure, and Ischemic Heart Disease S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6
1408
MORTALITY. The time of follow-up ranged between0 and 8.7 years (median 1.9 years). By the end ofthe study period, 14,144 patients (40%) had died,3,950 (46%) with T2DM and 10,194 (38%) without.Estimated survival curves among patients with andwithout T2DM and with and without IHD, beforeand after age adjustment, are shown in Figure 2 andCentral Illustration (left), whereas crude and adjustedsurvival rates in patients with IHD by previousrevascularization are shown in Figure 3 and CentralIllustration (right). The most serious prognosis wasseen in patients with IHD and T2DM (Figure 2),especially those without previous revascularization(Figure 3).
Hazard ratios (HRs) of mortality from univariateand multivariate analyses are presented in Table 4.T2DM predicted mortality regardless of the presenceor absence of IHD (unadjusted HR: 1.20 [95% CI: 1.14to 1.25] and 1.21 [95% CI: 1.14 to 1.29], respectively)and remained a mortality predictor in patients withand without IHD after adjustment (HR: 1.40 [95% CI:1.33 to 1.46] and 1.30 [95% CI: 1.22 to 1.39], respec-tively). This pattern persisted in the differentadjustment models, with a slight weakening of theHRs when the number of covariates increased(Table 4). T2DM remained an independent mortalitypredictor among revascularized IHD patients(adjusted HR: 1.36; 95% CI: 1.24 to 1.48), as well as in

TABLE 1 Continued
Nonischemic Heart Disease Ischemic Heart Disease
No T2DM(n ¼ 14,029; 81%)
T2DM(n ¼ 3,243; 19%) p Value
No T2DM(n ¼ 12,574; 70%)
T2DM(n ¼ 5,317; 30%) p Value
Laboratory analyses
Hb, g/l 134 � 18 129 � 18 <0.0001 130 � 17 127 � 17 <0.0001
Hb class (normal/mild anemia/severe anemia) 70/24/6 59/31/9 <0.0001 60/32/8 53/35/12 <0.0001
Creatinine, mmol/L 103 � 52 115 � 66 <0.0001 115 � 61 128 � 74 <0.0001
eGFR, ml/min/1.73 m2 65 � 40 60 � 28 <0.0001 59 � 26 55 � 27 <0.0001
eGFR class, ml/min/1.73 m2 <0.0001 <0.0001
<30 926 (7) 388 (12) 1,238 (10) 829 (16)
30–59 5,375 (38) 1,402 (43) 5,784 (46) 2,491 (47)
60–89 5,953 (42) 1,067 (33) 4,442 (35) 1,579 (30)
>90 1,775 (13) 386 (12) 1,110 (9) 418 (8)
Cholesterol, mmol/l 4.7 � 1.2 4.4 � 1.2 <0.0001 4.4 � 1.2 4.1 � 1.2 <0.0001
LDL, mmol/l 2.9 � 1.0 2.5 � 0.9 <0.0001 2.6 � 1.0 2.3 � 1.0 <0.0001
HbA1c, mmol/mol 41 � 9 59 � 18 <0.0001 42 � 9 59 � 16 <0.0001
BNP, pg/ml 982 � 1,322 769 � 926 0.41* 951 � 1,488 1,092 � 2,197 0.22*
NT-pro-BNP, pg/ml 4,906 � 6,927 4,892 � 6,826 0.43* 6,207 � 8,488 6,115 � 8,257 0.78*
Pharmacological and device intervention
RAA inhibition
ACEI 8,999 (65) 1,953 (61) <0.0001 7,783 (62) 3,212 (61) 0.05
ARB 2,194 (16) 745 (23) <0.0001 2,383 (19) 1,383 (26) <0.0001
ACEI or ARB 10,979 (78) 2,616 (81) 0.003 9,973 (79) 4,446 (84) <0.0001
MRA 3,858 (28) 1,077 (33) <0.0001 3,389 (27) 1,658 (32) <0.0001
BB 11,359 (81) 2,656 (82) 0.19 10,815 (86) 4,640 (88) 0.02
ACEI/ARB þ BB 9,345 (67) 2,248 (69) 0.003 8,862 (70) 3,997 (75) <0.0001
ACEI/ARB þ BB þ MRA 2,647 (19) 776 (24) <0.0001 2,435 (19) 1,309 (25) <0.0001
Diuretic agents (loop/thiazide) 11,082 (79) 2,871 (89) <0.0001 9,878 (79) 4,676 (88) <0.0001
Digitalis 3,107 (22) 672 (21) 0.07 1,749 (14) 761 (14) 0.49
Statins 2,663 (19) 1,318 (41) <0.0001 7,303 (59) 3,523 (67) <0.0001
Nitrates (long-lasting) 803 (6) 301 (9) <0.0001 3,514 (28) 1,755 (33) <0.0001
Antithrombotic agent 5,726 (41) 1,206 (37) <0.0001 3,761 (30) 1,579 (30) 0.79
Aspirin 4,919 (35) 1,429 (44) <0.0001 8,624 (69) 3,728 (71) 0.05
Device therapy 0.25 0.15
Pacemaker 1,165 (8) 298 (9) 1,277 (10) 498 (9)
Cardiac resynchronization therapy 132 (1.0) 26 (0.8) 169 (1.4) 74 (1.4)
Implantable cardioverter-defibrillator 254 (1.8) 48 (1.5) 391 (3.1) 166 (3.2)
Values are mean � SD, n (%), or %. Percentages were computed by group. Pearson chi-square test and Student t test were used for unpaired groups. *Logarithmically transformed before Student t test.
ACEI ¼ angiotensin-converting enzyme inhibitor; ARB ¼ angiotensin receptor II blocker; BB ¼ beta blocker; BMI ¼ body mass index; BNP ¼ B-type natriuretic peptide; CABG ¼ coronary artery bypassgrafting; EF ¼ ejection fraction; eGFR ¼ estimated glomerular filtration rate; Hb ¼ hemoglobin; HbA1c ¼ glycosylated hemoglobin A1c; LDL ¼ low-density lipoprotein; MRA ¼ mineralocorticoid receptorantagonist; NT-pro-BNP ¼ N-terminal fragment pro–B-type natriuretic peptide; NYHA ¼ New York Heart Association; PCI ¼ percutaneous coronary intervention; RAA ¼ renin-angiotensin-aldosterone;SD ¼ standard deviation; T2DM ¼ type 2 diabetes mellitus.
TABLE 2 Comorbidity Pattern Stratified by T2DM
Variable Combinations
Nonischemic Heart Disease Ischemic Heart Disease
No T2DM(n ¼ 14,029; 81%)
T2DM(n ¼ 3,243; 19%)
p Value
No T2DM(n ¼ 12,574; 70%)
T2DM(n ¼ 5,317; 30%)
p ValueMissing n (%) Missing n (%) Missing n (%) Missing n (%)
HTN/AF 317 9,958 (73) 53 2,563 (80) <0.0001 512 8,164 (68) 224 3,852 (76) <0.0001
HTN/AF/COPD 575 10,442 (78) 141 2,639 (85) <0.0001 745 8,675 (73) 381 3,952 (80) <0.0001
HTN/AF/COPD/VHD 1,012 10,763 (83) 261 2,617 (88) <0.0001 1,262 8,790 (78) 609 3,903 (83) <0.0001
HTN/AF/COPD/VHD/iDCM 1,160 11,349 (88) 288 2,674 (90) 0.0004 1,418 8,836 (79) 670 3,897 (84) <0.0001
HTN/AF/COPD/VHD/iDCM/CKD 1,160 11,911 (95) 288 2,817 (93) <0.0001 1,418 9,825 (88) 670 4,294 (92) <0.0001
AF ¼ atrial fibrillation; CKD ¼ chronic kidney disease; COPD ¼ chronic obstructive pulmonary disease; HTN ¼ hypertension; iDCM ¼ idiopathic dilated cardiomyopathy;T2DM ¼ type 2 diabetes mellitus; VHD ¼ valvular heart disease.
J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6 Johansson et al.S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6 Diabetes, Heart Failure, and Ischemic Heart Disease
1409

TABLE 3 Baseline Characteristics in Patients With IHD Stratified by Revascularization and T2DM
IHD: Revascularization IHD: No Revascularization
No T2DM(n ¼ 5,871; 68%)
T2DM(n ¼ 2,768; 32%) p Value
No T2DM(n ¼ 6,466; 73%)
T2DM(n ¼ 2,414; 27%) p Value
Demographics
Age, yrs 73.7 � 10 72.6 � 10 <0.0001 80.2 � 10 77.3 � 10 <0.0001
Age group, yrs <0.0001 <0.0001
#65 1,251 (21) 609 (22) 560 (9) 301 (12)
66–80 2,871 (49) 1,566 (57) 2,226 (34) 1,106 (46)
>80 1,749 (30) 596 (21) 3,680 (57) 1,007 (42)
Male sex 4,467 (76) 2,046 (74) 0.03 3,570 (55) 1,384 (57) 0.07
Level of care (hospital/outpatient visit) 60/40 69/31 <0.0001 76/24 79/21 0.004
Weight, kg 78 � 16 85 � 17 <0.0001 72 � 16 81 � 19 <0.0001
BMI, kg/m2 26 � 4.5 29 � 5.4 <0.0001 25 � 4.7 28 � 6.0 <0.0001
Smoking habit (never/former/current) 36/52/12 35/54/11 0.52 46/41/13 42/45/13 0.02
Alcohol consumption (never/ordinary/problematic) 9/84/7 12/80/8 0.02 14/79/7 16/74/9 0.002
Duration of heart failure (</>6 months) 48/52 39/61 <0.0001 45/55 40/60 <0.0001
NYHA functional class <0.0001 <0.0001
I 558 (13) 158 (8) 407 (9) 122 (7)
II 2,024 (46) 848 (42) 1,847 (42) 600 (36)
III 1,679 (38) 919 (45) 1,837 (42) 769 (46)
IV 177 (4) 112 (6) 313 (7) 163 (10)
Heart rate, beats/min 71 � 15 73 � 14 <0.0001 74 � 16 75 � 15 0.01
Blood pressure, mm Hg
Systolic 125 � 21 129 � 22 <0.0001 128 � 22 130 � 22 0.0002
Diastolic 72 � 12 71 � 12 0.30 72 � 13 72 � 12 0.28
Pulse pressure, mm Hg 53 � 17 58 � 19 <0.0001 56 � 18 58 � 18 <0.0001
Mean arterial pressure, mm Hg 90 � 13 91 � 13 <0.0001 91 � 14 91 � 14 0.20
Previous or present disease
Hypertension 2,494 (44) 1,570 (59) <0.0001 2,903 (46) 1,378 (59) <0.0001
Atrial fibrillation 2,253 (39) 987 (36) 0.02 2,955 (46) 1,062 (44) 0.17
Pulmonary disease 892 (15) 432 (16) 0.50 1,266 (20) 481 (21) 0.50
Valvular heart disease 1,041 (18) 429 (16) 0.008 1,372 (22) 444 (20) 0.008
Idiopathic dilated cardiomyopathy 378 (7) 172 (7) 0.71 422 (7) 153 (7) 0.79
Previous interventions
Valvular surgery 527 (9) 226 (8) 0.21 182 (3) 60 (2) 0.39
Left ventricular function (echocardiography) 0.04 0.046
EF $50% 774 (14) 396 (16) 1,091 (21) 383 (19)
EF 40%–49% 1,307 (25) 544 (22) 1,094 (21) 444 (22)
EF 30%–39% 1,762 (33) 840 (33) 1,546 (29) 560 (28)
EF <30% 1,502 (28) 732 (29) 1,536 (29) 643 (32)
Continued on the next page
Johansson et al. J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6
Diabetes, Heart Failure, and Ischemic Heart Disease S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6
1410
IHD patients without previous revascularization(HR: 1.45; 95% CI: 1.33 to 1.56).
Among patients with T2DM and IHD, previousrevascularization was associated with a decreasedmortality risk compared with T2DM patientswithout a history of any coronary intervention(adjusted HR: 0.82; 95% CI: 0.75 to 0.91). This as-sociation remained after adjustment for the pro-pensity score of previous revascularization (HR:0.87; 95% CI: 0.78 to 0.96). Likewise, previousrevascularization was associated with better prog-nosis within the non-T2DM cohort (adjusted HR:0.89; 95% CI: 0.83 to 0.96).
DISCUSSION
There are 3 findings of major importance in this studyof a large, contemporary HF population representingpatients receiving typical (“everyday”) clinical care.First, T2DM is associated with higher all-cause mor-tality, regardless of whether HF is of ischemic ornonischemic origin. In addition, previous revascu-larization was associated with improved survival,which highlights how important it is to alwaysconsider the possibility of a coronary intervention inpatients with T2DM and IHD. Finally, the vast ma-jority of patients with T2DM and HF of nonischemic

TABLE 3 Continued
IHD: Revascularization IHD: No Revascularization
No T2DM(n ¼ 5,871; 68%)
T2DM(n ¼ 2,768; 32%) p Value
No T2DM(n ¼ 6,466; 73%)
T2DM(n ¼ 2,414; 27%) p Value
Laboratory analyses
Hb, g/l 131 � 17 127 � 17 <0.0001 129 � 17 127 � 17 <0.0001
Creatinine, mmol/l 112 � 59 126 � 70 <0.0001 117 � 63 129 � 77 <0.0001
eGFR, ml/min/1.73 m2 62 � 27 56 � 24 <0.0001 56 � 24 53 � 29 <0.0001
eGFR class, ml/min/1.73 m2 <0.0001 <0.0001
<30 421 (7) 380 (14) 786 (12) 422 (17)
30–59 2,510 (43) 1,253 (45) 3,162 (49) 1,179 (49)
60–89 2,301 (39) 899 (32) 2,066 (32) 639 (26)
>90 639 (11) 236 (9) 452 (7) 174 (7)
Cholesterol, mmol/l 4.3 � 1.1 4.0 � 1.1 <0.0001 4.5 � 1.2 4.3 � 1.3 0.008
LDL, mmol/l 2.5 � 1.0 2.2 � 0.9 <0.0001 2.7 � 1.0 2.4 � 1.1 <0.0001
HbA1c, mmol/mol 41 � 9 59 � 16 <0.0001 42 � 10 58 � 15 <0.0001
BNP, pg/ml 846 � 1313 982 � 2,562 0.92* 1,051 � 1,642 1,241 � 1,560 0.02*
NT-pro-BNP, pg/ml 5,213 � 7,454 5,552 � 7,550 0.32* 7,208 � 9,199 6,956 � 9,119 0.47*
Pharmacological and device intervention
RAA inhibition
ACEI 3,895 (67) 1,677 (61) <0.0001 3,763 (59) 1,463 (61) 0.05
ARB 1,304 (23) 830 (30) <0.0001 1,039 (16) 521 (22) <0.0001
ACEI or ARB 5,091 (87) 2,412 (87) 0.58 4,720 (73) 1,932 (80) <0.0001
MRA 1,602 (27) 886 (32) <0.0001 1,721 (27) 725 (30) 0.001
BB 5,244 (90) 2,484 (90) 0.69 5,378 (84) 2,049 (85) 0.04
ACEI/ARB þ BB 4,623 (79) 2,205 (80) 0.33 4,103 (63) 1,704 (71) <0.0001
ACEI/ARB þ BB þ MRA 1,290 (22) 737 (27) <0.0001 1,107 (17) 535 (22) <0.0001
Diuretic agents (loop/thiazide) 4,287 (73) 2,391 (87) <0.0001 5,390 (84) 2,162 (90) <0.0001
Digitalis 694 (12) 344 (13) 0.44 1,020 (16) 391 (16) 0.62
Statins 4,431 (76) 2,151 (78) 0.03 2,772 (43) 1,302 (54) <0.0001
Nitrates (long-lasting) 1,495 (26) 880 (32) <0.0001 1,960 (31) 836 (35) <0.0001
Antithrombotic agent 1,900 (33) 856 (31) 0.17 1,791 (28) 682 (29) 0.58
Aspirin 4,280 (73) 2,047 (74) 0.38 4,192 (65) 1,605 (67) 0.14
Device therapy 0.07 0.25
Pacemaker 563 (10) 250 (9) 684 (11) 232 (10)
Cardiac resynchronization therapy 110 (2) 41 (1.5) 57 (0.8) 31 (1.3)
Implantable cardioverter-defibrillator 291 (5) 120 (4.8) 97 (1.5) 42 (1.8)
Values are mean � SD, n (%),or %. Percentages were computed by group. Pearson chi-square test and Student t test were used for unpaired groups. *Logarithmically transformed before Student t test.
IHD ¼ ischemic heart disease; other abbreviations as in Table 1.
J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6 Johansson et al.S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6 Diabetes, Heart Failure, and Ischemic Heart Disease
1411
origin have 1 or more manageable comorbiditiesknown to cause or influence HF.
There are 2 reasonable explanations for the lowuse of revascularization in patients with T2DM. Oneis that the risk of this intervention might have beenconsidered high because of the large comorbidityburden, and another is that T2DM often causes amore diffuse atherosclerosis with challenging coro-nary artery stenoses, which lessens the opportunityor even willingness to perform a PCI or CABG. Still,it is unlikely that these conditions can explain aproportion as large as 50% of eligible patients, thatis, patients with T2DM with HF of ischemic origin.Some discrepancy exists in the evidence thatsupports revascularization as a tool to improveprognosis in T2DM and coronary artery disease.
The BARI 2D (Bypass Angioplasty RevascularizationInvestigation 2 Diabetes) trial failed to show anysurvival benefit through revascularization comparedwith optimal medical therapy in patients with T2DMand coronary artery disease (16). These findings,however, should be interpreted bearing in mindthat all patients had undergone coronary angiog-raphy before inclusion. Those who fulfilled pre-vailing criteria for immediate revascularization wereexcluded, which left only those with mild to mod-erate disease eligible for BARI 2D. In addition, theneutral results might have been driven by a 49%crossover frequency from medical therapy torevascularization during the study period.Convincing evidence favoring revascularization toimprove prognosis in patients with T2DM and acute

FIGURE 2 Crude Survival Curves Stratified By T2DM and IHD
IHD yes/no & T2DM yes/no1.0
0.8
0.6
0.4
0.2
00 2 4 6
Follow-Up (Years)
Surv
ival
Pro
babi
lity
ClassNo T2DM, IHDNo T2DM, No IHDT2DM, IHDT2DM, No IHD
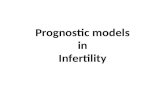
Events n (%)5 443 (43%)4 751 (34%)2 666 (50%)1 284 (40%)
No T2DM, No IHD
No T2DM, IHDT2DM, No IHD
T2DM, IHD
Number at riskNo T2DM, IHD
No T2DM, No IHDT2DM, IHD
T2DM, No IHD
125741402953173243
5791694323911565
21582535845499
537688183119
Long-term prognosis was evaluated with survival curves among patients with and without
type 2 diabetes mellitus (T2DM) and with and without ischemic heart disease (IHD). The
most serious prognosis was seen in patients with IHD and T2DM. T2DM independently
predicted mortality regardless of the presence or absence of IHD (unadjusted hazard ratio
[HR]: 1.20; 95% confidence interval [CI]: 1.14 to 1.25 and HR: 1.21; 95% CI: 1.14 to 1.29,
respectively) and remained a mortality predictor both in patients with and in those without
IHD after adjustment for age (HR: 1.40; 95% CI: 1.33 to 1.46 and HR: 1.30; 95% CI: 1.22 to
1.39, respectively).
Johansson et al. J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6
Diabetes, Heart Failure, and Ischemic Heart Disease S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6
1412
coronary syndromes and multivessel disease isprovided by the FRISC II (Fragmin and Fast Revas-cularization During Instability in Coronary ArteryDisease) and FREEDOM (Future RevascularizationEvaluation in Patients With Diabetes Mellitus:Optional Management of Multivessel Disease) trials(17,18), although neither of these trials addressedthe outcome of revascularization specifically inrelation to the presence of HF. With regard to HF ingeneral, a meta-analysis of 3,088 patients with leftventricular dysfunction and signs of preservedmyocardial viability found a strong association be-tween revascularization and survival (19). Unfortu-nately, this analysis did not report on theproportion of patients with diabetes. On the basis ofgeneral knowledge of T2DM prevalence in a popu-lation with coronary artery disease, it can beassumed that at least 20% to 30% of the studiedpopulation could have this disease (20,21). Theconcept of revascularization in patients with estab-lished HF has been challenged by the results of theSTICH (Surgical Treatment for Ischemic Heart Fail-ure) trial, which randomized 1,212 patients with IHDand left ventricular dysfunction to optimal medical
therapy alone or optimal medical therapy plusCABG. Unexpectedly, there was no difference in all-cause mortality (22), but as emphasized, there areseveral critical issues related to this trial (23). Oneimportant limitation is the considerable proportionof medically treated patients who crossed over torevascularization during the 5 years of follow-up.That this undermined the power of the observa-tions is highlighted by a renewed as-treated ratherthan intention-to-treat analysis of the STICH data-base, which showed that CABG reduced mortalitycompared with medical therapy alone (24). Indeed,a recently published 10-year follow-up of the STICHstudy (STICHES [STICH Extension Study]) foundCABG to be significantly superior to medical therapyalone when analyzed according to intention to treat,which provides a strong evidence base for thebenefits of such intervention in HF (25). In addition,the results of 2 studies that applied propensityscore analyses strengthened the benefit of CABGover medical therapy in patients with IHD and leftventricular dysfunction (26,27). Nonetheless, thereis a gap in knowledge concerning demand for pro-spective clinical trials to assess myocardial viabilitywith cardiac magnetic resonance imaging or posi-tron emission tomography and the actual impact ofrevascularization in patients with T2DM andischemic HF (14,28). It is hoped that the ongoingREVIVED (Revascularization for Ischemic Ventricu-lar Dysfunction) trial studying the efficacy andsafety of PCI in systolic HF will provide further in-sights in this field. Until results from this andsimilar trials are available, even a cautious inter-pretation of the present observational analysis of alarge HF population underscores the potentialbenefit of revascularization and the need to at leastoffer all patients a thorough investigation by meansof coronary angiography or computed tomographyangiography.
The finding that the vast majority (z90%) ofpatients with T2DM and HF of nonischemic originhad at least 1 comorbidity known to cause HF hasimportant clinical implications. These comorbiditiesincluded hypertension, atrial fibrillation, pulmonarydisease, and valvular heart disease, all conditionslargely manageable with well-established therapeu-tic or preventive strategies. Taking into consider-ation all T2DM patients in the present contemporaryHF population leaves only 7% to 10% of themwithout a reasonable pathogenesis. This makes ittempting to question the existence of a pure dia-betes cardiomyopathy that by definition requiressigns of left ventricular dysfunction in patients withT2DM without any obvious cause of the condition,

CENTRAL ILLUSTRATION Prognostic Implications of T2DM in IHD and Nonischemic HF and the Role ofPrevious Revascularization
Johansson, I. et al. J Am Coll Cardiol. 2016;68(13):1404–16.
Insights from the Swedish Heart Failure Registry (SwedeHF). In this study of a large heart failure (HF) population representing everyday clinical care, type 2
diabetes mellitus (T2DM) was associated with higher all-cause mortality, regardless of whether HF was of ischemic or nonischemic origin. The presence of
ischemic heart disease (IHD) was associated with the worst prognosis (left). In ischemic HF, previous revascularization (RV) was associated with improved
survival (right), which highlights the importance of always considering the possibility of a coronary intervention in patients with T2DM and IHD.
J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6 Johansson et al.S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6 Diabetes, Heart Failure, and Ischemic Heart Disease
1413
such as coronary artery disease, hypertension, orvalvular heart disease (29). Previous data reportedon deranged myocardial metabolism in HF relatedto T2DM with increased myocardial energy produc-tion via beta oxidation of free fatty acids (6). Morecurrent studies, using modern imaging methods,have reported on structural changes in themyocardial tissue of HF patients, with increaseddiffuse fibrosis enhancing myocardial stiffness andcompromising relaxation (6,30). These changesmight be more frequent in patients with diabetes asa consequence of high glucose and possibly alsohigh insulin levels; however, they could also beexplained by long-standing, poorly controlled hy-pertension or merely a result of aging. Anotherassumption behind the increased HF prevalence andpoor prognosis in patients with T2DM is that thegroup judged clinically to have nonischemic HFmight have a compromised myocardial functionsecondary to silent ischemia or atherosclerosis insmall vessels, causing hibernation or stunning, aswell as scar tissue resulting from silent MIs. Someobservational studies report that undiagnosed
ischemia is more common among patients withdiabetes than among those without and that it hasadverse prognostic implications (31,32). Further ev-idence for these pathogenic conditions is not pro-vided by the present investigation, which is onlyable to indicate opportunities for further studies.These investigations need to apply advanced imag-ing methods to well-defined diabetes populations tofurther enhance potential mechanisms for prevent-ing or treating HF, thereby improving the dismalprognosis in patients with the combination of T2DMand HF.
Lastly, to put our observations in the context oflarge clinical trials, compared with the placebo-treated group in a recent outcome trial focused onischemic HF in patients with T2DM, the EMPA-REGtrial (Empagliflozin Cardiovascular Outcome EventTrial in Type 2 Diabetes Mellitus Patients) (33), mor-tality in patients with T2DM and ischemic HFthroughout the trial period and median follow-up ofalmost 2 years was considerably higher in the presentstudy (50%) than in the EMPA-REG trial population(15%). Although such comparison must be made with

FIGURE 3 Crude Survival Curves in HF Patients With IHD Stratified By
Revascularization History and T2DM
Revascularization yes/no, T2DM yes/no1.0
0.8
0.6
0.4
0.2
00 2 4 6
Follow-Up (Years)
Surv
ival
Pro
babi
lity
ClassNo T2DM, RVNo T2DM, No RVT2DM, RVT2DM, No RV
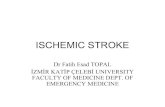
Events n (%)2 064 (34%)3 379 (52%)1 267 (44%)1 399 (58%)
Number at riskNo T2DM, RV
T2DM, RVNo T2DM, No RV
T2DM, No RV
5871276864662414
299513642710977
1183505937329
30610722475
No T2DM, RV
No T2DM, No RVT2DM, RV
T2DM, No RV
The prognostic impact of revascularization (RV) and type 2 diabetes mellitus (TD2M) in
patients with ischemic heart disease (IHD) was estimated in survival curves. Patients with
T2DM without previous revascularization had the worst outlook. Previous revascularization
was associated with a decreased mortality risk in T2DM patients compared with T2DM
patients without previous revascularization (hazard ratio [HR]: 0.82; 95% confidence in-
terval [CI]: 0.75 to 0.91) after adjustment for demographics, comorbidities, and pharma-
cological treatment. This association remained after the addition of the propensity score of
previous revascularization as a covariate in the adjusted model (HR: 0.87; 95% CI: 0.78 to
0.96). Likewise, previous revascularization was associated with better prognosis within the
non-T2DM cohort (adjusted HR: 0.89; 95% CI: 0.83 to 0.96).
Johansson et al. J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6
Diabetes, Heart Failure, and Ischemic Heart Disease S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6
1414
great caution because of obvious selection biases inthe trial participants (e.g., younger, fewer comorbid-ities), it underlines the serious prognosis in aneveryday population with T2DM and ischemic HF.
STUDY STRENGTHS AND LIMITATIONS. The majorstrength of the present report is the size and unse-lected nature of the population, which reflectscontemporary, everyday clinical practice. One
TABLE 4 Unadjusted and Adjusted HRs of Mortality by T2DM Status
Study Group: T2DM (Yes vs. No)
No IHD
n HR (95% CI) n
Unadjusted 17,272 1.21 (1.14–1.29) 17,891 1
Adjusted for age 17,272 1.30 (1.22–1.39) 17,891 1
Adjusted model 1 12,562 1.30 (1.20–1.41) 13,007
Adjusted model 2 9,193 1.21 (1.09–1.34) 9,183 1
Model 1: Adjusted for T2DM, age, sex, level of care, weight, systolic and diastolic blood ppulmonary disease, ACEI, ARB, MRA, beta blockers, diuretics, statins, nitrates, aspirin, anclass.
CI ¼ confidence interval; HR ¼ hazard ratio; other abbreviations as in Tables 1 to 3.
limitation with registry data is the possibility ofvarying diagnostic criteria. The registry defines thedifferent variables, but they have not been validatedin any detail. The proportion with T2DM is probablyan underestimation, because undiagnosed diabetes iscommon in populations with cardiovascular diseases(20,34). With regard to IHD in SwedeHF, the defini-tion was expanded in an attempt to cover as manypatients as possible (Figure 1), but information onpatient history at the time of inclusion was sometimesincomplete. In addition, no information was availableregarding silent angina, which raises the possibility ofmisclassification of IHD. This also applies to revascu-larization, and because it was retrospectivelycollected and not randomized, the assumptions maderegarding this treatment should be seen as hypothesisgenerating rather than representing facts. However,the large database allowed for extensive adjustmentof clinically relevant confounders when evaluatingthe outcome. Further on the adjustment, the appli-cation of a propensity score for treatment bias (whichto some degree mimics a randomization) strength-ened the assumptions of the benefits of revasculari-zation. It should be acknowledged that smalldifferences detected in the descriptive analyses be-tween different groups become statistically signifi-cant because of the large sample size. These statisticalsignificances might not always be of clinical rele-vance, and this necessitates a cautious interpretationof the data. Because of missing data on importantdiabetes variables, including hemoglobin A1c, it wasnot possible to extend prognostic analyses related todifferent levels of glucose control. Moreover, we didnot have details about diabetes duration or classes ofglucose-lowering therapy, factors with known prog-nostic implications. A median follow-up of 1.9 yearsmight appear short, but it is mainly an effect of alarger proportion being included during the mostrecent period and that the follow-up period wasgenerally fairly long.
in Groups Stratified by History of IHD and Revascularization
IHD IHD: Revascularization IHD: No Revascularization
HR (95% CI) n HR (95% CI) n HR (95% CI)
.20 (1.14–1.25) 8,639 1.37 (1.28–1.47) 8,880 1.14 (1.07–1.21)
.40 (1.33–1.46) 8,639 1.50 (1.39–1.61) 8,880 1.34 (1.26–1.43)
1.41 (1.33–1.50) 6,755 1.36 (1.24–1.48) 6,252 1.45 (1.33–1.56)
.34 (1.24–1.44) 4,914 1.28 (1.15–1.43) 4,160 1.43 (1.29–1.59)
ressure, duration of HF, EF class, Hb class, eGFR class, hypertension, atrial fibrillation,d anticoagulants. Model 2: Adjusted for model 1 plus heart rate and NYHA functional

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: T2DM is associ-
ated with a higher risk of mortality in patients with HF, whether
of ischemic or nonischemic origin. In patients with T2DM and
ischemic HF, previous revascularization is associated with
improved prognosis compared with patients without revascu-
larization. Most patients with nonischemic HF have other
comorbidities associated with HF.
TRANSLATIONAL OUTLOOK: Randomized trials are needed
to validate these observational data and confirm the impact of
revascularization in patients with T2DM and ischemic HF.
J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6 Johansson et al.S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6 Diabetes, Heart Failure, and Ischemic Heart Disease
1415
CONCLUSIONS
In a contemporary setting, almost 90% of HF patientswith T2DM have an accompanying risk factor that cancontribute to HF development, among which IHD isthe most common. The presence of IHD was associ-ated with the worst prognosis, which was, however,less severe if revascularization had been performedpreviously.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Isabelle Johansson, Cardiology Unit, Department ofMedicine, N3:06, Karolinska University HospitalSolna, SE-171 76 Stockholm, Sweden. E-mail: [email protected].
RE F E RENCE S
1. International Diabetes Federation. IDF DiabetesAtlas. Brussels, Belgium; 2013. Available at:http://www.idf.org/diabetesatlas. Accessed May15, 2016.
2. Olafsdottir E, Aspelund T, Sigurdsson G, et al.Similar decline in mortality rate of older personswith and without type 2 diabetes between 1993and 2004: the Icelandic population-based Rey-kjavik and AGES-Reykjavik cohort studies. BMCPublic Health 2013;13:36.
3. Lipscombe LL, Hux JE. Trends in diabetesprevalence, incidence, and mortality in Ontario,Canada 1995-2005: a population-based study.Lancet 2007;369:750–6.
4. McMurray JJ, Gerstein HC, Holman RR,Pfeffer MA. Heart failure: a cardiovascularoutcome in diabetes that can no longer beignored. Lancet Diabetes Endocrinol 2014;2:843–51.
5. Johansson I, Edner M, Dahlström U, Näsman P,Rydén L, Norhammar A. Is the prognosis in pa-tients with diabetes and heart failure a matter ofunsatisfactory management? An observationalstudy from the Swedish Heart Failure Registry. EurJ Heart Fail 2014;16:409–18.
6. Bugger H, Abel ED. Molecular mechanisms ofdiabetic cardiomyopathy. Diabetologia 2014;57:660–71.
7. Dries DL, Sweitzer NK, Drazner MH,Stevenson LW, Gersh BJ. Prognostic impact ofdiabetes mellitus in patients with heart failureaccording to the etiology of left ventricular sys-tolic dysfunction. J Am Coll Cardiol 2001;38:421–8.
8. Domanski M, Krause-Steinrauf H, Deedwania P,et al., BEST Investigators. The effect of diabeteson outcomes of patients with advanced heartfailure in the BEST trial. J Am Coll Cardiol 2003;42:914–22.
9. De Groote P, Lamblin N, Mouquet F, et al.Impact of diabetes mellitus on long-term survivalin patients with congestive heart failure. Eur HeartJ 2004;25:656–62.
10. Cubbon RM, Adams B, Rajwani A, et al. Diabetesmellitus is associated with adverse prognosis inchronicheart failureof ischaemic andnon-ischaemicaetiology. Diab Vasc Dis Res 2013;10:330–6.
11. Varela-Roman A, Shamagian LG, Caballero EB,et al. Influence of diabetes on the survival of pa-tients hospitalized with heart failure: a 12-yearstudy. Eur J Heart Fail 2005;7:859–64.
12. Jonsson A, Edner M, Alehagen U, Dahlström U.Heart failure registry: a valuable tool forimproving the management of patients with heartfailure. Eur J Heart Fail 2010;12:25–31.
13. Swedish Heart Failure Registry (RiksSvikt)website. Available at: http://www.ucr.uu.se/rikssvikt-en/. Accessed January 11, 2016.
14. Kolh P, Windecker S, Alfonso F, et al. 2014ESC/EACTS guidelines on myocardial revasculari-zation: the Task Force on Myocardial Revasculari-zation of the European Society of Cardiology (ESC)and the European Association for Cardio-ThoracicSurgery (EACTS): developed with the specialcontribution of the European Association ofPercutaneous Cardiovascular Interventions(EAPCI). Eur J Cardiothorac Surg 2014;46:517–92.
15. Rosenbaum PR, Rubin DB. The central role ofthe propensity score in observational studies forcausal effects. Biometrika 1983;70:41–55.
16. Frye RL, August P, Brooks MM, et al., BARI 2DStudy Group. A randomized trial of therapies fortype 2 diabetes and coronary artery disease.N Engl J Med 2009;360:2503–15.
17. Norhammar A, Malmberg K, Diderholm E, et al.Diabetes mellitus: the major risk factor in unstablecoronary artery disease even after consideration ofthe extent of coronary artery disease and benefitsof revascularization. J Am Coll Cardiol 2004;43:585–91.
18. Farkouh ME, Domanski M, Sleeper LA, et al.Strategies for multivessel revascularization in pa-tients with diabetes. N Engl J Med 2012;367:2375–84.
19. Allman KC, Shaw LJ, Hachamovitch R,Udelson JE. Myocardial viability testing andimpact of revascularization on prognosis in
patients with coronary artery disease and leftventricular dysfunction: a meta-analysis. J Am CollCardiol 2002;39:1151–8.
20. Norhammar A, Tenerz A, Nilsson G, et al.Glucose metabolism in patients with acutemyocardial infarction and no previous diagnosis ofdiabetes mellitus: a prospective study. Lancet2002;359:2140–4.
21. Gyberg V, De Bacquer D, Kotseva K, et al.,EUROASPIRE IV Investigators. Screening fordysglycaemia in patients with coronary arterydisease as reflected by fasting glucose, oralglucose tolerance test, and HbA1c: a report fromEUROASPIRE IV: a survey from the EuropeanSociety of Cardiology. Eur Heart J 2015;36:1171–7.
22. Velazquez EJ, Lee KL, Deja MA, et al., STICHInvestigators. Coronary-artery bypass surgery inpatients with left ventricular dysfunction. N Engl JMed 2011;364:1607–16.
23. Gurunathan S, Ahmed A, Senior R. The benefitsof revascularization in chronic heart failure. CurrHeart Fail Rep 2015;12:112–9.
24. Doenst T, Cleland JG, Rouleau JL, et al., STICHInvestigators. Influence of crossover on mortalityin a randomized study of revascularization in pa-tients with systolic heart failure and coronary ar-tery disease. Circ Heart Fail 2013;6:443–50.
25. Velazquez EJ, Lee KL, Jones RH, et al.,STICHES Investigators. Coronary-artery bypasssurgery in patients with ischemic cardiomyopathy.N Engl J Med 2016;374:1511–20.
26. Gheorghiade M, Flaherty JD, Fonarow GC,et al. Coronary artery disease, coronary revascu-larization, and outcomes in chronic advancedsystolic heart failure. Int J Cardiol 2011;151:69–75.
27. Velazquez EJ, Williams JB, Yow E, et al. Long-term survival of patients with ischemic cardiomy-opathy treated by coronary artery bypass graftingversus medical therapy. Ann Thorac Surg 2012;93:523–30.
28. Ryden L, Grant PJ, Anker SD, et al. ESCguidelines on diabetes, pre-diabetes, and cardio-vascular diseases developed in collaboration with

Johansson et al. J A C C V O L . 6 8 , N O . 1 3 , 2 0 1 6
Diabetes, Heart Failure, and Ischemic Heart Disease S E P T E M B E R 2 7 , 2 0 1 6 : 1 4 0 4 – 1 6
1416
the EASD: the Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the Eu-ropean Society of Cardiology (ESC) and developedin collaboration with the European Association forthe Study of Diabetes (EASD) [published correc-tion appears in Eur Heart J 2014;35:1824]. EurHeart J 2013;34:3035–87.
29. Schilling JD, Mann DL. Diabetic cardiomyopa-thy: bench to bedside. Heart Fail Clin 2012;8:619–31.
30. Ugander M, Oki AJ, Hsu LY, et al. Extracellularvolume imaging by magnetic resonance imagingprovides insights into overt and sub-clinicalmyocardial pathology. Eur Heart J 2012;33:1268–78.
31. Schelbert EB, Cao JJ, Sigurdsson S, et al.Prevalence and prognosis of unrecognizedmyocardial infarction determined by cardiacmagnetic resonance in older adults. JAMA 2012;308:890–6.
32. Zethelius B, Johnston N, Venge P. Troponin Ias a predictor of coronary heart disease and mor-tality in 70-year-old men: a community-basedcohort study. Circulation 2006;113:1071–8.
33. Fitchett D, Zinman B, Wanner C, et al., EMPA-REG OUTCOME Trial Investigators. Heart failureoutcomes with empagliflozin in patients with type2 diabetes at high cardiovascular risk: results ofthe EMPA-REG OUTCOME trial. Eur Heart J 2016;37:1526–34.
34. Bartnik M, Ryden L, Ferrari R, et al., Euro HeartSurvey Investigators. The prevalence of abnormalglucose regulation in patients with coronary arterydisease across Europe: the Euro Heart Survey on dia-betes and the heart. Eur Heart J 2004;25:1880–90.
KEY WORDS heart failure, ischemic heartdisease, prognosis, revascularization, type 2diabetes mellitus
APPENDIX For an expanded Methodssection, please see the online version of thisarticle.