Prognosis of intracranial dissection relates to site and presenting features
5
Clinical Study Prognosis of intracranial dissection relates to site and presenting features Simon Li a,⇑ , Bernard Yan a , Andrew Kaye b,d , Peter Mitchell c , Richard Dowling c , Marnie Collins e , Stephen Davis a a Department of Neurology, Royal Melbourne Hospital, Grattan Street, Parkville, Victoria 3050, Australia b Department of Neurosurgery, Royal Melbourne Hospital, Parkville, Victoria, Australia c Department of Radiology, Royal Melbourne Hospital, University of Melbourne, Parkville, Victoria, Australia d Neurosurgery, Academic Cluster, University of Melbourne/Royal Melbourne Hospital, Parkville, Victoria, Australia e Department of Mathematics and Statistics, Statistical Consulting Centre, University of Melbourne, Parkville, Victoria, Australia article info Article history: Received 22 December 2009 Accepted 8 November 2010 Keywords: Intracranial dissection Stroke Subarachnoid haemorrhage abstract Intracranial arterial dissection is relatively rare and generally considered to have a worse outcome than extracranial arterial dissection. It is a clinically significant entity that can cause severely disabling ischae- mic stroke or subarachnoid haemorrhage (SAH). Only a few large case series of intracranial arterial dis- section have been reported, particularly in the anterior circulation, but it is being increasingly recognized with advances in non-invasive angiographic diagnostic procedures. Patients with posterior circulation dissection appear to present more commonly with SAH and are traditionally said to have a worse out- come. Treatment options remain controversial and include medical therapy, as well as endovascular and surgical intervention. We reviewed the clinical features and outcome of 25 patients who had been treated for intracranial dissection at The Royal Melbourne Hospital over a period of 5 years. We recorded patient age, clinical presenting features, neuroimaging findings, treatment, and outcome assessment at 90 days using the modified Rankin Score (mRS). Eleven patients had anterior circulation dissection, while 14 had posterior circulation dissection; and overall 12 patients had cerebral ischaemia while 13 had sub- arachnoid haemorrhage (SAH). Almost all intracranial arterial dissections occurred spontaneously, with- out a history of trauma. Patients were relatively young, especially those in the group with ischaemia, with an average age of 39 years. Hypertension was the most commonly identified vascular risk factor. Eight out of 12 patients with ischaemia (66.7%) had anterior circulation dissection, while posterior circulation dissection occurred in 10 of 13 patients with SAH (76.9%). Location of anterior circulation dissection was variable, while the terminal vertebral artery segment was most commonly involved in the posterior cir- culation group. Most of the patients in the ischaemic group received medical therapy (n = 10/12), while 10 out of 13 (76.9%) patients with SAH underwent endovascular and/or surgical intervention. There was a trend towards more favourable outcome at 90 days (mRS P3) in the ischaemic group (n = 10/12, 83.3%) compared to the SAH group (n = 6/13, 46.2%), but this did not reach statistical significance (p value = 0.097). The mortality rate was 16.7% (n = 2/12) in the ischaemia group, and 7.7% in the SAH group (n = 1/13), not significant. Among all the ischaemic group patients who received medical therapy, there were no deaths or development of secondary intracranial bleeding complications including SAH at 90 days. Our series suggest that it is possible to divide patients with intracranial dissection into two groups: (i) an ischaemia group, associated with a more favourable clinical outcome even when treated with anti- platelet or anticoagulation therapy; or (ii) a SAH group with a less favourable prognosis. The mortality rate, especially in patients with SAH who are generally treated with endovascular and/or surgical inter- vention, is less than previously reported. Anterior circulation involvement appears more common than traditionally perceived. The spontaneous occurrence of intracranial dissection in a relatively young age group, the predominant site of dissection in the artery at some distance from its tethered proximal seg- ment, and the commonly observed hypertension, together raise the possibility of spontaneous dissection in arteries prematurely weakened by accelerated atherosclerosis. Ó 2010 Elsevier Ltd. All rights reserved. 1. Introduction Intracranial arterial dissection is traditionally perceived as rare. Most instances of cerebrovascular dissection involve the extracra- nial carotid and vertebral arteries. Case series on intracranial 0967-5868/$ - see front matter Ó 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.jocn.2010.11.006 ⇑ Corresponding author. Tel.: +61 3 9342 7000; fax: +61 3 9342 7802. E-mail address: [email protected] (S. Li). Journal of Clinical Neuroscience 18 (2011) 789–793 Contents lists available at ScienceDirect Journal of Clinical Neuroscience journal homepage: www.elsevier.com/locate/jocn
Transcript of Prognosis of intracranial dissection relates to site and presenting features

Journal of Clinical Neuroscience 18 (2011) 789–793
Contents lists available at ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Clinical Study
Prognosis of intracranial dissection relates to site and presenting features
Simon Li a,⇑, Bernard Yan a, Andrew Kaye b,d, Peter Mitchell c, Richard Dowling c, Marnie Collins e,Stephen Davis a
a Department of Neurology, Royal Melbourne Hospital, Grattan Street, Parkville, Victoria 3050, Australiab Department of Neurosurgery, Royal Melbourne Hospital, Parkville, Victoria, Australiac Department of Radiology, Royal Melbourne Hospital, University of Melbourne, Parkville, Victoria, Australiad Neurosurgery, Academic Cluster, University of Melbourne/Royal Melbourne Hospital, Parkville, Victoria, Australiae Department of Mathematics and Statistics, Statistical Consulting Centre, University of Melbourne, Parkville, Victoria, Australia
a r t i c l e i n f o a b s t r a c t
Article history:Received 22 December 2009Accepted 8 November 2010
Keywords:Intracranial dissectionStrokeSubarachnoid haemorrhage
0967-5868/$ - see front matter � 2010 Elsevier Ltd. Adoi:10.1016/j.jocn.2010.11.006
⇑ Corresponding author. Tel.: +61 3 9342 7000; faxE-mail address: [email protected] (S
Intracranial arterial dissection is relatively rare and generally considered to have a worse outcome thanextracranial arterial dissection. It is a clinically significant entity that can cause severely disabling ischae-mic stroke or subarachnoid haemorrhage (SAH). Only a few large case series of intracranial arterial dis-section have been reported, particularly in the anterior circulation, but it is being increasingly recognizedwith advances in non-invasive angiographic diagnostic procedures. Patients with posterior circulationdissection appear to present more commonly with SAH and are traditionally said to have a worse out-come. Treatment options remain controversial and include medical therapy, as well as endovascularand surgical intervention. We reviewed the clinical features and outcome of 25 patients who had beentreated for intracranial dissection at The Royal Melbourne Hospital over a period of 5 years. We recordedpatient age, clinical presenting features, neuroimaging findings, treatment, and outcome assessment at90 days using the modified Rankin Score (mRS). Eleven patients had anterior circulation dissection, while14 had posterior circulation dissection; and overall 12 patients had cerebral ischaemia while 13 had sub-arachnoid haemorrhage (SAH). Almost all intracranial arterial dissections occurred spontaneously, with-out a history of trauma. Patients were relatively young, especially those in the group with ischaemia, withan average age of 39 years. Hypertension was the most commonly identified vascular risk factor. Eightout of 12 patients with ischaemia (66.7%) had anterior circulation dissection, while posterior circulationdissection occurred in 10 of 13 patients with SAH (76.9%). Location of anterior circulation dissection wasvariable, while the terminal vertebral artery segment was most commonly involved in the posterior cir-culation group. Most of the patients in the ischaemic group received medical therapy (n = 10/12), while10 out of 13 (76.9%) patients with SAH underwent endovascular and/or surgical intervention. There was atrend towards more favourable outcome at 90 days (mRS P3) in the ischaemic group (n = 10/12, 83.3%)compared to the SAH group (n = 6/13, 46.2%), but this did not reach statistical significance (pvalue = 0.097). The mortality rate was 16.7% (n = 2/12) in the ischaemia group, and 7.7% in the SAH group(n = 1/13), not significant. Among all the ischaemic group patients who received medical therapy, therewere no deaths or development of secondary intracranial bleeding complications including SAH at 90days. Our series suggest that it is possible to divide patients with intracranial dissection into two groups:(i) an ischaemia group, associated with a more favourable clinical outcome even when treated with anti-platelet or anticoagulation therapy; or (ii) a SAH group with a less favourable prognosis. The mortalityrate, especially in patients with SAH who are generally treated with endovascular and/or surgical inter-vention, is less than previously reported. Anterior circulation involvement appears more common thantraditionally perceived. The spontaneous occurrence of intracranial dissection in a relatively young agegroup, the predominant site of dissection in the artery at some distance from its tethered proximal seg-ment, and the commonly observed hypertension, together raise the possibility of spontaneous dissectionin arteries prematurely weakened by accelerated atherosclerosis.
� 2010 Elsevier Ltd. All rights reserved.
1. Introduction
ll rights reserved.
: +61 3 9342 7802.. Li).
Intracranial arterial dissection is traditionally perceived as rare.Most instances of cerebrovascular dissection involve the extracra-nial carotid and vertebral arteries. Case series on intracranial

790 S. Li et al. / Journal of Clinical Neuroscience 18 (2011) 789–793
internal carotid artery (ICA) dissection are rare, most comprisingup to about 10 patients.1–4 Intracranial dissection is, however, aclinically significant condition that causes severely disablingischaemic stroke or subarachnoid haemorrhage (SAH), and isthought to carry a worse neurological prognosis than extracranialdissection. It has possibly been under-reported, but there is in-creased recognition with advances in non-invasive angiographicprocedures. Therapeutic options include medical therapy, endovas-cular and surgical intervention, but remain controversial withoutevidence-based guidelines.
The mean reported age of intracranial dissection is variable,ranging from the late 20s to 50s in various reports, and it also oc-curs in children.5–7 This may in part reflect the relatively few pa-tients and different geographic locations.5 It appears to be morecommon in people from Asia, and some of the largest case serieshave been reported from centres in Japan.4
Most reports are of patients with spontaneous intracranial dis-section. The reported predisposing risk factors are similar to thosefor extracranial dissection, including trauma and collagen disor-ders such as fibromuscular dysplasia, cystic medial necrosis,8
Ehlers–Danlos syndrome type IV and Marfan’s syndrome. It isuncertain whether underlying atherosclerosis, and vascular riskfactors including hypertension, smoking, diabetes mellitus, andhyperlipidaemia, are involved in the pathogenesis of dissection.There have been individual reports of intracranial dissection inthe setting of sex related headache,9,10 and in the post-partum per-iod,11 but no definite aetiology has been established in mostpatients.
Head and neck pain are the commonest symptoms, whetheranterior or posterior dissection, and in both patient groups (withor without SAH). Other features vary according to location of dis-section. For instance, diplopia and vertigo are far more commonin patients in the posterior circulation group. Presentation withSAH secondary to intracranial dissection is more commonly re-ported in the posterior circulation patients.
Neuroimaging techniques for the diagnosis of intracranial ar-tery dissection include catheter digital subtraction angiography(DSA), and less invasive modalities such as MRA and CT angiogra-phy (CTA), which are used to detect features including stenosiswith or without dilatation, presence of a false lumen or intimalflap, and intramural thrombus.12,13
Due to the rarity of intracranial dissection, there have been norandomized, controlled studies to guide treatment. This has ledto two major issues in its acute management:
(i) What are the early outcomes, and the risk of developingbleeding, including SAH, in intracranial dissection patientswith isolated cerebral ischaemia who are treated with anti-platelet and/or anticoagulation therapy?
(ii) In patients presenting with initial SAH, what are their earlyoutcomes and mortality rates, when more active treatmentoptions such as surgery and endovascular intervention arebecoming more readily available in the modern era?
We therefore reviewed 5 years’ experience from our compre-hensive stroke centre of 25 patients with intracranial dissections,and compared treatment and clinical outcomes of patients pre-senting with cerebral ischaemia and SAH.
Fig. 1. Cerebral angiogram of a vertebrobasilar intracranial dissection showing adissecting aneurysm extending from the right vertebral artery terminal segmentinto the proximal basilar artery (arrow) – stenosis with dilatation, the ‘‘pearl-and-string’’ sign.
2. Methods
2.1. Patients and inclusion criteria
We reviewed 25 patients with isolated intracranial dissectionswho were treated in the Stroke Care Unit and the Department of
Neurosurgery at our institution over 5 years (June 2003–June2008). The patients were identified from the Stroke Care Unit data-base and from the hospital medical records. Patients who fulfilledboth of the following criteria were registered in this study. The firstcriterion was sudden onset of ischaemic or haemorrhagic symp-toms. The second criterion was that cerebral angiogram (one ormore of the following: MRA, CTA, DSA) showed characteristic find-ings of arterial dissection in intracranial location(s) consistent withthe ischaemic or haemorrhagic symptoms: (i) stenosis withoutdilatation (string sign) or stenosis with dilatation (the pearl andstring sign, Fig. 1); or (ii) presence of a false lumen or an intimalflap (double lumen sign).
2.2. Data recorded
We reviewed the medical records of the 25 patients and re-corded their age, gender, clinical presenting features, predisposingfactors, vascular risk factors, neuroimaging findings and location ofthe dissection, acute medical and/or surgical and/or endovascularinterventional therapy, and clinical outcome at 90 days using themodified Rankin Score (mRS).14,15 The mRS for each patient wasestablished from the clinical assessment documented in the med-ical records by the treating neurologist or neurosurgeon. The sever-ity of SAH was graded using the Hunt and Hess scale.16 Cerebralischaemia is defined as either ischaemic stroke or transient ischae-mic attack.
2.3. Exclusion criteria
Patients with combined extracranial and intracranial dissectionwere excluded.
2.4. Comparison of clinical outcome
Clinical outcome of patients (the mRS at 90 days) was comparedbetween those in the cerebral ischaemia group and those withSAH, and also between those with anterior compared to posteriorcirculation. The results were compared using the Fisher’s exacttest, based on the dichotomization of clinical outcome into favour-able (mRS 63) or worse (mRS >3) at 90 days.
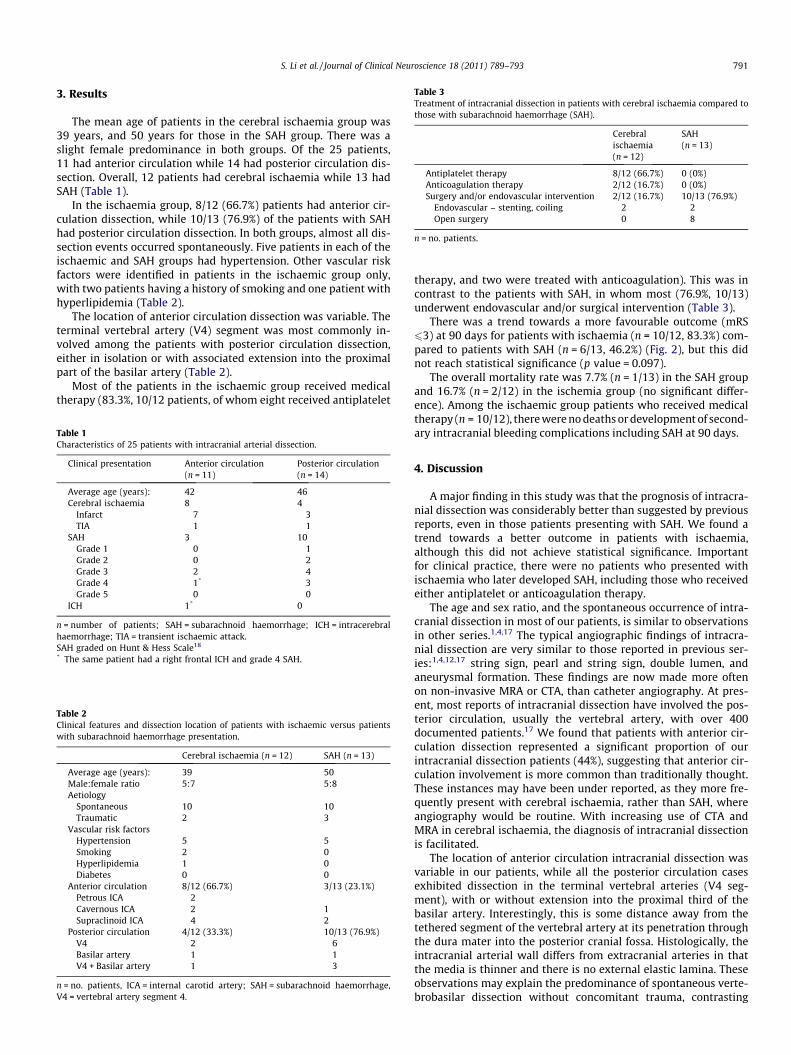
Table 3Treatment of intracranial dissection in patients with cerebral ischaemia compared tothose with subarachnoid haemorrhage (SAH).
Cerebralischaemia(n = 12)
SAH(n = 13)
Antiplatelet therapy 8/12 (66.7%) 0 (0%)Anticoagulation therapy 2/12 (16.7%) 0 (0%)Surgery and/or endovascular intervention 2/12 (16.7%) 10/13 (76.9%)
Endovascular – stenting, coiling 2 2Open surgery 0 8
n = no. patients.
S. Li et al. / Journal of Clinical Neuroscience 18 (2011) 789–793 791
3. Results
The mean age of patients in the cerebral ischaemia group was39 years, and 50 years for those in the SAH group. There was aslight female predominance in both groups. Of the 25 patients,11 had anterior circulation while 14 had posterior circulation dis-section. Overall, 12 patients had cerebral ischaemia while 13 hadSAH (Table 1).
In the ischaemia group, 8/12 (66.7%) patients had anterior cir-culation dissection, while 10/13 (76.9%) of the patients with SAHhad posterior circulation dissection. In both groups, almost all dis-section events occurred spontaneously. Five patients in each of theischaemic and SAH groups had hypertension. Other vascular riskfactors were identified in patients in the ischaemic group only,with two patients having a history of smoking and one patient withhyperlipidemia (Table 2).
The location of anterior circulation dissection was variable. Theterminal vertebral artery (V4) segment was most commonly in-volved among the patients with posterior circulation dissection,either in isolation or with associated extension into the proximalpart of the basilar artery (Table 2).
Most of the patients in the ischaemic group received medicaltherapy (83.3%, 10/12 patients, of whom eight received antiplatelet
Table 1Characteristics of 25 patients with intracranial arterial dissection.
Clinical presentation Anterior circulation(n = 11)
Posterior circulation(n = 14)
Average age (years): 42 46Cerebral ischaemia 8 4
Infarct 7 3TIA 1 1
SAH 3 10Grade 1 0 1Grade 2 0 2Grade 3 2 4Grade 4 1* 3Grade 5 0 0
ICH 1* 0
n = number of patients; SAH = subarachnoid haemorrhage; ICH = intracerebralhaemorrhage; TIA = transient ischaemic attack.SAH graded on Hunt & Hess Scale18
* The same patient had a right frontal ICH and grade 4 SAH.
Table 2Clinical features and dissection location of patients with ischaemic versus patientswith subarachnoid haemorrhage presentation.
Cerebral ischaemia (n = 12) SAH (n = 13)
Average age (years): 39 50Male:female ratio 5:7 5:8Aetiology
Spontaneous 10 10Traumatic 2 3
Vascular risk factorsHypertension 5 5Smoking 2 0Hyperlipidemia 1 0Diabetes 0 0
Anterior circulation 8/12 (66.7%) 3/13 (23.1%)Petrous ICA 2Cavernous ICA 2 1Supraclinoid ICA 4 2
Posterior circulation 4/12 (33.3%) 10/13 (76.9%)V4 2 6Basilar artery 1 1V4 + Basilar artery 1 3
n = no. patients, ICA = internal carotid artery; SAH = subarachnoid haemorrhage,V4 = vertebral artery segment 4.
therapy, and two were treated with anticoagulation). This was incontrast to the patients with SAH, in whom most (76.9%, 10/13)underwent endovascular and/or surgical intervention (Table 3).
There was a trend towards a more favourable outcome (mRS63) at 90 days for patients with ischaemia (n = 10/12, 83.3%) com-pared to patients with SAH (n = 6/13, 46.2%) (Fig. 2), but this didnot reach statistical significance (p value = 0.097).
The overall mortality rate was 7.7% (n = 1/13) in the SAH groupand 16.7% (n = 2/12) in the ischemia group (no significant differ-ence). Among the ischaemic group patients who received medicaltherapy (n = 10/12), there were no deaths or development of second-ary intracranial bleeding complications including SAH at 90 days.
4. Discussion
A major finding in this study was that the prognosis of intracra-nial dissection was considerably better than suggested by previousreports, even in those patients presenting with SAH. We found atrend towards a better outcome in patients with ischaemia,although this did not achieve statistical significance. Importantfor clinical practice, there were no patients who presented withischaemia who later developed SAH, including those who receivedeither antiplatelet or anticoagulation therapy.
The age and sex ratio, and the spontaneous occurrence of intra-cranial dissection in most of our patients, is similar to observationsin other series.1,4,17 The typical angiographic findings of intracra-nial dissection are very similar to those reported in previous ser-ies:1,4,12,17 string sign, pearl and string sign, double lumen, andaneurysmal formation. These findings are now made more oftenon non-invasive MRA or CTA, than catheter angiography. At pres-ent, most reports of intracranial dissection have involved the pos-terior circulation, usually the vertebral artery, with over 400documented patients.17 We found that patients with anterior cir-culation dissection represented a significant proportion of ourintracranial dissection patients (44%), suggesting that anterior cir-culation involvement is more common than traditionally thought.These instances may have been under reported, as they more fre-quently present with cerebral ischaemia, rather than SAH, whereangiography would be routine. With increasing use of CTA andMRA in cerebral ischaemia, the diagnosis of intracranial dissectionis facilitated.
The location of anterior circulation intracranial dissection wasvariable in our patients, while all the posterior circulation casesexhibited dissection in the terminal vertebral arteries (V4 seg-ment), with or without extension into the proximal third of thebasilar artery. Interestingly, this is some distance away from thetethered segment of the vertebral artery at its penetration throughthe dura mater into the posterior cranial fossa. Histologically, theintracranial arterial wall differs from extracranial arteries in thatthe media is thinner and there is no external elastic lamina. Theseobservations may explain the predominance of spontaneous verte-brobasilar dissection without concomitant trauma, contrasting
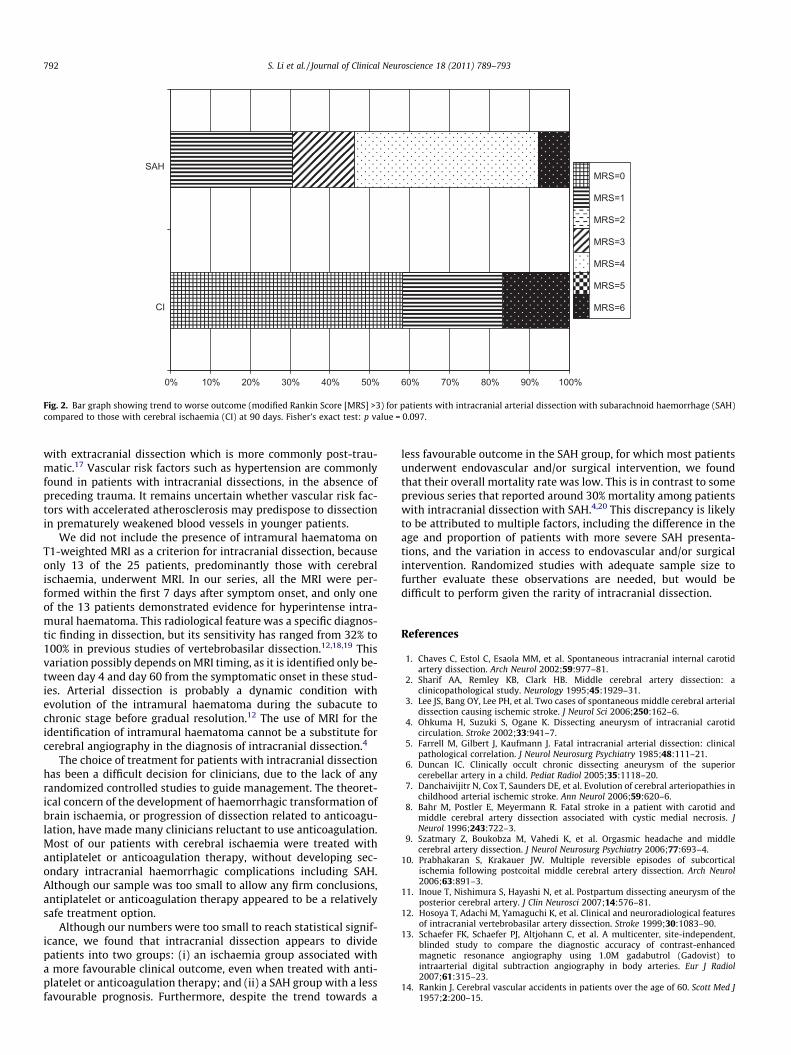
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
CI
SAHMRS=0
MRS=1
MRS=2
MRS=3
MRS=4
MRS=5
MRS=6
Fig. 2. Bar graph showing trend to worse outcome (modified Rankin Score [MRS] >3) for patients with intracranial arterial dissection with subarachnoid haemorrhage (SAH)compared to those with cerebral ischaemia (CI) at 90 days. Fisher’s exact test: p value = 0.097.
792 S. Li et al. / Journal of Clinical Neuroscience 18 (2011) 789–793
with extracranial dissection which is more commonly post-trau-matic.17 Vascular risk factors such as hypertension are commonlyfound in patients with intracranial dissections, in the absence ofpreceding trauma. It remains uncertain whether vascular risk fac-tors with accelerated atherosclerosis may predispose to dissectionin prematurely weakened blood vessels in younger patients.
We did not include the presence of intramural haematoma onT1-weighted MRI as a criterion for intracranial dissection, becauseonly 13 of the 25 patients, predominantly those with cerebralischaemia, underwent MRI. In our series, all the MRI were per-formed within the first 7 days after symptom onset, and only oneof the 13 patients demonstrated evidence for hyperintense intra-mural haematoma. This radiological feature was a specific diagnos-tic finding in dissection, but its sensitivity has ranged from 32% to100% in previous studies of vertebrobasilar dissection.12,18,19 Thisvariation possibly depends on MRI timing, as it is identified only be-tween day 4 and day 60 from the symptomatic onset in these stud-ies. Arterial dissection is probably a dynamic condition withevolution of the intramural haematoma during the subacute tochronic stage before gradual resolution.12 The use of MRI for theidentification of intramural haematoma cannot be a substitute forcerebral angiography in the diagnosis of intracranial dissection.4
The choice of treatment for patients with intracranial dissectionhas been a difficult decision for clinicians, due to the lack of anyrandomized controlled studies to guide management. The theoret-ical concern of the development of haemorrhagic transformation ofbrain ischaemia, or progression of dissection related to anticoagu-lation, have made many clinicians reluctant to use anticoagulation.Most of our patients with cerebral ischaemia were treated withantiplatelet or anticoagulation therapy, without developing sec-ondary intracranial haemorrhagic complications including SAH.Although our sample was too small to allow any firm conclusions,antiplatelet or anticoagulation therapy appeared to be a relativelysafe treatment option.
Although our numbers were too small to reach statistical signif-icance, we found that intracranial dissection appears to dividepatients into two groups: (i) an ischaemia group associated witha more favourable clinical outcome, even when treated with anti-platelet or anticoagulation therapy; and (ii) a SAH group with a lessfavourable prognosis. Furthermore, despite the trend towards a
less favourable outcome in the SAH group, for which most patientsunderwent endovascular and/or surgical intervention, we foundthat their overall mortality rate was low. This is in contrast to someprevious series that reported around 30% mortality among patientswith intracranial dissection with SAH.4,20 This discrepancy is likelyto be attributed to multiple factors, including the difference in theage and proportion of patients with more severe SAH presenta-tions, and the variation in access to endovascular and/or surgicalintervention. Randomized studies with adequate sample size tofurther evaluate these observations are needed, but would bedifficult to perform given the rarity of intracranial dissection.
References
1. Chaves C, Estol C, Esaola MM, et al. Spontaneous intracranial internal carotidartery dissection. Arch Neurol 2002;59:977–81.
2. Sharif AA, Remley KB, Clark HB. Middle cerebral artery dissection: aclinicopathological study. Neurology 1995;45:1929–31.
3. Lee JS, Bang OY, Lee PH, et al. Two cases of spontaneous middle cerebral arterialdissection causing ischemic stroke. J Neurol Sci 2006;250:162–6.
4. Ohkuma H, Suzuki S, Ogane K. Dissecting aneurysm of intracranial carotidcirculation. Stroke 2002;33:941–7.
5. Farrell M, Gilbert J, Kaufmann J. Fatal intracranial arterial dissection: clinicalpathological correlation. J Neurol Neurosurg Psychiatry 1985;48:111–21.
6. Duncan IC. Clinically occult chronic dissecting aneurysm of the superiorcerebellar artery in a child. Pediat Radiol 2005;35:1118–20.
7. Danchaivijitr N, Cox T, Saunders DE, et al. Evolution of cerebral arteriopathies inchildhood arterial ischemic stroke. Ann Neurol 2006;59:620–6.
8. Bahr M, Postler E, Meyermann R. Fatal stroke in a patient with carotid andmiddle cerebral artery dissection associated with cystic medial necrosis. JNeurol 1996;243:722–3.
9. Szatmary Z, Boukobza M, Vahedi K, et al. Orgasmic headache and middlecerebral artery dissection. J Neurol Neurosurg Psychiatry 2006;77:693–4.
10. Prabhakaran S, Krakauer JW. Multiple reversible episodes of subcorticalischemia following postcoital middle cerebral artery dissection. Arch Neurol2006;63:891–3.
11. Inoue T, Nishimura S, Hayashi N, et al. Postpartum dissecting aneurysm of theposterior cerebral artery. J Clin Neurosci 2007;14:576–81.
12. Hosoya T, Adachi M, Yamaguchi K, et al. Clinical and neuroradiological featuresof intracranial vertebrobasilar artery dissection. Stroke 1999;30:1083–90.
13. Schaefer FK, Schaefer PJ, Altjohann C, et al. A multicenter, site-independent,blinded study to compare the diagnostic accuracy of contrast-enhancedmagnetic resonance angiography using 1.0M gadabutrol (Gadovist) tointraarterial digital subtraction angiography in body arteries. Eur J Radiol2007;61:315–23.
14. Rankin J. Cerebral vascular accidents in patients over the age of 60. Scott Med J1957;2:200–15.

S. Li et al. / Journal of Clinical Neuroscience 18 (2011) 789–793 793
15. Bonita R, Beaglehole R. Recovery of motor function after stroke. Stroke1988;19:1497–500.
16. Hunt W, Hess R. Surgical risk as related to time of intervention in the repair ofintracranial aneurysms. J Neurosurg 1968;28:14–20.
17. Kocaeli H, Chaalala C, Andaluz N, et al. Spontaneous intradural vertebral arterydissection: a single center experience and review of literature. Skull Base2009;19:209–18.
18. Yoshimoto Y, Wakai S. Unruptured intracranial vertebral artery dissection:clinical course and serial radiographic imagings. Stroke 1997;28:370–4.
19. Fujiwara S, Yokoyama N, Fujii K, et al. Repeat angiography and magneticresonance imaging (MRI) of dissecting aneurysms of the intracranial vertebralartery. Acta Neurochir (Wien) 1993;121:123–9.
20. Metso T, Metso A, Helenius J, et al. Prognosis and safety of anticoagulation inintracranial artery dissections in adults. Stroke 2007;38:1837–42.