
Prof George Jelinek FACEM Consultant Physician Coroners Prevention Unit Improving recognition of...
29
Prof George Jelinek FACEM Consultant Physician Coroners Prevention Unit Improving recognition of aortic dissection: lessons learned from coronial dat
-
Upload
ethan-flynn -
Category
Documents
-
view
217 -
download
1
Transcript of Prof George Jelinek FACEM Consultant Physician Coroners Prevention Unit Improving recognition of...
Prof George Jelinek FACEMConsultant Physician
Coroners Prevention Unit
Improving recognition of aortic dissection: lessons learned from coronial data

Overview
• Coroners Court of Victoria (CCOV) overview• Coroners Prevention Unit (CPU) structure and
function– CPU data
• Aortic dissection (AD) background and coronial data
• Improving detection of AD

Coroners Court of Victoria• Structure– Recent major re-structure– State Coroner (Judge Ian Gray)
– 9 Coroners (Iain West, Heather Spooner, Peter White, Phil Byrne, Audrey Jamieson, Paresa Spanos, Jacquie Hawkins, Rosemary Carlin, Caitlin English)
– Many country coroners– All have legal qualifications (note very different from the US
Medical Examiner system)– Coroners’ solicitors– Registrars and support staff– Coroners Prevention Unit (CPU)
Coroners Prevention Unit
• Coroners Act (VIC) 2008– Major change in focus from a ‘blame’ approach to
a prevention approach– CPU began with four teams of case investigators,
including a Health and Medical Investigation Team– 2010 HMIT began with four clinicians, two nurses, two
emergency physicians– Restructured to single overall CPU investigation
unit, with three nurses, three emergency physicians examining health system related deaths
The value of emergency physicians to the coronial process
• Specialty of breadth rather than narrow focus• Interaction with most other disciplines,
community, pre-hospital, hospital, and the coronial system
• Experience of the full range of health conditions, from ambulatory to critical care in all ages
• Comfortable with making decisions

What we do
• Introduced and streamlined processes for investigating deaths related to health system– On arrival 2010, delays of up to 7 years before
case investigation finalised– Only then that some cases went to inquest– Not reasonable for families, system changes– Introduced triage system• Currently 60% of cases dealt with through short
discussion and review at triage meeting with coroner

Case investigation
• Once accepted via triage, Medical Examiners Report, medical records, family letters and other correspondence examined
• Objective to determine if opportunities for prevention, particularly with system changes– Not focused on apportioning blame, particularly to juniors– May involve requesting statements– May require expert opinion– If in the public interest, may proceed to inquest

CPU case numbers and outcomes
• Around 5,000 cases reported to the Coroner each year
• Approximately 10% referred to CPU
• CPU completes the investigation within 1 year in about 75%
• Current workload: 70 cases for health/medical investigation accepted after triage but not yet formally investigated, approximately 7 months behind

Aortic dissection
• Relatively uncommon in clinical practice but much over-represented in coronial data– Particularly unrecognised AD• Commonly patient plugged into ACS pathway• Thinking stops when ECGs and troponins normal• However, a variety of important clues to the diagnosis
– Multiple concurrent investigations and inquests into such deaths at CCOV prompted review

Classification
Any Arch = A

AHA guidelines for diagnosis 2010
• Any patient with complaints that ‘may represent acute aortic dissection’ should be evaluated to establish pre-test risk of AD:– History– Examination– Simple investigations

High risk features of historyRisk factors
• Hypertension Type A 71%, Type B 83%• Age – mean 63yo• Atherosclerosis (30%)• Known aortic aneurysm – (16%)• Marfan syndrome – younger patients (5%)• Known family history of aortic disease• Known aortic valve disease• Recent aortic manipulation – post surgery/angiogram (5%)

High risk features of historyPain
• Sudden, immediate in 90%• Severe intensity, worst ever in 90%• Classically tearing or ripping (50%), but frequently described
as sharp or stabbing (64%)• Classically ‘interscapular’ but frequently most severe pain in
anterior chest with proximal dissections (71%), posterior chest or back pain more common in Type B dissection (51%)
• Proximal dissections pain may radiate to neck, throat or jaw• Pain may migrate as dissection progresses – Type A 15%, Type
B 20%

High risk features on examination• Blood pressure on presentation
• Blood pressure difference
• Pulse deficit
• Aortic regurgitation murmur
• Stroke
Type A – 40% normal, 35% HT, 25% shockType B – 26% normal, 70% HT, 4% shock
20-50%
Type A 24%, Type B 14%
Type A 44%, Type B 12%
Type A 6%, Type B 2%

High risk features on investigationCXR
• Normal
• Widened mediastinum
• Abnormal aortic outline
• Normal or no aortic abnormality
• Any abnormality
Type A 11%, Type B 21%
Type A 63%, Type B 56%
Type A 47%, Type B 49%
35%
90%


High risk features on investigationECG
• No diagnostic changes of aortic dissection• Normal 31%• Non-specific ST-T changes in 40%• Left ventricular hypertrophy in 27%• Ischaemia Type A 17%, Type B 13%

Excluding the need for imaging
• Meta-analysis of d-dimer (< 500 ng/mL)– Sensitivity 97% (95% CI 94-99%)– Negative predictive value 96% (95% CI 93-98%)
• Conclusion: “Plasma d-dimer may thus be used to identify subjects who are unlikely to benefit from further aortic imaging”
-Shimony A, Filion KB, Mottillo S, et al. Meta-analysis of usefulness of d-dimer to diagnose acute
aortic dissection. Am J Cardiol 2011; 107: 1227-1234.

Clinical prediction• Aortic pain alone• Mediastinal widening alone• Aortic pain + mediastinal
widening• Aortic pain + BP/pulse
differentials• Aortic pain + widened
mediastinum or abnormal aortic outline + BP/pulse differentials
31% probability39% probability83% probability
92% probability
100% probability, but only present in about 30% of patients
from von Kodolitsch Y, Schwartz AG, Nienaber CA. Clinical Prediction of Acute Aortic Dissection. Arch Int Med 2000 (in those with clinical suspicion of AD)

Summary of risk assessment
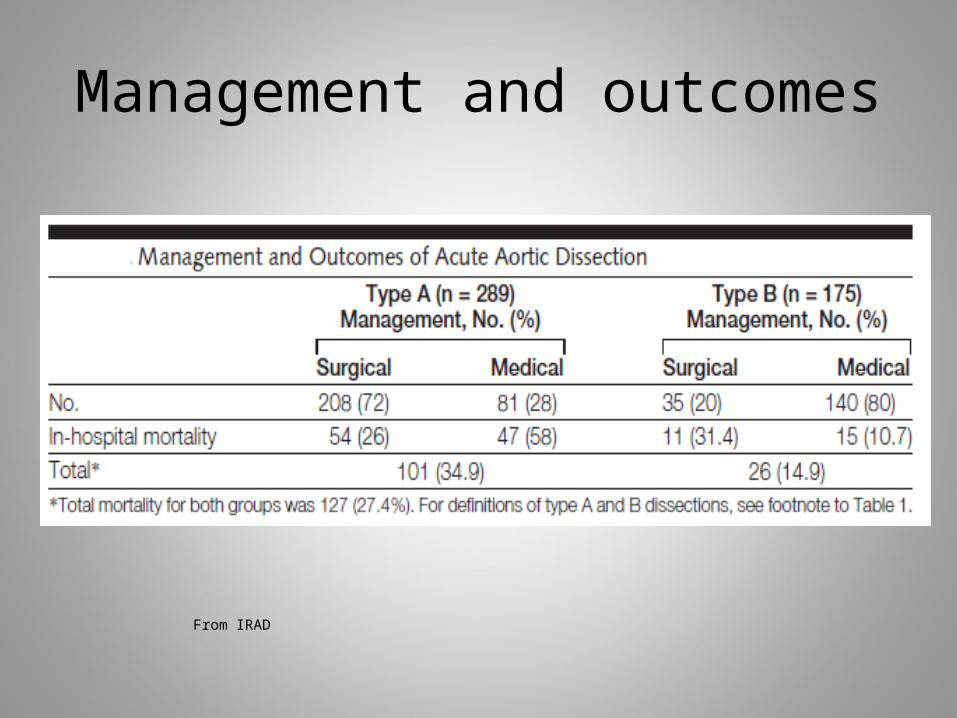
Management and outcomes
From IRAD
AD coronial numbers
• Approximately 50 deaths a year reported to CCOV with aortic dissection/thoracic aortic aneurysm in cause of death
• Cases with a prevention opportunity far fewer• 19 cases (11M, 8F; 19-79yrs) with health service
contact in previous 3 months potentially related– 2010: 4– 2011: 11– 2012: 4

Detailed review of 19 potentially preventable AD cases 2010-12
2010 2011 2012 Total Location of death ‐ At Home 3 7 2 12 ‐ Hospital 1 4 2 7
Presenting symptoms ‐ Chest pain ‐ 5 1 6 ‐ Chest pain and other 2 3 ‐ 5 ‐ Chest and back pain 2 1 ‐ 3 ‐ Other - 1 1 2 ‐ Back pain ‐ ‐ 2 2 ‐ Back pain and other ‐ 1 ‐ 1
Proximity of presentation to death ‐ Same day 1 1 ‐ 2 ‐ 1 day 1 4 1 6 ‐ 2 10 days ‐ 1 5 3 9 ‐ > 10 days 1 1 ‐ 2

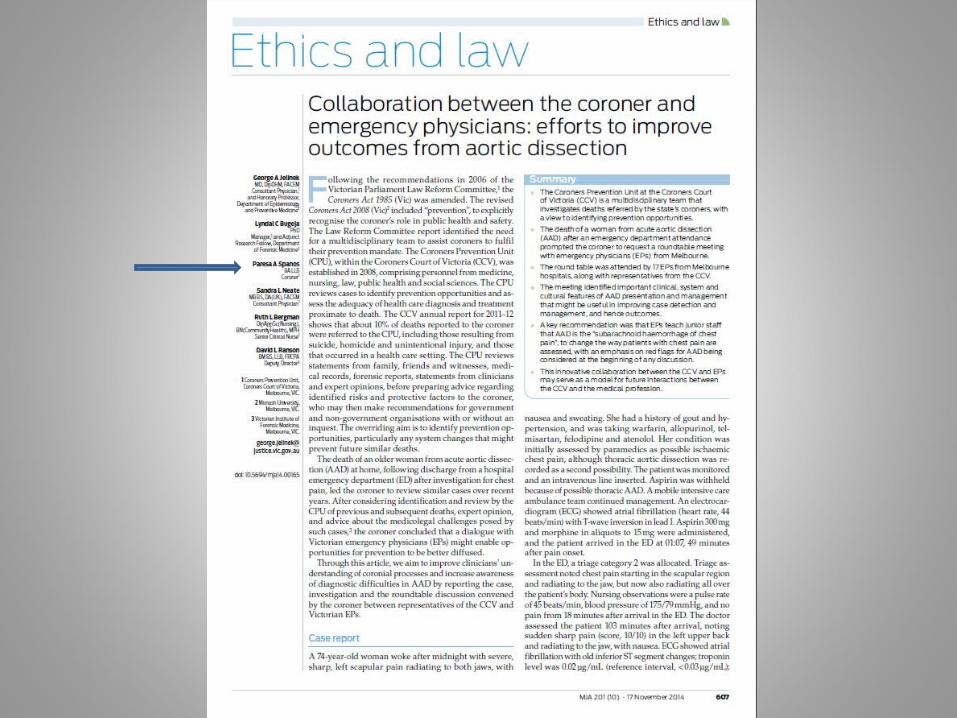
Coroners AD Round Table
– August 2013– Coroner Spanos– 17 prominent emergency physicians/Directors– 5 members of CCOV– Highly valuable meeting and discussion– Broke new ground for cooperation/consultation
between the Court and the profession

Key findings
• Importance of accurate history• Problems of following ACS pathways• Potential value of d-Dimer• Potential for an AD risk score– CALD a significant risk for missed diagnosis
• Address barriers to CT access• Need for cultural change to avoid missing

Recognising AD• First step: THINK OF IT!– Case detection improves in cluster presentations– A number of pick-ups since ECIICN talk
• Characteristics of pain, sudden onset, back• Pulse deficits, differences• Widened mediastinum (commonly dismissed
as artefact)• Neurology associated with chest pain

Changing culture
• Don’t just do something, stand there!– Contrary to much EM teaching
• AD must become the ‘sub-arachnoid’ of chest pain– “Before you present this case of chest pain, are
there any red flags for AD?”– “OK, ECGs and troponin are normal, before
discharge, have you considered AD?”
Summary
• AD very uncommon in clinical practice, but over-represented in coronial data
• Opportunity to make a difference with early detection
• Education and cultural change the keys• Coronial data can assist in changing clinical
practice


















