Prof. Franco Grego - MAC Conference 2016past.mac-conference.com/xconfig/upload/files/$03-Fr_F....
15
www.chirurgiavascolarepadova.it Prof. Franco Grego UNIVERSITY OF PADUA DEPARTMENT OF VASCULAR AND ENDOVASCULAR SURGERY Director: Prof. F. GREGO Predictors of endoleak type II risk, in the era of prevention with aneurysm sac filling during EVAR
-
Upload
phunghuong -
Category
Documents
-
view
227 -
download
1
Transcript of Prof. Franco Grego - MAC Conference 2016past.mac-conference.com/xconfig/upload/files/$03-Fr_F....
www.chirurgiavascolarepadova.it
Prof. Franco Grego
UNIVERSITY OF PADUADEPARTMENT OF VASCULAR AND ENDOVASCULAR SURGERY
Director: Prof. F. GREGO
Predictors of endoleak type II risk, in the era of prevention
with aneurysm sac fillingduring EVAR
www.chirurgiavascolarepadova.it
NO DISCLOSURE
UNIVERSITY OF PADUADEPARTMENT OF VASCULAR AND ENDOVASCULAR SURGERY
Director: Prof. F. GREGO
www.chirurgiavascolarepadova.it
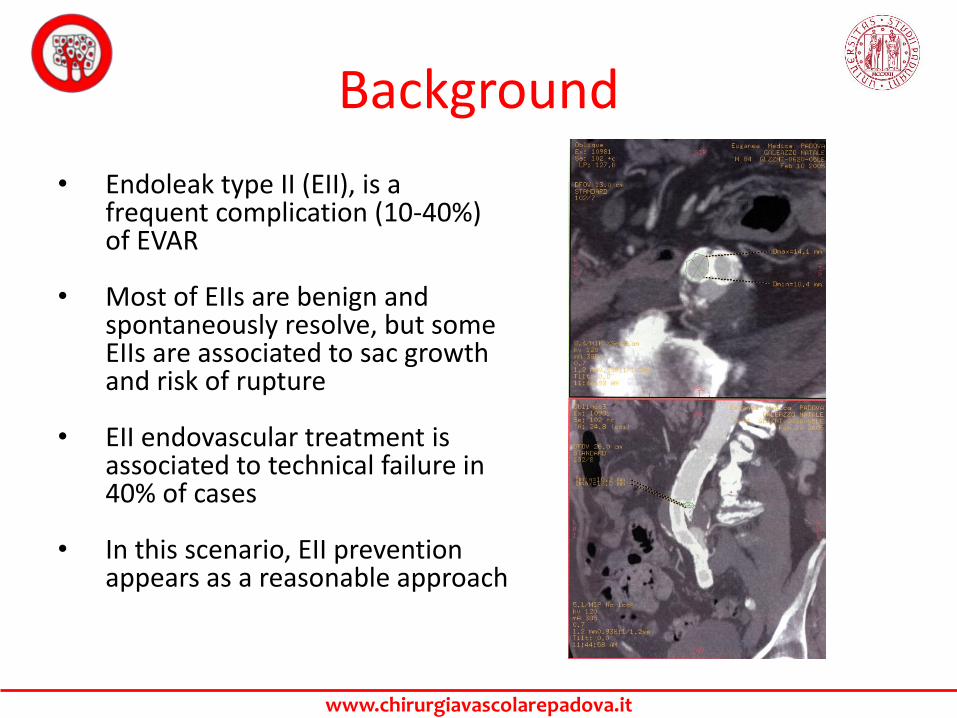
Background
• Endoleak type II (EII), is a frequent complication (10-40%) of EVAR
• Most of EIIs are benign and spontaneously resolve, but some EIIs are associated to sac growth and risk of rupture
• EII endovascular treatment is associated to technical failure in 40% of cases
• In this scenario, EII prevention appears as a reasonable approach
www.chirurgiavascolarepadova.it
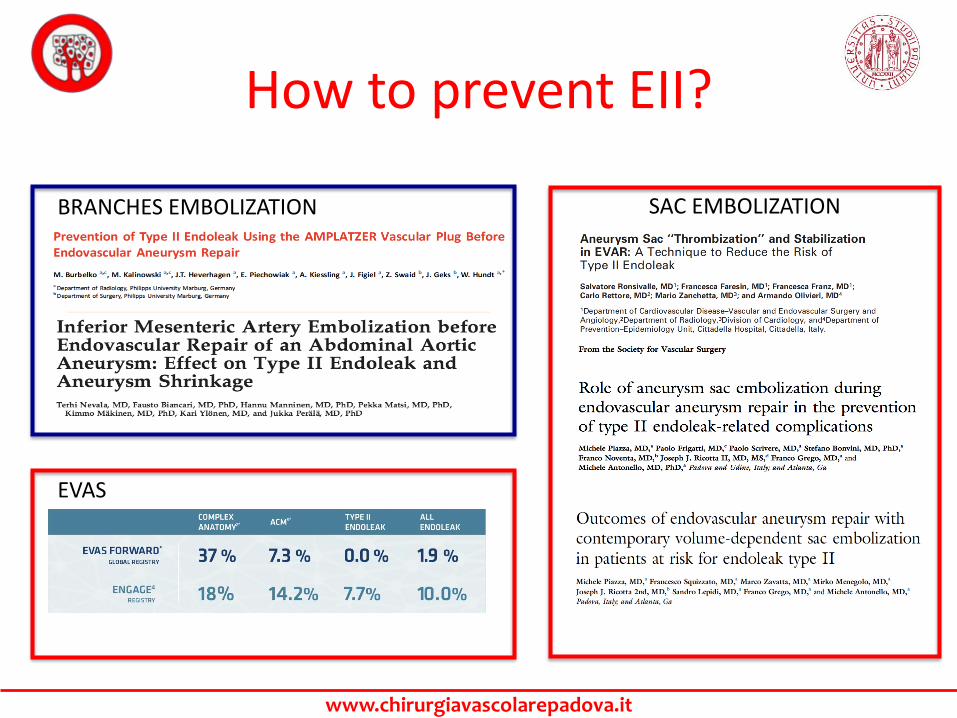
How to prevent EII?
BRANCHES EMBOLIZATION SAC EMBOLIZATION
EVAS
www.chirurgiavascolarepadova.it
When?
DURING EVAR• Exposure to a single procedure• Time-consuming compared to
standard EVAR• Technical feasibility
BEFORE EVAR• Exposure to the risks of 2
different procedures• Contrast and radiation exposure• Infection risk• Costs
www.chirurgiavascolarepadova.it
Who?All patients
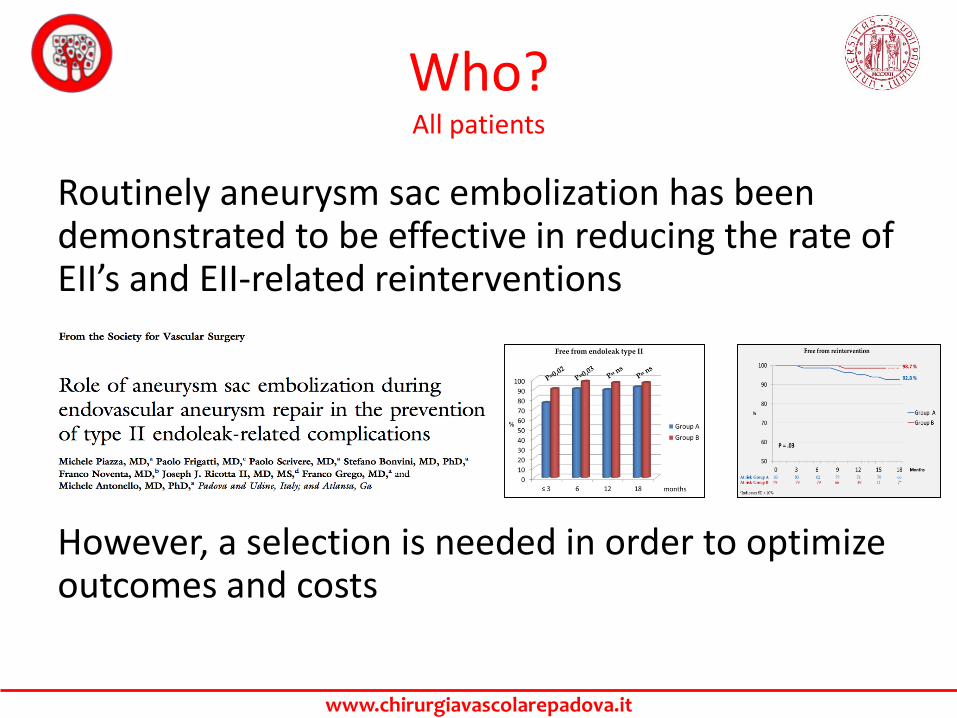
Routinely aneurysm sac embolization has been demonstrated to be effective in reducing the rate of EII’s and EII-related reinterventions
However, a selection is needed in order to optimize outcomes and costs
www.chirurgiavascolarepadova.it
Who?high risk patients
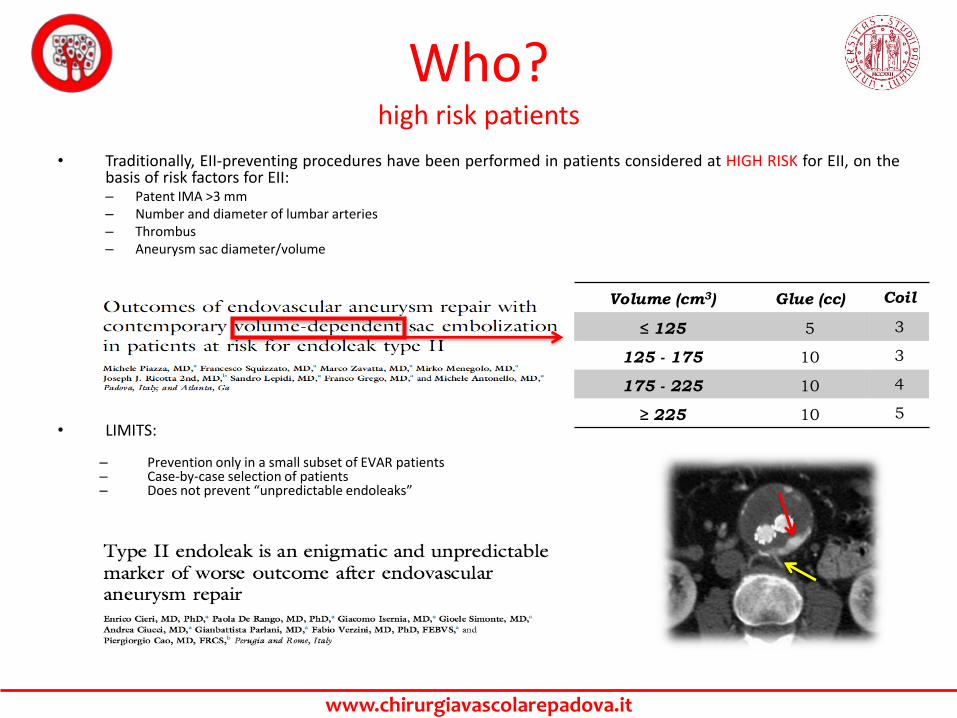
• Traditionally, EII-preventing procedures have been performed in patients considered at HIGH RISK for EII, on thebasis of risk factors for EII:– Patent IMA >3 mm– Number and diameter of lumbar arteries– Thrombus– Aneurysm sac diameter/volume
• LIMITS:
– Prevention only in a small subset of EVAR patients– Case-by-case selection of patients– Does not prevent “unpredictable endoleaks”
Volume (cm3) Glue (cc) Coil
≤ 125 5 3
125 - 175 10 3
175 - 225 10 4
≥ 225 10 5
www.chirurgiavascolarepadova.it
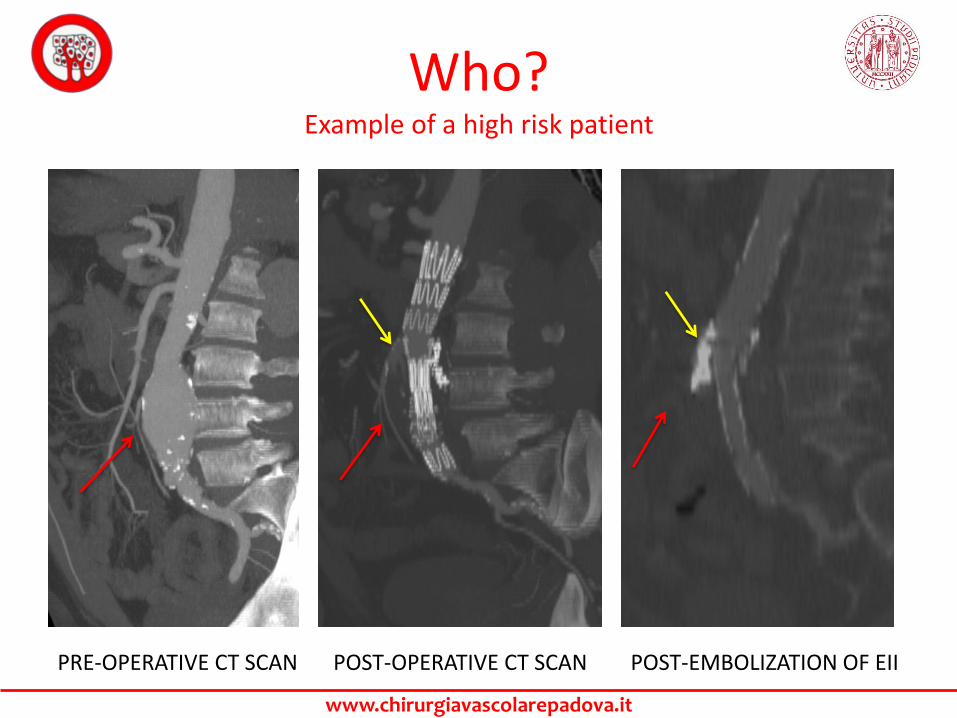
Who?Example of a high risk patient
PRE-OPERATIVE CT SCAN POST-OPERATIVE CT SCAN POST-EMBOLIZATION OF EII
www.chirurgiavascolarepadova.it
Who?Exclusion of patients at low risk
OBJECTIVES
• Reproducible, easy method of selection
• Prevention of EII’s
• Prevention of EII-related reinterventions(malignant endoleaks)
• Prevention of “unpredictable EII’s”
www.chirurgiavascolarepadova.it
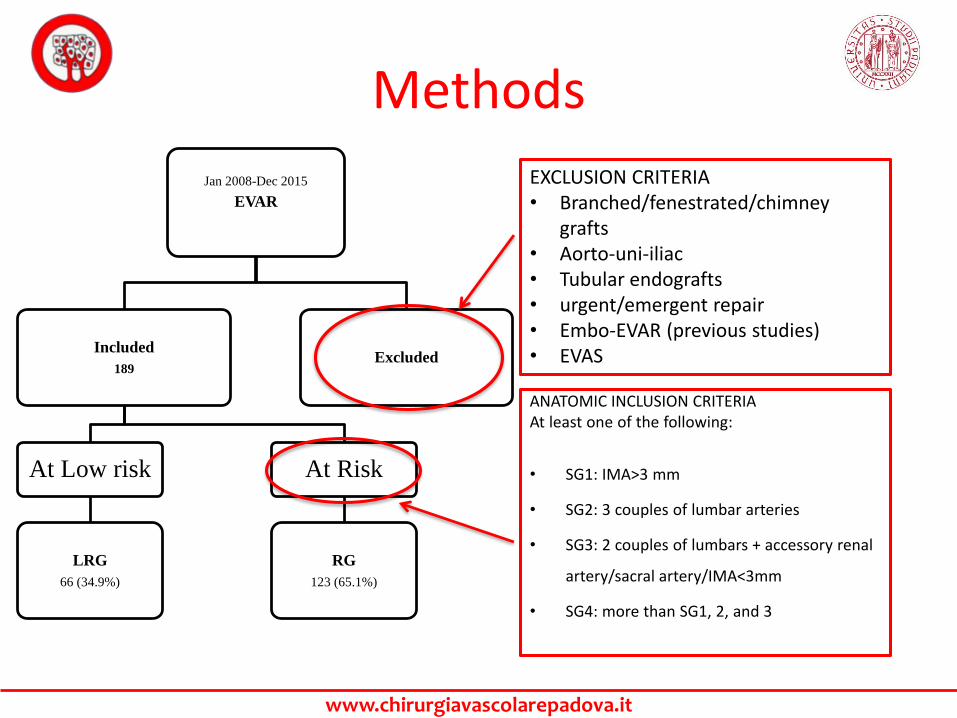
Methods
ANATOMIC INCLUSION CRITERIAAt least one of the following:
• SG1: IMA>3 mm
• SG2: 3 couples of lumbar arteries
• SG3: 2 couples of lumbars + accessory renal
artery/sacral artery/IMA<3mm
• SG4: more than SG1, 2, and 3
Jan 2008-Dec 2015
EVAR
ExcludedIncluded
189
At Low risk
LRG
66 (34.9%)
At Risk
RG
123 (65.1%)
EXCLUSION CRITERIA• Branched/fenestrated/chimney
grafts• Aorto-uni-iliac• Tubular endografts• urgent/emergent repair• Embo-EVAR (previous studies)• EVAS
www.chirurgiavascolarepadova.it
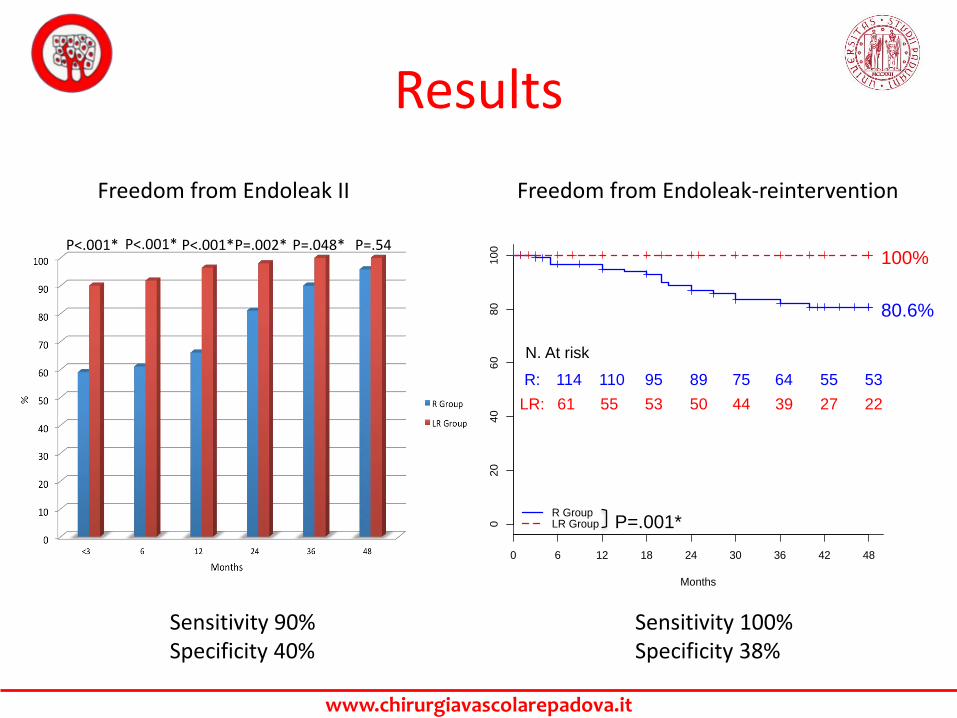
Results
P<.001* P<.001* P<.001*P=.002* P=.048*
02
04
06
080
10
0
Months
0 6 12 18 24 30 36 42 48
R GroupLR Group
80.6%
100%
N. At risk
R:
LR: 55 3950 22
110 6489 5395 75 55
61
114
53 44 27
P=.001*
P=.54
Sensitivity 90%Specificity 40%
Sensitivity 100%Specificity 38%
Freedom from Endoleak II Freedom from Endoleak-reintervention
www.chirurgiavascolarepadova.it
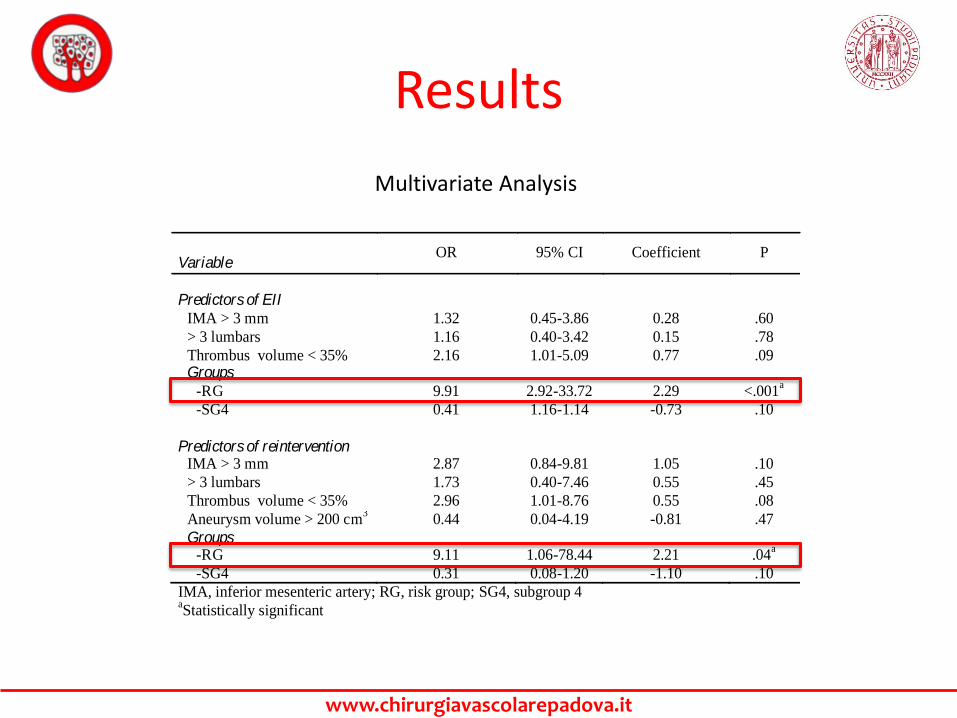
Results
Variable OR 95% CI Coefficient P
Predictors of EII
IMA > 3 mm 1.32 0.45-3.86 0.28 .60
> 3 lumbars 1.16 0.40-3.42 0.15 .78
Thrombus volume < 35% 2.16 1.01-5.09 0.77 .09
Groups
-RG 9.91 2.92-33.72 2.29 <.001a
-SG4 0.41 1.16-1.14 -0.73 .10
Predictors of reintervention
IMA > 3 mm 2.87 0.84-9.81 1.05 .10
> 3 lumbars 1.73 0.40-7.46 0.55 .45
Thrombus volume < 35% 2.96 1.01-8.76 0.55 .08
Aneurysm volume > 200 cm3
0.44 0.04-4.19 -0.81 .47
Groups -RG 9.11 1.06-78.44 2.21 .04
a
-SG4 0.31 0.08-1.20 -1.10 .10
IMA, inferior mesenteric artery; RG, risk group; SG4, subgroup 4 aStatistically significant
Multivariate Analysis
www.chirurgiavascolarepadova.it
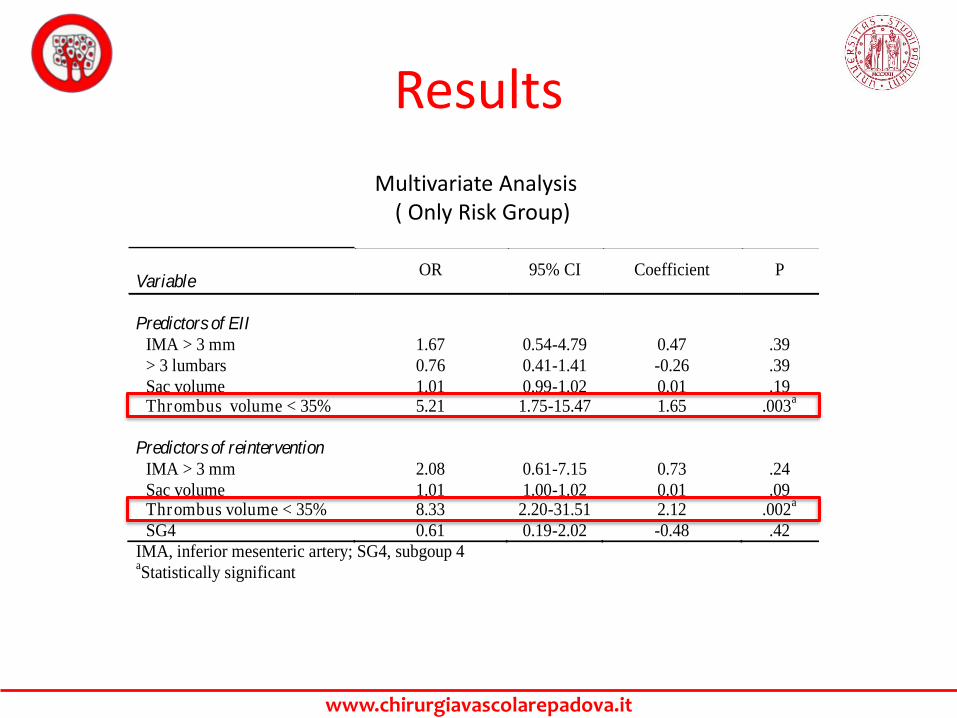
Results
Variable OR 95% CI Coefficient P
Predictors of EII
IMA > 3 mm 1.67 0.54-4.79 0.47 .39
> 3 lumbars 0.76 0.41-1.41 -0.26 .39
Sac volume 1.01 0.99-1.02 0.01 .19 Thrombus volume < 35% 5.21 1.75-15.47 1.65 .003
a
Predictors of reintervention
IMA > 3 mm 2.08 0.61-7.15 0.73 .24
Sac volume 1.01 1.00-1.02 0.01 .09 Thrombus volume < 35% 8.33 2.20-31.51 2.12 .002
a
SG4 0.61 0.19-2.02 -0.48 .42
IMA, inferior mesenteric artery; SG4, subgoup 4 aStatistically significant
Multivariate Analysis( Only Risk Group)
www.chirurgiavascolarepadova.it
Conclusions
• The identification of a group of patients AT LOW RISK forEII is feasible on the basis of simple CT characteristics. Thisgroup is very unlikely to develop EII or EII-complications.
• On the other hand, the criteria to define patients AT RISKfor EII are effective and reliable, and the association tothrombus volume <35% increases the risk 5-8 fold
• EII-preventive procedures or a careful follow-up protocolshould be performed in this subpopulation of EVARpatients
www.chirurgiavascolarepadova.it
THANKS FOR YOUR ATTENTION
I SINCERELY HOPE TO SEE ALL OF YOU IN PADUA AT THE VIP CONGRESS 2018