
Prof EK Yeoh - Nursing Conf 2018 26Jan2018 (with Logo) speaker - Nursing Conf... · 2018-02-14 ·...
59
Nursing, Professionalism, and Leadership for the 21 st Century Health Systems 27 January 2018 1 Director, The Jockey Club School of Public Health and Primary Care Head, Division of Health System, Policy and Management Faculty of Medicine, The Chinese University of Hong Kong Professor Eng-Kiong YEOH, GBS, OBE, JP
Transcript of Prof EK Yeoh - Nursing Conf 2018 26Jan2018 (with Logo) speaker - Nursing Conf... · 2018-02-14 ·...

Nursing, Professionalism, and Leadership for the 21st Century Health Systems
27 January 2018
1
Director, The Jockey Club School of Public Health and Primary CareHead, Division of Health System, Policy and ManagementFaculty of Medicine, The Chinese University of Hong Kong
Professor Eng-Kiong YEOH, GBS, OBE, JP
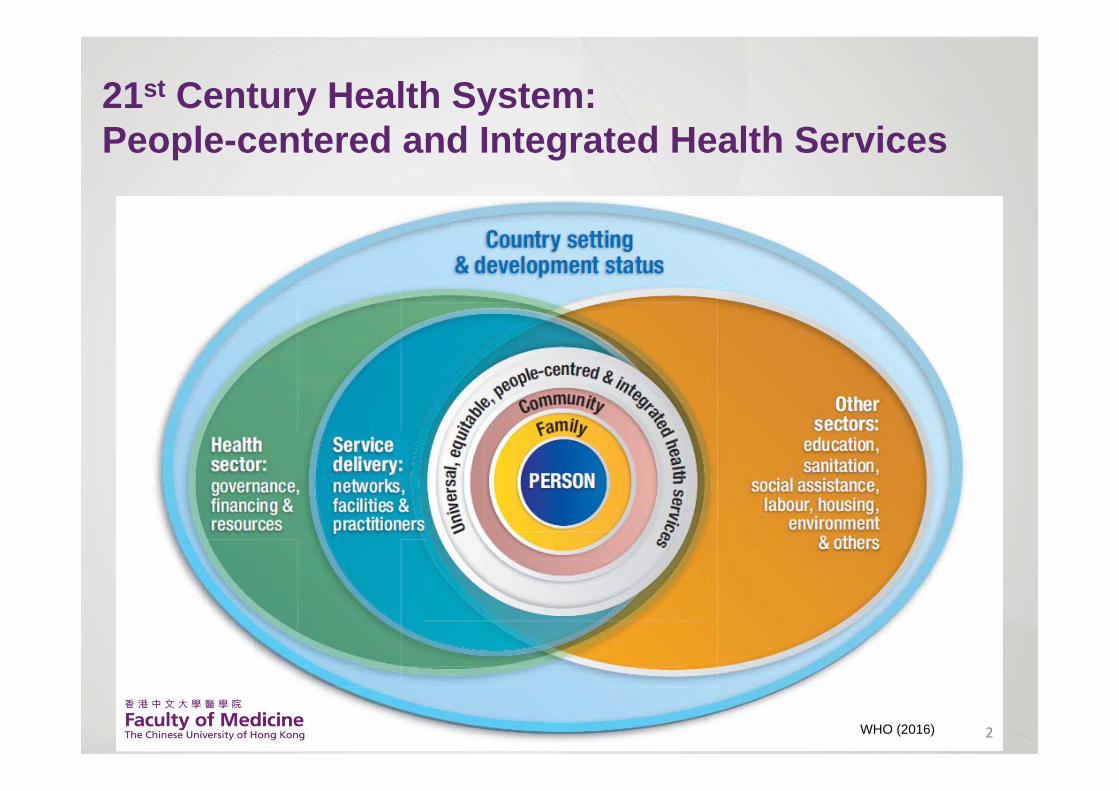
21st Century Health System: People-centered and Integrated Health Services
2WHO (2016)

Challenges for Health System• Demographic changes – life expectancy, lower fertility
• Epidemiological transition – chronic non-communicable diseases
• Social determinants of health
• Health inequalities• Preventable diseases that require lifestyle changes Advances in medical knowledge Technology transformations
• Organisational complexity
• Continuity and coordination of health services
• Collaboration and coordination of health and social care 3

Lifestyle and Chronic Diseases
• Four chronic diseases – cardiovascular disease, cancer, chronic obstructive pulmonary disease and type 2 diabetes
• Linked by common and preventable biological risk factors, high blood pressure, high blood cholesterol and overweight
• By behavioural risk factor, unhealthy diet, physical activity and tobacco use
4

Lifestyle & Chronic Diseases
• Major risk factors for chronic diseases: unhealthy lifestyle
• If the major risk factors for chronic disease were eliminated– at least 80% of heart disease, stroke and diabetes would be
prevented; – 40% of cancer would be prevented
Figures quoted from WHO (http://www.who.int/chp/en/)
5

Health Systems Framework for Healthy Ageing: Opportunities across the life course
WHO World Report on Ageing and Health (2015) 6

Chronic Disease Characteristics
• Emerge throughout life cycle, more prevalent in later life and associated with multimorbidity
• Multiple causes and complication with 80% life style related• Usually insidious in onset, may present acutely • Life long and persistent, requiring long term medical care• Progresses without treatment with deterioration of health• Progression and complications compromise quality of life
and functional limitations and disabilities• Preventable with life-style changes, progression delayed
and complications averted with treatments• Functional limitations improved with rehabilitation
7

Needs of Patients with Chronic Disease
1. Completed medical & illness diagnosis including physical and social functioning situation and role
2. Proactive, preventive (primary and secondary) and rehabilitation interventions are important
3. Patient and the carer play important role in successful outcome of the intervention
4. Require a coordinated approach to person centred(individualized) care at all levels and types of care throughout the duration of the illness
5. Biophysical emotional, social, material, and spiritual needs and priorities of each individuals over the lifetime
8

Chronic Disease Management
• Effective chronic care management requires continuity of care over the life-course to prevent deterioration, complications and disability
• 3 primary sites of fragmentation:
- between hospital, specialized, secondary and tertiary care and ambulatory, primary and preventive care
- between the public and private health sector
- between health and social care
9

Healthcare Delivery System
10
Primary Care
Specialty Care
SocialCare
Robust – Frail – Disabled – Dependent – End of LifeMultiple Chronic Diseases and Multiple Morbidity
Social Needs
Episodic illness
AffordabilityAcceptability
AvailabilityAccessibility
Organisation of Healthcare• Public & private Provision
• Financing
Healthcare Delivery• Types of care• Public & private
Needs and Demand for Care
Primary Care• General doctor consultation
• Health promotion• Disease prevention• Self management(Patient Empowerment)
Secondary/ Tertiary Care• Specialty care• Acute care• Sub‐acute care• Rehabilitation care• Geriatric day care• Outreach services: CNS, CGAT, etc.
Community care• Elderly centres & care support
• Day care places• Home care places
Residential Care• Nursing home places• Care‐and attention (C&A) places
Health promotion
Disease prevention
Chronic Disease managementPalliative care
Life Course
JCSPHPC (2017)

Integrated Health Services
• Health services that are managed and delivered in a way that ensures people receive a continuum of health promotion, disease prevention, diagnosis, treatment, disease management, rehabilitation and palliative care services, at the different levels and sites of care within the health system, and according to their needs throughout their life course
WHO global strategy on people-centred and integrated health services (2015)
11

Key Elements of Integrated Care
Comprehensive assessment • Using comprehensive geriatric assessment can evaluate needs and enable care plans to be developed (Beland and Hollander 2011, Goodwin, 2014)
Discharge planning: • Personalized plans for patients aim to improve the efficiency and quality of health care surrounding the discharge process and ensure appropriate and coordinated services are in place to support the patient (Beland and Hollander 2011, Goodwin, 2014)
Case managers/ care co‐ordinators
• A named individual is identified as care coordinator/case manager, who has direct responsibility for supporting service users by coordinating care, engaging service users in their own care and providing care directly (Eklund and Wilhelmson2009, Beland and Hollander 2011, Goodwin 2014).
Multi‐disciplinary teams • Providers from all services must work together in a flexible way to provide coordinated care and so that patients can benefit from expertise from multiple specialties (Billings 2005, Ellis et al. 2011)
12
JCSPHPC (2017)

Communication • This is a vital component for all involved in care and extends to the communication between health care professional by providing integrated electronic record management (Belandand Hollander, 2011, 2005, Goodwin, 2014).
Policy and shared values
• Processes need to be facilitated through integrated systems of care so providers can work within common governance or work towards incentives (Goodwin, 2014).
Patient‐centred care • Holistic and respectful care should be delivered with a focus on the individual and on enabling autonomy by empowering individuals to be involved in their own care (Morgan and Yoder, 2012).
Care‐givers • Informal carers provide much of the care for older people living in the community and in order to fully integrate care, caregivers should be involved in the care plan and processes.
13
Key Elements of Integrated Care (Cont’d)
JCSPHPC (2017)

(a) Type of Integration
14
Type
Functional integration(Marco level)
The extent to which key support functions and activities such as financial management, human resources, strategic planning, information management and quality improvement are coordinated across operating units
Organisationintegration(Meso level)
The creation of networks, mergers, contracting or strategic alliances between healthcare institutions
Professional integration(Meso level)
Joint working, group practices, contracting or strategic alliances of healthcare professionals within and between institutions and organisations
Clinical integration (Micro level)
Extent to which patient care services are coordinated across the various personnel, functions, activities and operating units of a system
RAND Europe (2012)

Persons having Chronic Health Conditions by Age
Census and Statistics Department: Thematic Household Survey 50 (2013)
N=1,896,100
Rate of having chronic health conditions among all persons in HK is 28.1%
15

Ageing with an Increase in Chronic Diseases
16

Hong Kong Health System
Health Expenditure (2013/14)Total expenditure on health as % of GDP 5.7%
Public Expenditure on Health (48.9%)
Private Expenditure on Health (51.1%)
Food and Health Bureau – Hong Kong’s Domestic Health Accounts 2013/14)
17

Hong Kong Health System
18
Public
Service Delivery
Inpatient (Hospital beds)In 2016
Private
Outpatient(Attendances)In 2013 ‐ Refers to consultations made to Western medicine and Chinese medicine practitioners during the 30 days before enumeration
31% 69%
Inpatient data from Department of Health and Hospital Authority; Outpatient data from Census and Statistics Department Thematic Household Survey Report No. 50
87% 13%

Hong Kong Health System
19

Hong Kong elderly 65+
20
No chronic diseases
At least 1 chronic diseases
Approaching end of life
Private(56.5%)
Outpatient Inpatient
Public(81.6%)
Most cannot go for outpatient due to physical problem or transportation
Public(2.9%)
Public(13.7%)
Most deaths in public hospitals
Private(0.6%)
Public(24.3%)
Both (11.7%)
Both (44.7%)
Private(59.0%)
Private(1.7%)
JCSPHPC (2017)

Conceptual integrated system model: Hospital‐Community Network
Community call centre
Care in residential/ nursing homes (CGAT)
Volunteers & community involvement
Allied health care professionals
Palliative services
Social service centres (Neighbourhood elderly centres)
Clinic/ nursing care*Specialist clinics*Community Nursing*Day hospitals*Private clinics
Community Hub: services coordination team
Community Network
Private primary care
Informal caregivers
Hospital/ inpatient Network
Hospital Hub: services coordination team
A&E multidisciplinary community referral team
Inpatient assessment & discharge team
Specialist wards
General medical wards
Accident & Emergency Department
Rehabilitation / convalescent facility
Palliative beds & services
Geriatric‐care focus (i.e. cognitive impairment)
Enabling policies
Shared medical + social services
records
Improved training/ education
Common goals & values
Person‐centered care
EOL policy and
programmes
Medical‐social service connections
Visiting medical officers
Emergency medical wards
Post‐discharge care (ICDS)
Post‐discharge care (ICDS)
Note: (1) Hubs and networks are intended as ‘virtual connections’, (2) Service lists are for illustrative purposes, and (3) manyconnections between services are encouraged, in addition to the close working connection between hospital and community hubs.
Family Medicine/ primary care community care centres (HA)
Elderly health centres (DOH)
Hub/ patient coordinators
21JCSPHPC (2017)

Primary care● General Out Patient Clinic● Private Doctors
Community care● Department of Health Elderly Health Centres (health promotion, disease prevention & screening)
Sub‐acute care ● Rehab hospital● Integrated Care Discharge Support
Community services●Meal delivery● Home care visits● Non‐government organisations
Long‐term care●Community Geriatric Assessment Service (CGAS) in Residential Care Homes for the Elderly (RCHE)● Community Nursing Service
22
Intensity
of care ne
eds
Social service centres● Neighbourhood/ district elderly centres
Post‐hospital discharge/ high intensity needs
Occasional acute illness, otherwise stable
Requires regular additional support
Stable chronic disease/Generally ‘well elderly’
Clinic/ nursing care● Specialist Out Patient Clinic● Community Nursing Service
‘Medical’ services ‘Social’ services
Enabling policies
Linked budgets
Improved training/ education
Common goals & values
Information sharing/
communication
EOL policy and
programmes
Harness volunteer potential
Public‐private
partnership
Commitment to change
An integrated medical-social service network for providing needs-matched care and support
Note: services listed are illustrative rather than definitive
Patient‐CenteredCare
JCSPHPC (2017)

Profession
• “Profession” as “The occupation which one professes to be skilled in and to follow. a) A vocation in which professed knowledge of some department
of learning or science is used in its application to the affairs of others or in the practice of an art founded upon it
b) In a wider sense: any calling or occupation by which a person habitually earns his living.”
Oxford English Dictionary
23

“Professes”
• “Professes” represents a public commitment to a set of values i.e. the Hippocratic Oath or its modern equivalent.
• Knowledge is applied in serving others, professions are seen as altruistic and value based
Cruess, Cruess & Johnston (2000)
24

Profession
• Knowledge base• Skills and competencies• Attributes• Values and attitudes• Vocation and duties• Unique service and occupation• Societal recognition
25

Professional –Sociological Perspectives1. Possession of specialised knowledge and training that
enable professionals to know what to do in particular circumstances, to be able to provide a rational explanation for their actions, and to undertake the action safely
2. Dedication to public service3. Socially approved self-governance
McDonald (1995)
26
Professional –Professional Perspectives• Traditionally, professionals had a broader concept of
professionalism goes beyond sociological description to include a complex of virtues and ideals involving habits of mind and character
Benatar (1997)
27

Professionals
• Professionals only have duties – they do not have privileges. The have duties over and above the duties of being a citizen.
Sir Ian Kennedy (20 May 2005)
28

Professionalism
29

Professionalism
[Professionalism] is based around standards, and the starting point is that it is not just about standards that the individual acquires, but they are [also] in the context of the institution. By standards we are talking not just about clinical standards, but about behaviour and values.
Sir Nigel Crisp (20 May 2005)
30

Professionalism
While a body of knowledge is clearly essential, it is the interpretation of knowledge, the engagement with new knowledge, the acknowledgement of uncertainty about knowledge, the sharing of knowledge, not the holding of knowledge, that are the characteristics of modern medicine.
Harry Cayton (12 November 2004)
31

Professionalism:Behaviour and Systems View• Specific behaviours required multidimensional
competencies• A practiced skill• Profoundly influenced by organization and environmental
context• External forces need to be harnessed to support, not
inhibit
Lesser et al. (2010)
32

Systems View of Professionalism
Lesser et al. (2010)
33

Professionalization• Process through a person becomes socialized into a
profession (Chitty KK, 2001)• A process “by which a person acquires the knowledge, skills,
and sense of occupational identity characteristic of a professional and involves the internalization of the values and norms of a professional group” (Jacox A, 1978)
• Professional socialization – begins during the foundational education programs when nurses
internalize the knowledge, skills, attitudes and professional standards– continues as the nurse practices
• Goal of professional socialization – Development of professionalism
34

Nursing Professional – Theoretical Framework
Person
Body Pathology
Three interlocking circles Core circle – social, emotional, spiritual, and intellectual needs of the family, community, and world and the therapeutic use of self
Cure circle – functions collaboratively with healthcare team members
Care circle – bodily care
Hall’s Care, Cure, and Core Theory (1969) 35

Prime Feature of Nursing Professionalism
• Relationship between the nurse and the patient (Volp K, 2006)
• Demonstrate certain professional attributes– Knowledge and skills– Accountability– Interpersonal skills and professional attitudes including
communication, empathy and courtesy
36

Wheel of Professionalism in Nursing
Copyright ©1984 Barbara Kemp Miller 37

Nursing Professionalism
4 properties:1. High degree of systematic and public knowledge,
2. awareness about the interests of society rather than the personal interest
3. High degree of self-control in behavior through moral codes
4. existence of a reward system as a sign for success
Barber (1965)
38

Nursing Professionalism
Defined codes of professional behavior:1. Respecting the dignity, value, and beliefs of the patients
2. Maintaining patients’ trust, making informed decision
3. Provision of competent and safe care, maintaining standards of activities
4. Presenting the image of nursing, having a harmony with the law in action
Lui (2007)
39

Nursing Professionalism 1. Continuum in the professional socialization process
2. 5 groups of antecedents of nursing professionalization:
(i) Demographic: ethnic differences, gender differences
(ii) Experience: years of experience, previous experiences, maturity in professional experiences
(iii) Education: membership in professional organizations, specialized certification, educational readiness, training and socialization
(iv) Position: gap between education and clinical practice, expectations & type of organization, workload
(v) Value: professional satisfaction organizational commitment, professional freedom and independence, motivation, belonging, knowing, acknowledging, support and guidance, responsibility, altruism, professional identity, belonging to a team, valuing the work.
40

Nursing Professionalism –beginner – expert continuum
5 levels: Beginner
Advanced
Competent
Proficient
Expert
Represent progressive stages of acquired skills and experience
41

Concept map of the Professional Value
DignityUniqueness
Right to PrivacyConfidentialityProtection fromIncompetencyResponsibilityCompetence
Informed JudgementProfession’s Body of
KnowledgeStandards of Care
Conditions of EmploymentCollaboration
Protection of the Public
Unique Body of Knowledge Autonomy
Strong OrganizationAltruism
High Education Service
ProfessionalValues
ANA Co
de
of Ethics
Characteristics
of Professions
ANA = American Nurses AssociationAACN = American Association of Colleges of Nursing
Kubsch (2008)42

Perceived Professional Values
• Nursing education• Leadership position• Professional organization membership• Age• Baccalaureate registered nurses in first 2 years of
employment
Kubsch (2008)
Correlated with:
43

Nursing Professionalism –
Professional vales embodied by the more experienced and older nurses through years of work, insight, and rewards of nursing care that is empathetic, altruistic, holistic, ethical, nutritive, generative, and protective in nature
Kubsch (2008)
44

Nursing Professional Development –Clinical Nursing Model – Building
and Enabling Environment
45
Hospital Authority Dr Eric Chan (2014)

Career Progression Model for Nurses in HA
46
CGMNGMN
DOM/SNONurse
ConsultantDepartment OperationsManager
WM/NS/NO/NE
AdvancedPracticeNurse
Nurse Unit Manager
RN Specialty Nurse
Practice Nurse (pre‐specialty level)
Practice Nurse (perceptive level)
EN
Nursing Service Department , HAHO (2008)

Framework of model
47
Tier 5 Servicemanager
Manageservice operation & development
Tier 4 Team manager Manage team operation & development
Tier 5 Specialty /Subspecialtyleader
Lead professionaldevelopment of the specialty/subspecialty
Tier 4 Specialty /Subspecialtypractitioner
Lead a team provide complex care independently for specialty/subspecialty
Tier 3 Specialty practitioner Provide complex care independently for general specialty
Tier 2 Practitioner Provide general patient care independently Complex/ difficult case under supervision
Tier 1 Entrant practitioner License to practiceProvide service under supervision
Management Clinical
Nursing Service Department , HAHO (2008)

What’s the future?Current Issues Opportunities for Nursing
Ageing population
Primary Health Care
Non‐communicable diseases
Hospital accreditation
Health care financing & insurance
Health system pressure – waiting list and waiting time
Professional advancement –academy
Tertiary education for nurses
Prevention/ early prevention: health maintenance
Enhancing care in the community
Independent practice
Enhanced scope of practice and credentialing
Refine and redefine of health professional boundaries – service needs and pressure from patients
Relevancy of nursing education and practice – basic and post basic
48Dr Eric Chan (2014)
Professional Regulation
Main purposes
• Ensure that minimally acceptable standards of care are being provided
• Provide accountability and reassure patients and payers that medical professionals are deserving trust; and
• Improve quality of care by providing guidance about best practice and fostering improvements in performance through measurement and feedback
Sutherland and Leatherman (2006)
49

Integrated Mechanisms for Regulation
• Personal regulation• Team-based regulation• Organisational regulation• National professional regulation system• Meta-regulation• Patient and public assurance
Department of Health of UK (2009)
50

51

8 Myths in Leadership
52Source: https://www.elsevier.com/connect/8‐myths‐of‐leadership‐by‐a‐stem‐leader
Myth #1: Leadership is a rare skillMyth #2: Leaders are born, not madeMyth #3: Leaders are charismaticMyth #4: Leadership exists only at the
top of the organizationMyth #5: The leader controls, directs,
prods and manipulatesMyth #6: How you behave outside of
work and online does not affect your ability to lead
Myth #7: Leaders have all the answersMyth #8: Your team is there to serve you

Leaders, Leading and Leadership: Confusions in Application• Leaders
– Formally position defined role
– Informal (charismatic/heroic)
"As we look ahead into the next century, leaders will be those who empower others“ (Bill Gates)
• Leadership also refers to “leading” towards achievement of a goal.
• Leadership– Noun: to describe people who lead
– Adjective: to describe quality of leaders or leading
– Adverb: refers to the process of leading
53Source 1: https://www.forbes.com/sites/kevinkruse/2013/04/09/what‐is‐leadership/2/#709fbdd541f0Source 2: http://www.nwlink.com/~donclark/leader/leadled.html

Leadership
Leadership is a dynamic process ofsocial influence towards achievement of a goal
54

Health System
• Healthcare leadership takes place at multiple levels and involves multiple professionals
• Requires organisations to redistribute leadership power to wherever expertise, capability and motivation within organisations.
• It calls for collective and shared leadership with the health system and a healthcare organization
• The leadership emphasis is shifted to building relationships, networking, trusts, commitment and social capital
55

Psychology 101 for Leaders?• Leadership is about understanding, changing and enhancing human
behavior• Good knowledge of how humans operate in an organization helps the
leadership process – Role of Motivation – People dynamics, how self, groups and organizations behave and
interact– Relationships building and Conflict management, – Building commitment and group identity– Adapting influencing behavior to increase effectiveness– Understanding and influencing culture– Understanding psychodynamic processes
A process of influence that occurs within relationships between leaders and their stakeholders establishing shared vision and generating motivation and inspiration.
56

Harnessing Health Professionalism for Clinical Excellence
57
Leader
ManagerHealth
Professional
Self ManagementEmotional intelligence
TraitsStyles
Behaviours
RegistrationClinical Governance
Credentialing
Influencing(clinical excellence)
Psychodynamics Process
ContextTask
CultureSituation
Power (instrument of influence): PositionalPersonalSocietal
Clinician
Health ProfessionalManager
Motivation (Individual, group)
NeedsExpectancy
InstrumentalityValenceGoals
Professionalism:Values
BehavioursRelationship
Dynamic Dynamic Temporal Temporal
Relationship RelationshipEnvironment Environment JCSPHPC (2017)

Philosophy of Science, Theory and Knowledge Relating to Nursing and Professionalism
“Philosophy, knowledge and theory are intrinsically linked”
“…explore the nature of the philosophy of science, knowledge and theory and their interrelationships, with particular reference to professionalization by considering where nursing has come from and consequently the way forward to ascertaining professional status.”
Rutty (1998)
58

Thank you!
59


















