
PRODUCT MONOGRAPH XYLOCARD
22
- 1 - © The Aspen Group, 2017. All rights reserved PRODUCT MONOGRAPH XYLOCARD ® 20 mg/mL (lidocaine hydrochloride injection USP) Antiarrhythmic Aspen Pharmacare Canada Inc 111 Queen Street East, Suite 450, Toronto, Ontario M5C 1S2 Date of Revision: August 15, 2017 Control No.: 206687 XYLOCARD ® is a registered trademark of the AstraZeneca group of companies.
Transcript of PRODUCT MONOGRAPH XYLOCARD

- 1 -
© The Aspen Group, 2017. All rights reserved
PRODUCT MONOGRAPH
XYLOCARD®
20 mg/mL
(lidocaine hydrochloride injection USP)
Antiarrhythmic
Aspen Pharmacare Canada Inc
111 Queen Street East, Suite 450,
Toronto, Ontario
M5C 1S2
Date of Revision:
August 15, 2017
Control No.: 206687
XYLOCARD® is a registered trademark of the AstraZeneca group of companies.

- 2 -
© The Aspen Group, 2017. All rights reserved
PRODUCT MONOGRAPH
NAME OF DRUG
XYLOCARD®
20 mg/mL
(lidocaine hydrochloride injection USP)
THERAPEUTIC CLASSIFICATION
Antiarrhythmic
ACTIONS AND CLINICAL PHARMACOLOGY
Mechanism of Action
The mode of action of the antiarrhythmic effect of XYLOCARD (lidocaine hydrochloride)
appears to be similar to that of procaine, procainamide, and quinidine. Ventricular excitability
is depressed and the stimulation threshold of the ventricle is increased during diastole. The
sinoatrial node is, however, unaffected. In contrast to the latter three drugs, XYLOCARD in
therapeutic doses does not produce a significant decrease in arterial pressure or in cardiac
contractile force. In larger doses, XYLOCARD may produce circulatory depression, but the
magnitude of the change is less than that found with comparable doses of procainamide.
Neither drug appreciably affects the duration of the absolute refractory period.
Onset of Action
The onset of action following a single intravenous injection varies from 45 to 90 seconds.
Duration of action is 10 to 20 minutes.
INDICATIONS AND CLINICAL USE
The intravenous administration of XYLOCARD (lidocaine hydrochloride) is indicated in the
treatment of ventricular tachycardia occurring during cardiac manipulation, such as surgery or
catheterization, or which may occur during acute myocardial infarction, digitalis toxicity, or
other cardiac diseases.

- 3 -
© The Aspen Group, 2017. All rights reserved
CONTRAINDICATIONS
XYLOCARD (lidocaine hydrochloride) is contraindicated in patients with:
1. Known hypersensitivity to local anesthetics of the amide type, such as prilocaine,
mepivacaine or bupivacaine, or to other components of the solution;
2. Adams-Stokes syndrome, or severe degrees of sinoatrial, atrioventricular or
intraventricular block.
The safety of XYLOCARD in the treatment of arrhythmias in children has not been
established.
WARNINGS
Constant ECG monitoring is essential for the proper administration of XYLOCARD
(lidocaine hydrochloride) intravenously. Signs of excessive depression of cardiac
conductivity, such as prolongation of PR interval and QRS complex, and the appearance of
aggravation of arrhythmias, should be followed by prompt cessation of the intravenous
infusion.
It is mandatory to have emergency resuscitative equipment and drugs immediately available to
manage possible adverse reactions involving the cardiovascular, respiratory, or central
nervous systems.
In emergency situations, when a ventricular rhythm disorder is suspected, and ECG equipment
is not available, a single dose may be administered when the physician in attendance has
determined that the potential benefits outweigh the possible risks. If possible, emergency
resuscitative equipment and drugs should be available.
PRECAUTIONS
XYLOCARD (lidocaine hydrochloride) should be used with caution in patients with
bradycardia, severe digitalis intoxication, first or second degree heart block in the absence of a
pacemaker, or hypokalaemia (see CONTRAINDICATIONS and WARNINGS).
In unconscious patients circulatory collapse should be watched for, since CNS effects may not
be apparent as an initial manifestation of toxicity.
Caution should be observed in patients with cardiac decompensation and hypotension or
posterior diaphragmal infarction with a tendency towards development of heart block.
Intravenous administration of XYLOCARD is sometimes accompanied by a hypotensive
response, and, in overdosage, this may be precipitous. For this reason the intravenous dose
should not exceed 100 mg in a single injection, and no more than 200-300 mg in a one hour
period (see DOSAGE and ADMINISTRATION).

- 4 -
© The Aspen Group, 2017. All rights reserved
When high doses are used and the patient’s myocardial function is impaired, combination with
other drugs which reduce the excitability of cardiac muscle requires caution.
Repeated doses of XYLOCARD may cause significant increases in blood levels with each
repeated dose because of slow accumulation of the drug or its metabolites. Tolerance to
elevated blood levels varies with the status of the patient. Debilitated, elderly patients and
acutely ill patients should be given reduced doses commensurate with their age and physical
condition. XYLOCARD should also be used with caution in patients with epilepsy, impaired
cardiac conduction, bradycardia, impaired hepatic function or renal function and in severe
shock.
Use in the Elderly
A reduction in dosage may be necessary for elderly patients, particularly those with
compromised cardiovascular and/or hepatic function and/or prolonged infusion. Elderly
patients should be given reduced doses corresponding to their age and physical status.
Impaired Renal Function
Caution should be employed in the repeated use of XYLOCARD in patients with severe renal
disease, since possible accumulation of lidocaine or its metabolites may lead to toxic
phenomena.
Impaired Hepatic Function
Caution should be employed in the repeated use of XYLOCARD in patients with severe liver
disease, since possible accumulation of lidocaine or its metabolites may lead to toxic
phenomena.
Use in Pregnancy
It is reasonable to assume that lidocaine has been used, mainly as a local anesthetic, by a large
number of pregnant women and women of child-bearing age. No specific disturbances to the
reproductive process have so far been reported, e.g., no increased incidence of malformations.
However, care should be taken during early pregnancy when maximum organogenesis takes
place.
There are no adequate and well-controlled studies with intravenous administration of lidocaine
in pregnant women.
Use in Nursing Mothers
Lidocaine is excreted in the breast milk, but in such small quantities that there is generally no
risk of affecting the infant at therapeutic dose levels.
- 5 -
© The Aspen Group, 2017. All rights reserved
Use in Neonates
Through their lower enzyme capacity, very rarely, neonates are at risk of
methaemoglobinaemia. Methaemoglobinaemia can become clinically overt (cyanosis), and
treatment with methylene blue may be considered necessary.
Use in Patients with Acute Porphyria
Theoretical evidence suggests that lidocaine may have porphyrogenic properties. The clinical
significance of this is unknown. Caution should be exercised if intravenous lidocaine
(XYLOCARD) is administered to patients with acute porphyria.
Drug Interactions
Lidocaine is mainly metabolized in the liver by CYP1A2 and CYP3A4 to its two major
metabolites, monoethylglycinexylidine (MEGX) and glycinexylidine (GX), both of which are
pharmacologically active. Lidocaine has a high hepatic extraction ratio. Only a small fraction
(3%) of lidocaine is excreted unchanged in the urine. The hepatic clearance of lidocaine is
expected to depend largely on blood flow.
Since the affinity of lidocaine to CYP1A2 and CYP3A4 is very low compared to therapeutic
plasma concentrations, it is less likely that the metabolism of substrates for these enzymes will
be inhibited when coadministered with lidocaine. However, there is a potential for influence
of other drugs on the plasma levels/effect of lidocaine, e.g. strong inhibitors or inducers of
CYP1A2 and/or CYP3A4 and drugs that affect liver blood flow (see Table 1).
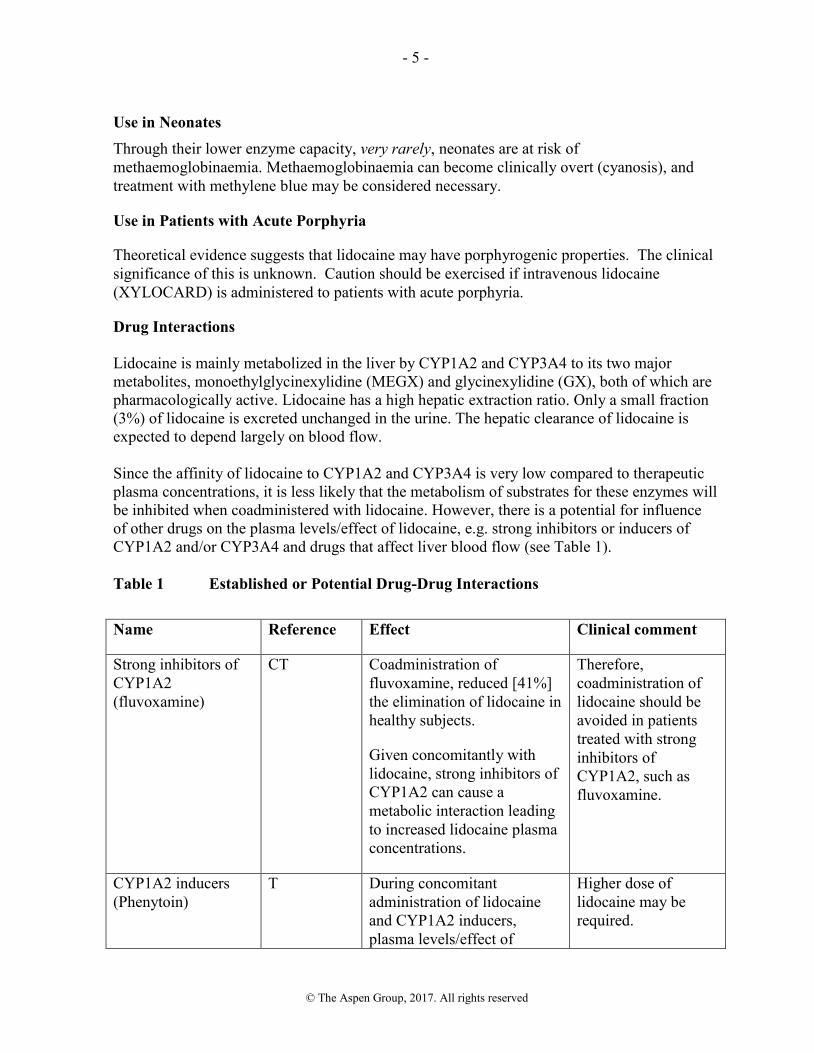
Table 1 Established or Potential Drug-Drug Interactions
Name Reference Effect Clinical comment
Strong inhibitors of
CYP1A2
(fluvoxamine)
CT Coadministration of
fluvoxamine, reduced [41%]
the elimination of lidocaine in
healthy subjects.
Given concomitantly with
lidocaine, strong inhibitors of
CYP1A2 can cause a
metabolic interaction leading
to increased lidocaine plasma
concentrations.
Therefore,
coadministration of
lidocaine should be
avoided in patients
treated with strong
inhibitors of
CYP1A2, such as
fluvoxamine.
CYP1A2 inducers
(Phenytoin)
T During concomitant
administration of lidocaine
and CYP1A2 inducers,
plasma levels/effect of
Higher dose of
lidocaine may be
required.

- 6 -
© The Aspen Group, 2017. All rights reserved
Name Reference Effect Clinical comment
lidocaine may decrease.
Strong inhibitors of
CYP3A4
(erythromycin,
itraconazole)
CT Erythromycin and
itraconazole have each been
shown to have a modest or no
effect on the
pharmacokinetics of
intravenous lidocaine (0-18%
decreased elimination with
erythromycin but no effect
with itraconazole).
No dose adjustment
seems required.
CYP3A4 inducers
(carbamazepine,
phenobarbital,
phenytoin,
primidone)
CT Concomitant administration
with carbamazepine,
phenobarbital, phenytoin, and
primidone, may slightly
decrease plasma levels of
lidocaine (<10%).
No dose adjustment
seems required.
Beta-blockers
(propranolol,
metoprolol, nadolol)
CT Propranolol, metoprolol, and
nadolol have been reported to
reduce intravenous lidocaine
clearance, probably through
effects on hepatic blood flow
and/or metabolism, and may
increase the plasma
concentration of lidocaine by
about 30%, less with
metoprolol.
Therefore,
concomitant
administration of
beta-blockers with
lidocaine should be
avoided. If not
possible, close
monitoring and dose
adjustment may be
required.
Cimetidine CT Cimetidine has an unspecific
inhibitory effect on CYP
(including CYP1A2 and CYP
3A4) mediated metabolism
and reduces hepatic blood
flow.
Clinical experiments showed
that the concomitant
administration of cimetidine
reduces the systemic
clearance of lidocaine and
increases lidocaine serum
Therefore,
concomitant
administration with
lidocaine should be
avoided. If not
possible, close
monitoring and dose
adjustment of
lidocaine and/or
cimetidine may be
required.

- 7 -
© The Aspen Group, 2017. All rights reserved
Name Reference Effect Clinical comment
concentration by as much as
50%. Thus, therapeutic
serum levels of lidocaine may
rise to toxic levels when
cimetidine is used
concomitantly. Ranitidine
has not displayed this effect.
Amiodarone CT, C Like cimetidine, amiodarone
has an unspecific inhibitory
effect on CYP mediated
metabolism. Concomitant
administration has resulted in
increased plasma levels of
lidocaine and may result in
toxic effects.
Therefore,
concomitant
administration with
lidocaine should be
avoided. If not
possible, close
monitoring and dose
adjustment of
lidocaine and/or
amiodarone may be
required.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Studies of lidocaine in animals to evaluate the carcinogenic and mutagenic potential or the
effect on fertility have not been conducted.
ADVERSE REACTIONS
Adverse experiences following the administration of lidocaine are similar in nature to those
observed with other amide type agents. These adverse experiences are, in general, dose-
related and may result from high plasma levels caused by excessive dosage or rapid
absorption, or may result from a hypersensitivity, idiosyncrasy or diminished tolerance on the
part of the patient.
Common adverse reactions are those from the central and peripheral nervous system. They
occur in 5-10% of the patients and are mostly dose-related. The following definitions of
frequencies are used: Very common ( ≥ 10%), common (1 – 9.9%), uncommon (0.1 – 0.9%),
rare (0.01 – 0.09%) and very rare (< 0.01%).
Systemic reactions of the following types have been reported:
Central Nervous System
CNS manifestations are excitatory and/or depressant. Common adverse reactions are
circumoral paresthesia, dizziness and drowsiness. Rare adverse reactions would include
- 8 -
© The Aspen Group, 2017. All rights reserved
persistent dizziness, lightheadedness, nervousness, apprehension, euphoria, confusion,
hyperacusis, tinnitus, blurred vision, vomiting, sensations of heat, cold or numbness,
twitching, tremors, convulsions, unconsciousness, apnea, respiratory depression and arrest.
The excitatory manifestations may be very brief or may not occur at all, in which case the first
manifestation of toxicity may be drowsiness merging into unconsciousness and respiratory
arrest.
Drowsiness following the administration of lidocaine is usually an early sign of a high
lidocaine plasma level and may occur as a consequence of rapid absorption.
Cardiovascular System
Rare cardiovascular manifestations are usually depressant and are characterized by
bradycardia, hypotension, asystole and cardiovascular collapse which may lead to cardiac
arrest. Arrhythmias, including ventricular tachycardia/ventricular fibrillation have also been
reported.
Hematologic System
Very rarely, neonatal methaemoglobinaemia can occur (see Precautions).
Immune System
Allergic reactions are characterized by cutaneous lesions, urticaria, edema, or in the most
severe and very rare instances, hypersensitivity including anaphylactic shock. Allergic
reactions of the amide type are rare and may occur as a result of sensitivity either to the drug
itself, or to other components of the formulation.
Idiosyncratic reactions have been reported at low doses in some patients. Cross-sensitivity
between XYLOCARD and procainamide or XYLOCARD and quinidine have not been
reported.
SYMPTOMS AND TREATMENT OF OVERDOSAGE
Symptoms of idiosyncratic reactions are described under ADVERSE REACTIONS.
Symptoms
Lidocaine toxicity may appear at serum concentrations greater than 8 mg/L. The most serious
effects of lidocaine intoxication are on the central nervous system and cardiovascular system
and overdosage can result in dizziness, delirium, severe hypotension, conduction defects,
bradycardia, asystole, arrhythmias, including ventricular tachycardia/fibrillation,
cardiovascular collapse which may lead to cardiac arrest, apnea, seizures, coma, respiratory
arrest and death.
Central nervous system toxicity is a graded response, with symptoms and signs of escalating
severity. The first symptoms are circumoral paresthesia, numbness of the tongue,
lightheadedness, hyperacusis and tinnitus. Visual disturbance and muscular tremors are more
serious and precede the onset of generalized convulsions. Unconsciousness and grand mal

- 9 -
© The Aspen Group, 2017. All rights reserved
convulsions may follow, which may last from a few seconds to several minutes. Hypoxia and
hypercarbia occur rapidly following convulsions due to the increased muscular activity,
together with the interference with normal respiration. In severe cases apnea may occur.
Acidosis increases the toxic effects.
Recovery is due to redistribution and metabolism of the drug. Recovery may be rapid unless
large amounts of the drug have been administered.
Cardiovascular effects may be seen in cases with high systemic concentrations. Severe
hypotension, bradycardia, arrhythmia and cardiovascular collapse may be the result in such
cases.
Cardiovascular toxic effects are generally preceded by signs of toxicity in the central nervous
system, unless the patient is receiving a general anesthetic or is heavily sedated with drugs
such as a benzodiazepine or barbiturate.
Treatment
The first consideration is prevention, best accomplished by careful and constant monitoring of
cardiovascular and respiratory vital signs and the patient's state of consciousness. At the first
sign of change, oxygen should be administered.
The first step in the management of convulsions consists of immediate attention to the
maintenance of a patent airway and assisted or controlled ventilation with oxygen and a
delivery system capable of permitting immediate positive airway pressure by mask.
Immediately after the institution of these ventilatory measures, the adequacy of the circulation
should be evaluated, keeping in mind that drugs used to treat convulsions sometimes depress
the circulation when administered intravenously.
An anticonvulsant should be given i.v. if the convulsions do not stop spontaneously in 15-20
seconds. Thiopental 100-150 mg i.v. will abort the convulsions rapidly. Alternatively,
diazepam 5-10 mg i.v. may be used, although its action is slower. Succinylcholine will stop
the muscle convulsions rapidly, but will require tracheal intubation and controlled ventilation,
and should only be used by those familiar with these procedures.
Hypotension may be counteracted by giving sympathicomimetic drugs (e.g., adrenaline).
Adrenergic agents of both α-adrenoceptor stimulating (e.g., metaraminol) and β-adrenoceptor
stimulating type (e.g., isoprenaline) are generally effective. The bradycardia may be treated
with parasympatholytic agents (e.g., atropine).
Should circulatory arrest occur, immediate cardiopulmonary resuscitation should be instituted.
Optimal oxygenation and ventilation and circulatory support as well as treatment of acidosis
are of vital importance, since hypoxia and acidosis will increase the systemic toxicity of local
anesthetics. Epinephrine (0.1-0.2 mg as intravenous or intracardial injections) should be given
as soon as possible and repeated, if necessary.

- 10 -
© The Aspen Group, 2017. All rights reserved
DOSAGE AND ADMINISTRATION
Single Intravenous Injection
The usual dose is 50 to 100 mg XYLOCARD (lidocaine hydrochloride) administered under
ECG and blood pressure monitoring. This dose may be administered at the rate of
approximately 25 to 50 mg/min. Sufficient time should be allowed to enable a slow
circulation to carry the drug to the site of action. If the initial injection of 50 to 100 mg does
not produce a desired response, a second dose may be repeated after 10 minutes. NO MORE
THAN 200 TO 300 MG OF XYLOCARD SHOULD BE ADMINISTERED DURING A
ONE HOUR PERIOD.
Continuous Intravenous Infusion
Following intravenous injection, XYLOCARD may be administered by intravenous infusion
at a rate of 1-2 mg/min (approximately 15-30 µg/kg/min in the average 70 kg patient) in those
patients in whom the arrhythmia tends to recur, and who are incapable of receiving oral
antiarrhythmic therapy.
Intravenous infusions of XYLOCARD must be administered under constant ECG and blood
pressure monitoring and with meticulous regulation of infusion rate, in order to avoid
potential overdosage and toxicity.
Intravenous infusions should be terminated as soon as the patient's basic cardiac rhythm
appears to be stable or at the earliest signs of toxicity. It should rarely be necessary to
continue intravenous infusion beyond 24 hours. As soon as possible, and when indicated,
patients should be changed to an oral antiarrhythmic agent for maintenance therapy.
Solution for intravenous infusion may be prepared by the addition of one gram of
XYLOCARD (i.e., contents of ten 5 mL ampoules) to one litre of an appropriate infusion
solution. Approximately a 0.1% solution will result from this procedure; that is, each mL will
contain approximately 1 mg of XYLOCARD.
In those cases in which fluid restriction is medically desirable a more concentrated solution
may be prepared by adding one gram of XYLOCARD (i.e., contents of ten 5 mL ampoules) to
500 mL of diluent. Approximately a 0.2% solution will result from this procedure; that is,
each mL will contain approximately 2 mg of XYLOCARD.
Solutions should be prepared using aseptic technique. As with all intravenous admixtures,
dilution should be made just prior to administration. Prepared solutions should be used within
12 hours.

- 11 -
© The Aspen Group, 2017. All rights reserved
PHARMACEUTICAL INFORMATION
Drug Substance
Proper name: Lidocaine hydrochloride
Chemical Name: 2-(Diethylamino)-2',6'-acetoxylidide monohydro-chloride monohydrate
Structural Formula:
Molecular Formula: C14H22N2OH2O
Molecular Weight: 288.82
Description: Lidocaine hydrochloride is a white, odourless, crystalline powder which has a
slightly bitter taste. It is very soluble in water and in alcohol, soluble in
chloroform and insoluble in ether.
Composition/mL
XYLOCARD
100 mg
Active:
Lidocaine
hydrochloride
20 mg
Non-medicinal:
Sodium chloride
for (isotonicity)
Water for
injection
6 mg
Sodium hydroxide and/or hydrochloric acid to adjust pH to 5.0-7.0.
Stability and Storage Recommendations
Store at room temperature (15-30°C).
XYLOCARD solutions are preservative free and are for single use. Discard unused portion.

- 12 -
© The Aspen Group, 2017. All rights reserved
AVAILABILITY OF DOSAGE FORMS
Single Intravenous Injection
XYLOCARD 100 mg is available in a 5 mL glass ampoule (contains 20 mg/mL, a 2%
solution).
Continuous Intravenous Infusion
5% dextrose in water is the preferred diluent.
See DOSAGE and ADMINISTRATION section for instructions regarding preparation of
solutions for continuous intravenous infusion.
PHARMACOLOGY
Lidocaine hydrochloride is a well known anesthetic agent which has been used for many years
for regional and topical anesthesia. However, it has been demonstrated to exert an
antiarrhythmic effect by increasing the electrical stimulation threshold of the ventricle during
diastole.
In decerebrated, vagotomized cats with stellate ganglia destroyed, lidocaine hydrochloride
intravenous suppressed cardiac arrhythmias induced by faradic stimulation, barium chloride
and epinephrine. The minimal effective dose was 0.5 mg per kg. This was 4 and 5 times less
than the minimal doses of procaine and procainamide respectively.
In anesthetized open-chest dogs, lidocaine hydrochloride 5 mg per kg intravenously reduced
the duration of methacholine-induced auricular arrhythmias by 55.5%. The effect of quinidine
sulphate at the same dose was a reduction 46.5%. Ventricular arrhythmias induced by
coronary ligation were controlled by total intravenous doses of 50 mg/kg. Convulsions and
vomiting were produced and death occurred in 1 of 6 dogs at 75.5 mg/kg. In the same
preparation, interruption of the arrhythmia was obtained by an injection of 15 mg/kg directly
into the ventricle. In normothermic or hypothermic dogs the same effect was obtained in
ventricular fibrillation induced by mechanical stimulation.
In anesthetized dogs, intravenous infusions of 40-80 mg converted digitalis-induced
ventricular arrhythmia to sinus rhythm. Also, acetylstrophanthidin-induced ventricular
tachycardia was suppressed at a minimal effective dose of lidocaine hydrochloride of 1 mg/kg
intravenously. Digitalis-induced ventricular tachycardia, which failed to respond to electro-
shock was converted to normal sinus rhythm by intravenous injection of lidocaine
hydrochloride 100 mg and ventricular tachycardia, induced by ouabain, was converted to
supraventricular tachycardia by intravenous injection of 1-2 mg/kg.
In unanesthetized dogs with ventricular arrhythmia induced by coronary occlusion,
intravenous injections of 5-10 mg/kg suppressed the arrhythmia. This effect could be

- 13 -
© The Aspen Group, 2017. All rights reserved
maintained by intravenous infusion with calculated lidocaine hydrochloride blood levels of
1-3 µg/mL.
Other effects in anesthetized intact dogs were depression of myocardial contractile force, heart
rate and femoral arterial pressure with lidocaine hydrochloride 0.5 to 6 mg/kg intravenously.
At 2.0 mg/kg intra-arterially the same effects were obtained but there was less diminution of
contractile force. In both anesthetized and conscious dogs, lidocaine hydrochloride in rapid
intravenous injection of 2, 4 and 8 mg/kg caused transient decrease of systolic arterial
pressure, venous pressure, cardiac output, mean ejection rate, rate of development of arterial
pressure, stroke work and calculated peripheral resistance. Heart rate was slightly increased.
Effects were greatest at 8 mg/kg and were more pronounced and of longer duration in
anesthetized dogs. There was return to basal levels in 3-5 minutes.
Absorption, Distribution and Excretion
In rats which received 14
C-labelled lidocaine hydrochloride by intravenous injection, rapid
uptake by all tissues was noted. Tissue distribution studies in monkeys have indicated: high
affinity for lung, spleen, kidney, stomach and adipose tissue; moderate affinity for brain and
most gastrointestinal organs; and low affinity for musculoskeletal tissue and skin. Similar
distribution has been observed in the dog.
Studies on plasma binding in monkey and man have indicated approximately 60% plasma
binding within the plasma concentration range usually seen in clinical use. However, plasma
binding was markedly reduced at concentrations of lidocaine hydrochloride exceeding
10 μg/mL, presumably due to saturation of the binding sites.
Studies in rabbit and rat have demonstrated that the liver is the principal site of metabolism.
In man, hepatic clearance studies have shown that approximately 70% of the lidocaine
hydrochloride passing through the liver was extracted. Microsomal enzyme systems are
primarily responsible for hepatic metabolism. The major degradative pathway appears to be
by conversion to monoethylglycinexylidide, followed by hydrolysis to 2,6,-xylidine; further
conversion to 4-hydroxy-2,6-xylidine appears to occur in man.
Up to 10% of administered lidocaine hydrochloride may be excreted in the urine as unchanged
drug. Although biliary secretion and intestinal absorption of lidocaine hydrochloride
metabolites have been reported in rats, there is no evidence of biliary secretion in man.
The pharmacokinetics of lidocaine hydrochloride has been studied in normal subjects and in
patients.
Following a single intravenous injection, or termination of a continuous intravenous infusion,
declining plasma concentration follows a biphasic curve. Plasma half-lives of 8 to 15 minutes
have been reported for the initial phase. Various studies have reported the mean half-life at
the terminal phase to be in the range 1.2 to 1.9 hours. The minimum effective antiarrhythmic
plasma concentration of lidocaine hydrochloride has been reported to be in the range of 1.0 to

- 14 -
© The Aspen Group, 2017. All rights reserved
1.2 μg/mL; concentrations higher than 5-6 μg/mL are associated with an increased risk of
toxicity.
TOXICOLOGY
Acute Toxicity
SPECIES SEX ROUTE LD50(mg/kg)
mice F i.v. 17.9
mice F i.p. 164
mice F i.m. 200
mice M i.m. 154
rat F i.v. 19.7
rat M i.v. 21.4
dog M & F i.m. 100
guinea pig F i.m. 73
guinea pig M i.m. 67
rabbit M i.m. 450
Acute intravenous studies were performed in rabbits which received six serial injections of 1,
2, 3, 4 or 5 mg/kg at 15 minute intervals. At the 2 mg/kg dose level, slight depression was
seen, beginning with the third injection. At 3 mg/kg there was depression and rigid extension
of limbs after the last 5 injections. At 5 mg/kg there was severe depression and rigid limb
extension after each injection; loss of righting reflex and convulsions began with the second
injection and there was gasping for breath after each of the last injections.
Dogs were given intravenous incremental doses at 30 minute intervals until death occurred.
Doses of 0.1 to 3.0 mg/kg were tolerated with minimal CNS or cardiovascular effects.
Convulsions, mydriasis, salivation, urination and defecation were observed after 10 mg/kg.
Respiratory arrest and death occurred in one dog after 30 mg/kg; cardiovascular collapse,
respiratory arrest and death occurred in remaining animals after 100 mg/kg. Mean arterial
blood pressure and heart rate increased briefly, beginning at 3.0 mg/kg, and decreased after
100 mg/kg. Myocardial conduction time was not significantly changed prior to 100 mg/kg
administration.
Acute local responses were studied in rats and rabbits following single intramuscular
injections of 2%, 4%, 6%, 8% and 10% solutions of lidocaine hydrochloride. Microscopic
examination revealed inflammatory changes with all solutions. In general, reactions produced
by 2% solutions were least, although lesions seen with all other concentrations were of similar
degree.

- 15 -
© The Aspen Group, 2017. All rights reserved
In rabbits sacrificed seven days after intramuscular administration, there was evidence of
marked muscle fiber regeneration; after 30 days there was virtually complete resolution of
inflammatory changes at the site of injection.
Subacute Toxicity
In one study, dogs received daily intravenous injections according to the following schedule:
0.1 mg/kg for 7 days, 0.3 mg/kg for 7 days, 1 mg/kg for 7 days and 3 mg/kg for 21 days. Mild
transient convulsions were seen in one dog at the high dose level. No other signs of toxicity
were observed. Gross and microscopic examination at autopsy did not reveal any drug related
effects.
In a second study, dogs received daily intravenous injections of 2.5, 5 or 10 mg/kg for 28
days. No overt symptoms were observed at the low dose level. At the 5 mg/kg level there
was transient sedation, ataxia, head tremor, prostration and emesis. At the 10 mg/kg level
there were severe tremors, muscular weakness, ataxia, prostration and convulsions, although
animals recovered within 5-10 minutes. No ECG or hemochemistry changes were seen. No
evidence of drug-related pathology was seen at autopsy. Injection sites showed inflammatory
changes in drug and saline-treated animals.
In rats which received daily intravenous doses of 1.5, 4.5 or 15.0 mg/kg for 14 days, overt
effects were observed only at the 15.0 mg/kg level, at which convulsions and death occurred.
Increased blood glucose levels were seen in male rats at all dose levels. At autopsy, no
changes were attributed to drug treatment. Mild inflammatory changes were seen at injection
sites.

- 16 -
© The Aspen Group, 2017. All rights reserved
BIBLIOGRAPHY
Ahmad K.
Distribution of lidocaine in blood and tissues after single doses and steady infusion. Research
Communications in Chemical Pathology and Pharmacology 1971;2:813-828.
Austin WG, Moran JM.
Cardiac and peripheral vascular effects of lidocaine and procainamide. Survey of Anesthesiol
1967;11:322-324.
Bassan MM.
Use of lidocaine by continuous infusion. Amer Heart J 1974;87:302-303.
Bedynek JL, Weinstein KN, Kah RE, Minton PR.
Ventricular tachycardia-control by intermittent intravenous administration of lidocaine
hydrochloride. JAMA 1966;198:553.
Benowitz N, et al.
Lidocaine disposition kinetics in monkey and man. Clin Pharmacol Ther 1974;16:87-98.
Braid DP, Scott DB.
The systemic absorption of local analgesic drugs. Brit J Anaesth 1965;37:394.
Canstantino RT, Crockett SE, Vasko JS.
Cardiovascular effects and dose-response relationships of lidocaine.
Circ 1967;36(Suppl. 2):89-90.
Collinsworth KA, et al.
The clinical pharmacology of lidocaine as an antiarrhythmic drug. Circ 1974;50:1217-1230.
Conrad KA, Byers JM, Finley PR, Burnham, L.
Lidocaine elimination: Effects of metoprolol and of propranolol. Clinical Pharmacology
Therapeutics 1983;33(2):133-138.
Crampton RS, Oriscello RG.
Petit and grand mal convulsions during lidocaine hydrochloride treatment of ventricular
tachycardia. JAMA 1968;204:201.
Engelsson SE, Eriksson S, Wahlqvist, Ortengren B.
Differences in tolerance to intravenous Xylocaine and Citanest, a new local anesthetic.
A double blind study in man. Proc 1st European Congress of Anesthesiology. Wien. 3.9 IX,
1962.
Ettinger E, Hayes J, Forde TP, Wanat FE, Killip T.
Lidocaine in ventricular arrhythmia. Clin Res 1967;15:201.

- 17 -
© The Aspen Group, 2017. All rights reserved
Feely J, Wilkinson GR, McAllister CB, Wood JJ.
Increased toxicity and reduced clearance of lidocaine by cimetidine. Annals of Internal Med
1982;96:592-594.
Fehmers MCO, Dunning AJ.
Intramuscularly and orally administered lidocaine in the treatment of ventricular arrhythmias
in acute myocardial infarction. Amer J Cardiol 1972;29:514.
Galindo AH, Sprouse JH.
The effect of anesthesia on cardiac excitability produced by single pulse electrical stimulation.
An experimental study. Anesth Analg 1962;41:659-669.
Gianelly RE, Spivak AP, von der Groeben J, Harrison DC.
Effect of lidocaine on ventricular arrhythmias in patients with coronary heart disease.
New Eng J Med 1967;277:1216.
Graham CF, Turner WM, Jones, JK.
Lidocaine-Propranolol Interactions. New Eng J Med 1981;304(21):1301.
Grossman J, Lubow LA, Frieden J, Rubin IL.
Lidocaine in cardiac arrhythmias. Arch Int Med 1968;121:396.
Ha et al.
Interaction between amiodarone and lidocaine. J Cardiovascular Pharmacol 1996; 28:533-
539.
Harris AS, Guerra CA, Liptak RA, Brigham, JC.
Effects of certain local anesthetic drugs upon ventricular tachycardia resulting from
myocardial infarction. J Appl Physiol 1956;8:499.
Harrison DC.
Antiarrhythmic actions of lidocaine. Annual Rev Med 1974;25:143-148.
Harrison DC, Sprouse HJ, Morrow AG.
The antiarrhythmic properties of lidocaine and procainamide. Clinical and physiological
studies of their cardiovascular effects in man. Circ 1963;28:486.
Hitchcock P, Keown KK.
The management of cardiac arrhythmias during cardiac surgery. Southern Med J
1959;52:702.
Jewitt DE, Kishon Y, Thomas M.
Lignocaine in the management of arrhythmias after acute myocardial infarction.
Lancet 1968;1(7537):266.

- 18 -
© The Aspen Group, 2017. All rights reserved
Katz MJ, Zitnik RS.
Direct current shock and lidocaine in the treatment of digitalis-induced ventricular
tachycardia. Amer J Cardiol 1966;18:252.
Knapp AB, Maguire W, Keren G, Karmen A, Levitt B, Miura DS, Somberg JC.
The cimetidine-lidocaine interaction. Annals of Internal Med 1983;98:174-177.
Lewis KB.
Treatment of ventricular arrhythmias with intravenous lidocaine in non-surgical patients.
Clin Res 1967;15:213.
Nattel et al.
Absence of pharmacokinetic interaction between amiodarone and lidocaine. Amer J Cardiol
1994; 73: 92-94
Orlando R, Piccoli P, De Martin S, et al.
Effect of the CYP 3A4 inhibitor erythromycin on the pharmacokinetics of lignocaine and its
pharmacologically active metabolites in subjects with normal and impaired liver function.
Br J Clin Pharmacology 2003; 55:86-93.
Orlando R, Piccoli P, De Martin S, et al.
Cytochrome P450 1A2 is a major determinant of lidocaine metabolism in vivo: effects of liver
function. Clin Pharmacol Ther 2004; 75:80-88.
Paradise RR, Stoelting VK.
Comparison of B.W. 62-235 and lidocaine with respect to cardiovascular, anti-arrhythmic and
local anesthetic actions. Arch Int Pharmacodyn 1966;161:17.
Ryden L, et al.
Effect of lignocaine on heart rate in patients with sinus bradycardia associated with proven
suspected acute myocardial infarction. Cardiovascular Research 1972;6:664.
Scott DB.
Blood levels of lidocaine following various routes of administration. Editors: Scott DB,
Julian DG. Lidocaine in the treatment of ventricular arrhythmias. Edinburgh and London
1971, E & S Livingstone, pp. 153-160.
Selden R, Sashara AA.
Central nervous system toxicity induced by lidocaine. Report of a case in a patient with liver
disease. JAMA 1967;202:908-909.
Siegmund et al.
Amiodarone interaction with lidocaine. J Cardiovascular Pharmacol 1993; 21: 513-515

- 19 -
© The Aspen Group, 2017. All rights reserved
Southerworth JL, McKusick VA, Pierce EC, Rawson FL.
Ventricular fibrillation precipitated by cardiac catheterization. Complete recovery of the
patient after forty-five minutes. JAMA 1950;143:717.
Spracklen FHW, Kimerling JJ, Besterman EMM, Litchfield JW.
Use of lignocaine in treatment of cardiac arrhythmias. Brit Med J 1968;1:89.
Steinhaus JE, Siebecker KL, Kimmey, JR.
Comparative effects of anesthetic agents on cardiac irritability during hypothermia.
JAMA 1959;169:8.
Stenson RE, et al.
Interrelationships of hepatic blood flow, cardiac output, and blood levels of lidocaine in man.
Circ 1971;XLIII:205-211.
Sung CY, Truant AP.
The physiological disposition of lidocaine and its comparison in some respects with procaine.
J Pharmacol Exp Ther 1954;112(4):432-443.
Tucker GT, Bax NDS, Lennard MS, Al-Asady S, Bharaj HS, Woods HF.
Effects of -adrenoceptor antagonists on the pharmacokinetics of lignocaine. Br J Clin
Pharmac 1984;17:21S-28S.
Usubiaga JE, Gustafson W, Moya F, Goldstein B.
The effect of intravenous lignocaine on cardiac arrhythmias during electroconvulsive therapy.
Brit J Anaesth 1967;39:867.
Wang J-S, Backman JT, Wen X, et al.
Fluvoxamine is a more potent inhibitor of lidocaine metabolism than ketoconazole and
erythromycin in vitro. Pharmacol Toxicol 1999; 85: 201-205.
Wang J-S, Backman JT, Taavitsainen P, et al.
Involvement of CYP 1A2 and CYP 3A4 in lidocaine N-deethylation and 3-jhydoxylation in
humans. Drug Metab Dispos 2000; 28:959-965.
Weiss WA.
Intravenous use of lidocaine for ventricular arrhythmias. Anesth Analg 1960;39:369.
Zeisler JA, Gaarder TC, De Mesquita SA.
Lidocaine excretion in breast milk. Drug Intel Clin Pharm 1986;20:691-693.

- 20 -
IMPORTANT: PLEASE READ
© The Aspen Group, 2017. All rights reserved
PART III: CONSUMER INFORMATION
XYLOCARD®
lidocaine hydrochloride injection
Read this carefully before you start taking
XYLOCARD and each time you get a refill. This
leaflet is a summary and will not tell you
everything about XYLOCARD. Talk to your
doctor, nurse, or pharmacist about your medical
condition and treatment and ask if there is any
new information about XYLOCARD.
ABOUT THIS MEDICATION
What the medication is used for:
XYLOCARD is used to treat abnormal heart
rhythms that may occur during heart surgery or
other procedures, heart attacks or due to other heart
conditions.
What it does:
XYLOCARD belongs to a class of drugs called
antiarrhythmic drugs. It works by reducing the
excitability of the heart which helps return the
heartbeat to normal.
When it should not be used:
Do not use XYLOCARD if you:
are allergic or sensitive to lidocaine
hydrochloride, to any of the nonmedicinal
ingredients in XYLOCARD or other local
anaesthetics (e.g. prilocaine, mepivacaine
or bupivacaine).
have Adams-Stokes syndrome, or severe
degrees of sinoatrial, atrioventricular or
intraventricular block.
What the medicinal ingredient is:
lidocaine hydrochloride
What the nonmedicinal ingredients are:
Sodium chloride, sodium hydroxide (and/or
hydrochloric acid) and water for injection
What dosage forms it comes in:
Liquid: 20 mg/mL
WARNINGS AND PRECAUTIONS
BEFORE you use XYLOCARD talk to your
doctor, nurse or pharmacist if you:
have a slow heartbeat.
have low levels of potassium in your
blood.
have epilepsy.
have low blood pressure.
have problems with your heart, liver or
kidneys.
have been diagnosed with acute porphyria.
are experiencing severe shock.
are pregnant or plan to become pregnant.
are breastfeeding or planning to breastfeed.
INTERACTIONS WITH THIS MEDICATION
As with most medicines, interactions with other
drugs are possible. Tell your doctor, nurse, or
pharmacist about all the medicines you take,
including drugs prescribed by other doctors,
vitamins, minerals, natural supplements, or
alternative medicines.
The following may interact with XYLOCARD:
Antiarrhythmic drugs used to treat heart
problems such as; mexiletine,
amiodaraone.
Other anesthetics such as; lidocaine.
Cimetidine used for stomach problems.
Fluvoxamine used to treat depression.
Drugs used to treat migraines.
Antipsychotic drugs.
Beta-blockers, used to treat heart
problems, such as; metoprolol, nadolol,
propranolol.
Drugs used to treat epilepsy and seizures
such as; carbamazepine, phenobarbital,
phenytoin, primidone.
PROPER USE OF THIS MEDICATION
Usual dose:
XYLOCARD must be administered by a doctor.
The doctor will decide on the dose you will be
given based on your individual needs.
Overdose:
Serious side effects can occur if you are given too
much XYLOCARD. Early signs that too much
XYLOCARD has been given include:
- 21 -
IMPORTANT: PLEASE READ
© The Aspen Group, 2017. All rights reserved
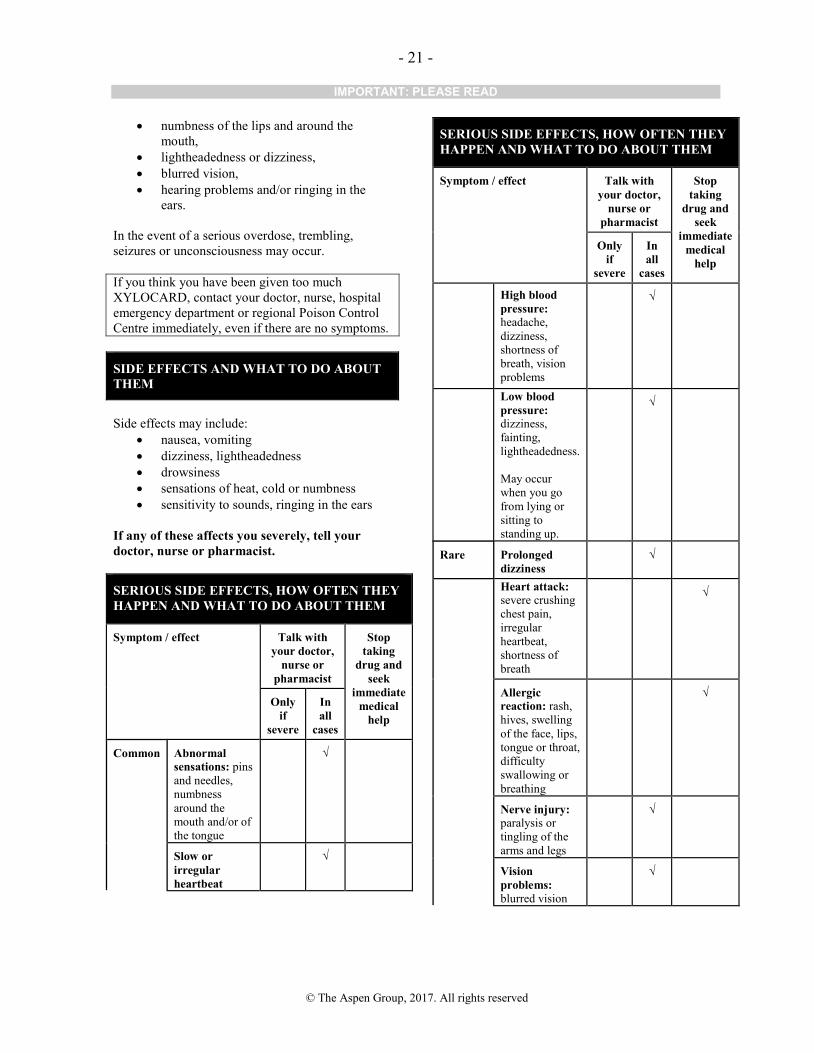
numbness of the lips and around the
mouth,
lightheadedness or dizziness,
blurred vision,
hearing problems and/or ringing in the
ears.
In the event of a serious overdose, trembling,
seizures or unconsciousness may occur.
If you think you have been given too much
XYLOCARD, contact your doctor, nurse, hospital
emergency department or regional Poison Control
Centre immediately, even if there are no symptoms.
SIDE EFFECTS AND WHAT TO DO ABOUT
THEM
Side effects may include:
nausea, vomiting
dizziness, lightheadedness
drowsiness
sensations of heat, cold or numbness
sensitivity to sounds, ringing in the ears
If any of these affects you severely, tell your
doctor, nurse or pharmacist.
SERIOUS SIDE EFFECTS, HOW OFTEN THEY
HAPPEN AND WHAT TO DO ABOUT THEM
Symptom / effect Talk with
your doctor,
nurse or
pharmacist
Stop
taking
drug and
seek
immediate
medical
help
Only
if
severe
In
all
cases
Common
Abnormal
sensations: pins
and needles,
numbness
around the
mouth and/or of
the tongue
√
Slow or
irregular
heartbeat
√
SERIOUS SIDE EFFECTS, HOW OFTEN THEY
HAPPEN AND WHAT TO DO ABOUT THEM
Symptom / effect Talk with
your doctor,
nurse or
pharmacist
Stop
taking
drug and
seek
immediate
medical
help
Only
if
severe
In
all
cases
High blood
pressure: headache,
dizziness,
shortness of
breath, vision
problems
√
Low blood
pressure:
dizziness,
fainting,
lightheadedness.
May occur
when you go
from lying or
sitting to
standing up.
√
Rare
Prolonged
dizziness
√
Heart attack: severe crushing
chest pain,
irregular
heartbeat,
shortness of
breath
√
Allergic
reaction: rash,
hives, swelling
of the face, lips,
tongue or throat,
difficulty
swallowing or
breathing
√
Nerve injury: paralysis or
tingling of the
arms and legs
√
Vision
problems: blurred vision
√

- 22 -
IMPORTANT: PLEASE READ
© The Aspen Group, 2017. All rights reserved
SERIOUS SIDE EFFECTS, HOW OFTEN THEY
HAPPEN AND WHAT TO DO ABOUT THEM
Symptom / effect Talk with
your doctor,
nurse or
pharmacist
Stop
taking
drug and
seek
immediate
medical
help
Only
if
severe
In
all
cases
Nervous
system
disorders: nervousness,
apprehension,
euphoria,
confusion,
twitching,
tremors,
convulsions,
unconsciousness
√
Respiratory
arrest: severe
trouble
breathing,
unconsciousness
√
This is not a complete list of side effects. For any
unexpected effects while taking XYLOCARD
contact your doctor, nurse or pharmacist.
HOW TO STORE IT
Store at room temperature (15-30ºC).
Keep out of reach and sight of children.
REPORTING SUSPECTED SIDE EFFECTS
You can report any suspected adverse reactions
associated with the use of health products to the
Canada Vigilance Program by one of the following 3
ways:
---------------------------------------------------------------------
Report online at
www.healthcanada.gc.ca/medeffect
Call toll-free at 1-866-234-2345
Complete a Canada Vigilance Reporting
Form and:
- Fax toll-free to 1-866-678-6789, or
- Mail to: Canada Vigilance Program
Health Canada
Postal Locator 0701D
Ottawa, Ontario
K1A 0K9
Postage paid labels, Canada Vigilance Reporting
Form and the adverse reaction reporting guidelines
are available on the MedEffect™ Canada Web site at
www.healthcanada.gc.ca/medeffect.
NOTE: Should you require information related to the
management of side effects, contact your health
professional. The Canada Vigilance Program does not
provide medical advice.
MORE INFORMATION
NOTE: This CONSUMER INFORMATION leaflet
provides you with the most current information at
the time of printing.
The most current information, the Consumer
Information leaflet plus the full Product
Monograph, prepared for health professionals can
be found at: www.aspenpharma.ca, or by contacting
the sponsor, Aspen Pharmacare Canada Inc. at: 1-
844-330-1213.
This leaflet was prepared by
Aspen Pharmacare Canada Inc, 111 Queen Street
East, Suite 450, Toronto, Ontario, M5C 1S2
XYLOCARD® is a registered trademark of the
AstraZeneca group of companies.
Last revised: August 15, 2017.


















