Procurement Policy for Clinical Services - Archived ... · Procurement Policy for Clinical...
40
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 1 of 40 Appendix 1 Procurement Policy for Clinical Services Document Version Control Version 0.1 – draft Pilot version 27/08/09 Version Version 10 draft PRCC governance framework finalised 08/09/09 Version 11 Final draft Legal opinion incorporated 09/09/09 Version Version
Transcript of Procurement Policy for Clinical Services - Archived ... · Procurement Policy for Clinical...
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 1 of 40
Appendix 1
Procurement Policy for Clinical Services
Document Version Control
Version 0.1 – draft
Pilot version 27/08/09
Version
Version 10 draft PRCC governance framework finalised
08/09/09
Version 11 Final draft Legal opinion incorporated 09/09/09
Version
Version
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 2 of 40
Document Management
Title of document Procurement Policy for Clinical Services
Type of document Policy
Description A Policy describing the framework by which NHS Northamptonshire will procure clinical services and ensure compliance with the PCT Procurement Guide for Health Services (2008) and the Principles and Rules for Co-operation and Competition (2008).
Target audience All staff
Author Chris Pallot, Associate Director of System Management
In Association with Governance Colleagues
Department System Management
Directorate Strategy and System Management
Approved by NHS Northamptonshire Board
Date of approval 30 September 2009
Next review date October 2010
Related documents Principles and Rules for Co-operation and Competition (2008)
PCT Procurement Guide for Health Services (2008)
Public Contracts Regulations 2006
Superseded documents
Procurement Policy for Clinical Services, September 2008
Internal distribution All staff
External distribution Freely available
Availability All ratified policies, strategies, procedures and protocols are published on the Trust Intranet and Public Website.
Contact details (of main contact for this document)
Name: Chris Pallot
Address: Francis Crick House
Tel: 01604 651312
E-mail: [email protected]
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 3 of 40
CONTENTS
Section Page
1. Executive Summary 4
2. Introduction 4
2.1 Objectives 4
2.2 Guiding Principles 5
2.3 Assessing the Need for Procurement 6
2.4 System Management 8
2.4.1 Market Concentration 9
2.5 Managing New and Existing Provider Relationships 9
2.5.1 Duty to Involve 10
2.6 Deciding if Procurement is Necessary 10
2.7 Any Willing Provider 12
3 Policy Framework 14
4. Governance Process 18
Appendices
Appendix A – Report for PCT Co-operation and Competition Panel where a decision not to competitively tender a service is recommended
19
Appendix B – Governance Framework 20
Section 1 = Generic Checklist 20
Section 2 = Mergers Checklist 24
Section 3 = Procurement Checklist 28
Section 4 = Conduct Checklist 31
Section 5 = Advertising and Promotional Activity Checklist 35
Section 6 = Process Compliance Checklist 36
Appendix C - Equality Impact Assessment Template 39
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 4 of 40
1. Executive Summary This Policy describes the framework by which NHS Northamptonshire will procure clinical services and ensure compliance with the legally binding EU Treaty procurement principles (the EU principles), the PCT Procurement Guide for Health Services (Department of Health, 2008) and the Principles and Rules for Co-operation and Competition (Department of Health 2008) (PRCC). Healthcare (i.e. clinical) services are classified as Part B services under the European Union (EU) Public Procurement Directives. This means that there are no formal legal requirements to tender them but there is a need to follow the principles therein, as far as practicable. This Policy ensures that a framework for complying with these regulations is clearly documented for staff to follow. This policy will ensure that market management mechanisms are embedded in the way that the organisation operates; that all options for service improvement are considered prior to procurement activities and that should a formal market testing process be needed it is carried out in a transparent and non-discriminatory manner. This document should be read in conjunction with NHS Northamptonshire‟s Market Development Strategy and the documents referred to above.
2. Introduction The Framework for Managing Choice Competition and Co-operation (Department of Health, 2008) lays out the principles and behaviours that are needed for a commissioner to develop World Class expertise and processes in its management of a health system. It recognises that market redesign and system management is not solely about re-tendering for services but about a set of behaviours and management techniques that are designed to build relationships, interpret and make judgements on the principles and rules for choice, Co-operation and competition and above all personal leadership. This document sets out the policy for procurement of clinical services, with the main objectives being:
2.1. Objectives
2.1.1 To support NHS Northamptonshire in securing its strategic objectives to
commission efficient and effective clinical services that represent best value for the population of Northamptonshire.
2.1.2 To support NHS Northamptonshire in developing a supply base that ensures local access to a continuing, and expanding, range of services that are deemed necessary to meet the needs of the local population.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 5 of 40
2.1.3 To provide clear guidance on NHS Northamptonshire‟s interpretation and implementation of the PCT Procurement Guide for Health Services (Department of Health, 2008), national policy and guidance and emerging judgements by the national Co-operation and Competition Panel.
2.1.4 To ensure all NHS Northamptonshire employees and service providers
are aware of the agreed approach and follow the guidance of this policy and the NHS Northamptonshire Standing Orders and Standing Financial Instructions (SFIs) of delegated authority.
2.1.5 To set out a clear framework for deciding when competitive procurement
or any willing provider processes are necessary; and when existing contracts can be maintained and improved using alternative improvement levers.
2.1.6 To demonstrate compliance with the EU Principles and the principles of
the PRCC should a challenge be made regarding a PCT procurement exercise.
2.1.7 To propose the establishment of a Partnership Development Forum with
NHS organisations that will ensure engagement, consultation and understanding of NHS Northamptonshire and current market incumbent positions. This will ensure that communication channels remain open with existing providers during the service review process. This will ensure all options regarding future procurement are explored with providers whilst still ensuring a transparent process is maintained should the service be subject to tender.
2.2. Guiding Principles
NHS Northamptonshire will when commissioning clinical services adhere to the EU Principles, PCT Procurement Guide (Department of Health, 2008), as defined by the Operating Framework in the PRCC and any other relevant aspects of EU procurement law, namely issues relating to conflict of interest, transparency and non-discrimination. For guidance on the EU Principles and their application, please see Section 2.6. The following is a summary of the PRCC:
2.2.1 Commissioners should use the providers best placed to meet patient needs.
2.2.2 Providers and commissioners must cooperate to ensure that the patient experience is of a seamless health service, and to ensure service continuity and sustainability.
2.2.3 Commissioning and procurement should be fair, transparent and non-
discriminatory.
2.2.4 Commissioners and providers should foster choice and ensure patients have reliable information to exercise more choice and control over their healthcare.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 6 of 40
2.2.5 Appropriate promotional activity is encouraged as long as it remains
consistent with patients‟ best interests and the brand and reputation of the NHS.
2.2.6 Providers must not discriminate against patients and must promote
equality.
2.2.7 Payment regimes must be transparent and fair.
2.2.8 Financial intervention in the system must be transparent and fair.
2.2.9 Mergers, acquisitions, de-mergers and joint ventures are permissible when demonstrated to be in patient and taxpayers‟ best interests and there remains sufficient choice and competition.
2.2.10 Vertical integration is permissible when demonstrated to be in patient
and taxpayers‟ best interests and protects the primacy of the GP gatekeeper function.
2.3 Assessing the Need for Procurement
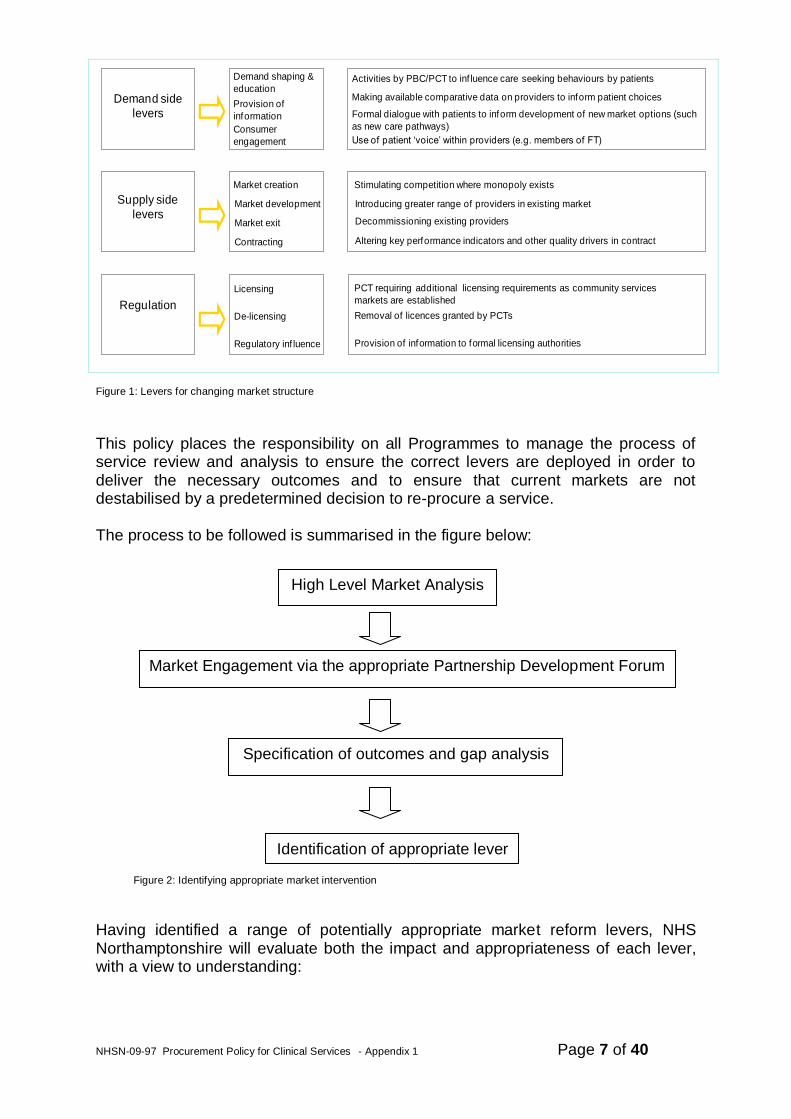
NHS Northamptonshire recognises that in order to deliver exceptional outcomes it is necessary to engage with current service providers to ensure a full analysis of all options is undertaken. Engaging with the market will inform both the future market state and help to assess the procurement route. NHS Northamptonshire will engage with market incumbents and potential new providers to determine their interest in entering, exiting or remaining within the market. This engagement will inform both the future market state within each priority market area and the procurement route required to deliver the change necessary. Only after the process of market analysis and engagement is concluded can NHS Northamptonshire determine the correct market reform levers to deploy. The range of „levers‟ available to us can be described within three broad categories, and are detailed in below in Figure 1.
Demand side levers
Supply side levers
Regulatory levers
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 7 of 40
Demand side
levers
Supply side
levers
Regulation
Demand shaping &
education
Market creation
Licensing
Provision of
information
Consumer
engagement
Activities by PBC/PCT to inf luence care seeking behaviours by patients
Making available comparative data on providers to inform patient choices
Formal dialogue with patients to inform development of new market options (such
as new care pathways)
Use of patient „voice‟ within providers (e.g. members of FT)
Market development
Market exit
Contracting
De-licensing
Regulatory inf luence
Stimulating competition where monopoly exists
Introducing greater range of providers in existing market
Decommissioning existing providers
Altering key performance indicators and other quality drivers in contract
PCT requiring additional licensing requirements as community services
markets are established
Removal of licences granted by PCTs
Provision of information to formal licensing authorities
Figure 1: Levers for changing market structure
This policy places the responsibility on all Programmes to manage the process of service review and analysis to ensure the correct levers are deployed in order to deliver the necessary outcomes and to ensure that current markets are not destabilised by a predetermined decision to re-procure a service.
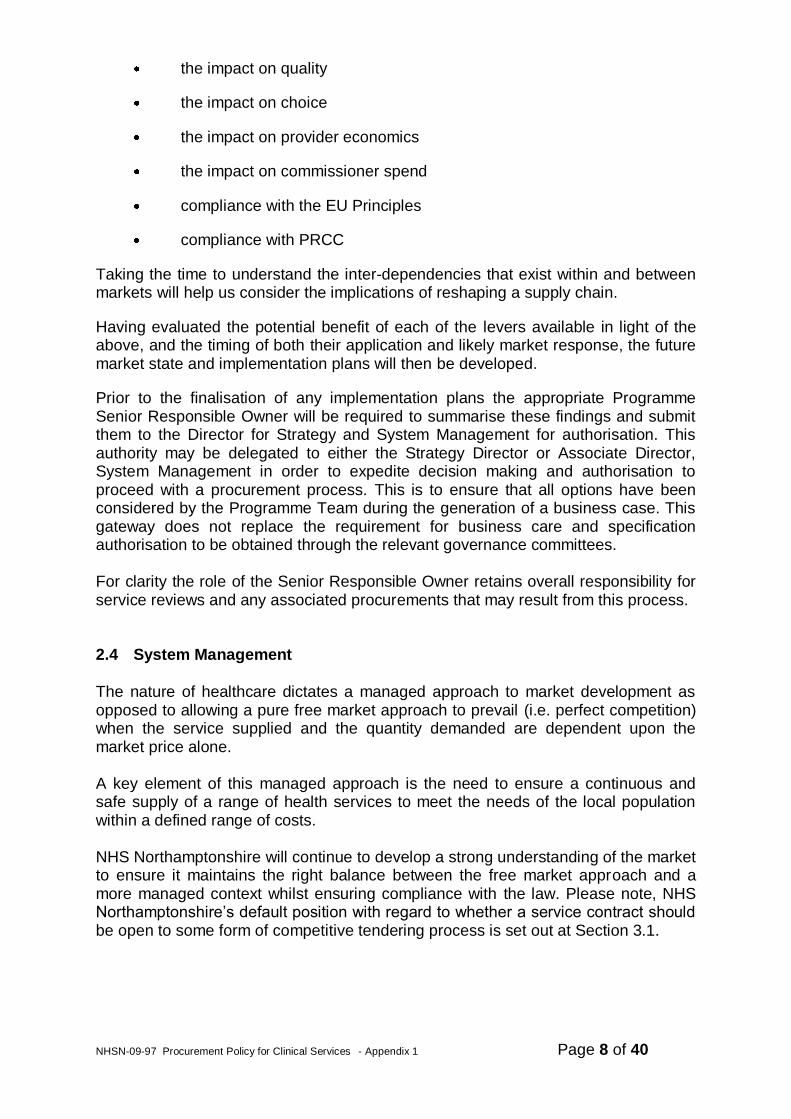
The process to be followed is summarised in the figure below:
Figure 2: Identifying appropriate market intervention
Having identified a range of potentially appropriate market reform levers, NHS Northamptonshire will evaluate both the impact and appropriateness of each lever, with a view to understanding:
High Level Market Analysis
Market Engagement via the appropriate Partnership Development Forum
Specification of outcomes and gap analysis
Identification of appropriate lever
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 8 of 40
the impact on quality
the impact on choice
the impact on provider economics
the impact on commissioner spend
compliance with the EU Principles
compliance with PRCC
Taking the time to understand the inter-dependencies that exist within and between markets will help us consider the implications of reshaping a supply chain.
Having evaluated the potential benefit of each of the levers available in light of the above, and the timing of both their application and likely market response, the future market state and implementation plans will then be developed.
Prior to the finalisation of any implementation plans the appropriate Programme Senior Responsible Owner will be required to summarise these findings and submit them to the Director for Strategy and System Management for authorisation. This authority may be delegated to either the Strategy Director or Associate Director, System Management in order to expedite decision making and authorisation to proceed with a procurement process. This is to ensure that all options have been considered by the Programme Team during the generation of a business case. This gateway does not replace the requirement for business care and specification authorisation to be obtained through the relevant governance committees. For clarity the role of the Senior Responsible Owner retains overall responsibility for service reviews and any associated procurements that may result from this process.
2.4 System Management
The nature of healthcare dictates a managed approach to market development as opposed to allowing a pure free market approach to prevail (i.e. perfect competition) when the service supplied and the quantity demanded are dependent upon the market price alone. A key element of this managed approach is the need to ensure a continuous and safe supply of a range of health services to meet the needs of the local population within a defined range of costs. NHS Northamptonshire will continue to develop a strong understanding of the market to ensure it maintains the right balance between the free market approach and a more managed context whilst ensuring compliance with the law. Please note, NHS Northamptonshire‟s default position with regard to whether a service contract should be open to some form of competitive tendering process is set out at Section 3.1.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 9 of 40
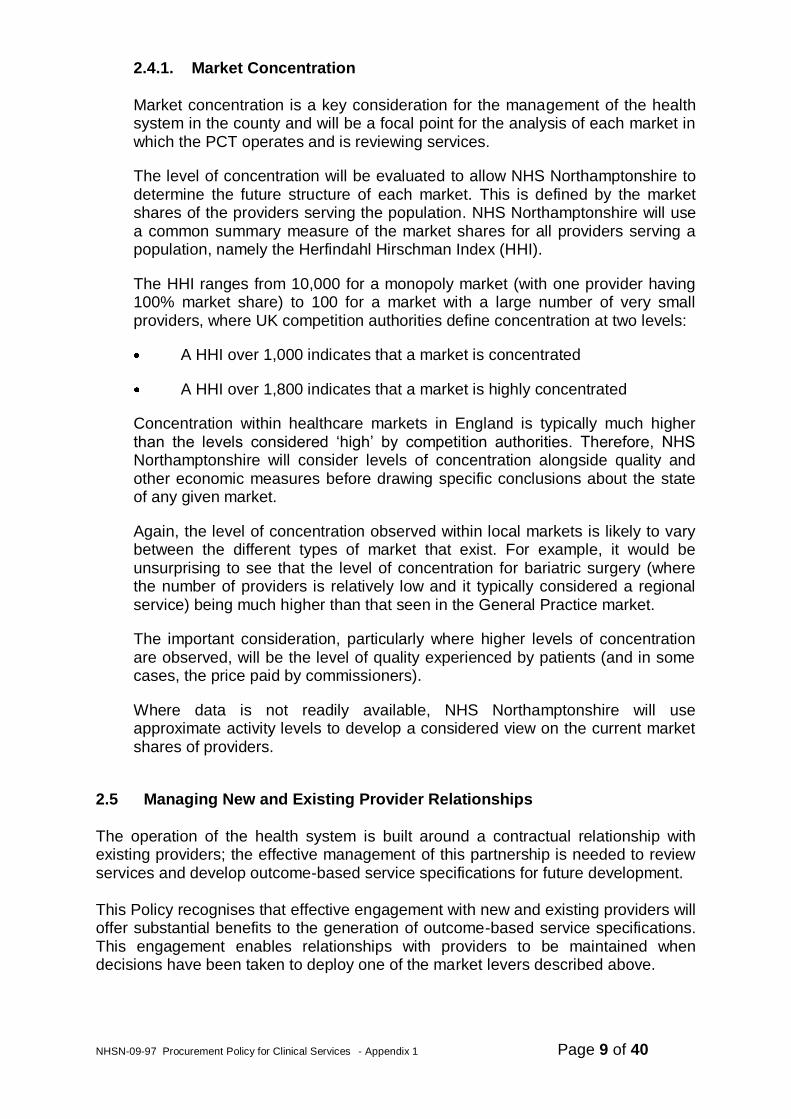
2.4.1. Market Concentration Market concentration is a key consideration for the management of the health system in the county and will be a focal point for the analysis of each market in which the PCT operates and is reviewing services.
The level of concentration will be evaluated to allow NHS Northamptonshire to determine the future structure of each market. This is defined by the market shares of the providers serving the population. NHS Northamptonshire will use a common summary measure of the market shares for all providers serving a population, namely the Herfindahl Hirschman Index (HHI).
The HHI ranges from 10,000 for a monopoly market (with one provider having 100% market share) to 100 for a market with a large number of very small providers, where UK competition authorities define concentration at two levels:
A HHI over 1,000 indicates that a market is concentrated
A HHI over 1,800 indicates that a market is highly concentrated
Concentration within healthcare markets in England is typically much higher than the levels considered „high‟ by competition authorities. Therefore, NHS Northamptonshire will consider levels of concentration alongside quality and other economic measures before drawing specific conclusions about the state of any given market.
Again, the level of concentration observed within local markets is likely to vary between the different types of market that exist. For example, it would be unsurprising to see that the level of concentration for bariatric surgery (where the number of providers is relatively low and it typically considered a regional service) being much higher than that seen in the General Practice market.
The important consideration, particularly where higher levels of concentration are observed, will be the level of quality experienced by patients (and in some cases, the price paid by commissioners).
Where data is not readily available, NHS Northamptonshire will use approximate activity levels to develop a considered view on the current market shares of providers.
2.5 Managing New and Existing Provider Relationships
The operation of the health system is built around a contractual relationship with existing providers; the effective management of this partnership is needed to review services and develop outcome-based service specifications for future development. This Policy recognises that effective engagement with new and existing providers will offer substantial benefits to the generation of outcome-based service specifications. This engagement enables relationships with providers to be maintained when decisions have been taken to deploy one of the market levers described above.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 10 of 40
A new Partnership Development Forum will be Chaired by the Director of Strategy and System Management or Associate Director, System Management and will ensure existing NHS providers remain engaged with the process of service reviews, especially when service redesign or re-provision is being considered. This is necessary to ensure consistency of message and also compliance with PRCC rule 3: “Commissioning and procurement should be fair, transparent and non-discriminatory” Stakeholder engagement will occur at key points in the service review process; in the initial information gathering phase via the Forum mentioned above and via market place events that will be held during the formal procurement phase (if applicable). This will explain the final outcome-based specification to potential providers and to ensure all parties are aware of the expectations being placed upon them. Any information provided to existing or potential providers will be done in an open and transparent way to ensure compliance with EU principles.
2.5.1 Duty to Involve
Section 242 of the consolidated NHS Act 2006 places a duty on NHS trusts, primary care trusts and strategic health authorities to make arrangements to involve patients and the public in service planning and operation, and in the development of proposals for changes. NHS Northamptonshire will conform to this requirement by involving relevant parties in the service review process which is managed through each strategic review process.
2.6 Deciding if Procurement is Necessary
In deciding whether a competitive tender process is necessary following a service review, NHS Northamptonshire will comply with the EU Principles, the guidance contained within the PCT Procurement Guide (2008) and in particular the procurement routes that are applicable to clinical services that are regarded as Part B services under EU legislation. Clinical services are “Part B Services”, as defined by the Public Contracts Regulations 2006 (the “Regulations”), and the full rigour of the Regulations does not apply to such services. For example, there is no obligation on NHS Northamptonshire to advertise a procurement via OJEU, though this is not prohibited. However, although the Regulations may not apply in full, case law has established that there is a legal requirement on PCTs to award contracts for Part B Services in such a manner as to satisfy the EU Treaty Principles. These EU Principles include the principles of transparency, equal treatment, proportionality, mutual recognition, non-discrimination and freedom to provide services.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 11 of 40
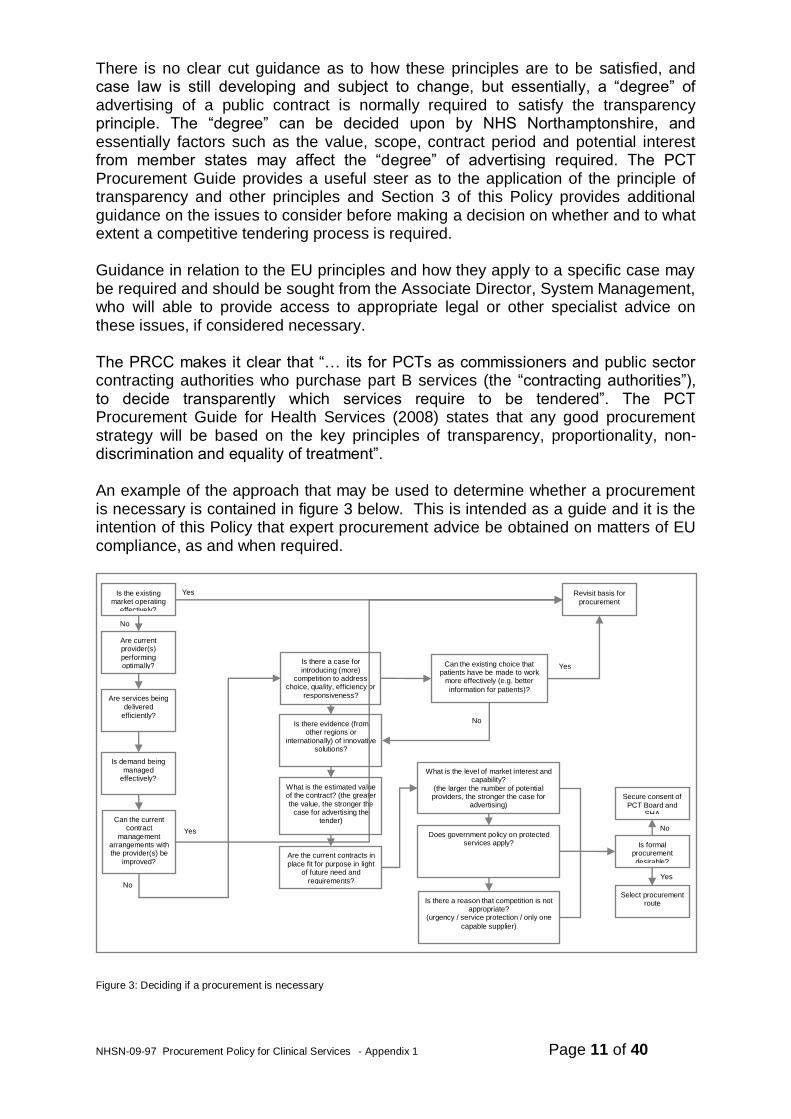
There is no clear cut guidance as to how these principles are to be satisfied, and case law is still developing and subject to change, but essentially, a “degree” of advertising of a public contract is normally required to satisfy the transparency principle. The “degree” can be decided upon by NHS Northamptonshire, and essentially factors such as the value, scope, contract period and potential interest from member states may affect the “degree” of advertising required. The PCT Procurement Guide provides a useful steer as to the application of the principle of transparency and other principles and Section 3 of this Policy provides additional guidance on the issues to consider before making a decision on whether and to what extent a competitive tendering process is required. Guidance in relation to the EU principles and how they apply to a specific case may be required and should be sought from the Associate Director, System Management, who will able to provide access to appropriate legal or other specialist advice on these issues, if considered necessary. The PRCC makes it clear that “… its for PCTs as commissioners and public sector contracting authorities who purchase part B services (the “contracting authorities”), to decide transparently which services require to be tendered”. The PCT Procurement Guide for Health Services (2008) states that any good procurement strategy will be based on the key principles of transparency, proportionality, non-discrimination and equality of treatment”. An example of the approach that may be used to determine whether a procurement is necessary is contained in figure 3 below. This is intended as a guide and it is the intention of this Policy that expert procurement advice be obtained on matters of EU compliance, as and when required.
Figure 3: Deciding if a procurement is necessary
Is the existing market operating
effectively?
Are current provider(s)
performing optimally?
Are services being
delivered
efficiently?
Is demand being
managed effectively?
No
Revisit basis for
procurement
Yes
Are the current contracts in
place fit for purpose in light of future need and
requirements?
Is there a case for
introducing (more) competition to address
choice, quality, efficiency or
responsiveness?
Is there evidence (from other regions or
internationally) of innovative solutions?
What is the estimated value of the contract? (the greater
the value, the stronger the case for advertising the
tender)
What is the level of market interest and capability?
(the larger the number of potential providers, the stronger the case for
advertising)
Does government policy on protected services apply?
Is there a reason that competition is not appropriate?
(urgency / service protection / only one
capable supplier)
Is formal procurement
desirable?
Select procurement route
Secure consent of
PCT Board and SHA
No
Yes
Can the current contract
management arrangements with the provider(s) be
improved?
Can the existing choice that patients have be made to work
more effectively (e.g. better
information for patients)?
No
Yes
No
Yes
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 12 of 40
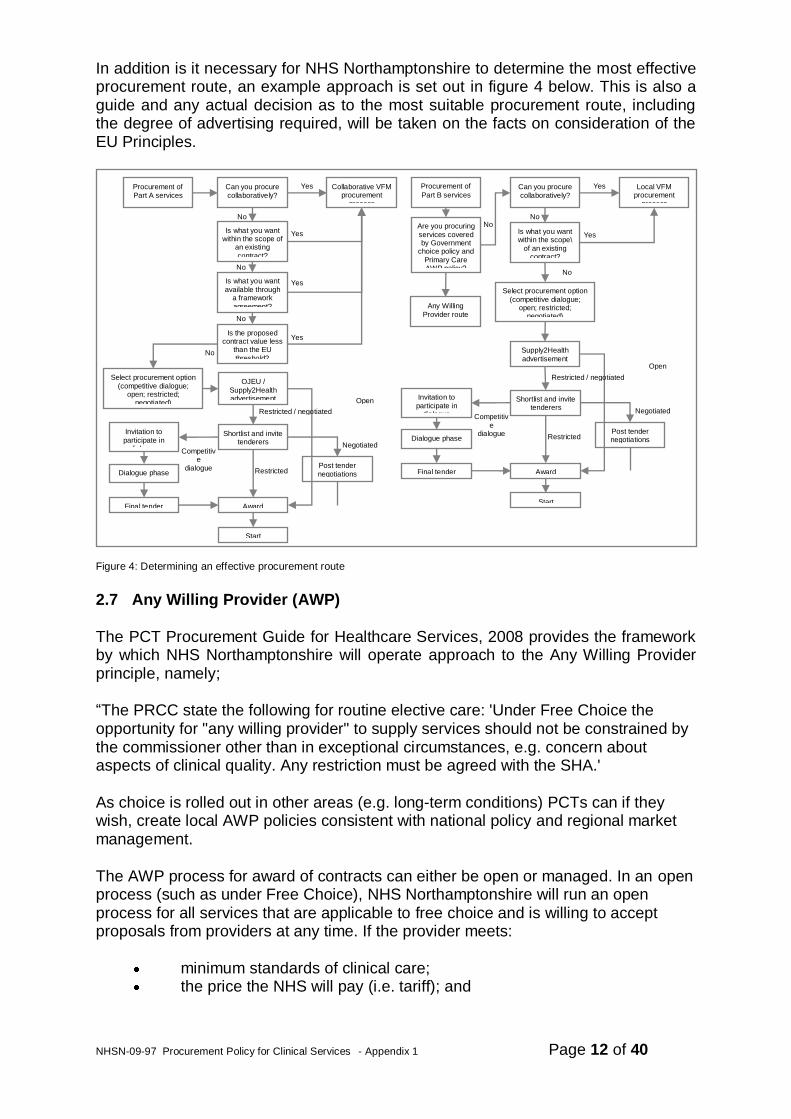
In addition is it necessary for NHS Northamptonshire to determine the most effective procurement route, an example approach is set out in figure 4 below. This is also a guide and any actual decision as to the most suitable procurement route, including the degree of advertising required, will be taken on the facts on consideration of the EU Principles.
Figure 4: Determining an effective procurement route
2.7 Any Willing Provider (AWP)
The PCT Procurement Guide for Healthcare Services, 2008 provides the framework by which NHS Northamptonshire will operate approach to the Any Willing Provider principle, namely;
“The PRCC state the following for routine elective care: 'Under Free Choice the opportunity for "any willing provider" to supply services should not be constrained by the commissioner other than in exceptional circumstances, e.g. concern about aspects of clinical quality. Any restriction must be agreed with the SHA.'
As choice is rolled out in other areas (e.g. long-term conditions) PCTs can if they wish, create local AWP policies consistent with national policy and regional market management.
The AWP process for award of contracts can either be open or managed. In an open process (such as under Free Choice), NHS Northamptonshire will run an open process for all services that are applicable to free choice and is willing to accept proposals from providers at any time. If the provider meets:
minimum standards of clinical care; the price the NHS will pay (i.e. tariff); and
Can you procure
collaboratively?
Is what you want within the scope of
an existing
contract?
Is what you want
available through a framework
agreement?
Is the proposed contract value less
than the EU
threshold?
No
No
No
Collaborative VFM procurement
process
Yes
Yes
Yes
No
Select procurement option
(competitive dialogue; open; restricted;
negotiated)
OJEU /
Supply2Health advertisement
Shortlist and invite tenderers
Post tender
negotiations
Award
Start
Restricted / negotiated
Open
Restricted
Negotiated
Invitation to
participate in dialogue
Dialogue phase
Final tender
Competitive
dialogue
Are you procuring
services covered by Government
choice policy and
Primary Care AWP policy?
Any Willing
Provider route
Procurement of
Part A services
Yes
Can you procure
collaboratively?
Is what you want within the scope\
of an existing contract?
No
No
Local VFM procurement
process
Yes
Yes
Select procurement option
(competitive dialogue; open; restricted;
negotiated)
Supply2Health
advertisement
Shortlist and invite tenderers
Post tender negotiations
Award
Start
Restricted / negotiated
Open
Restricted
Negotiated
Invitation to
participate in dialogue
Dialogue phase
Final tender
Competitiv
e dialogue
Procurement of
Part B services
No
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 13 of 40
the regulatory standards for IS providers registered with the Healthcare Commission and from April 2010 the registration requirements that will apply to all providers under the Health and Social Care Bill, then a standard NHS contract will be awarded to that provider.
NHS Northamptonshire will also undertake managed processes in relation to AWP providers. In these instances the PCT will award contracts from time to time for particular purposes; this may result in contracts not being awarded to providers even though they meet minimum standards. This managed process is essentially run as a simplified procurement and may be appropriate to address local issues such as demand for specialist services or to deal with performance issues.
NHS Northamptonshire will review whether it may move to a fully open process for all aspects of AWP in the future (e.g. for other than elective services).
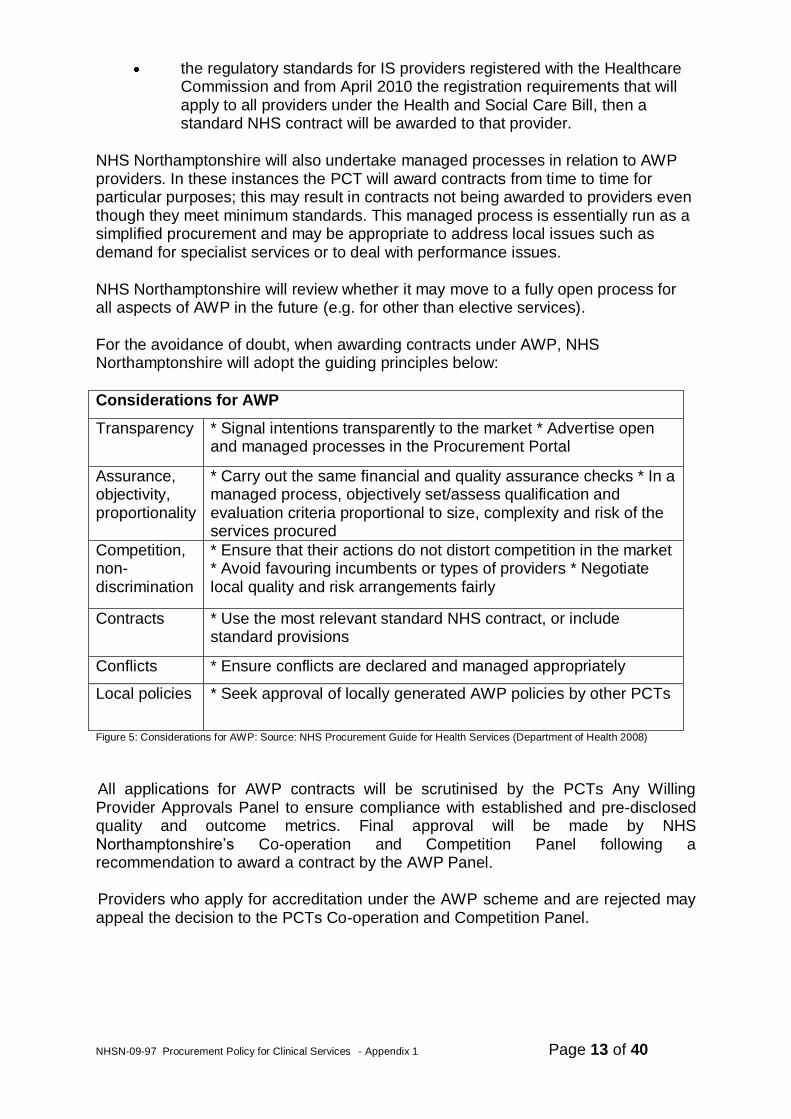
For the avoidance of doubt, when awarding contracts under AWP, NHS Northamptonshire will adopt the guiding principles below:
Considerations for AWP
Transparency * Signal intentions transparently to the market * Advertise open and managed processes in the Procurement Portal
Assurance, objectivity, proportionality
* Carry out the same financial and quality assurance checks * In a managed process, objectively set/assess qualification and evaluation criteria proportional to size, complexity and risk of the services procured
Competition, non-discrimination
* Ensure that their actions do not distort competition in the market * Avoid favouring incumbents or types of providers * Negotiate local quality and risk arrangements fairly
Contracts * Use the most relevant standard NHS contract, or include standard provisions
Conflicts * Ensure conflicts are declared and managed appropriately
Local policies * Seek approval of locally generated AWP policies by other PCTs
Figure 5: Considerations for AWP: Source: NHS Procurement Guide for Health Services (Department of Health 2008)
All applications for AWP contracts will be scrutinised by the PCTs Any Willing Provider Approvals Panel to ensure compliance with established and pre-disclosed quality and outcome metrics. Final approval will be made by NHS Northamptonshire‟s Co-operation and Competition Panel following a recommendation to award a contract by the AWP Panel. Providers who apply for accreditation under the AWP scheme and are rejected may appeal the decision to the PCTs Co-operation and Competition Panel.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 14 of 40
3. Policy Framework
3.1 Reflecting the strong theoretical benefits of competition, it is the key premise of this policy that contesting health services should be NHS Northamptonshire‟s default position when commissioning a new service for which there is no existing provider or any existing service. However, NHS Northamptonshire shall ensure that prior to awarding any contract under this policy, each case will be considered according to its facts in order to comply with the EU Principles (described in more detail at Section 2.6) and the PRCC.
NB: In the context of the above, some examples of facts to take into account on deciding whether and to what extent a competitive process is desirable following any service review include but are not limited to:
A previously awarded contract term is due to end. There are concerns about the performance of the market in terms of
quality, access, appropriateness and choice, value for money or effectiveness of an existing service. This could be evidenced through data collection and/or commissioner judgement or be predicted as a result of a required significant change in an outcome-based service specification.
The National Co-Operation and Competition Panel have issued a judgement on a related or similar case
Where a contract is for a high value and it can be demonstrated that a number of interested providers exist
3.2. There are a number of other factors that may be applicable to a particular service area that NHS Northamptonshire could take into account when deciding whether and to what extent a competitive tender process is necessary and to adopt a preferred provider approach to the identification of a future service provider. However, any decision taken not to competitively tender must also be compliant with the EU Principles and the PRCC as set out in this Policy. .
The following are examples of factors that may be taken into account when deciding whether or not to tender a service, although prior to making such a decision, please refer to the contacts at Section 2.6 if there is any uncertainty as to how to apply the EU Principles:
The service is a specialised service where provider designation has already taken place at a national or regional level.
Where the time required to undertaking a contested approach will jeopardise continuity of service provision or timely delivery of a new service.
Where the service to be procured has such strong service alliances with an existing service that an extension to an existing agreement is appropriate. Specialist legal advice will be sought in this instance to ensure the contract variation does not amount to a contract that is viewed as “new” in law.
Where the cost of undertaking a contested approach cannot be justified in light of the contract value.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 15 of 40
Where NHS Northamptonshire wishes to encourage provision from within a sector that might otherwise not prevail through a contested approach.
Where there is not reasonable expectation of more than one player coming forward to compete to provide services i.e. the lack of supply in the market will mean that the benefits of competition will not be realised.
Where failing to award a contract to a preferred provider would put other core services at risk i.e. recognising the need to safe guard against unintended consequences relating to service viability and tipping points.
Where NHS Northamptonshire is protecting a public service (e.g. services for which the NHS is best placed to meet patients‟ needs).
There are legal reasons e.g. services protected by monopoly rights in accordance with a legal or administrative instrument, or other considerations beyond NHS Northamptonshire‟s control that require an urgent response.
3.3 NHS Northamptonshire recognises the principle of proportionality and that from a practical perspective it does not have the resource to formally tender all services. However, it also recognises that it is legally required to ensure that all services under this policy are awarded in compliance with the EU Principles.
3.4 After assessment against the criteria outlined above (section 3.1-3.4), where a
decision is made by any NHS Northamptonshire commissioner or other employee not to tender a service, particularly where the value is above that required by the SFI‟s limit to tender, a report will be submitted by the Senior Responsible Owner to NHS Northamptonshire‟s Co-Operation and Competition panel for consideration (see Appendix A for report template). Where a decision is taken not to tender a contract for new or significantly changed services, Board approval will also be required and the SHA informed.]
3.5 For all other NHS Northamptonshire procurements where it does competitively
tender a Part B service, the NHS Northamptonshire will reside over the procurement route and decision to contract award. In all instances of competitive tender the NHS Supply2Health portal will be used to advertise the opportunity for contracts with a total contract value of above £100,000 (this typically represents an annual value of around £33,000 based on the move to three year contracts). This is to be considered as the minimum requirement for compliance with EU Principles and further advertising may be necessary to comply with all requirements which will be decided on a case by case basis.
For contracts that are above the OJEU (Official Journal of the European Union) limit (currently £139,893) then NHS Northamptonshire is legally required under the Regulations to notify OJEU of a contract award no later than 48 days after the award of contract or conclusion of a framework agreement. In some cases, in order to appeal to markets outside the UK, NHS Northamptonshire may also wish to advertise Part B clinical service opportunities on OJEU. 3.6 For routine elective services and other services considered appropriate NHS
Northamptonshire will give consideration to the Any Willing Provider Model (AWP) model. This means that organisations who meet certain quality and
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 16 of 40
financial viability criteria will be „accredited‟ to provide a certain service at national tariff or an agreed local alternative price, which NHS Northamptonshire considers the NHS is willing to pay.
NB: The PCT Procurement Guide for Health Services (May 2008) states: For routine elective services, the principles of free choice of provider for patients and the opportunity for any willing provider to supply services should not be constrained by commissioners. Other than in exceptional circumstances, there should be no guarantees of volume or payment in any contract given. PCT‟s, through contracts, give permission for the provider to supply services to their population without any promises regarding income. PCT‟s should give such contracts only to providers who can demonstrate that they meet national minimum quality criteria, as set out by the Care Quality Commission. It is, in effect, a local approval process for providers with the intention that competition is encouraged within a range of services rather than for them. This means that for providers looking to supply a routine elective service or other appropriate services, including those developed through practice based commissioning (PBC), tendering is not required, but in the interests of openness and non-discrimination, consideration ought to be given to advertising to ensure competition. 3.7 NHS Northamptonshire may, from time to time and, with regard to our strategic
priorities, assess the applicability of the AWP model beyond routine elective services.
3.8 NHS Northamptonshire will use the NHS Supply2Health portal to advertise
opportunities specifically targeted at AWP, along with announcements of any AWP contracts awarded.
3.9 NHS Northamptonshire supports the development of a rich mix of locally based,
service providers and as such will consider the ways in which it can support lower barriers to entry and assist market exit where this is desirable.
3.10 NHS Northamptonshire will ensure it recognises all other contracting routes
available to ensure the appropriateness of service delivery in terms of choice, access and quality outcomes. This will include but not be limited to:
APMS
SPMS
Social Enterprise
Local Enhanced Services
3.11 The impact of the Office of Fair Trading (OFT's) and the European Commission (EC's) competition jurisdiction is still in a state of development. OFT/EC has clear jurisdiction over non-governmental healthcare providers, but the situation in relation to NHS bodies is not definitive. EU law is still developing. There have
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 17 of 40
been a number of cases, but these have left several points yet to be clarified, which may come as a result of future case law. The present Department of Health view of the application of competition law to NHS bodies' activity is in-line with that of the OFT, which can be summarised as : NHS bodies (when acting in their capacity as purchasers and providers of health services ) are not subject to the Competition Act 1998 (CA98) as they are not presently regarded as undertakings for the purposes of CA98. There is always the possibility that the case law will develop in this area, and as the position changes, we will review our policy.
3.12 NHS Northamptonshire will provide assurance regarding any probity issues
relating to patient choice i.e. ensure patients are furnished with appropriate information regarding their choices and that any financial or other interest in a particular provider is declared by the referrer.
3.13 Employment issues relating to TUPE will be considered early in the pre-tender
process. Usually TUPE rules will apply where there is a defined group of staff carrying out a defined service for a single commissioner (i.e. on a one-to-one basis). Procurements will be considered on a case by case basis and specialist advice sought.
3.14 TUPE regulations do not apply to an AWP model and, where appropriate, legal
advice will be sought for individual cases where a service is provided to multiple commissioners (i.e. on a one-to-many basis).
3.15 The principles set out in this policy will apply equally to all types of service
provider including the NHS Northamptonshire own service provider arm and primary care providers.
3.16 Where contracts are being agreed with a Foundation Trust or commercial
partner the Contracting Department will be responsible for seeking legal opinion to ensure a robust agreement is reached.
3.17 All Providers who submit a response to an Any Willing Provider or competitive
tender specification must be registered with SID4Health. This is the sole official NHS supplier information database holding supplier pre-qualification information. The service is shared among all purchasing organisations in the NHS and is free of charge to all suppliers and NHS users.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 18 of 40
4. Governance Processes
4.1 In order to demonstrate that the EU Principles and the PRCC have been followed when commissioning clinical services the Senior Responsible Owner (or their representative) will submit the specification, the summary of the procurement process followed and the completed PRCC governance framework to NHS Northamptonshire‟s Co-operation and Competition Panel (CCP).
There are a series of PRCC checklists within NHS Northamptonshire‟s governance framework (Appendix B) that will be used to demonstrate PRCC compliance, namely:
Section 1 = Generic Checklist
Section 2 = Mergers Checklist
Section 3 = Procurement Checklist
Section 4 = Conduct Checklist
Section 5 = Advertising and Promotional Activity Checklist
Section 6 = Process Compliance Checklist
4.2 The CCP will have responsibility for ensuring that the processes followed during any procurement phase are in accordance with the PRCC and the EU Principles, using these checklists. Members of the CCP will review the submission received, paying attention to the completed PRCC Governance Framework, in order to come to a decision as to whether the process has been compliant and can proceed to contract award.
4.3 Once the CCP is assured that due process has been followed, and ensuring all other requirements are satisfied, they will award the contract and arrange for it to be signed.
4.4 The CCP will advise the Resources & Performance Committee (RPC), by way of the completed PRCC Governance Framework, of any contracts that have been awarded.
The RPC (which is a formally constituted Committee of the Board) has delegated responsibility for ensuring that the decisions made in relation to commissioning, procurement and tendering are PRCC compliant.
4.5 Members of the RPC will review the completed PRCC Governance Framework and ensure that any identified governance issues have associated action plans to rectify these. The decision as to whether there are any governance issues and the action taken as a result of using this assessment is the responsibility of the Board, although delegated to the RPC.
4.6 The RPC will report on an exception basis to the Board, any governance issues and the action taken, that have been identified through the process outlined above. Thus, the Board will take assurance that procurement activity is PRCC compliant unless advised otherwise through the exception reports.
NHSN-09-97 Procurement Policy for Clinical Services - Appendix 1 Page 19 of 40
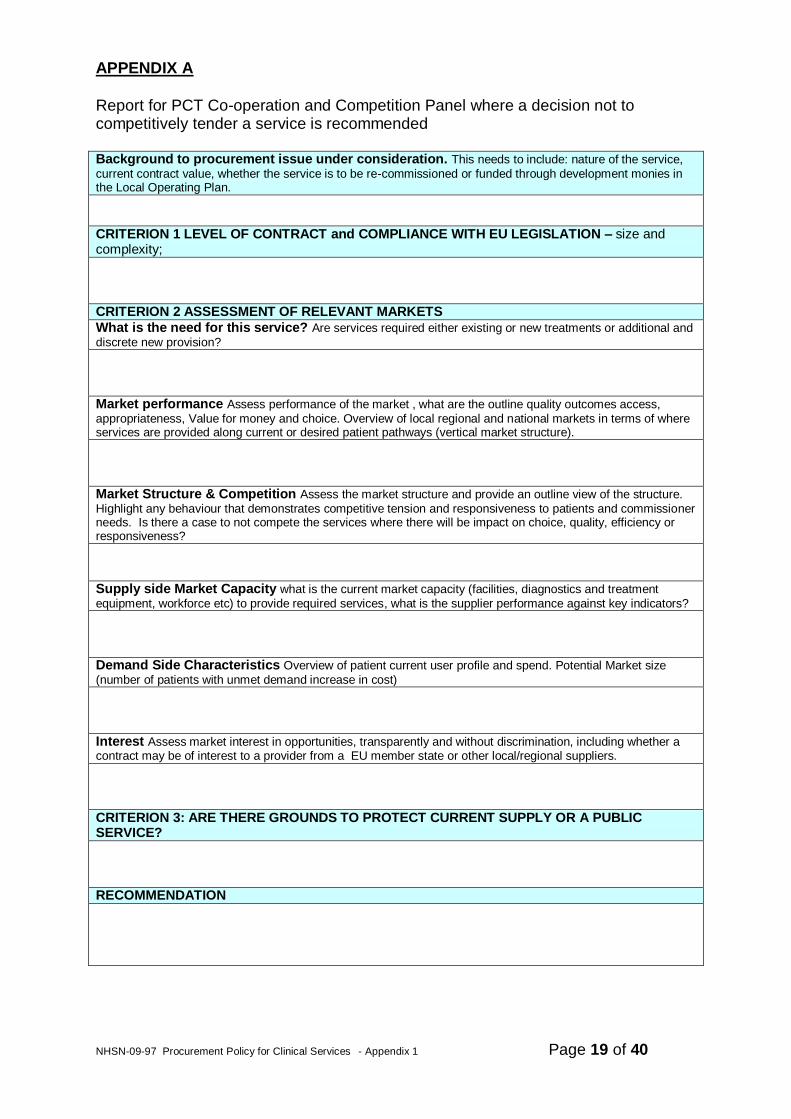
APPENDIX A
Report for PCT Co-operation and Competition Panel where a decision not to competitively tender a service is recommended Background to procurement issue under consideration. This needs to include: nature of the service,
current contract value, whether the service is to be re-commissioned or funded through development monies in the Local Operating Plan.
CRITERION 1 LEVEL OF CONTRACT and COMPLIANCE WITH EU LEGISLATION – size and complexity;
CRITERION 2 ASSESSMENT OF RELEVANT MARKETS
What is the need for this service? Are services required either existing or new treatments or additional and
discrete new provision?
Market performance Assess performance of the market , what are the outline quality outcomes access,
appropriateness, Value for money and choice. Overview of local regional and national markets in terms of where services are provided along current or desired patient pathways (vertical market structure).
Market Structure & Competition Assess the market structure and provide an outline view of the structure.
Highlight any behaviour that demonstrates competitive tension and responsiveness to patients and commissioner needs. Is there a case to not compete the services where there will be impact on choice, quality, efficiency or responsiveness? Supply side Market Capacity what is the current market capacity (facilities, diagnostics and treatment
equipment, workforce etc) to provide required services, what is the supplier performance against key indicators?
Demand Side Characteristics Overview of patient current user profile and spend. Potential Market size
(number of patients with unmet demand increase in cost)
Interest Assess market interest in opportunities, transparently and without discrimination, including whether a contract may be of interest to a provider from a EU member state or other local/regional suppliers.
CRITERION 3: ARE THERE GROUNDS TO PROTECT CURRENT SUPPLY OR A PUBLIC SERVICE?
RECOMMENDATION
Procurement Policy V1 / Aug 2009 Page 20 of 40
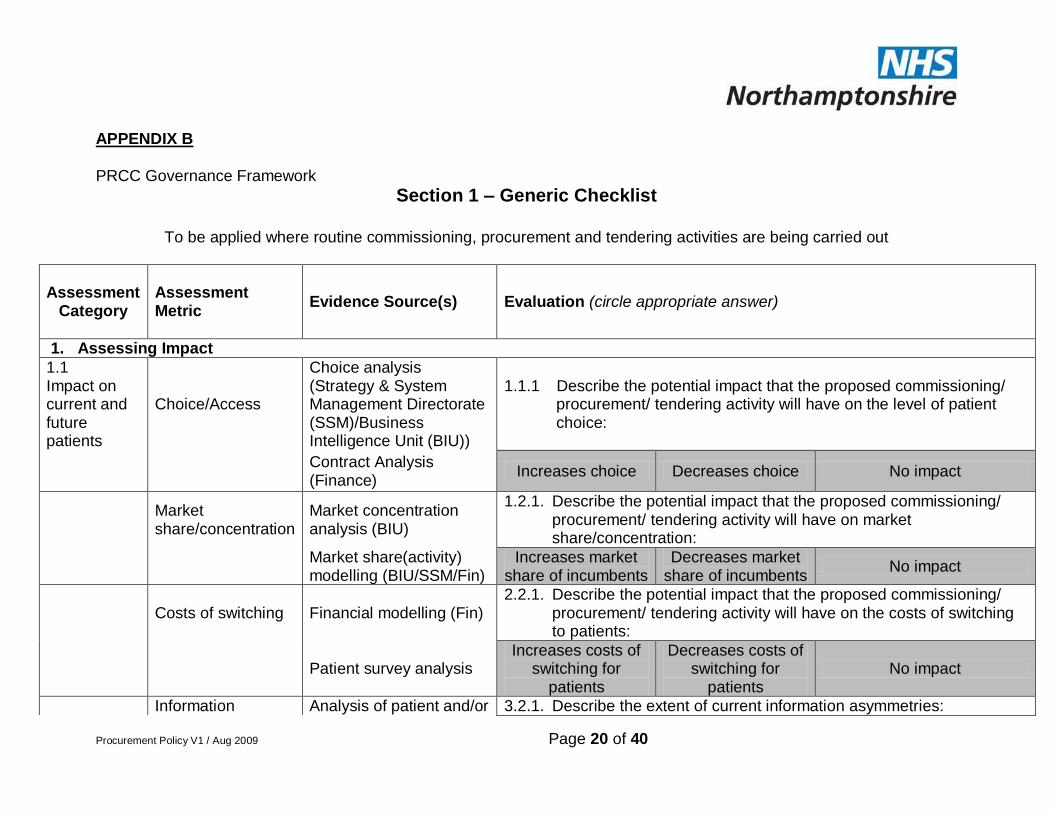
APPENDIX B
PRCC Governance Framework
Section 1 – Generic Checklist
To be applied where routine commissioning, procurement and tendering activities are being carried out
Assessment
Category
Assessment Metric
Evidence Source(s) Evaluation (circle appropriate answer)
1. 1. Assessing Impact
1.1 Impact on current and future patients
Choice/Access
Choice analysis (Strategy & System Management Directorate (SSM)/Business Intelligence Unit (BIU))
1.1.1 Describe the potential impact that the proposed commissioning/ procurement/ tendering activity will have on the level of patient choice:
Contract Analysis (Finance)
Increases choice Decreases choice No impact
Market share/concentration
Market concentration analysis (BIU)
1.2.1. Describe the potential impact that the proposed commissioning/ procurement/ tendering activity will have on market share/concentration:
Market share(activity) modelling (BIU/SSM/Fin)
Increases market share of incumbents
Decreases market share of incumbents
No impact
Costs of switching Financial modelling (Fin) 2.2.1. Describe the potential impact that the proposed commissioning/
procurement/ tendering activity will have on the costs of switching to patients:
Patient survey analysis Increases costs of
switching for patients
Decreases costs of switching for
patients No impact
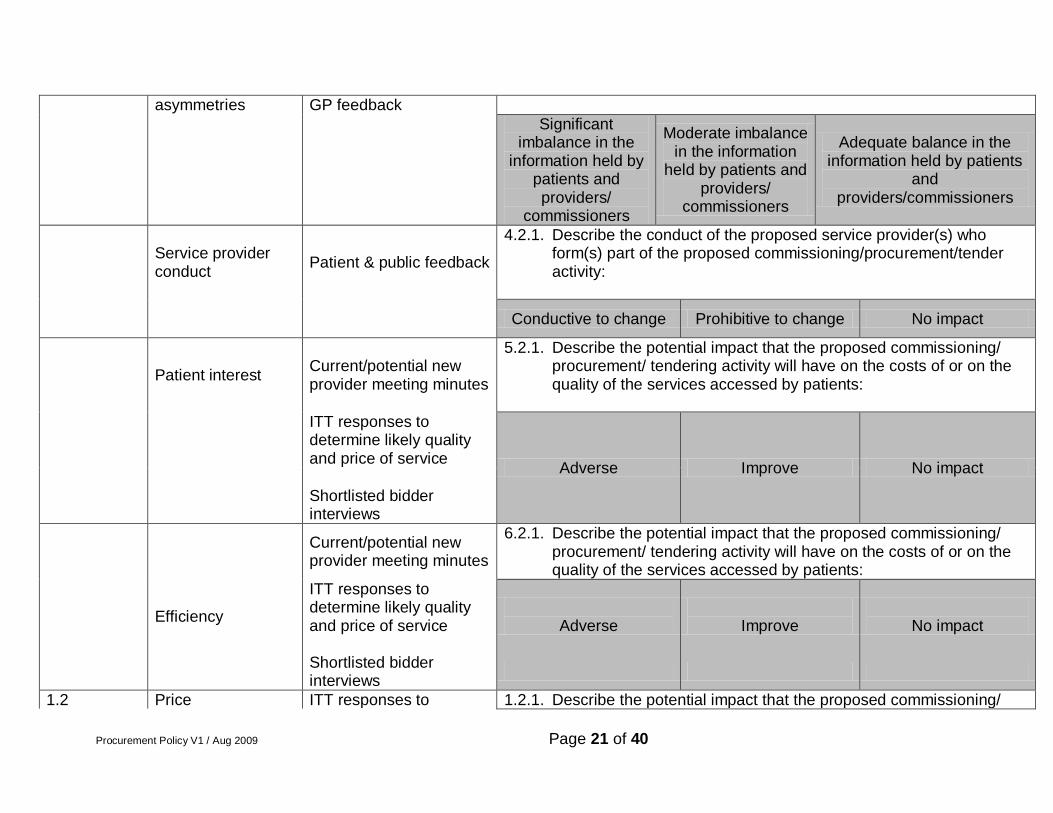
Information Analysis of patient and/or 3.2.1. Describe the extent of current information asymmetries:
Procurement Policy V1 / Aug 2009 Page 21 of 40
asymmetries GP feedback
Significant imbalance in the
information held by patients and providers/
commissioners
Moderate imbalance in the information
held by patients and providers/
commissioners
Adequate balance in the information held by patients
and providers/commissioners
Service provider conduct
Patient & public feedback
4.2.1. Describe the conduct of the proposed service provider(s) who form(s) part of the proposed commissioning/procurement/tender activity:
Conductive to change Prohibitive to change No impact
Patient interest Current/potential new provider meeting minutes
5.2.1. Describe the potential impact that the proposed commissioning/ procurement/ tendering activity will have on the costs of or on the quality of the services accessed by patients:
ITT responses to determine likely quality and price of service
Adverse Improve No impact
Shortlisted bidder interviews
Current/potential new provider meeting minutes
6.2.1. Describe the potential impact that the proposed commissioning/ procurement/ tendering activity will have on the costs of or on the quality of the services accessed by patients:
Efficiency
ITT responses to determine likely quality and price of service
Adverse
Improve
No impact
Shortlisted bidder interviews
1.2 Price ITT responses to 1.2.1. Describe the potential impact that the proposed commissioning/
Procurement Policy V1 / Aug 2009 Page 22 of 40
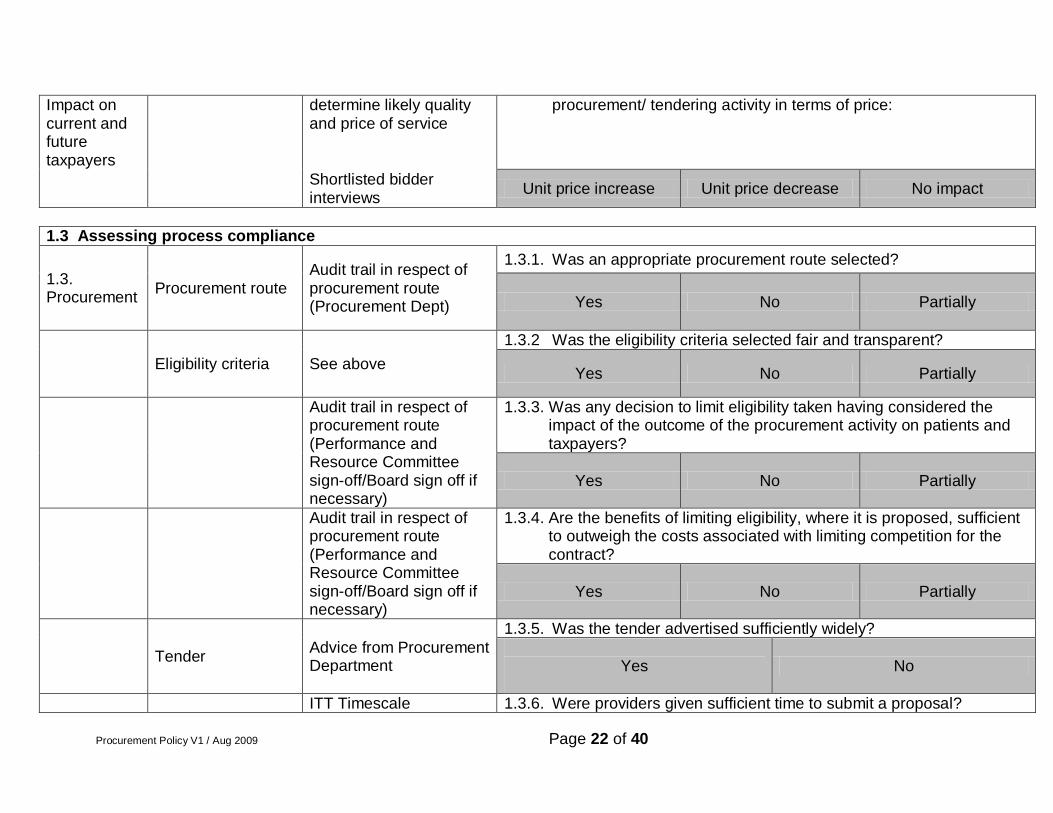
Impact on current and future taxpayers
determine likely quality and price of service
procurement/ tendering activity in terms of price:
Shortlisted bidder interviews
Unit price increase Unit price decrease No impact
1.3 Assessing process compliance
1.3. Procurement
Procurement route Audit trail in respect of procurement route (Procurement Dept)
1.3.1. Was an appropriate procurement route selected?
Yes No Partially
Eligibility criteria See above
1.3.2 Was the eligibility criteria selected fair and transparent?
Yes No Partially
Audit trail in respect of procurement route (Performance and Resource Committee sign-off/Board sign off if necessary)
1.3.3. Was any decision to limit eligibility taken having considered the impact of the outcome of the procurement activity on patients and taxpayers?
Yes No Partially
Audit trail in respect of procurement route (Performance and Resource Committee sign-off/Board sign off if necessary)
1.3.4. Are the benefits of limiting eligibility, where it is proposed, sufficient to outweigh the costs associated with limiting competition for the contract?
Yes No Partially
Tender Advice from Procurement Department
1.3.5. Was the tender advertised sufficiently widely?
Yes
No
ITT Timescale 1.3.6. Were providers given sufficient time to submit a proposal?
Procurement Policy V1 / Aug 2009 Page 23 of 40
Yes
No
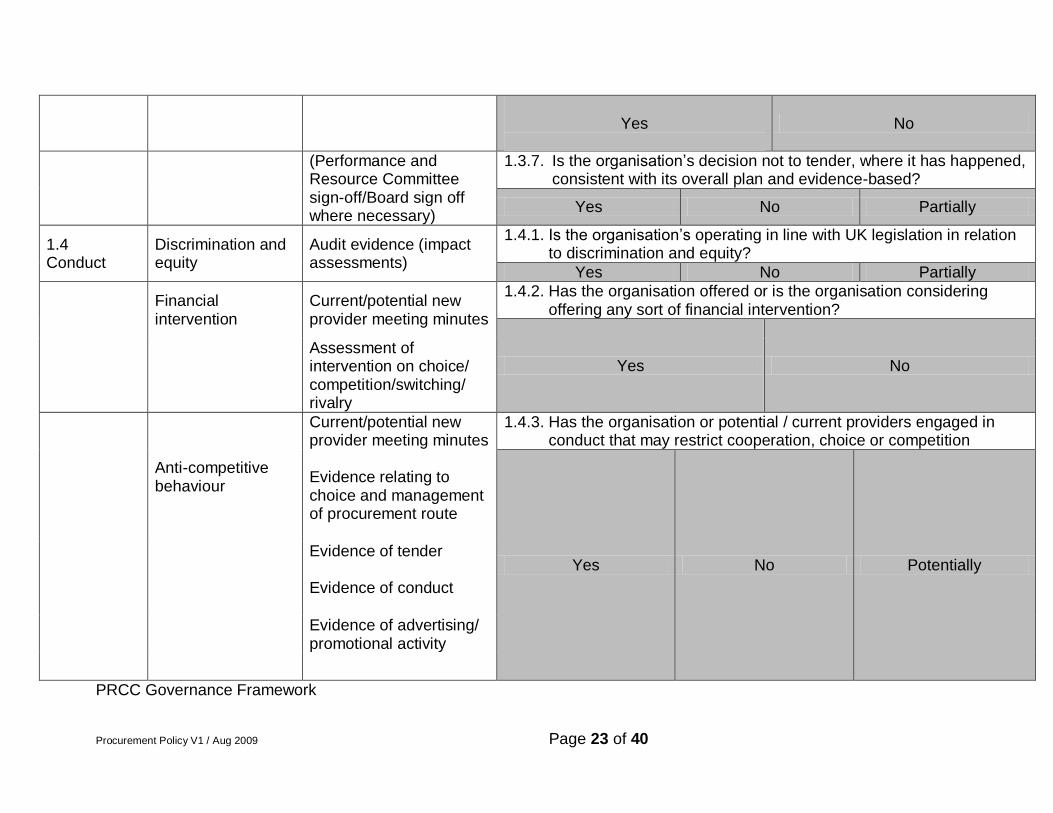
(Performance and Resource Committee sign-off/Board sign off where necessary)
1.3.7. Is the organisation‟s decision not to tender, where it has happened, consistent with its overall plan and evidence-based?
Yes No Partially
1.4 Conduct
Discrimination and equity
Audit evidence (impact assessments)
1.4.1. Is the organisation‟s operating in line with UK legislation in relation to discrimination and equity?
Yes No Partially
Financial intervention
Current/potential new provider meeting minutes
1.4.2. Has the organisation offered or is the organisation considering offering any sort of financial intervention?
Yes No
Assessment of intervention on choice/ competition/switching/ rivalry
Anti-competitive behaviour
Current/potential new provider meeting minutes Evidence relating to choice and management of procurement route
1.4.3. Has the organisation or potential / current providers engaged in conduct that may restrict cooperation, choice or competition
Yes No Potentially
Evidence of tender Evidence of conduct
Evidence of advertising/ promotional activity
PRCC Governance Framework
Procurement Policy V1 / Aug 2009 Page 24 of 40
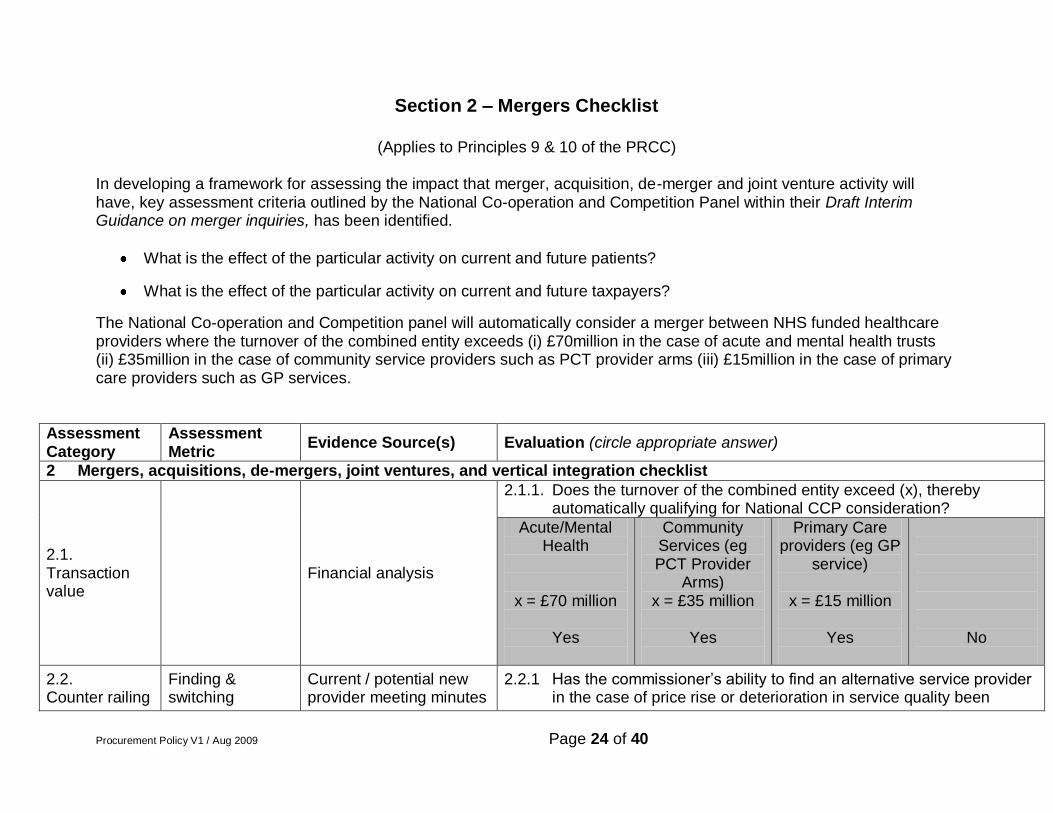
Section 2 – Mergers Checklist
(Applies to Principles 9 & 10 of the PRCC)
In developing a framework for assessing the impact that merger, acquisition, de-merger and joint venture activity will have, key assessment criteria outlined by the National Co-operation and Competition Panel within their Draft Interim Guidance on merger inquiries, has been identified.
What is the effect of the particular activity on current and future patients?
What is the effect of the particular activity on current and future taxpayers?
The National Co-operation and Competition panel will automatically consider a merger between NHS funded healthcare providers where the turnover of the combined entity exceeds (i) £70million in the case of acute and mental health trusts (ii) £35million in the case of community service providers such as PCT provider arms (iii) £15million in the case of primary care providers such as GP services.
Assessment Category
Assessment Metric
Evidence Source(s) Evaluation (circle appropriate answer)
2 Mergers, acquisitions, de-mergers, joint ventures, and vertical integration checklist
2.1. Transaction value
Financial analysis
2.1.1. Does the turnover of the combined entity exceed (x), thereby automatically qualifying for National CCP consideration?
Acute/Mental Health
x = £70 million
Yes
Community Services (eg PCT Provider
Arms) x = £35 million
Yes
Primary Care providers (eg GP
service)
x = £15 million
Yes
No
2.2. Counter railing
Finding & switching
Current / potential new provider meeting minutes
2.2.1 Has the commissioner‟s ability to find an alternative service provider in the case of price rise or deterioration in service quality been
Procurement Policy V1 / Aug 2009 Page 25 of 40
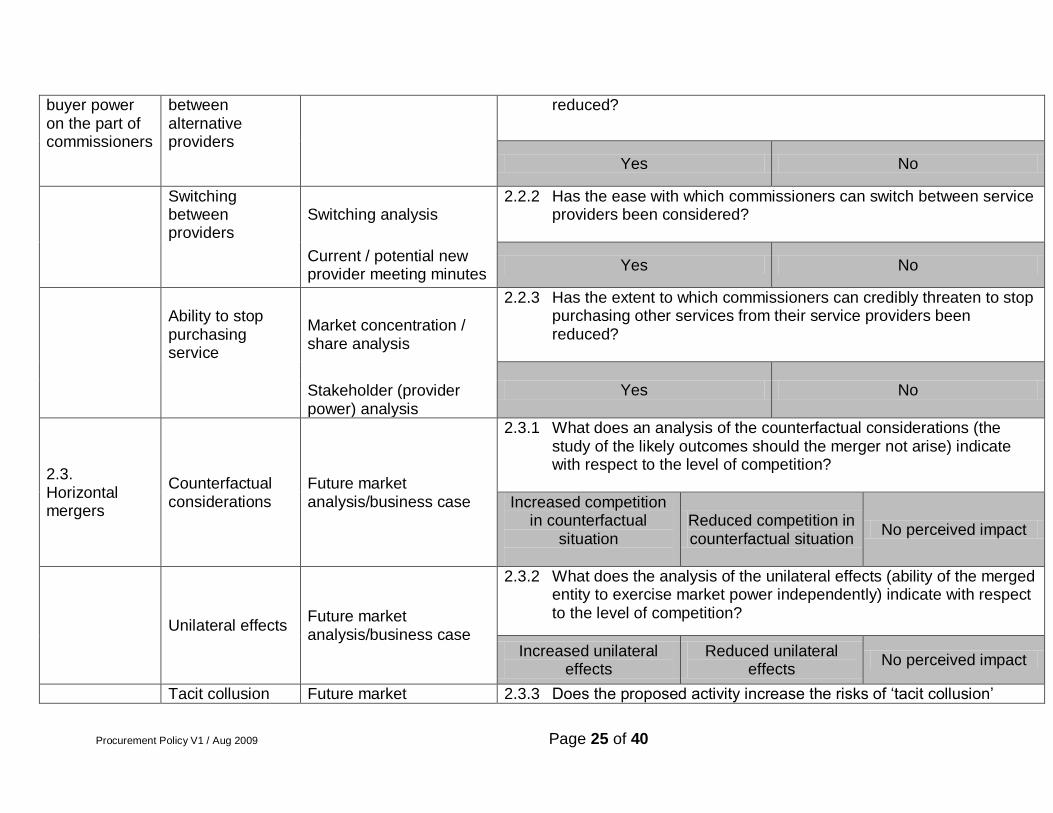
buyer power on the part of commissioners
between alternative providers
reduced?
Yes No
Switching between providers
Switching analysis 2.2.2 Has the ease with which commissioners can switch between service
providers been considered?
Current / potential new provider meeting minutes
Yes No
Ability to stop purchasing service
Market concentration / share analysis
2.2.3 Has the extent to which commissioners can credibly threaten to stop purchasing other services from their service providers been reduced?
Yes No
Stakeholder (provider power) analysis
2.3. Horizontal mergers
Counterfactual considerations
Future market analysis/business case
2.3.1 What does an analysis of the counterfactual considerations (the study of the likely outcomes should the merger not arise) indicate with respect to the level of competition?
Increased competition in counterfactual
situation
Reduced competition in counterfactual situation
No perceived impact
Unilateral effects Future market analysis/business case
2.3.2 What does the analysis of the unilateral effects (ability of the merged entity to exercise market power independently) indicate with respect to the level of competition?
Increased unilateral effects
Reduced unilateral effects
No perceived impact
Tacit collusion Future market 2.3.3 Does the proposed activity increase the risks of „tacit collusion‟
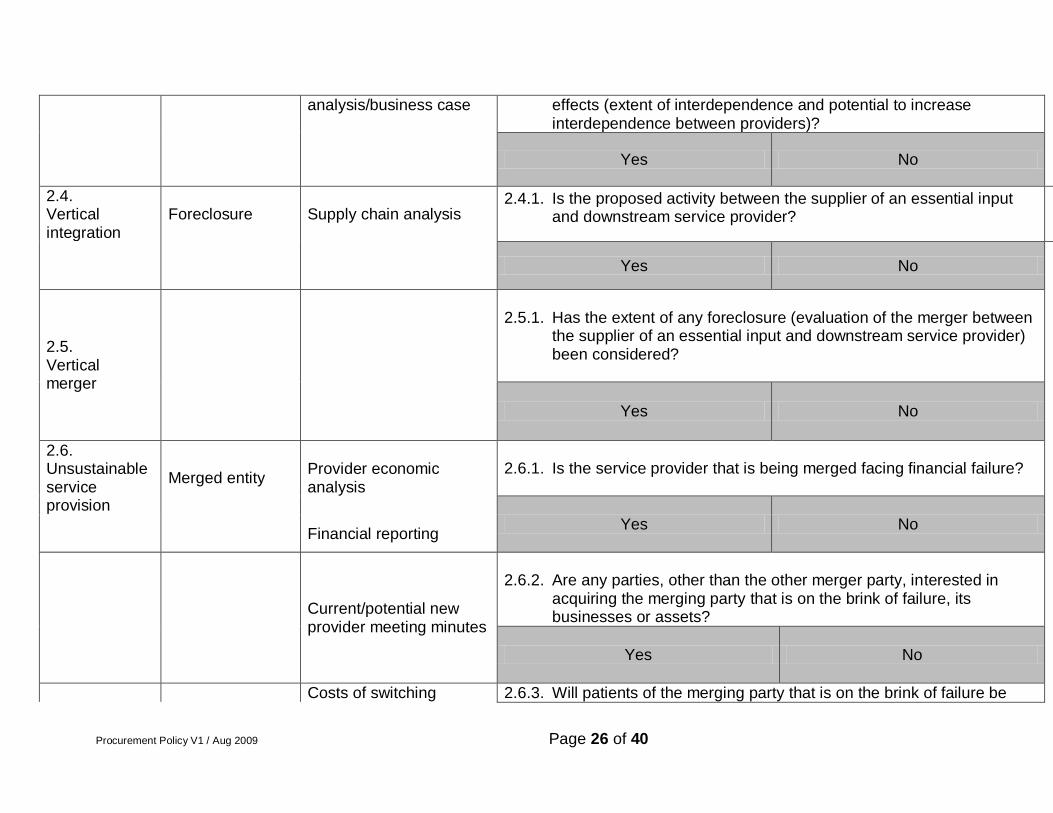
Procurement Policy V1 / Aug 2009 Page 26 of 40
analysis/business case effects (extent of interdependence and potential to increase interdependence between providers)?
Yes No
2.4. Vertical integration
Foreclosure Supply chain analysis 2.4.1. Is the proposed activity between the supplier of an essential input
and downstream service provider?
Yes No
2.5. Vertical merger
2.5.1. Has the extent of any foreclosure (evaluation of the merger between
the supplier of an essential input and downstream service provider) been considered?
Yes No
2.6. Unsustainable service provision
Merged entity Provider economic analysis
2.6.1. Is the service provider that is being merged facing financial failure?
Yes No Financial reporting
Current/potential new provider meeting minutes
2.6.2. Are any parties, other than the other merger party, interested in
acquiring the merging party that is on the brink of failure, its businesses or assets?
Yes No
Costs of switching 2.6.3. Will patients of the merging party that is on the brink of failure be
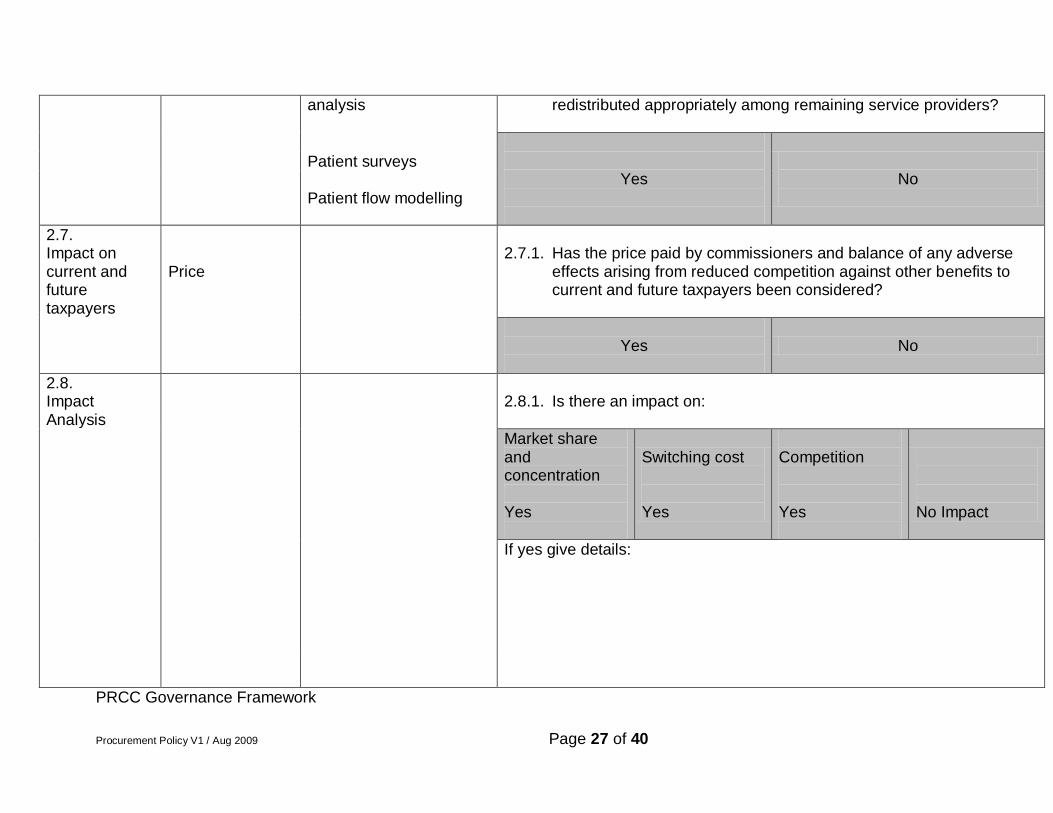
Procurement Policy V1 / Aug 2009 Page 27 of 40
analysis redistributed appropriately among remaining service providers?
Yes
No
Patient surveys
Patient flow modelling
2.7. Impact on current and future taxpayers
Price 2.7.1. Has the price paid by commissioners and balance of any adverse
effects arising from reduced competition against other benefits to current and future taxpayers been considered?
Yes
No
2.8. Impact Analysis
2.8.1. Is there an impact on:
Market share and concentration Yes
Switching cost Yes
Competition Yes
No Impact
If yes give details:
PRCC Governance Framework
Procurement Policy V1 / Aug 2009 Page 28 of 40
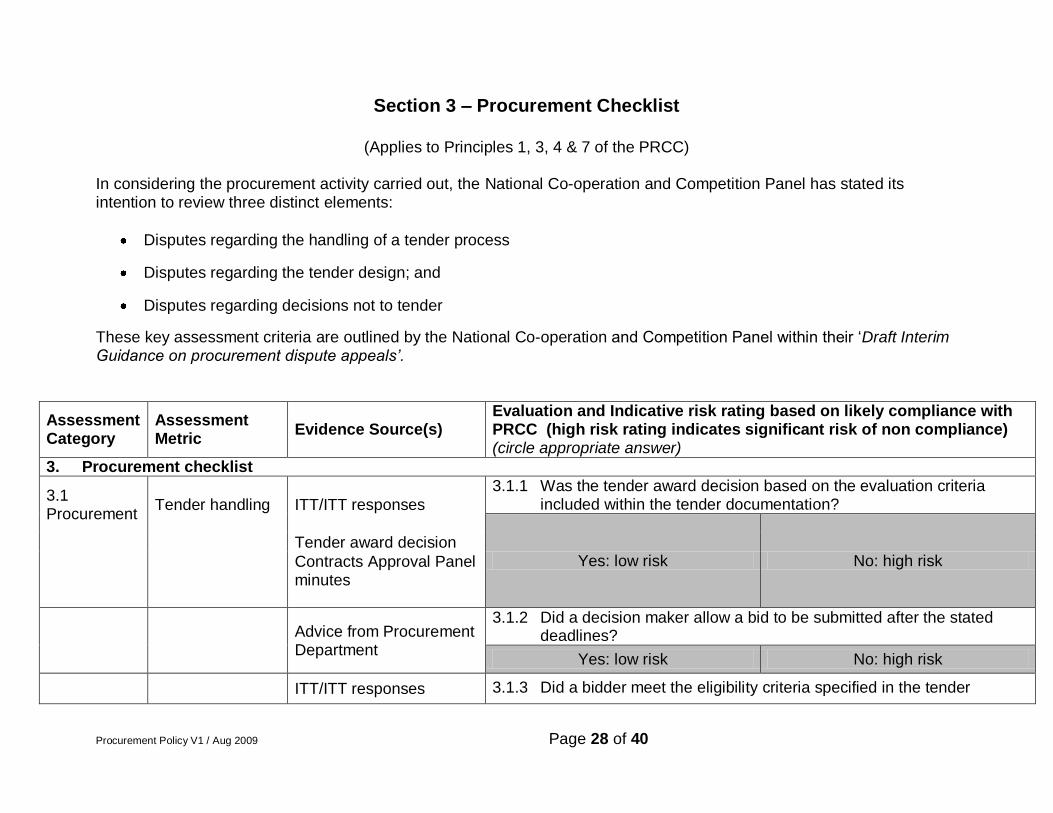
Section 3 – Procurement Checklist
(Applies to Principles 1, 3, 4 & 7 of the PRCC)
In considering the procurement activity carried out, the National Co-operation and Competition Panel has stated its intention to review three distinct elements:
Disputes regarding the handling of a tender process
Disputes regarding the tender design; and
Disputes regarding decisions not to tender
These key assessment criteria are outlined by the National Co-operation and Competition Panel within their „Draft Interim Guidance on procurement dispute appeals’.
Assessment Category
Assessment Metric
Evidence Source(s) Evaluation and Indicative risk rating based on likely compliance with PRCC (high risk rating indicates significant risk of non compliance) (circle appropriate answer)
3. Procurement checklist
3.1 Procurement
Tender handling ITT/ITT responses
3.1.1 Was the tender award decision based on the evaluation criteria included within the tender documentation?
Yes: low risk No: high risk
Tender award decision
Contracts Approval Panel minutes
Advice from Procurement Department
3.1.2 Did a decision maker allow a bid to be submitted after the stated deadlines?
Yes: low risk No: high risk
ITT/ITT responses 3.1.3 Did a bidder meet the eligibility criteria specified in the tender
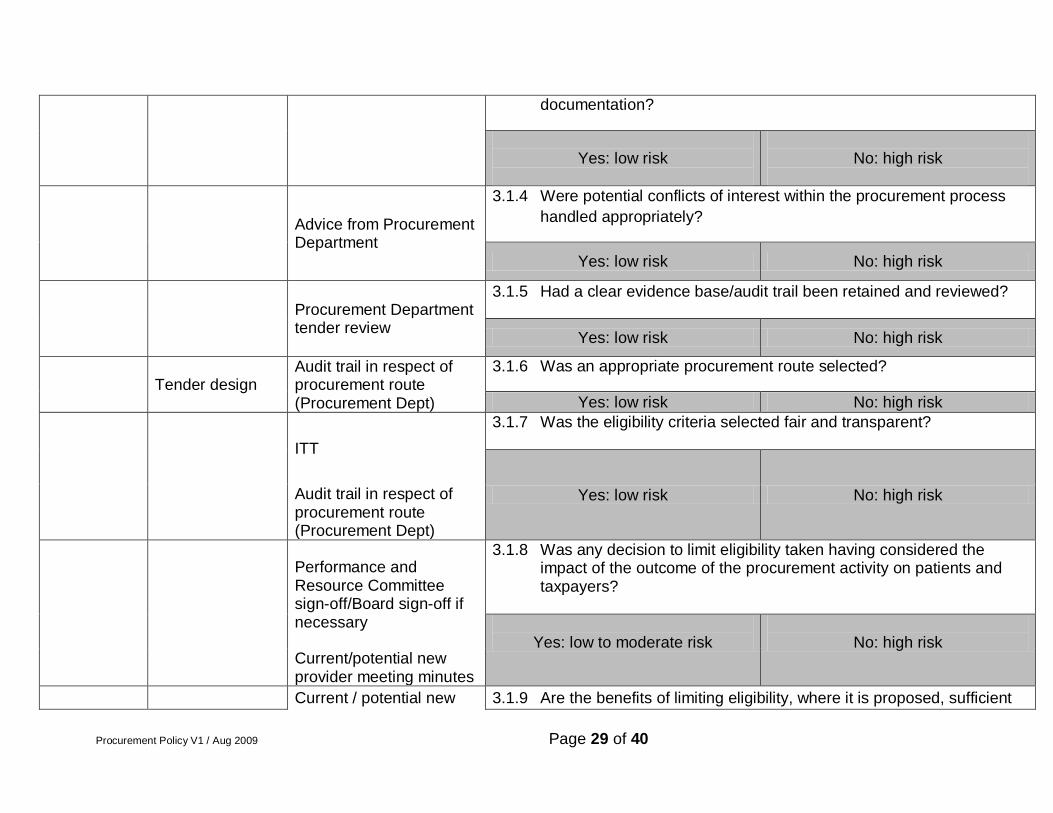
Procurement Policy V1 / Aug 2009 Page 29 of 40
documentation?
Yes: low risk
No: high risk
Advice from Procurement Department
3.1.4 Were potential conflicts of interest within the procurement process
handled appropriately?
Yes: low risk No: high risk
Procurement Department tender review
3.1.5 Had a clear evidence base/audit trail been retained and reviewed?
Yes: low risk No: high risk
Tender design Audit trail in respect of procurement route (Procurement Dept)
3.1.6 Was an appropriate procurement route selected?
Yes: low risk No: high risk
ITT
3.1.7 Was the eligibility criteria selected fair and transparent?
Yes: low risk No: high risk
Audit trail in respect of procurement route (Procurement Dept)
Performance and Resource Committee sign-off/Board sign-off if necessary
3.1.8 Was any decision to limit eligibility taken having considered the impact of the outcome of the procurement activity on patients and taxpayers?
Yes: low to moderate risk
No: high risk
Current/potential new provider meeting minutes
Current / potential new 3.1.9 Are the benefits of limiting eligibility, where it is proposed, sufficient
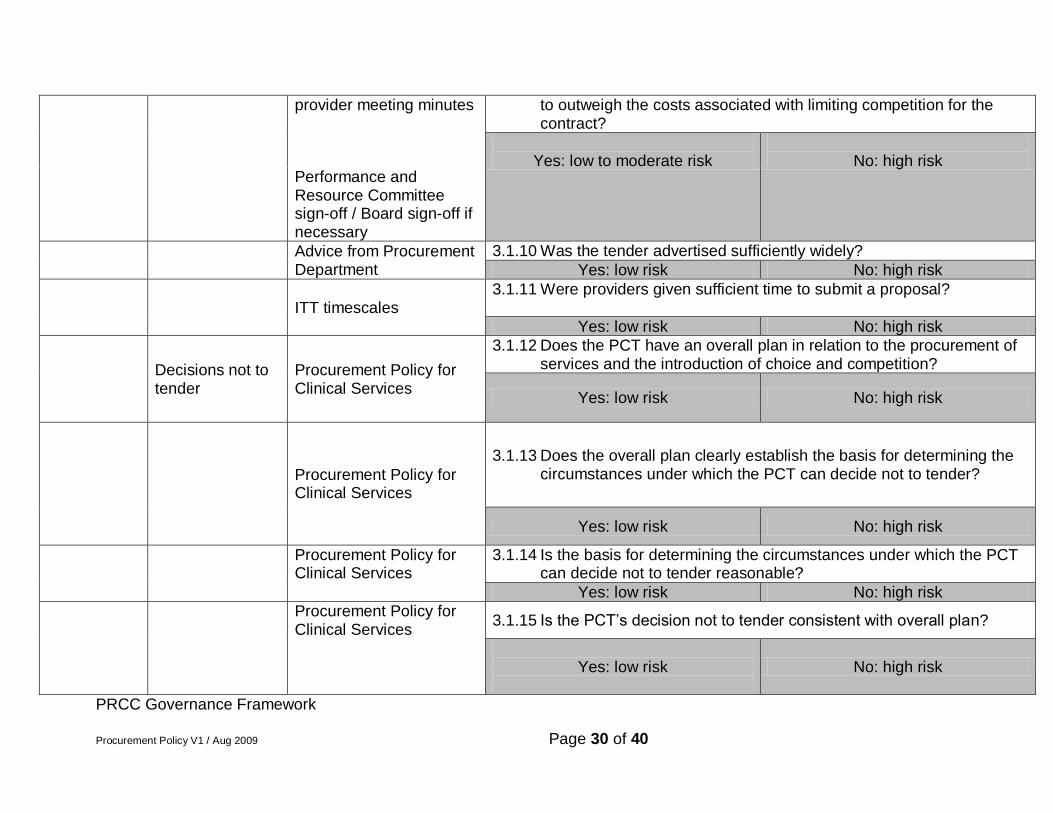
Procurement Policy V1 / Aug 2009 Page 30 of 40
provider meeting minutes to outweigh the costs associated with limiting competition for the contract?
Yes: low to moderate risk
No: high risk
Performance and Resource Committee sign-off / Board sign-off if necessary
Advice from Procurement Department
3.1.10 Was the tender advertised sufficiently widely?
Yes: low risk No: high risk
ITT timescales 3.1.11 Were providers given sufficient time to submit a proposal?
Yes: low risk No: high risk
Decisions not to tender
Procurement Policy for Clinical Services
3.1.12 Does the PCT have an overall plan in relation to the procurement of services and the introduction of choice and competition?
Yes: low risk No: high risk
Procurement Policy for Clinical Services
3.1.13 Does the overall plan clearly establish the basis for determining the circumstances under which the PCT can decide not to tender?
Yes: low risk No: high risk
Procurement Policy for Clinical Services
3.1.14 Is the basis for determining the circumstances under which the PCT can decide not to tender reasonable?
Yes: low risk No: high risk
Procurement Policy for Clinical Services
3.1.15 Is the PCT‟s decision not to tender consistent with overall plan?
Yes: low risk
No: high risk
PRCC Governance Framework
Procurement Policy V1 / Aug 2009 Page 31 of 40
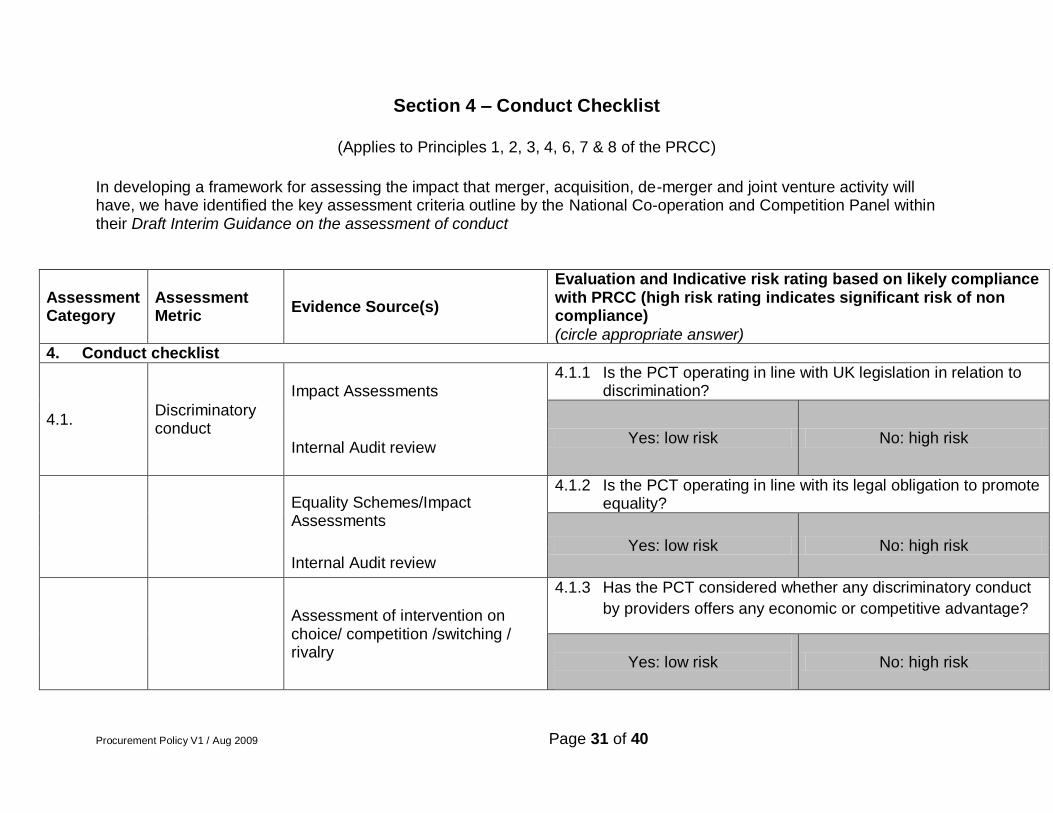
Section 4 – Conduct Checklist
(Applies to Principles 1, 2, 3, 4, 6, 7 & 8 of the PRCC)
In developing a framework for assessing the impact that merger, acquisition, de-merger and joint venture activity will have, we have identified the key assessment criteria outline by the National Co-operation and Competition Panel within their Draft Interim Guidance on the assessment of conduct
Assessment Category
Assessment Metric
Evidence Source(s)
Evaluation and Indicative risk rating based on likely compliance with PRCC (high risk rating indicates significant risk of non compliance)
(circle appropriate answer) 4. Conduct checklist
4.1. Discriminatory conduct
Impact Assessments 4.1.1 Is the PCT operating in line with UK legislation in relation to
discrimination?
Yes: low risk No: high risk Internal Audit review
Equality Schemes/Impact Assessments
4.1.2 Is the PCT operating in line with its legal obligation to promote equality?
Yes: low risk No: high risk Internal Audit review
Assessment of intervention on choice/ competition /switching / rivalry
4.1.3 Has the PCT considered whether any discriminatory conduct
by providers offers any economic or competitive advantage?
Yes: low risk
No: high risk
Procurement Policy V1 / Aug 2009 Page 32 of 40
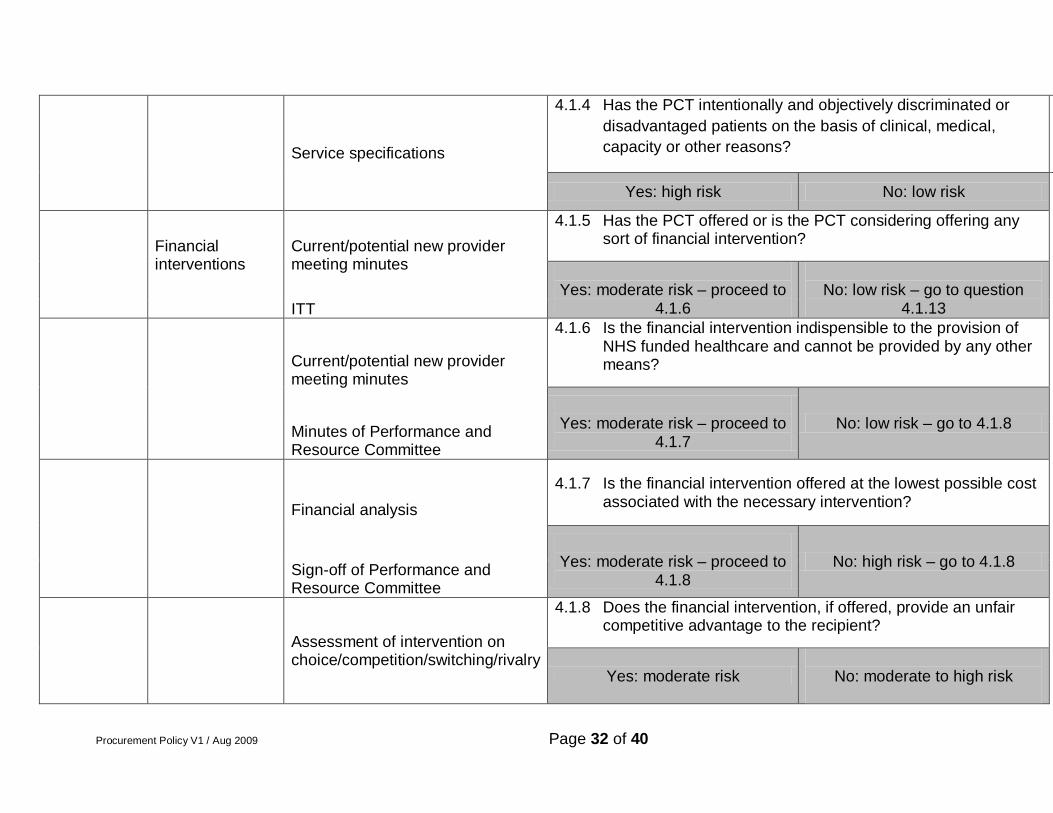
Service specifications
4.1.4 Has the PCT intentionally and objectively discriminated or
disadvantaged patients on the basis of clinical, medical,
capacity or other reasons?
Yes: high risk No: low risk
Financial interventions
Current/potential new provider meeting minutes
4.1.5 Has the PCT offered or is the PCT considering offering any sort of financial intervention?
Yes: moderate risk – proceed to
4.1.6
No: low risk – go to question
4.1.13 ITT
Current/potential new provider meeting minutes
4.1.6 Is the financial intervention indispensible to the provision of NHS funded healthcare and cannot be provided by any other means?
Yes: moderate risk – proceed to
4.1.7 No: low risk – go to 4.1.8
Minutes of Performance and Resource Committee
Financial analysis
4.1.7 Is the financial intervention offered at the lowest possible cost associated with the necessary intervention?
Yes: moderate risk – proceed to
4.1.8 No: high risk – go to 4.1.8
Sign-off of Performance and Resource Committee
Assessment of intervention on choice/competition/switching/rivalry
4.1.8 Does the financial intervention, if offered, provide an unfair competitive advantage to the recipient?
Yes: moderate risk
No: moderate to high risk
Procurement Policy V1 / Aug 2009 Page 33 of 40
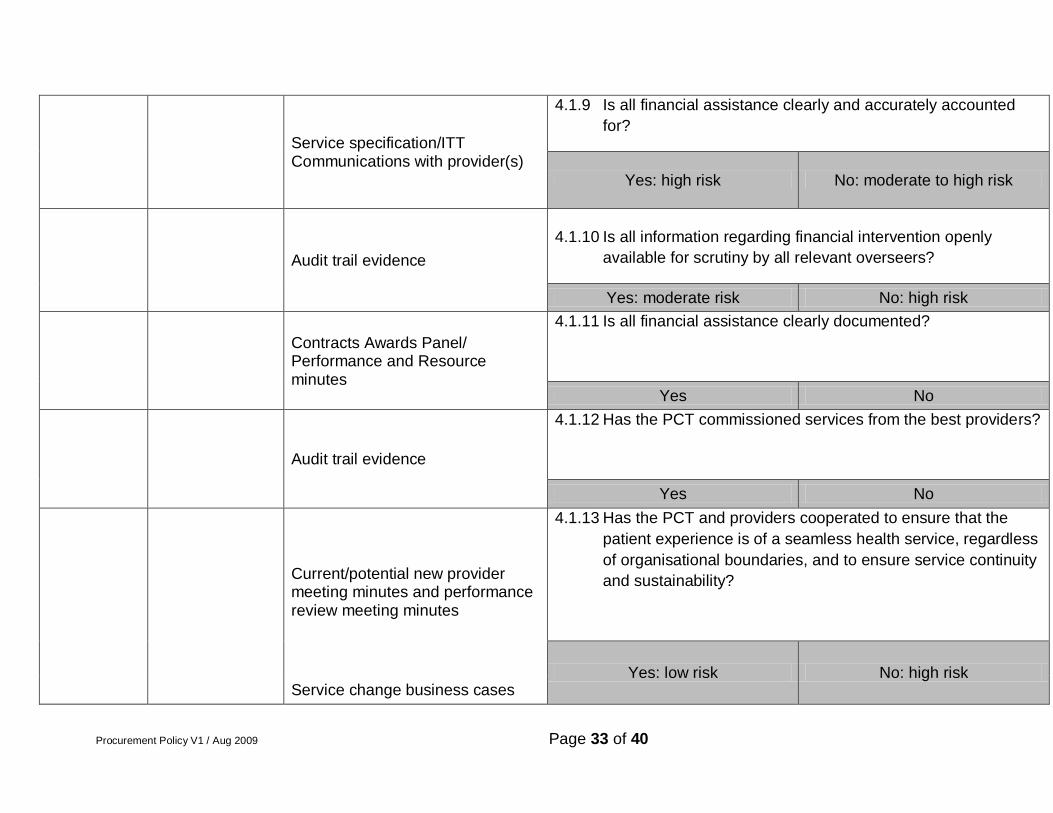
Service specification/ITT Communications with provider(s)
4.1.9 Is all financial assistance clearly and accurately accounted
for?
Yes: high risk No: moderate to high risk
Audit trail evidence
4.1.10 Is all information regarding financial intervention openly
available for scrutiny by all relevant overseers?
Yes: moderate risk No: high risk
Contracts Awards Panel/ Performance and Resource minutes
4.1.11 Is all financial assistance clearly documented?
Yes No
Audit trail evidence
4.1.12 Has the PCT commissioned services from the best providers?
Yes No
Current/potential new provider meeting minutes and performance review meeting minutes
4.1.13 Has the PCT and providers cooperated to ensure that the
patient experience is of a seamless health service, regardless
of organisational boundaries, and to ensure service continuity
and sustainability?
Yes: low risk No: high risk Service change business cases
Procurement Policy V1 / Aug 2009 Page 34 of 40
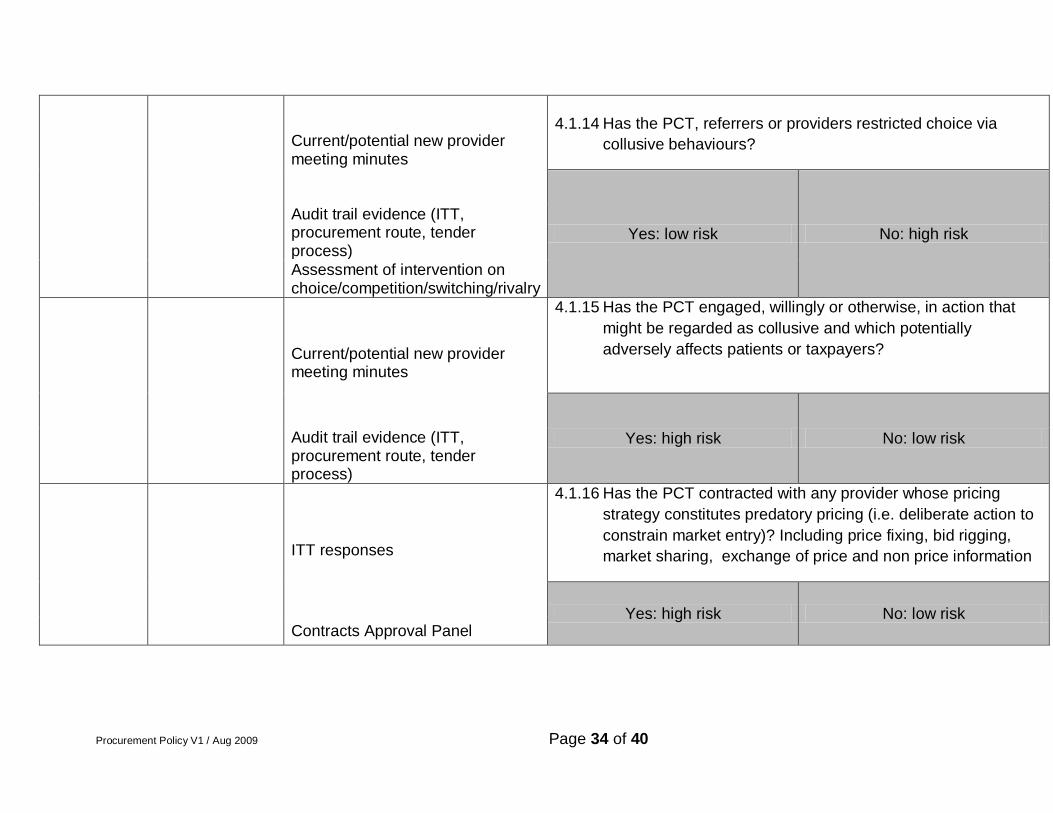
Current/potential new provider meeting minutes
4.1.14 Has the PCT, referrers or providers restricted choice via
collusive behaviours?
Yes: low risk No: high risk Audit trail evidence (ITT, procurement route, tender process)
Assessment of intervention on choice/competition/switching/rivalry
Current/potential new provider meeting minutes
4.1.15 Has the PCT engaged, willingly or otherwise, in action that
might be regarded as collusive and which potentially
adversely affects patients or taxpayers?
Yes: high risk No: low risk
Audit trail evidence (ITT, procurement route, tender process)
ITT responses
4.1.16 Has the PCT contracted with any provider whose pricing
strategy constitutes predatory pricing (i.e. deliberate action to
constrain market entry)? Including price fixing, bid rigging,
market sharing, exchange of price and non price information
Yes: high risk No: low risk Contracts Approval Panel
Procurement Policy V1 / Aug 2009 Page 35 of 40
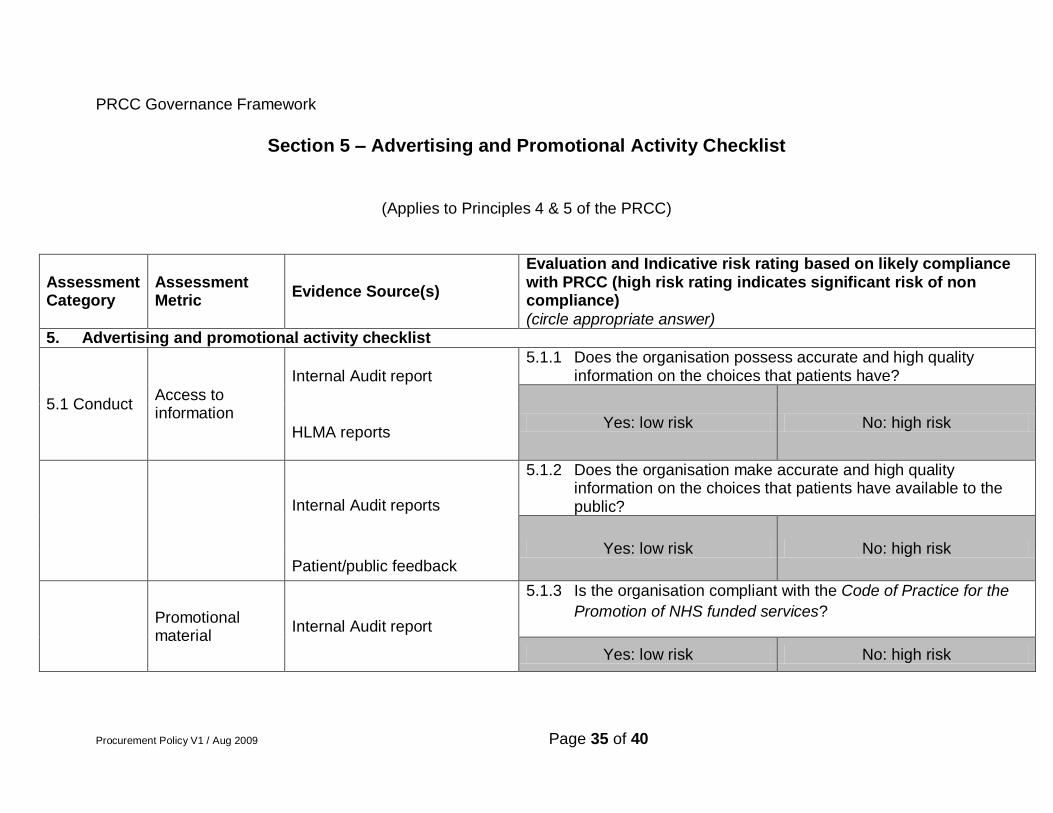
PRCC Governance Framework
Section 5 – Advertising and Promotional Activity Checklist
(Applies to Principles 4 & 5 of the PRCC)
Assessment Category
Assessment Metric
Evidence Source(s)
Evaluation and Indicative risk rating based on likely compliance with PRCC (high risk rating indicates significant risk of non compliance)
(circle appropriate answer) 5. Advertising and promotional activity checklist
5.1 Conduct Access to information
Internal Audit report
5.1.1 Does the organisation possess accurate and high quality information on the choices that patients have?
Yes: low risk No: high risk HLMA reports
Internal Audit reports
5.1.2 Does the organisation make accurate and high quality information on the choices that patients have available to the public?
Yes: low risk No: high risk Patient/public feedback
Promotional material
Internal Audit report
5.1.3 Is the organisation compliant with the Code of Practice for the
Promotion of NHS funded services?
Yes: low risk No: high risk
Procurement Policy V1 / Aug 2009 Page 36 of 40
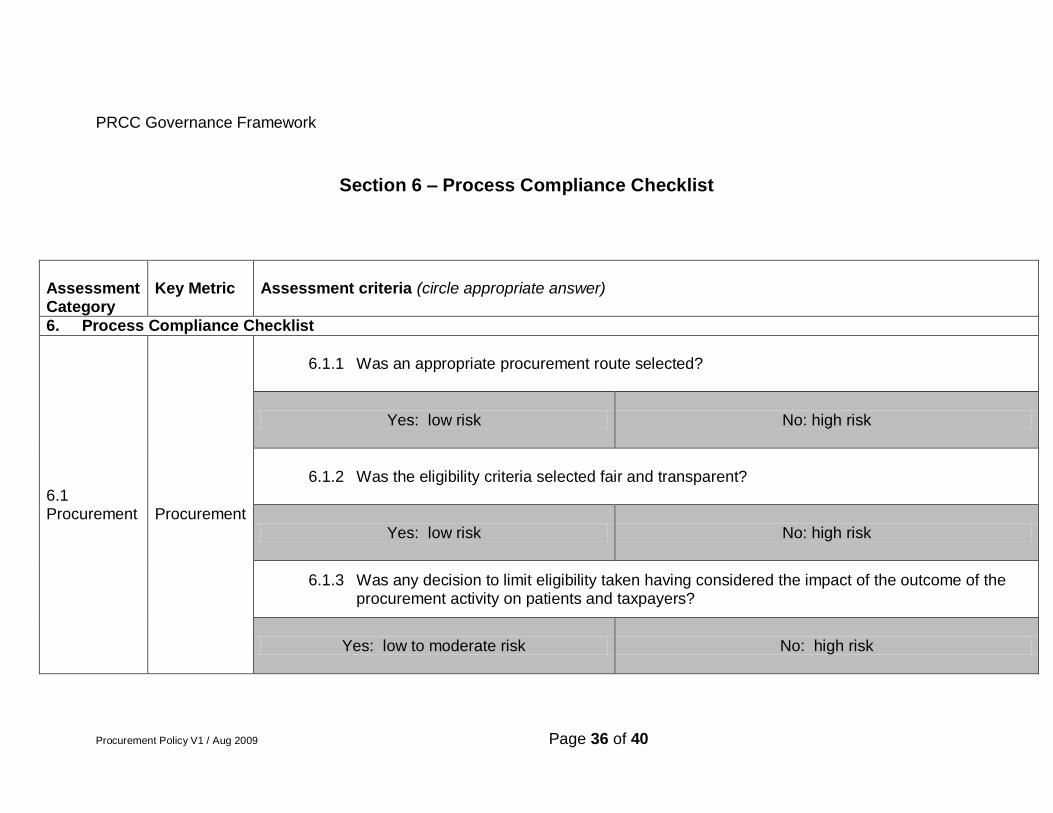
PRCC Governance Framework
Section 6 – Process Compliance Checklist
Assessment Category
Key Metric Assessment criteria (circle appropriate answer)
6. Process Compliance Checklist
6.1 Procurement
Procurement
6.1.1 Was an appropriate procurement route selected?
Yes: low risk No: high risk
6.1.2 Was the eligibility criteria selected fair and transparent?
Yes: low risk No: high risk
6.1.3 Was any decision to limit eligibility taken having considered the impact of the outcome of the procurement activity on patients and taxpayers?
Yes: low to moderate risk No: high risk
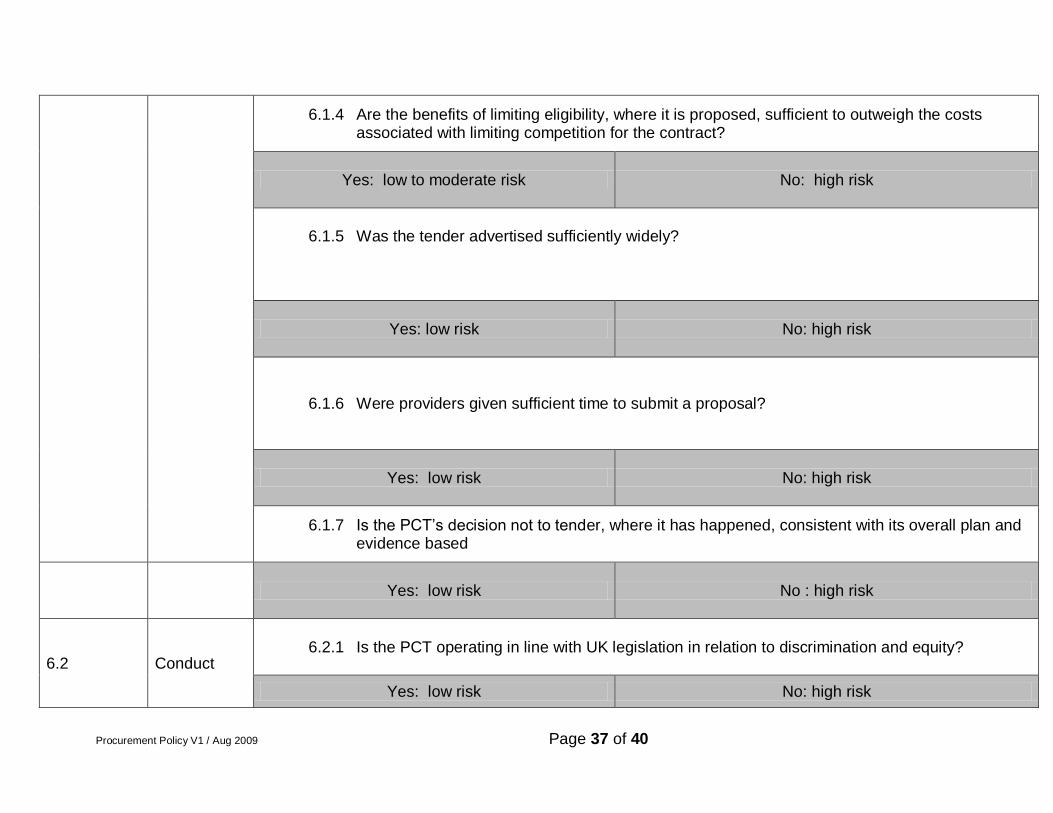
Procurement Policy V1 / Aug 2009 Page 37 of 40
6.1.4 Are the benefits of limiting eligibility, where it is proposed, sufficient to outweigh the costs associated with limiting competition for the contract?
Yes: low to moderate risk No: high risk
6.1.5 Was the tender advertised sufficiently widely?
Yes: low risk No: high risk
6.1.6 Were providers given sufficient time to submit a proposal?
Yes: low risk No: high risk
6.1.7 Is the PCT‟s decision not to tender, where it has happened, consistent with its overall plan and evidence based
Yes: low risk No : high risk
6.2 Conduct 6.2.1 Is the PCT operating in line with UK legislation in relation to discrimination and equity?
Yes: low risk No: high risk
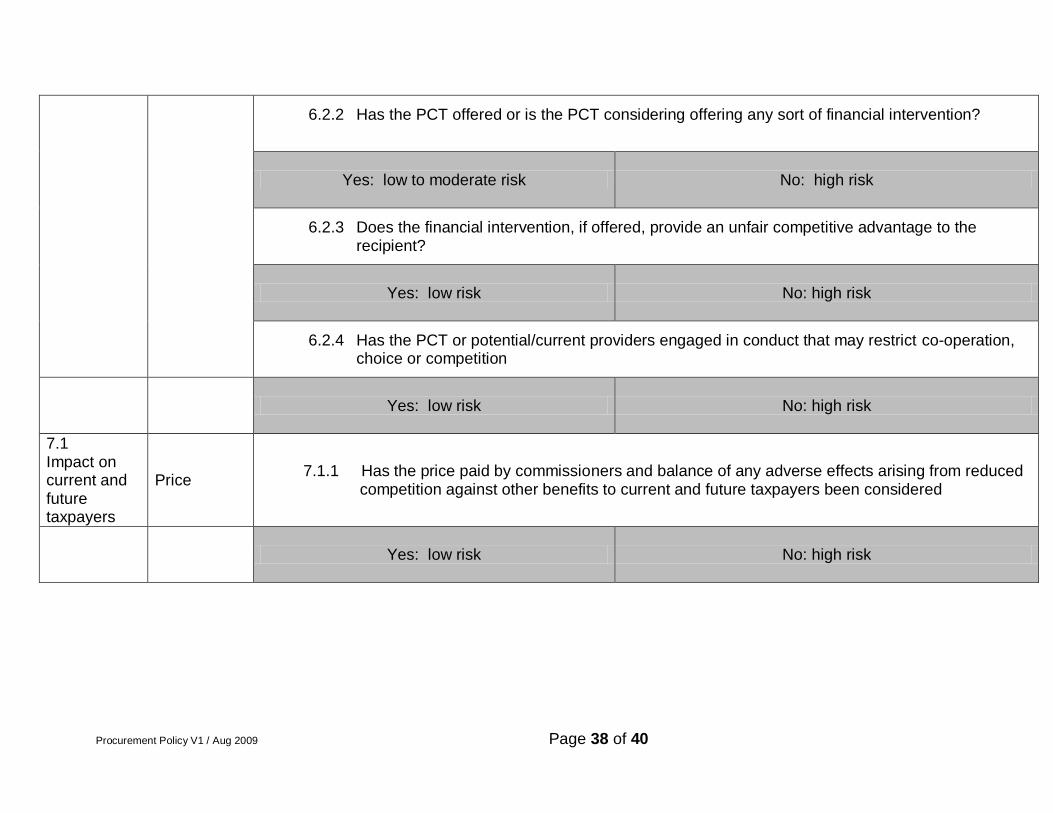
Procurement Policy V1 / Aug 2009 Page 38 of 40
6.2.2 Has the PCT offered or is the PCT considering offering any sort of financial intervention?
Yes: low to moderate risk No: high risk
6.2.3 Does the financial intervention, if offered, provide an unfair competitive advantage to the recipient?
Yes: low risk No: high risk
6.2.4 Has the PCT or potential/current providers engaged in conduct that may restrict co-operation, choice or competition
Yes: low risk No: high risk
7.1 Impact on current and future taxpayers
Price 7.1.1 Has the price paid by commissioners and balance of any adverse effects arising from reduced
competition against other benefits to current and future taxpayers been considered
Yes: low risk No: high risk
Procurement Policy V1 / Aug 2009 Page 39 of 40
Appendix C
Equality Impact Assessment Template
A. Function: Strategy and System Management
B.
Policy / Strategy / Piece of Work to be assessed:
This template has been completed in relation to the Procurement Policy for Clinical Services. This policy, which was approved originally in September 2008, has been amended to provide a much improved level of compliance with legislation and best practice guidance.
C.
Aims & Objectives of Policy/Strategy Piece of Work to be assessed
This Policy describes the framework by which NHS Northamptonshire will procure clinical services and ensure compliance with the legally binding EU Treaty procurement principles (the “EU principles”), the PCT Procurement Guide for Health Services (Department of Health, 2008) and the Principles and Rules for Co-operation and Competition (Department of Health 2008). Healthcare (i.e. clinical) services are classified as Part B services under the European Union (EU) Public Procurement Directives. This means that there are no formal legal requirements to tender them but there is a need to follow the principles therein, as far as practicable. This Policy ensures that a framework for complying with these regulations is clearly documented for staff to follow.
D. Groups who the piece of work should benefit, for example: - Patients
-Staff
-Other internal or external stakeholders
This policy is intended for all staff who are involved in the review of clinical services and the procurement process that may result following a review. It will ensure that legal and policy requirements surrounding the procurement of clinical services are followed and that as a result the organisational risk of potential challenges are mitigated. This policy and its requirements place an onus on staff to follow certain procedures during the process of service review. It is believed that these process do not present a negative or discriminatory impact on existing and potential service users or staff. It is therefore not proposed to undertake a full equality impact
Procurement Policy V1 / Aug 2009 Page 40 of 40
assessment in this instance.
Lead Officer: Chris Pallot Equality Impact Assessment Person / Team:
Date of Assessment: 09/09/09