
Principles of Geriatrics ประเสริฐ อัสสันตชัย...
42
Principles of Geriatrics ปปปปปปปป ปปปปปปปปปป ปปปปปปปปปปปปปปปปปปป ป.ปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปป
-
Upload
annabelle-fletcher -
Category
Documents
-
view
220 -
download
0
Transcript of Principles of Geriatrics ประเสริฐ อัสสันตชัย...

Principles of Geriatrics
ประเสร�ฐ อัสสนตชัยเวชัศาสตร�ผู้��ส�งอัาย�
ภ.เวชัศาสตร�ป�อังกันฯคณะแพทยศาสตร�ศ�ร�ราชั
พยาบาล

United Nations 1999
8 6 4 2 0 2 4 6 80
20
40
60
80
100+
Age
Males Females1999
Percentage of population8 6 4 2 0 2 4 6 8
Males Females2050
Percentage of population
0
20
40
60
80
100+
Age
The world population will be olderMore developed countries

Special Characteristics in Geriatrics
RAMPSReduced body reserveAtypical presentationMultiple pathologyPolypharmacySocial adversity
Geriatric Giants -atypical presentation
Instability (Fall)ImmobilityIntellectual impairment
IncontinenceInappetiteIatrogenesis

What is “Geriatric Medicine” ?
“….that branch of general medicine concerned with the
clinical (physical & mental) rehabilitative social preventiveaspects of illness and health in the elderly”
British Geriatrics Society

Examples of atypical presentation
diseases present as mechanism hyperthyroidism apathy not agitated ↓ ß-receptor
sense hypothyroidism depression, weak sedentary life infections no fever,leucocytosis ↓ interleukin I peritonitis no guarding weak rectus M. hypoglycemiano adrenergic ↓ ß-receptor sense congestive heart no dyspnea, sedentary life
failure confusion, ↓ function of liver & brain mild jaundice
RUQ pain

General changes in Aging
Physiologic changes Clinical correlation
osteoporosis, loss real height, bodyvertebral compression mass index ?↑fat to lean body mass ↑ distribution of fat- soluble
ratio drugs ↓ muscle mass poor indicator of serum
creatinine to glomerular filtration
↓ total body water ↓distribution of water-soluble drug
impaired shivering less febrile during infection

Dermatologic Changes in Aging
Physiologic changes Clinical correlation ↓stratum corneum ↓frequency of local
agentturnover rate
↓Pacinian corpuscle ↓high freq. vibration ↓Meissner corpuscle ↓low freq. vibration↓capillary, ↓urticaria, sign of
inflammatory cell cellulitis↓elasticity sodium depletion,
senile purpura↓sweat gland hyperthermia↓sebaceous gland xerotic dermatitis ↓ nail growth rate ↑duration of treatment
of onychomycosis

Cardiovascular Changes in Aging
Physiologic changes Clinical correlation
↓ maximal heart rate stroke volume dependent = 208 – (0.95xage) cardiac output
↓ heart rate response syncope when change of to postural stress, postureValsalva manouvre atrial fibrosis ↑ atrial fibrillation↓ pacemaker cell in SAnodeimpaired LV filling ↑ reliance on atrial systole ↔LV contract&relax↑ hemodynamic effect from
atrial fibrillation↓ maximal C.O. ↓ hemodynamic reserve

Comparison of heart rate between the old and the young
Sympathetic stimulation
Intrinsic heart rate
Age 20 Age 80Resting heart rate
Vagal tone
Actual
heart
rate

Cardiovascular Changes in Aging
Physiologic changes Clinical correlation↓inotropic, chronotrpic ↓response to β
response to βadrenergic sti. receptor drugsless distensible, ↑systolic BP
↓ compliance artery ↑peripheral vascular ↑ hypertension
resistanceimpaired autoregulation postural hypotensiondegeneration of conducting ↑ heart block,
tissue left axis deviationcalcification of aortic valve aortic stenosis/sclerosis

Framingham – Study Blood pressure and age
Kannel et al 1978
BP (mmHg)
70
80
90
120
130
140
150
160
36 41 46 51 56 61 66 71 76 81
WomenMen
WomenMen
Systolic BP
Diastolic BP
yearsAge
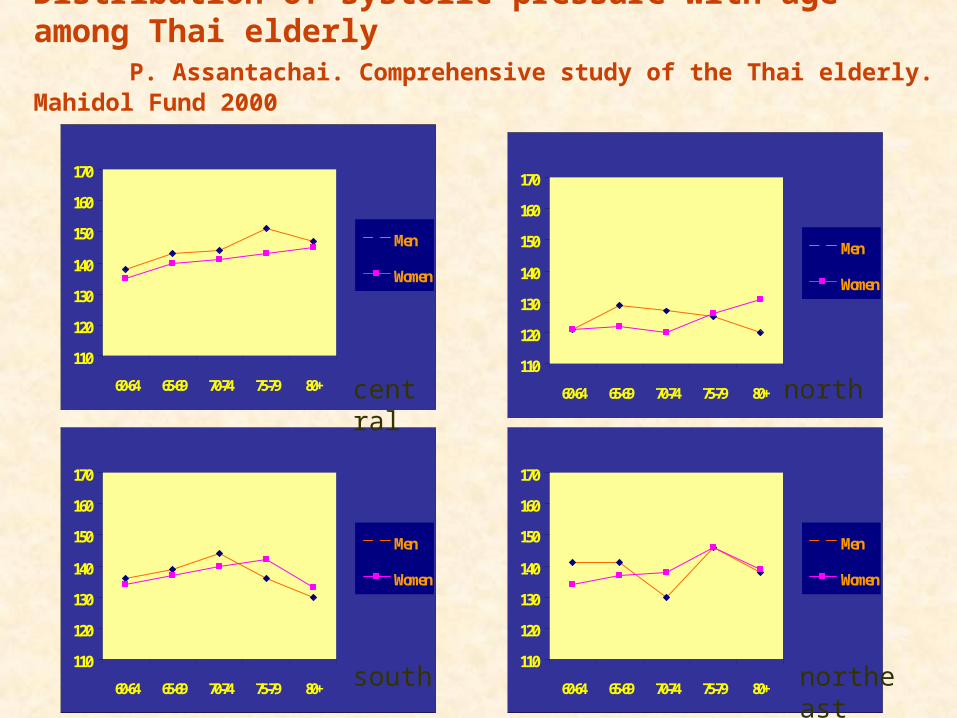
Distribution of systolic pressure with age among Thai elderlyP. Assantachai. Comprehensive study of the Thai elderly. Mahidol Fund 2000
110
120
130
140
150
160
170
60-64 65-69 70-74 75-79 80+
Men
Women
110
120
130
140
150
160
170
60-64 65-69 70-74 75-79 80+
Men
Women
110
120
130
140
150
160
170
60-64 65-69 70-74 75-79 80+
Men
Women
110
120
130
140
150
160
170
60-64 65-69 70-74 75-79 80+
Men
Women
central north
south northeast

Respiratory Changes in Aging
Physiologic changes Clinical correlation
kyphoscoliosis, costal ↓ chest wall compliance cartilage calcification ↑ work of breathing,
↑ diaphargm and abdominal muscle dependency
↓respiratory m.strength ↓ maximal inspiratory & expiratory pressure
↓ elastin in alveolar wall ↓alveolar elasticity recoil
↓ distal bronchiole diameter, ↑ closing volume
rearrangement in collagen
↑ residual volume ↓ vital capacity, tidal volume

Respiratory Changes in Aging
Physiologic changes Clinical correlation
thinning of alveolar wall, ↓ alveolar surface area
enlagement of terminal lung unitventilation-perfusion ↓PaO2 =(100-0.32x
age) mismatching↓ FEV1, FVC inadequate cough
less effective ciliary action↓ventilatory response to prolonged hypercapnia
hypercapnia

0
10
20
30
40
50
60
70
80
0-4 5-9 10-1920-3940-4950-5950-69 +70
%
age groups
Source: Betts FR, Douglas RG. Influenza virus. In: Mandsel GL, Douglas RG, Bennet JE, Eds. Principles and practice of infectious diseases, Churchill Livingstone Inc. 1990: 1306-1325
respiratory complications
Age Distribution of Respiratory Complications
years
Dr.Prasert Assantachai, M.D., Division of Preventive Medicine, Siriraj Hospital

Endocrine Changes in Aging
Physiologic changes Clinical correlationimpaired glucose tolerance ↑ DM
↑ BS 5.3 mg%/10yrs after 30 years old
↑ serum insulin metabolic syndrome
↓ DHEA ↓ libido
↓free testosterone
↓ T3 sick euthyroid syndrome
↑ PTH interpretation & ↓Ca
↓ vitamin D by skin ↓ Ca absorption
↑ serum homocysteine ↑ atherosclerosis

Changes in blood glucose levels with age
80.0090.00
100.00110.00120.00130.00140.00150.00160.00170.00180.00
age20 age30 age40 age50 age60 age70 age80 age90
Postprandial
Fasting
Elahi D, et al. Eur J Clin Nutr 2000; 54: S112-S120.

Dietary therapy: special considerations for older people with diabetes
financial difficultyshopping difficulty due to mobility problemspoor food preparation skills esp. widowed meningrained dietary habitsdifficulty following dietary instruction because of impaired cognitive function↓ taste↑ frequency of constipation

Hematologic Changes in Aging
Physiologic changes Clinical correlation
↓ bone marrow reserve ↓ response during stress
↓ reticulocytosis to ↑ anemia
erythropoitin
↓ erythropoietin ↑ anemia
production

Gastrointestinal Changes in Aging
Physiologic changes Clinical correlation
poor oral health ↑ gingivitis, dental cariesmaxillary bone loss poorly fitting denture,
malnutritionweakening of lower ↑ hiatus hernia
esophageal sphincter ↓ parietal cell, ↓ hydrochloric acid,
atrophic gastritis bacterial over growth, anemia
↓response to gastric ↑NSAID-induced PUmucosal injury

Gastrointestinal Changes in Aging
Physiologic changes Clinical correlation
↓liver size and blood flow ↓drug clearance esp. phase I metabolism
↓ cytochrome P450 prolonged half life of oxidation drug via liver
biotransformation ↓pancreatic mass dyspepsia↓effective colonic constipationcontractionweakening of muscular diverticulum, layer
diverticulosis↓gut-associated lymphoid infection, malignancytissue

Neurologic Changes in Aging
Physiologic changes Clinical correlation loss of neurone & subdural hematoma
after brain weight trivial head injury
impaired autoregulation ↓ brain blood flow ↓ dendritic connections impaired memory
retrieveshort term memory loss ↑interview time↓ dopamine activity ↑Parkinsonism↑ neurofibrillary tangle pathologic change of
& senile plaques Alzheimer disease↓ acetylcholine activity ↑amnesia

Neurologic Changes in Aging
Physiologic changes Clinical correlation↓ serotonin activity :↑depressionchange of sleep :unnecessary narcotic
pattern drug change of :↑sensitivity to
pharmacodynamics benzodiazepines slow central processing :↓ intelligence
& reaction time

Normal AD
AP NFT
AP = amyloid plaquesNFT = neurofibrillary tangles Courtesy of George Grossberg, St Louis University, USA
Neuropathological ChangesCharacteristic of Alzheimer disease

The Cholinergic Deficit in AD Underlies the Clinical Symptomatology Cholinergic deficit
progressive loss of cholinergic neurones
progressive decrease in available ACh
impairment in ADL, behaviour and cognition
Hippocampus
Cortex
N. basalis Meynert
Bartus et al., 1982; Cummings and Back, 1998, Perry et al., 1978

Peripheral Nervous System Changes in Aging
Physiologic changes Clinical correlation ↓ vibratory sense esp. interpretation of
feet neuropathy↓ thermal sensitivity ↑ injury esp.men ↓ size of large ↓propioceptive &
myelinated fiber vibratory sense ↓ two-point impaired use of
discrimination test fine instrument

Renal Changes in Aging
Physiologic changes Clinical correlation↓ 25%renal mass esp.cortex ↓ nephron, ↓excretion
↓ creatinine clearance of water soluble drugs ~ 10 ml/decade
↓ medullary tonicity poor concentrating & diluting ability
↑basal level of ADH 75% of SIADH >65 yr.
2-2.5 greater increase ↑tendency of ↓[Na]+
in ADH response to stress
↓ammonia production susceptibility to acidosis

Renal Changes in Aging
Physiologic changes Clinical correlation ↓ 1-alpha hydroxylase ↓ active vitamin D
↓ calcium absorption
↓ distensibility of hyporeninemic
juxtaglomerular apparatus hypoaldosteronism

Age-related changes in sodium-modulating factors
↓ functioning nephron number
↓ renin-angiotensin-aldosterone formation and effect
↓ insulin secretion
↑ atrial natriuretic peptide levels with relatively reduced effect
↑ plasma norepinephrine levels
↓ renal dopamine
↓ kallikrein-kinin activity

Genitourinary Changes in Aging
Physiologic changes Clinical correlation↓ elasticity of detrusor urgency incontinence muscle ↑ residual urine↓ prostatic secretion in urine↓ Tamm-Horsefall protein ↑ UTI ↔ refractory period for ↓ libido
erections for men ↓ intensity of orgasm for
men and women

Muscle Changes in Aging
Physiologic changes Clinical correlation↓ muscle fiber sarcopenia↓ muscle strength except intact diaphragmatic
diaphragm, activityleg weaker than arm tend to fall↑ fat infiltration ↑ fat to lean body
mass ratio↑ fatigability ↓ muscle endurance ↓ innervation (motor unit) poor fine movement↓ basal metabolic rate ↓nutritional 4%/decade after age50 requirement

Bone & Joint Changes in Aging
Physiologic changes Clinical correlation↓ rate of fracture healing longer duration of
follow up↓ bone mass :cortical bone ↑ osteoporosis
0.6%,trabecular 0.7%/yr. ↑ fractureproteoglycans disordered cartilage glycosaminoglycans matrix
↑ osteoarthritis

Bone Remodeling–Normal
Bone
OsteoblastOsteoclast
CaCa

Bone Remodeling–Osteoporotic
Bone
OsteoblastOsteoclast
CaCa

Normal Bone
Reproduced from J Bone Miner Res. 1986;1:15-21with permission of the American Society for Bone and Mineral Research
Osteoporotic Bone Loss

Immune System Changes in Aging
Physiologic changes Clinical correlation↓ cell-mediated immunity ↑ TB, leprosy
macrophage function↑autoantibodies ↑ temporal arteritis,
↑ bullous pemphigoidlower affinity Ab production ↑ nonresponders to
vaccine ↓ delayed-type poor prognosis in
hypersensitivity anergy case↓B cell production by serious infection in
bone marrow malnutrition

Changes of Vision in Aging
Physiologic changes Clinical correlation impaired dark adaptationfall at night denature of lens protein cataract, glaring
effect presbyopia bifocal lens↓dynamic acuity ↓seeing moving target↓contrast sensitivity ↓ color discrimination↓lacrimation dry eye↓aqueous humor reabsorption glaucoma

Changes of Audition in Aging
Physiologic changes Clinical correlation
↓ hair cells of organ of Corti presbycusis, high tone hearing loss
↓discriminating source of ↑ handicap
sound↓discriminating of verbal poor compliance to
sound from noise hearing aids↑ keratin wax content ear wax impaction
Changes of Other Sensory Functions in Aging
Physiologic changes Clinical correlation
↓ smell ~ 50% ↓ appetite↓thirst drive poor fluid intake
dehydration↓ gustatory sense spicy, salty food↑threshold vestibular poor body balance
responses

Approach to an elderly patientApproach to an elderly patientPhysical assessment
Mental assessment
Function assessment
Social assessment

Thank you for your excellent attention


















