
Primary glomerulonephritides (GN) Miroslav Merta Klinika nefrologie 1. LF a VFN.
41
Primary glomerulonephritides (GN) Miroslav Merta Klinika nefrologie 1. LF a VFN
-
Upload
kathlyn-oliver -
Category
Documents
-
view
218 -
download
2
Transcript of Primary glomerulonephritides (GN) Miroslav Merta Klinika nefrologie 1. LF a VFN.

Primary glomerulonephritides (GN)
Miroslav Merta
Klinika nefrologie 1. LF a VFN

Definition of GN, definition of primary GN
In GN (generally) we find:
• an immunological process
• an inflammatory character of glomerular affection
In primary GN we find:
• an isolated affection of kidneys
Some GN can manifest as well as primary or as secondary GN (MGN, MPGN…)

Mechanisms of glomerular lesions
GEC: glomerular endotelial and epitelial cells
= „membrane attack
complex“)
PMNs: polymorphonuclears

Pattern of GN - immunofluorescency
• Immune complexe – 85%
• Pauci – immune 14%
• Anti- GBM 1-2%

Inflammatory affection of glomeruli
is characterized by:
• Exsudation of neutrophils/macrophages
• Proliferation of mesangial/endothelial cells

Classification of primary GN
1. Non-proliferative GN- minimal change nephropathy-disease (MCN)
- focal segmental glomerular sclerosis (FSGS) - membranous GN (MGN)
2. Proliferative GN - Acute GN- IgA nefropathy (IGAN)
- membranoproliferative GN (MPGN)

Role of renal biopsy in glomerular disease
1. Diagnosis of GN
2. Assessment of activity of the disease – important for the decision to treat (intention to treat)
3. Assessment of chronicity – important for the prognosis of the disease

Treatment of primary GN1. Treatment and treatment tactics
with well defined indications, good clinical experience
• corticosteroids• cytotoxic agents (CPA, chlorambucil)• azathioprine• cyklosporine• symptomatic treatment:
– ACEI či AT2 receptors blockers,– Hypolipidemics (statins)
2. Drugs with limited clinical experience• mycophenolate• tacrolimus• rapamycine• intravenous immunoglobulins• monoclonal antibodies
– anti-TNF=infliximab, adalimumab– anti-CD20=rituximab
• solubile cytokine receptors (TNF rec.=etanercept)• plasmaexchange
Treatment of primary GN

Treatment of primary GN - conclusions
1. Patients with primary GN are threatened with:a. complications of NSb. progression of the disease to ESRF
2. Urinary findings important, however renal biopsy essential for dg., treatment and prognosis.
3. Primary GN are treatable diseases. Patients should be treated according to available clinical evidence.

Proliferative versus nonproliferative GN (glomerular capillary wall – ultrastructural changes)
Normal glomerulusMembranous GN
(MGN)
FSGS
Basement
membrane
Epitelial
cells=podocytes
Mesangial
cells
Endothelial
cells
Urinary
space
Capllary
lumenMinimal chenge nephropathy
(MCN)Nonproliferative GNNonproliferative GN
Fusion of
pedicels
Subepithelial
deposits
Sclerotisation of the loops
(here in perihilar region)

Glomerular permeability and proteinuria
Normal,,,, glomerulus
Basement
membrane
Epithelial cells =
podocytes
Mesangial
cells
Endothelial
cells
Urinary
space
Capillary
lumen Role of nephrin, podocin, actinin in the structure and
function of podocytes and interpedicellar space (=„slit
diaphragma“)
Fusion of pedicels (= lesion of
podocytes) is important for initiation
of proteinuria (=probably not only
consequence of pru)
Glomerulární permeabilita a proteinurie
Filtration barrier is formed by: endothel (pores), GBM and interpedicellar processes.
Permeability of proteins through glomerular wall is influenced by charge (repelling of negatively charged proteins as
albumine by the negative charge of GEC) a also by the selective permeability of capillary wall of the glomerulus in
dependence on the size of the particules sieved (modulated particularly by the„slit diaphragma“, and podocytes).
Interpedicellar space = slit diaphragma and the scheme showing possible anchoring of nephrin in this domain.
Slit diaphragma Nephrin
Nonproliferative GN- selectivity of proteinuria
Impairment of glomerular capillary wall leads to:
1. Selective proteinuria – nefrotic range – minimal change nephropathy (MCN)
2. Non-selective proteinuria (associated event. with microscopic hematuria) - FSGS
- idiopatic membranous GN

Relative frequency of primary GN in causes of nephrotic syndrome (NS)
Korbet et al., Am. J. Kidney Dis., 1996, 27: 647 - 651

Minimal changes of glomeruli (minimal change disease – MCD, minimal change nephropathy –
MCN)
Fůze pedicel
Normal glomerulus Minimal changes of glomeruli

Minimal changes of glomeruli- histological findings
Lignt microscopy (LM): normal glomerulus or weak
mesangial hypercellularity (<5%),
Electrone microscopy (EM): fusion of
pedicels, microvilous changes
Fusion of pedicels Mikrovilous changes
Immunofluorescence (IF): weak positivity of IgM, event. IgA,IgG, C3

Patogenetic factors involved in the process of development of minimal changes of glomeruli
1. Circulating soluble permeable factor (hemopexin?)
2. Decreased synthesis of glomerular polyanionts (heparan sulfate) by podocytes
3. Impairment of adhesion of podocytes on GBM ( -dystroglycan, 1-integrins?)
4. Impairment of expression of TGF1 (expression of TGF1 observed only in steroid-resistant MCD and FSGS)
Minimal changes of glomeruli – basic characteristics
1. Full blown nephrotic syndrome with selective proteinuria
2. Rarely presence of hematuria, hypertension a decrease of kidney function
3. Absence of glomerular abnormits in the histological (LM, IF) picture.
4. Typical picture of damage of epithelial cells (fusion of pedicels) in EM

Minimal changes of glomeruli- prevalence in patients with NS
(dependence on age)
Children - 85 – 95%
Adults < 40 y - 50%
Adults > 40 y - 20 – 25%

Classification of patients with MCN in dependance on the answer to the treatment with
corticosteroids (KS) – cortico-sensitivity
1. Cortico-sensitive patientsdo develop full remission of proteinuria during 8
– 12 weeks of treatment (in adults within 16 weeks)
2. Cortico (steroid) dependant patientsdo develop relapse during the period of tapering
the dosis of CS or shortly (2 weeks) after termination of CS treatment
3. Cortico (steroid) resistant do not respond to the treatment with CS

Therapy of MCD in adults
1. Initial treatment with prednisone 1mg/kg for a period of 8-16 weeks or at least 1 week after achievement of remission, thereafter several weeks (4) a treatment with dosis of 1 mg/kg in alterning interval, thereafter slow withdravel of CS („tapering“) during a period of several months.
2. Relapses should be treated in the same regime3. In patients suffering from frequent relapses or
corticosteroid-dependent patients to give the treatment:Cyclophosphamide 2 mg/kg/day for a period of 8 weeksor CyA 5 mg/kg/day for a period of 6-12 months
Treatment of CS-resistant patients is not usually successful

FSGS – basic histological features (LM)
Light microscopy (LM): only focally (in some glomeruli – especially juxtamedullar ones) a
segmentally (only in some segments of glomeruli) presence and sclerotisation of glomerular loops,
caused by accumulation of acelular matrix with adhesions to Bowman´s.capsule (hyalinosis). Mild
mesangial hypercelularity may be present,Further development of FSGS is followed by global
sclerotisation of glomeruli and tubular atrophy and fibrosis interstitium..

FSGS – basic histological types
Perihilar FSGS: most commonTip lesion FSGS: more often
corticosensitive ?
Collapsing FSGS: rare variant, often
secondary (HIV)

Etiology of FSGS1. Primary FSGS
a. perihilar variantb. „tip“lesion
2. Secondary FSGSa. foci of healing b. hyperfiltration in residual nephrones
- agenesis of kieny- vesico-ureteral reflux- morbid obesity
c. injury of epithelial cells- HIV nephropathy („collapsing FSGS“)- heroin nephropathy

Patogenesis of primary FSGS
1. Late manifestation of inborn FSGSimpairment of morphrology/function podocytar proteins (podocin, -actinin, CD2AP, and other)
2. Circulating permeabile factor/sa. immunoglobulin, or Ig-like moleculeb. protein with MW of 30-50 kDa
c. faktor inhibating NO inducible synthasis in mesangial cells (hemopexin)
3. Deficit of inhibitors of permeabile factors by loss into urineapolipoproteins of HDL complexe
(e.g. apo J, apo E2 and apo E4)

Mutations of podocytar proteins in FSGS

Mutations of podocytar genes and their gene products/proteins
Disease Gene Locus
Inheritance Gene Protein
CNF
(MIM 256300)
19q13.1 AR NPHS1 Nephrin
SRN1
(MIM 600995)
1q25-q31 AR NPHS2 Podocin
FSGS1
(MIM 603278)
19q13 AD ACTN4 -actinin
FSGS2
(MIM 603965)
11q21-22 AD FSGS2 ?
FSGS3 (mouse)
(MIM 607832)
6q AD FSGS3 CD2 AP
CNF congenital NS of Finnish type SRN(S) steroid resistant NS

Odstranění cirkulujícího permeabilního faktoru (plasmaferézou, plasmaadsorbcí) u FSGS snižuje
vylučování bílkovin do moči
Dantal et al., NEJM, 1994 Mitwalli et al., NDT, 1998

Focal segmental glomerulosclerosis
- basic characteristics 1. Asymptomatic proteinuria or full blown
nephrotic syndrome2. Commonly presence of hematuria,
hypertension and decrease of renal functions
3. Slow decrease of renal functions - 10y renal survival in 50%
4. Typical histological finding is focal and segmental sclerosis of glomerular tuft
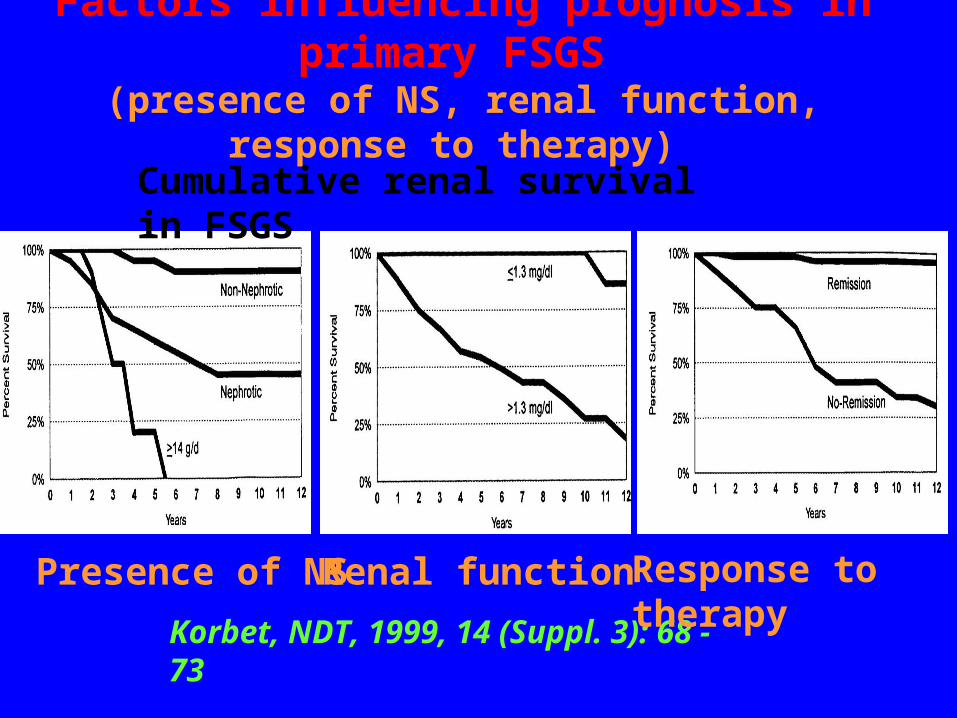
Factors influencing prognosis in primary FSGS (presence of NS, renal function, response to therapy)
Korbet, NDT, 1999, 14 (Suppl. 3): 68 - 73
Cumulative renal survival in FSGS
Presence of NS Renal function Response to therapy

Therapy of FSGS
1. Response to CS may increase from 10-30% to 60% by prolongation of therapy by higher doses (60 mg/m2) for a period minimum of 3 months, patients should be considered steroid – resistant after 6 mo.
2. Cyclosporine may cause a decrease of proteinuria and decrease the risk of progression to ESRD even in steroid-rezistant patients, the therapy should be prolonged (at least 6 mo), relapses after withdravel of CyA are frequent
3. Cytotoxic agents are drugs of 2nd line, evidence of their efficacy are not convincing

Membranous nephropathy (MGN)
Subepithelial immunocomplexe
deposits (arrows)
GBM surrounds subepithelial
deposits (picture of „spikes“)
Subepithelial deposits loose in EM
electrolucent appearance (they
are“wash-out“), thickened BM
„Intramembranous„ rather than
subetelial deposits
Notice: mesangial
(event.
subendothelial)
deposits are found in
secondary MGN
Event. We recognize stage V – reparation of epithel

Membranous GN– histological findings
Light microscopy (LM): thickened BM
Electrone microscopy (EM): demonstration of deposits, or event. „spikes“(BM)
GBM surrounds subepithelial
deposits (picture of „spikes“)
Subepithelial immunocomplexe
deposits (D)
Immunofluorescence (IF): diffuse granular positivity of
IgG, event. C3. (= sign of activity?).
GBM surrounds subepithelial
deposits (pictureof „spikes“)

Etiology of membranous GN
1. Idiopathic MGN
2. Secondary MGN (therapy different from therapy of
idiopthic MGN)
- infection (hepatitis B, syphilis, malaria)
- drugs (organic gold, penicillamine, NSAID)
- tumors (carcinomas, for ex. Ca of coli, lung Ca,
or gastric Ca, also lymphomas)
- systemic lupus erythematosus

Idiopathic membranous GN - basic characteristics
1. Membranous GN accounts for 15-25% cases of NS in adults
2. Proteinuria of nephrotic range is present approxiomately in 80% of patients, in the remaining subgroup the proteinuria is less pronounced
3. Microscopic hematuria is frequent4. Hypertension and ESRD are not initial symptoms,
but may develop during the further course of the disease.
5. Histology – subepithelial deposit leading to thickening of GBM

(Untreated) Idiopatic MGN - high frequency of spontaneous remissions
Mosconi et al., NEJM, 1993

Idiopatic membranous GN - natural course of the disease
1. Spontaneous remission develops approximately in 1/3 of patients
2. Nephrotic syndrome outlasts in other 1/3 of patients
3. Approximately 20-30% of patients do progress to ESRD during 20-30 y of follow-up

Idiopatic MGN – efficacy of immunosupressive (IS) therapy
Ponticelli et al., NEJM, 1992Torres et al., Kidney Int., 2002, 61: 219 - 227
Conservative versus IS therapyIS therapy: Prednisone vs Prednisone +
alkylating agents
Immunosupression
Conservative
treatment

Treatment of idiopatic MGN 1. Before starting IS therapy do consider its necessity, do
exploit the profit of conzervative treatment (ACEi, ABR)2. Cortikosteroids only partially efficient in monotherapy3. Cytotoxic agents (cyclophosphamide, leukerane) bring
about long-term remission of NS and ameliorate renal survival. With regard to serious side-effects these agents should be reserved to patients with serious involvement/resp. with progressing form of MGN
4. Cyklosporine seems to be satisfactory alternative to cytotoxic therapy. The impact on proteinuria is clear, however the effect on stabilisation of disease is questionable. There is concern about relapse after withdraval.

Guideline for the treatment of IMGN
Cattran, Kidney Int., 2001, 59: 1983 - 1994

Proliferative versus neproliferative GN (glomerular capillary loop – ultrastructural changes)
Normal glomerulus
Mesangioproliferative GN
Proliferative GNProliferative GN
Basal
membrane
Epitheliál
cells=podocytes
Mesangial
cells
Endotehelial
cells
Urinary
space
Capillary
lumen
neutrophils
Acute GN
Membranoproliferative GN
Increased number and
proliferation of mesangial
cells
Increaed number
and proliferation
of mesangial cells
to distal parts of
capillary loop
Subendothelial deposits
mesangial deposits of IgA
neutrophils
Subendothelial
deposits
Subepithelial deposits
Increased number and
proliferation of mesangial
cells


















