Primary failure of eruption of primary moiars: A review ...
6
Primary failure of eruption of primary moiars: A review and case report Mai Diab, DDS, MSc' Prinriary failure of eruption, or primary retention, is an abnormality of tooth eruption that is characterized by cessation of eruption in the pre-eruptive stage, resulting in a deeply embedded tooth in the alveolar bone. This condition should be differentiated from secondary failure of eruption, which implicates termination of the eruptive process following tooth emergence into the oral cavity, resulting in infraclusion associated with impaired growth of the supporting alveolar bone. Primary failure of eruption of primary molars may have several effects on the developing dentition, which include malformation, impaction, or ectopic eruption of the succeeding premolars. Another possible complication is inversion between the premolar and its embedded predecessor primary molar. Primary retention of the primary second molars may result in ectopic eruption of the permanent first molars. This paper reviews the characteristics, etiology, and seque- lae of primary failure of eruption of primary molars and describes a case of an unerupted mandibular right primary second molar in a healthy 5-year-old girl. The child had no previous facial trauma or infection and a noncontributory familial history. Treatment consisted of surgical extraction of the embedded molar fol- lowed by placement of an intra-alveolar space maintainer and regular follow-up examinations. (Quintessence Int 2001 ¡32:55-60) Key words: ankylosis, eruption, impaction, primary failure, primary teeth, uneruption CLINICAL RELEVANCE: Primary failure of eruption of primary molars should be carefully evaluated to decide on the appropriate treatment, which can include surgical extraction, space management, and a close follow-up. T ooth eruption is a multifactorial physiologic process involving 3 stages. First, a pre-eruptive stage starts with growth of the dental follicle and initi- ates movement of the tooth in an occlusal direction from its position of development in the alveolar bone until emergence into the oral cavity. This is followed by a second pre-functional eruptive stage that extends from emergence until the erupting tooth achieves occlusion with the antagonist teeth. At this point, the tooth reaches the third functional eruptive stage that continues throughout the tooth's life.^-^ Tooth erup- tion can be impaired by several systemic and local dis- 'Clinical Assistant Professor, Division of Pédiatrie Dentistry, Department of Dentistry, University of Alberta, Edmonton, Alberta, Canada. Reprint requests: Dr Mai Diab, 4021 Dentistry/Pharmacy Centre, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta T6G 2N8, Canada. E-mail: [email protected] turbances, which may result in termination of the eruptive process at any stage, either before or after emergence into the oral cavity.''"^ Primary failure of eruption or primary retention is characterized by cessation of the tooth's movement in the pre-eruptive stage, which results in a deeply embed- ded tooth that fails to achieve emergence and remains covered with a thick layer of alveolar bone.'-'^-** The crown of the unerupted tooth is free of caries, restora- tions, fracture, and attrition; the roots are fully formed and usually without signs of résorption.*'-' Several studies reported primary failure of erupfion of the permanent molars in the permanent denti- tion,'-5 '"-" but this eruption anomaly is presumed to be rare in the primary dentition. However, only one epidemiological investigation by Bianchi and Roccuzzo' has been conducted to date. This study indicated a prevalence of 1:10,000 upon reviewing 30,000 panoramic radiographs. Additionally, several authors reported cases of primary failure of eruption of one,«'''''-2* or numerous primary molars,''•^^ Other authors reported cases of severely infra-occluded pri- mary molars, in which primary retention was suggested as a differential diagnosis.^"' The reported age of patients ranges between 4 and 21 years with more females affected than Quintessence Internationa 55
Transcript of Primary failure of eruption of primary moiars: A review ...

Primary failure of eruption of primary moiars:A review and case reportMai Diab, DDS, MSc'
Prinriary failure of eruption, or primary retention, is an abnormality of tooth eruption that is characterized bycessation of eruption in the pre-eruptive stage, resulting in a deeply embedded tooth in the alveolar bone.This condition should be differentiated from secondary failure of eruption, which implicates termination ofthe eruptive process following tooth emergence into the oral cavity, resulting in infraclusion associated withimpaired growth of the supporting alveolar bone. Primary failure of eruption of primary molars may haveseveral effects on the developing dentition, which include malformation, impaction, or ectopic eruption ofthe succeeding premolars. Another possible complication is inversion between the premolar and itsembedded predecessor primary molar. Primary retention of the primary second molars may result inectopic eruption of the permanent first molars. This paper reviews the characteristics, etiology, and seque-lae of primary failure of eruption of primary molars and describes a case of an unerupted mandibular rightprimary second molar in a healthy 5-year-old girl. The child had no previous facial trauma or infection anda noncontributory familial history. Treatment consisted of surgical extraction of the embedded molar fol-lowed by placement of an intra-alveolar space maintainer and regular follow-up examinations.(Quintessence Int 2001 ¡32:55-60)
Key words: ankylosis, eruption, impaction, primary failure, primary teeth, uneruption
CLINICAL RELEVANCE: Primary failure of eruption ofprimary molars should be carefully evaluated to decideon the appropriate treatment, which can include surgicalextraction, space management, and a close follow-up.
Tooth eruption is a multifactorial physiologicprocess involving 3 stages. First, a pre-eruptive
stage starts with growth of the dental follicle and initi-ates movement of the tooth in an occlusal directionfrom its position of development in the alveolar boneuntil emergence into the oral cavity. This is followedby a second pre-functional eruptive stage that extendsfrom emergence until the erupting tooth achievesocclusion with the antagonist teeth. At this point, thetooth reaches the third functional eruptive stage thatcontinues throughout the tooth's life. - Tooth erup-tion can be impaired by several systemic and local dis-
'Clinical Assistant Professor, Division of Pédiatrie Dentistry, Department of
Dentistry, University of Alberta, Edmonton, Alberta, Canada.
Reprint requests: Dr Mai Diab, 4021 Dentistry/Pharmacy Centre, Faculty
of Medicine and Dentistry, University of Alberta, Edmonton, Alberta T6G
2N8, Canada. E-mail: [email protected]
turbances, which may result in termination of theeruptive process at any stage, either before or afteremergence into the oral cavity.''"^
Primary failure of eruption or primary retention ischaracterized by cessation of the tooth's movement inthe pre-eruptive stage, which results in a deeply embed-ded tooth that fails to achieve emergence and remainscovered with a thick layer of alveolar bone.'-' -** Thecrown of the unerupted tooth is free of caries, restora-tions, fracture, and attrition; the roots are fully formedand usually without signs of résorption.*'-'
Several studies reported primary failure of erupfionof the permanent molars in the permanent denti-tion,'-5 '"-" but this eruption anomaly is presumed tobe rare in the primary dentition. However, only oneepidemiological investigation by Bianchi andRoccuzzo' has been conducted to date. This studyindicated a prevalence of 1:10,000 upon reviewing30,000 panoramic radiographs. Additionally, severalauthors reported cases of primary failure of eruptionof one,«'''''-2* or numerous primary molars,''• ^ Otherauthors reported cases of severely infra-occluded pri-mary molars, in which primary retention was suggestedas a differential diagnosis.^"'
The reported age of patients ranges between 4 and21 years with more females affected than
Quintessence Internationa 55

Diab
The mandibular primary second molars are the mostcommonly affected teeth.^-^ The unerupted primarymolars can be deeply embedded in the alveolar boneand the depth of their impaction increases graduallyas the alveolar bone grows vertically with age.- Forexample, the unerupted tooth can be located near theinferior border of the mandible."''-"'^ The majority ofreports noted that the embedded primary molarsremained asymptomatic until their detection with aroutine radiographie examination.'''*"5'''''2''-2
Primary failure of eruption of primary molars shouldbe distinguished from a more common eruption anom-aly, which is secondary failure of eruption (secondaryretention, infi'aclusion, submergence, submersion, sec-ondary infraposition, hypotrusion, re-impaction, or re-inclusion). These symptoms portray a tooth that previ-ously erupted and possibly achieved occlusion. Later,this tooth failed to continue its functional eruptionconcomitant with the adjacent teeth and progressivelyacquired an inferior position in relation to the occlusalplane. This is associated with cessation of the verticalgrowth of the supporting alveolar bone, which givesthe illusion of a submerged tooth.'•'•'''• • •-5-' Secondaryretention has been related to tooth anlcylosis that canresult from metabolic and/or structural disturbances tothe periodontal l
ETIOLOGY OF PRIMARY FAILURE OF ERUPTION
Several authors implicated hereditary factors in theetiology of failure of tooth eruption.'"- ' ^ For example,studies conducted on monozygotic twins provided evi-dence of the role of genetics in the etiology of sec-ondary retention or infraclusion."" Additionally,Boker et aP' concluded that secondary retention ofpermanent molars can be inherited and transmitted asan autosomal dominant trait. Similarly, the familialtendency to primary failure of eruption has been pro-posed because this condition affects members in thesame family.'•'"'^•^^ Moreover, Rasmussen andKotsaki-' suggested that primary failure of eruption ofprimary molars could be inherited as a dominant trait.
Primary failure of eruption has also been associatedwith hormonal disturbances or developmental syn-dromes such as cleidocranial dysplasia, -"*"' in whichabnormal eruptive mechanisms could delay or preventtooth eruption. Several theories were proposed toexplain the impaired eruptive process, includingabnormal résorption of the alveolar bone,'-'* aberrantdevelopment of the primary tooth germ, or displace-ment of the follicle from its original site leading todepletion or misdirection of the eruptive force.'''^-" Inaddition, failure of tooth eruption can result from aphysical barrier created by a supernumerary tooth,
localized infection, or an odontogenic cyst ortumor.'"'-'"'•'•• According to several authors, this condi-tion wouldn't be considered primary failure of erup-tion but rather an impaction resulting from mechanicalinterference in the path of eruption.'*^
On the other hand, it has been suggested that toothankylosis could contribute to failure of tooth eruption.However, the role played by ankylosis in the etiologyof primary failure of eruption remains controversial.Several researchers propose that metabolic or struc-tural alterations in the periodontal ligament can arisein early stages of root development and leadto abnormal root résorption, followed by excessivedeposition of cementum-like tissue and fusionbetween the cementum and/or dentin and the alveolarbone.5''-919.20,29,30 other researchers believe that pri-mary failure of eruption is not related to disturbancesin the periodontal ligament, but rather to an impairederuptive process.''*
SEQUELAE OF PRIMARY FAILURE OF ERUPTION
Primary failure of eruption may result in severalsequelae on the developing dentition, which includemalformation, and impaction or alteration in the erup-tion path of the succeeding developing pre-molars.*"''''''*'25-2'''' Most frequently, primary retentionof primary molars was associated with intraosseousinversion between the embedded tooth and its suc-ceeding premolar.'5"'5-2i,24 -pj g inversion can beexplained by the position of the successor germ thatdevelops palatally and lingually to the crown of itspredecessor tooth. When root formation and eruptionof the primary molar begin, the developing germmoves to a new position between the roots of its pre-cursor. Such movement may not occur if the predeces-sor primary molar remained unerupted or ankylosed.Consequently, the premolar becomes inclinedmesially, distally, lingually, or even occlusally to thecrown of the embedded primary molar."''9,20
In addition, primary retention of primary secondmolars can resuh in ectopic or delayed eruption of thefirst permanent molar, which becomes locked beneaththe distal curvature of the unerupted adjacentmolar. "•25,27,34 ¡f ^^^ fjj-gj permanent molar eruptsectopically, it tilts mesially leading to space loss anddisturbed occlusion. In the permanent dentition, fail-ure of eruption of the permanent molars may result inposterior open bite and malocclusion.''' '"'-' Other pos-sible complications include pathologic root résorptionof the adjacent teeth and pathologic growth of the fol-Iicular tissues leading to cysts, odontogenic tumors, or
56 Volume 32, Number 1 2OOI

Diab •
Fig 1 Intraoral occlusal view showing clinical absence of themandibular right primary second molar. Primary teeth in the archareaiigned normally.
Fig 2 Intraoral view of the mandibular right side showing depres-sion in the area of the missing primary molar. Note the normalcolor of the mucosa, which appears slightly hypertrophie on thebuccal side.
Fig 3 Panoramic radiograph showing failure of eruption of the mandibular rightprimary second molar. The embedded molar is iocated between the permanentfirst molar and the germ of the succeeding second premolar, which is displacedmesially and delayed in its development in comparison with the left second pre-molar.
Fig 4 Periapical radiograph showing the embed-ded molar. The crown is free of caries, restorations,fracture, or attrition, and the roots are fully formed.Note the thick alveolar bone covering the uneruptedtooth, and the slightly enlarged follicie. Also, note themesially dislocated and rotated germ of the develop-ing second premolar.
CASE REPORT
A 5-year-old white female was referred to the pédiatrieservice at the dental clinic of the University of AlbertaHospital, The parents' chief complaint was the absenceof a mandibular primary molar. The child's medicalhistory was unremarkable without familial history oferuption failure of primary teeth. Dental historyincluded regular dental visits without previous facialtrauma or dental infection. The parents presented apreviously taken panoramic, from a private clinic toinvestigate absence of a primary second molar.
Extraoral examination of the child was noncontribu-tory. The intraoral examination showed a complete andnormally developing primary dentition except for theclinical absence of the mandibular right primary second
molar (Figs 1 and 2), There was no complaint of painor discomfort. All the primary teeth were free of cariesor restorations and aligned normally (Fig 1).Examination of the mandibular right side showeddepression in the area of the missing tooth, and the oralmucosa displayed normal color but appeared slightlyhypertrophie on the buccal side. Palpation of the alveo-lar ridge did not reveal any enlargement (Fig 2),
The panoramic and periapical radiographs revealedan embedded mandibular right primary second molar,which was free of caries, restorations, fracture, andattrition. The roots were fully formed without signs ofrésorption, and the tooth was covered with a thicklayer of alveolar bone, with slight enlargement of thesurrounding follicle (Figs 3 and 4), All the permanentmolars and successor premolars were developing
Quintessence International 57

• Diab
Fig 5 Photo showing the design ot the intra-alveolar (dis-tal-shoe) space maintainer. Note the thin and V-shapedintra-alveolar extension.
Fig 6 Intraoral occlusal view showing the space maintainer Themandibular primary first molar was used as an abutment for thestainless steel crown. The intra-alveolar portion is inserted into thesoft tissue so as to contact the mesial surface of the uneruptedfirst permanent molar.
Fig 7 Prontal view showing the normal occlusion foiiowing inser-tion of the space maintainer.
Fig 8 Periapical radiograph showing the position of the ¡ntra-alveolar portion, which is contacting the mesial surface of the per-manent first molar and extending 1,5 mm inferior to the occlusalmarginal ridge. The space maintainer will guide the molar intoproper position and maintain space for the second premoiar.
normally, except the germ of the succeeding secondpremolar, which was displaced mesially and delayed inits development (Figs 3 and 4). The clinical and radio-logic features of this case satisfy the established crite-ria of primary failure of tooth eruption.*'
The treatment plan included surgical extraction ofthe embedded primary second molar followed by inser-tion of a fixed intra-alveolar (distal-shoe) space main-tainer to guide the permanent first molar into properposition and to maintain the space for the second pre-molar. Extraction of the unerupted molar has beenfavored for the following reasons: Normal eruption ofthis tooth was not expected to occur, there was poten-tial for formation of a cyst or odontogenic tumor, andthere was interference with the normal developmentand eruption of the succeeding premolar. Additionally,because of its mesial inclination, the permanent firstmolar, could erupt ectopically leading to space loss and
malocclusion, which may also surgically complicateremoval of the embedded primary molar.
The surgical extraction of the primary second molarhad been performed by an oral surgeon under a generalanesthetic. Extreme care was given to avoid disturbingthe developing germ of the succeeding second premoiarand to maintain crown and root integrity of the perma-nent first molar. A 2-week follow-up evaluation showedthat the child recovered nicely, and she was ready for afixed intra-alveolar space maintainer using the primaryfirst molar as abutment for the stainless steel crown. On asecond visit, the space maintainer was inserted, and aradiograph was exposed to verify the position of theintra-alveolar extension before the crown was cemented(Figs 5 to 8). A 1-week check-up revealed a normal clini-cal picture. The child was happy with the appliance andreported no discomfort so regular follow-up visits werescheduled every 3 months.
58 Volume 32, Number 1, 2001
Diab •
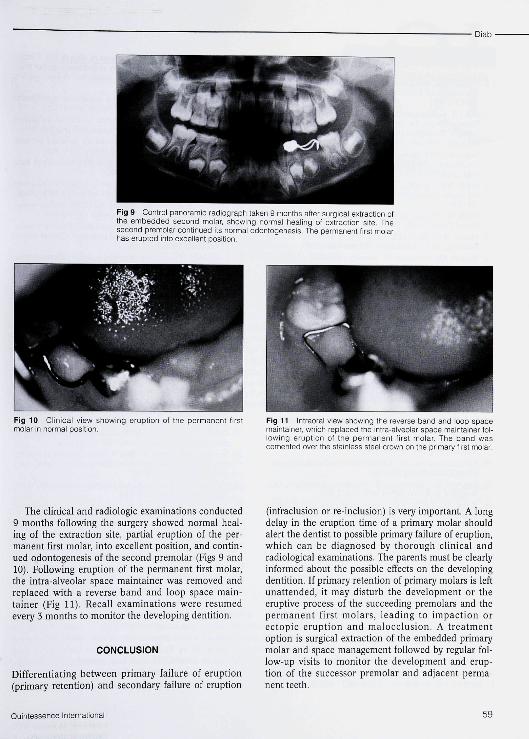
Fig 9 Control panoramic radiograph taken 9 months after surgical extraction ofthe embedded second molar, showing normal healing of extraction site. Thesecond premolar continued its normal odontogenesis. The permanent first moiarhas erupted into excellent position.
Fig 10 Clinical view showing eruption of the permanent firstmoiar in normal position.
Fig 11 Intraoral view showing the reverse band and loop spacemaintainer, which replaced the intra-alveolar space maintainer foi-iowing eruption of the permanent first molar. The band wascemented over the stainless steei crown on the primary first molar.
The clinical and radiologie examinations conducted9 months following the surgery showed normal heal-ing of the extraction site, partial eruption of the per-manent first molar, into excellent position, and contin-ued odontogenesis of the second premolar (Figs 9 and10). Following eruption of the permanent first molar,the intra-alveolar space maintainer was removed andreplaced with a reverse band and loop space main-tainer (Fig 11). Recall examinations were resumedevery 3 months to monitor the developing dentition.
CONCLUSION
Differentiating between primary failure of eruption(primary retention) and secondary failure of eruption
(infraclusion or re-inclusion) is very important. A longdelay in the eruption time of a primary molar shouldalert the dentist to possible primary failure of eruption,which can be diagnosed by thorough clinical andradiological examinations. The parents must be clearlyinformed about the possible effects on the developingdentition. If primary retention of primary molars is leftunattended, it may disturb the development or theeruptive process of the succeeding premolars and thepermanent first molars, leading to impaction orectopic eruption and malocclusion. A treatmentoption is surgical extraction of the embedded primarymolar and space management followed by regular fol-low-up visits to monitor the development and erup-tion of the successor premolar and adjacent perma-nent teeth.
Quintessence International 59

• D iab
REFERENCES
1. Bhaskar SN. Tooth eruption. In: Bhaskar SN (ed). Orban'sHistology and Embriology, ed 11. St Louis: CV Mosby,1990:372-405.
2. Full CA. Conception to age three. The dynamics of change.Dental changes. In: Pinkham JR (ed). Pédiatrie Dentistry.Infancy Through Adolescence, ed 3. Philadelphia: WBSaunders, 1999:148-171.
3. Raghoebar GM, Boering G, Vissink A, Stegenga B. Eruptiondisturbances of permanent molars: A review. ) Oral PatholMed 1991;20:159-166.
4. Proffit WR, Vig ICWL. Primary failure of eruption: A possi-ble cause of posterior open-bite. Am J Orthod 1981 ;80:173-190.
5. Pytllk W. Primary failure of eruption: A case report. IntDental J 1991 ;41:274-278.
6. Shafer WG, Hine MK, Levy BM. A Textbook of OralPathology, ed 4. Philadelphia: WB Saunders, 1983.
7 Bianchi SD, Roccuzzo M. Primary impaction of primaryteeth: A review and report of three cases. J Clin PediatrDent 1991:15:165-168.
8. Winter GB, Gelbier MJ, Goodman JR. Severe infra occlu-sion and failed eruption of deciduous molars associatedwith eruptive and developmental disturbances in the perma-nent dentition: A report of 28 selected cases. Br J Ortho1997;24:149-157
9. de la Rosa-Gay C, Valrnaseda-Castellon E, Costa-Codina X,Gay-Escoda C. Infraclusion of primary molars: Reports ofcases. J Dent Child 1998;65:47-51.
10. Brady J. Familial primary failure of eruption of permanentteeth. BrJ Orthod 1990;17:109-113.
11. Kaban BK, Needleman HL, Hertzberg J. Idiopathic failureof eruption of permanent molar teeth. Oral Surg 1976;42:155-163.
12. Ireland AJ. Familial posterior open bite: A primary failure oferuption. BrJ Orthod 1991;18:233-237
13. Piattelli A, Eleuterio A. Primary failure of eruption. ActaStomatol Belg 1991;88:127-130.
14. Amir E, Duperon DF. Unerupted second primary molar.J Dent Child 1982;49:365-368.
15. Bateman RC, Emmering TE. Deciduous impaction. OralSurg Oral Med Oral Pathol 1976;42:852-853.
16. Black SL, Zallen RD. An unusual case of deciduousimpacted molar. Oral Surg Oral Med Oral Pathol 1977 ;43:160.
17 Borsatto MC, Sant'Anna AT, Niero H, Soares UN, PardiniLC. Unerupted second primary mandibular molar posi-tioned inferior to the second premolar: A case report.Pediatr Dent 1999;21:205-208.
18. Brady FA, Blum M. Unerupted deciduous mandibularmolar. Oral Surg Oral Med Oral Pathol 1979;47:201.
19. Jameson GD, Burke PH. Inversion of second deciduousmolar and second premolar. Br Dent J 1987;162:265-266.
20. Järvinen SHK. Unerupted secondary primary molars:Report of two cases. J Dent Child 1994;61:397-400.
21. Park JK. Submerged impacted primary molar. Oral SurgOral Med Oral Pathol 1979;48:383.
22. Perri de Carvalho AC. A rare case of impacted deciduoussecond molar. Oral Surg Oral Med Oral Pathol 1977;43:647
23. Seeliger JE. Embedded primary maxillary second molartooth. Oral Surg Oral Med Oral Pathol 1975;40:818.
24. Tsukamato S, Braham RL. Unerupted second primary molarpositioned inferior to the second premolar: Clinical report.J Dent Child 1986;53:67-69.
25. Rasmussen P, Kotsaki A. Inherited primary failure of erup-tion in the primary dentition: Report of five cases. J DentChild 1997;64:43-47
26. Alexander SA. Premolar impaction related to ankylosed,totally submerged second primary molar: A case report.J Clin Pediatr Dent 1992;16:267-270.
27 Ben Bassat Y, Brin I, Fuks AB. Occlusal disturbances result-ing from neglected submerged primary molars. J Dent Child1991;58:129-133.
28. Raghoehar GM, Boering G, Stegenga B, Vissink A. Secon-dary retention in the primary dentition. J Dent Child 1991;58:17-22.
29. Kurol J, Magnusson BC. Infraocclusion of primary molars:A histologie study. Scand J Dent Res 1984;92:564-576.
30. Mancini G, Francini E, Vichi M, Tollaro I, Romagnoli P.Primary tooth ankylosis: Report of case with histologicalanalysis. J Dent Child 1995;62:215-219.
31. Boker H, Ten kate LP, Nijenhuis LE. Familial reinclusion ofpermanent molars. Clin Genet 1978;13:314-320.
32. Dewhurst SN, Harris JC, Bedi R. Infraocclusion of primarymolars in monozygotic twins: Report of two cases. Int JPediatr Dent 1997;7:25-30.
33. Helpin ML, Duncan WK. Ankylosis in monozygotic twins,J Dent Child 1986;53:135-139.
34. Rohlin M. An impacted deciduous first molar. Report ofcase. Oral Surg Oral Med Oral Pathol 1974;37:820-823.
60 Volume 32, Number l . 2001


















