Primary Care: Improving Access in Alberta€¦ · Alberta Primary Care Initiative Vision The...
28
Primary Care: Primary Care: Improving Improving Access in Access in Alberta Alberta
Transcript of Primary Care: Improving Access in Alberta€¦ · Alberta Primary Care Initiative Vision The...

Primary Care:Primary Care: Improving Improving Access in Access in AlbertaAlberta

Alberta Primary Care Initiative Vision
The Alberta Primary Care Initiative is an agreement between AHW, AMA and RHAsto:
Improve access to, and effectiveness of, primary care servicesThrough a collaborative, comprehensive approachEntrusting local solutions to local problems

Quality Care
The ability for a patient to receive the care he or she wants/needs when he
or she wants/needs it.Don Berwick

“ The Old Paradigm”Single physician One visit at a time
(responsible for that visit only)Focus is acute and episodicNo measurement
- Guidelines- Outcomes- Value (accountability)
High return visit ratesLow continuity of careFollow up sporadic
“The New Paradigm”Physician and Team Responsible for a patient
panel (population) Focus on:- continuity- optimizing visitsSame day accessScreening and surveillanceChronic disease managementMeasures of process and
outcomesIntegration with specialty
programs/medical specialists (service agreements)Information system to support

What Do Patients Want?
Patients want:To choose their providerTo access their provider when they chooseA quality healthcare experience

The Panel
The patient panel is key to system performance and patient outcomes
“A panel is the unique, unduplicated, discrete patient population for which the physician/team is responsible.”

Panel
Unit of measure – the yardstickDefines work (demand) by physician/teamDivided by patient characteristics (diabetes, depression, elderly, etc.)Adjusted for determinants such as age, sexDefines the population for which each provider is responsible and accountableSum of all panels encompasses the entire population (everyone is cared for)

Physicia n (FTE)
Panel (Adjuste d Panel)
# of Visits by my patients
to me
Return Visit Rate (Provider)
# of Visits by my
patients to anyone in the clinic
Return Visit Rate
(To Clinic)Continuit
y Rate
A (1.6)1622
(1934) 4244 2.6 4401 2.7 96.4%
B (1.0)1703
(1799) 5957 3.5 6519 3.8 91.4%
C (2.0)2453
(2796) 13773 5.6 14884 6.1 92.5%
D (1.2)1904
(2063) 9143 4.8 10603 5.6 86.2%
E (1.2)1956
(2104) 9733 5.0 11783 6.0 82.6%
F (1.7)2885
(3238) 18314 6.3 22171 7.7 82.6%
G (0.1) 267 (234) 853 3.2 1055 4.0 80.9%

Continuity
The percentage of time a patient sees his/her own physician• Chance of a return visit in 2 weeks
• X if see own Family Physician• 2X if see “allied” Family Physician• 4X if see “unallied” physician (Ie. - ER)

“ The Old Paradigm”Single physician One visit at a time
(responsible for that visit only)Focus is acute and episodicNo measurement
- Guidelines- Outcomes- Value (accountability)
High return visit ratesLow continuity of careFollow up sporadic
“The New Paradigm”Physician and Team Responsible for a patient
panel (population) Focus on:- continuity- optimizing visitsSame day accessScreening and surveillanceChronic disease managementMeasures of process and
outcomesIntegration with specialty
programs/medical specialists (service agreements)Information system to support

Access: Why Focus on Delay?
Delays cost moneyDelays adversely effect clinical outcomesWe can only go as fast as the slowest stepPerception that delay = lack of resourceDelays lead to patient dissatisfactionDelays lead to staff dissatisfactionDelays lead to provider dissatisfaction

DemandforAppointments
Panel
The “Universe” From Which Demand Comes Is……
Variation
BacklogNo ShowsTriageRework
Supply
ThePanel

Clinic Weekly Demand and Supply
Clinic Weekly Demand, Supply and Supply Used
0
50
100
150
200
250
300
Demand Suppl y Suppl y Used

Time to 3rd Next Appointment
Average Clinic Delay
0
5
10
15
20
25
30
35
40
8/1/2 0059/1/2 005
10/1/200511/1/200512/1/2005
1/1/2 0062/1/2 0063/1/2 0064/1/2 0065/1/2 0066/1/2 0067/1/2 0068/1/2 0069/1/2 006
10/1/ 200611/1/200612/1/2006
1/1/2 0072/1/2 0073/1/2 007

Results
Patient satisfaction improvedStaff satisfaction improvedProvider satisfaction improvedDelays reducedContinuity improvedQuality improvedUnnecessary visits reducedIncreased capacity

“ The Old Paradigm”Single physician One visit at a time
(responsible for that visit only)Focus is acute and episodicNo measurement
- Guidelines- Outcomes- Value (accountability)
High return visit ratesLow continuity of careFollow up sporadic
“The New Paradigm”Physician and Team Responsible for a patient
panel (population) Focus on:- continuity- optimizing visitsSame day accessScreening and surveillanceChronic disease managementMeasures of process and
outcomesIntegration with specialty
programs/medical specialists (service agreements)Information system to support

200 not seen

Key Quality Indicators for Primary Care
PREVENTIVE MEASURES:Breast Cancer Screening (Mammography)
Percent of eligible women, age 50-69, screened every two years for breast cancer
Cervical Cancer Screening (Pap Smears)Percent of eligible women, age 18-69, screened every three years for cervical cancer

PREVENTIVE MEASURES:Colorectal Cancer Screening
Percent of eligible patients, age 50-80, who are up to date with screening for colorectal cancer (depending on personal risk, type of screening used and recommended frequencies)
Blood Pressure Screening and ControlPercent of eligible patients who had a blood pressure reading done at the most recent clinic visit, or in the last 6 months (if BP reading was less than or equal to 140/90)Percent of eligible patients whose most recent blood pressure (within the last 6 months) was less than or equal to 140/90

CHRONIC DISEASE SCREENING & MANAGEMENT MEASURES:Diabetes HgbA1c Testing
Percent of diabetic adult patients having at least one HgbA1c test done in the past 6 monthsPercent of diabetic adult patients whose most recent HgbA1c reading (within last 6 months) was less than or equal to 7.0
IMMUNIZATION MEASURES:Influenza Vaccination
Percent of patients, age 65 and older, who received influenza vaccination within the previous 12 months
Pneumococcal VaccinationPercent of patients, age 65 and older, who have received pneumonia vaccination

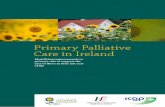
38%
47%
57%
15%
55% 56%
18% 18%
30%
0%
10%
20%
30%
40%
50%
60%
% Patients with Timely Screening
Breast Cervical Colorectal
Types of Cancer Screening
Cancer Screening RatesRandom samples of 10 eligible patient charts per provider were pulled and reviewed for each of the below measures to
determine if timely cancer screening was performed for each patient
Clinic A Clinic B Clinic C

33%
80%
24%
76%
71%
84%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
% o
f Pat
ient
s
Clinic A Clinic B Clinic C
Blood Pressure Monitoring and OutcomesRandom samples of 10 eligible patient charts per provider were pulled and reviewed to determine if BP was measured at
each patient's most recent visit and if the most recent BP for each patient was normal (< 140/90)
BP Done at Last Visit BP in Control

63%
48%45%
55% 56%
69%
0%
10%
20%
30%
40%
50%
60%
70%
% of Patients
Clinic A Clinic B Clinic C
Diabetic HgbA1c Testing and ControlRandom samples of 10 eligible diabetic patient charts per provider were pulled and reviewed to determine if each patient
had a HgbA1c test done within the previous 6 months and if it was in normal range (< 7.0%)
HgbA1c Done in Last 6 Months
HgbA1c in Control

10%
100%
20%
90%
30%
60%
30%
70%
0%
60%
20%
70%
30%
70%
30%
80%
30%
90%
30%
60%
40%
90%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% P a t i e n t s*Samples may be smaller f or some physician s wher e t her e wer e n ot 10 pat ien t s on t heir pan els who met
in clusion cr it er ia
P hysi c i an A Physi ci an B P hysi ci an C P hysi c i an D Physi c i an E Physi ci an F P hysi ci an G P hysi c i an H P hysi c i an I Physi ci an J P hysi ci an K
B loo d Pressure M o nit o ring and Out co mesRandom sampl es of 10* el i gi bl e pat i ent char ts per pr ovi der wer e pul l ed and r evi ewed to deter mi ne i f B P was measur ed at each pat i ent 's most r ecent vi s i t and i f the most r ecent BP f or each pat i ent was nor mal (< 140/ 90)
BP Done at Last VisitBP in Control

50%
20%
30%
40% 40% 40%
50%
30% 30%
80%
60% 60%
40%
30%
50%
90%
40% 40%
50%
70%
10% 10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
% o f P a t i e n t s*Samples may be smaller f or some physician s wher e t her e wer e n ot 10 pat ien t s on t heir pan els who met
in clusion cr it er ia
Physi ci an A P hysi ci an B P hysi c i an C Physi ci an D Physi ci an E P hysi ci an F P hysi c i an G Physi c i an H Physi ci an I P hysi ci an J P hysi c i an K
Di abet i c HgbA1c T est i ng and Cont r olRandom sampl es of 10* el i gi bl e di abet i c pat i ent char t s per pr ov i der wer e pul l ed and r ev i ewed to deter mi ne i f each pat i ent had a HgbA1c test done wi thi n t he pr evi ous 6 months and i f i t was i n nor mal r ange (< 7.0%)
HgbA 1c Done i n Last 6 M onths HgbA1c i n Cont r ol

Supporting the Panel
The “core” family practice team is the group that support physicians in their day to day generalist work of serving their panel of patientsRHA services, including community care nurses, public health nurses, rehab, social work and mental health, community and hospital based pharmacies, and specialists support the primary care teams to be successful.

Measure Value?
You won’t fix:CPGOutcomesCare plansAccessCapacityPhysician remunerationSpecialty referralLab usageHuman resources
……………………………..Without Panels

For More Information
Please visit our website at:www.chinookprimarycarenetwork.ab.ca
Or contact the Chinook Primary Care Network office at (403) 388-6510