
PREVENTIVE AND REHABILITATIVE …ijncollege.edu.my/PDF/20161112 - PREVENTIVE AND...PREVENTIVE AND...
41
PREVENTIVE AND REHABILITATIVE MANAGEMENT OF ACUTE CORONARY SYNDROMES (NSTEMI, STEMI, PCI) Dato’ Dr. Balachandran Kandasamy Institut Jantung Negara 12 th November 2016
Transcript of PREVENTIVE AND REHABILITATIVE …ijncollege.edu.my/PDF/20161112 - PREVENTIVE AND...PREVENTIVE AND...
PREVENTIVE AND REHABILITATIVE
MANAGEMENT OF ACUTE CORONARY SYNDROMES
(NSTEMI, STEMI, PCI)Dato’ Dr. Balachandran Kandasamy
Institut Jantung Negara 12th November 2016
KEY MESSAGES
1. Initiate a long-term management plan for all patients with acute coronary syndromes (ACS)
2. Consider guideline-recommended medicines for all patients with ACS
3. Identify risk factors and refer all patients with ACS to secondary prevention programs
4. Communicate management plan to the patient, carers and the community healthcare providers
INITIATE A LONG-TERM MANAGEMENT PLAN FOR ALL PATIENTS WITH ACUTE CORONARY SYNDROMES
“Patients with ACS are at high risk of further cardiovascular events and death. For long-term management a medicines management plan, a chest pain action plan and a comprehensive cardiovascular risk reduction program are recommended. Communicate this plan to the patient and/or carer and their community healthcare providers”.
INITIATE A LONG-TERM MANAGEMENT PLAN FOR ALL PATIENTS WITH ACUTE CORONARY SYNDROMES
i. Medicines management plan
ii. Chest pain action plan
iii. Identify risk factors and refer to secondary prevention programs
i. Medicines Management Plan
• Consider starting guideline-recommended medicines in hospital before discharge.
• Provide all patients with a written medicines management plan which includes:
a list of all medicines
the dose and plan for any required dose titration
intended duration of therapy
the purpose and potential benefits of therapy
potential adverse effects of each medicines
schedule for follow-up and monitoring
access to consumer medicine information.
INITIATE A LONG-TERM MANAGEMENT PLAN FOR ALL PATIENTS WITH ACUTE CORONARY SYNDROMES
“Communicate the management plan to patients and all those involved in care”
ii. Identify Risk Factors And Refer To Secondary Prevention Programs
Discuss the warning signs of a heart attack and an immediate plan of action, including the use of short-acting nitrates and the importance of dialling 000 if pain is not relieved. Each patient should receive a written chest pain action plan which includes:
warning signs of a heart attack
when and how to take the short-acting nitrate
self-administration of aspirin, unless contraindicated
instructions to call an ambulance if chest pain or discomfort lasts longer than 10 minutes
additional instructions for patients who live in rural and remote locations
iii. Identify Risk Factors And Refer To Secondary Prevention Programs
Actively refer to, and encourage attendance at, secondary prevention and cardiac rehabilitation programs.
Provide education and set goals on lifestyle factors, including advice on smoking cessation where appropriate.
Assess for depression and level of social support.
CONSIDER GUIDELINE-RECOMMENDED MEDICINES FOR ALL PATIENTS WITH ACS
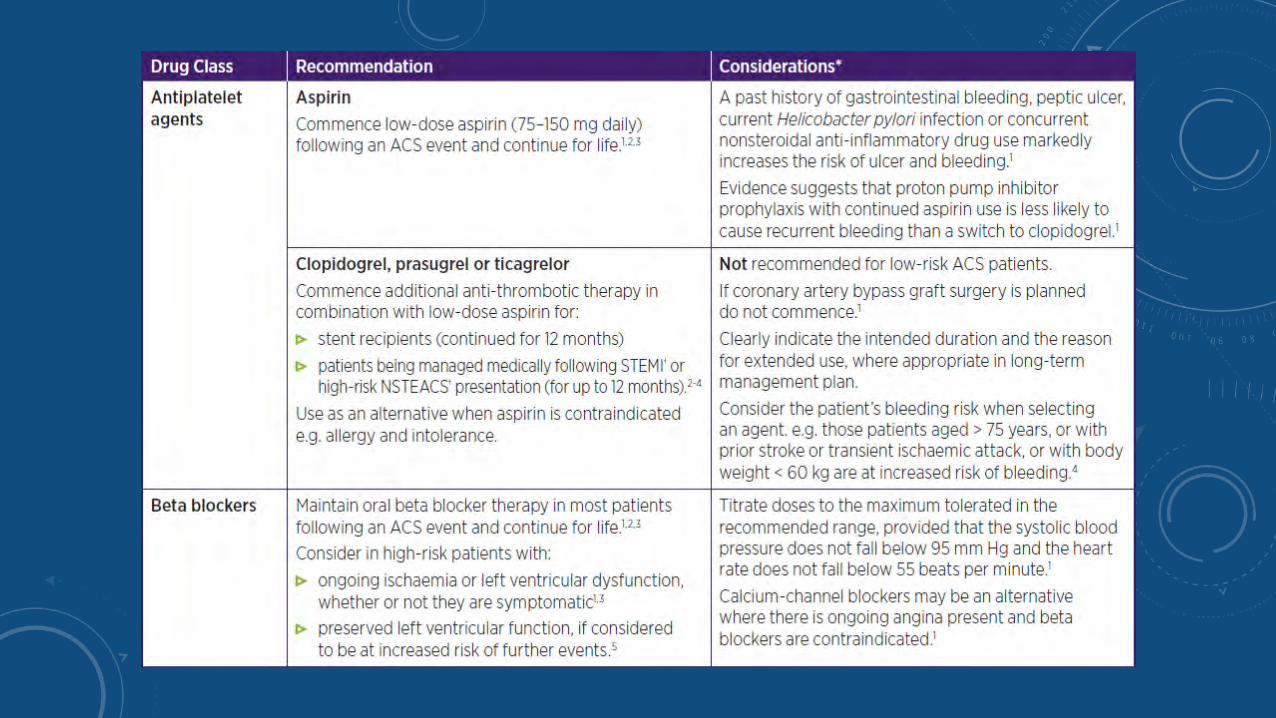
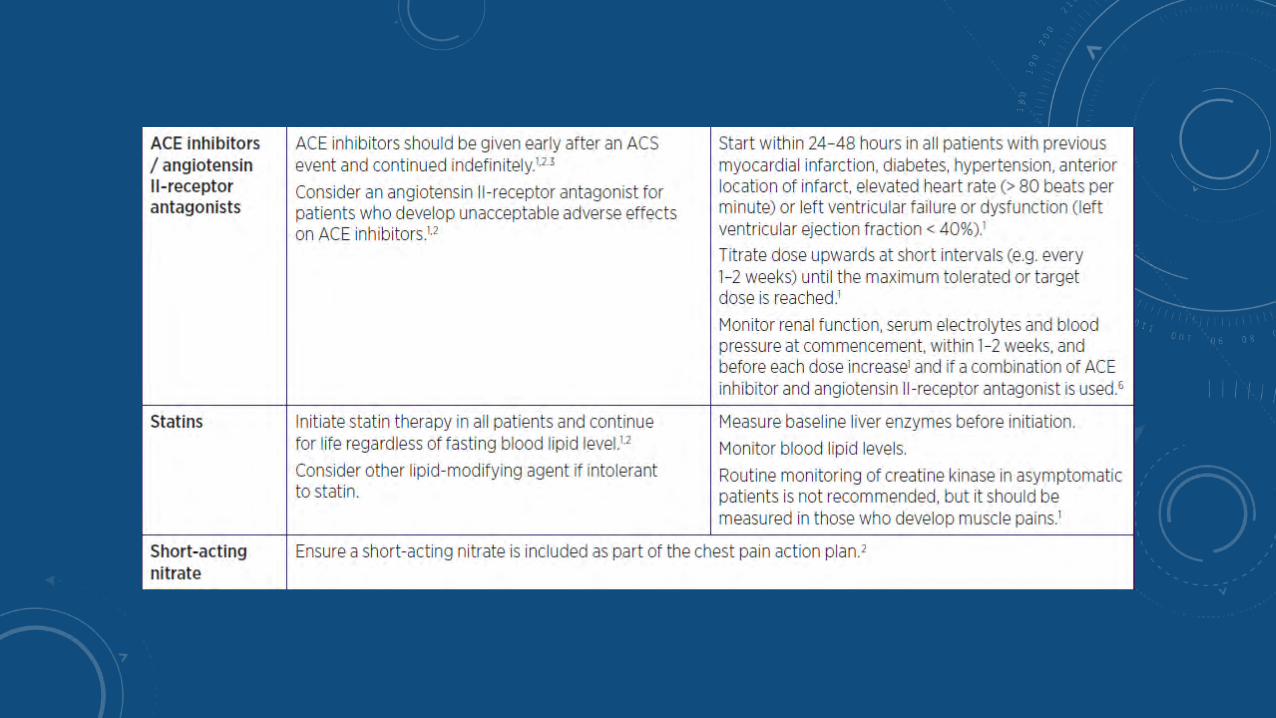
The combination of antiplatelet agents, a beta blocker, a statin and an angiotensin-converting enzyme (ACE) inhibitor is recommended for most patients, unless contraindicated. All four drug classes have been proven to reduce subsequent cardiac events and death.
Individualise therapy according to known comorbidities, risk of adverse effects and clinical judgement.
If the guideline-recommended therapy is not indicated for an individual, document this and the reason(s) why in the patient’s medical record and long-term management plan.
IDENTIFY RISK FACTORS AND REFER ALL PATIENTS WITH ACS TO SECONDARY PREVENTION PROGRAMS
• Provide patients with a self-management plan before discharge, as patients and their families/carers are focused on promoting health and are more receptive to medical interventions immediately after an acute event.
• The plan should include advice on lifestyle changes that will reduce the risk of further cardiac events (including quitting smoking, good nutrition, moderating alcohol intake, regular physical activity and weight management), as appropriate. All patients should have access to, and be actively referred to, comprehensive secondary prevention and cardiac rehabilitation programs.
Refer All Patients to Their Closest Available Cardiac Rehabilitation Program
Cardiac rehabilitation is a proven effective intervention.
Attendance at cardiac rehabilitation outpatient programs reduces risk of further cardiac events.
Cardiac rehabilitation, including advice about physical activity, improves individual health outcomes.
Patients who participate in cardiac rehabilitation programs can improve physical activity, weight loss, smoking cessation, blood lipid levels and blood pressure control.
CARDIAC REHABILITATION
PRINCIPAL GOAL:
• To lessen the risk of future coronary events, control symptoms arising from coronary disease and to return the patient to optimal or previous functional status
• Patient population predominantly confined to post MI, bypass graft, angioplasty & stable angina but must also be made available to heart failure patients.
M.A CALDWELL & K. DRACUP, JOURNAL OF CARDIOPULMONARY REHABILITATION 2001
THE FOUR PHASES OF CARDIAC REHABILITATION
• Phase I – Before discharge from hospital
• Phase II – Early post-discharge period
• Phase III – 4 -6 weeks after an acute cardiac event
• Phase IV – Long term maintenance of changed behaviour
Inpatients & Outpatients
Ward
Gym
Exercise Programme
Patient Referral
Acute Care Cardiac
Rehabilitation
Programme I &
II
PHYSIOTHERAPY IN IJN
OTHER BENEFICIAL EFFECTS OF CARDIAC REHABILITATION FOR PATIENTS WITH CHD
• Improves Control of Dyslipidemia in secondary prevention
B.L.,Verges et al Journal of Cardiopulmonary Rehabilitation, 1998
• Weight loss intervention
P.D., Savage et al Journal of Cardiopulmonary Rehabilitation, 2002
• Post Myocardial infarction or CABG
J. Redfern, Journal of Physiotherapy, 2011
• Stable Chronic Heart Failure- can achieve significant improvement in functional capacity from a low intensity exercise training program.
R. Belardinelli et al J Am Coll Cardiol, 1995
• Exercise training improves exercise tolerance and LV function in patients with Dilated Cardiomyopathy
K.Q., Stolen et al J Am Coll Cardiol, 2003
“The Sum of Activities required to ensure the patients, the best possible
physical, mental and social conditions, so that they may (by their own
efforts), resume and maintain as normal a place as possible in the
community”
WHO Definition of Cardiac Rehabilitation
F.J.Brannon et al:Cardiopulmonary rehabilitation: Basic Theory
and Application 2nd Ed , pg.148(1993)
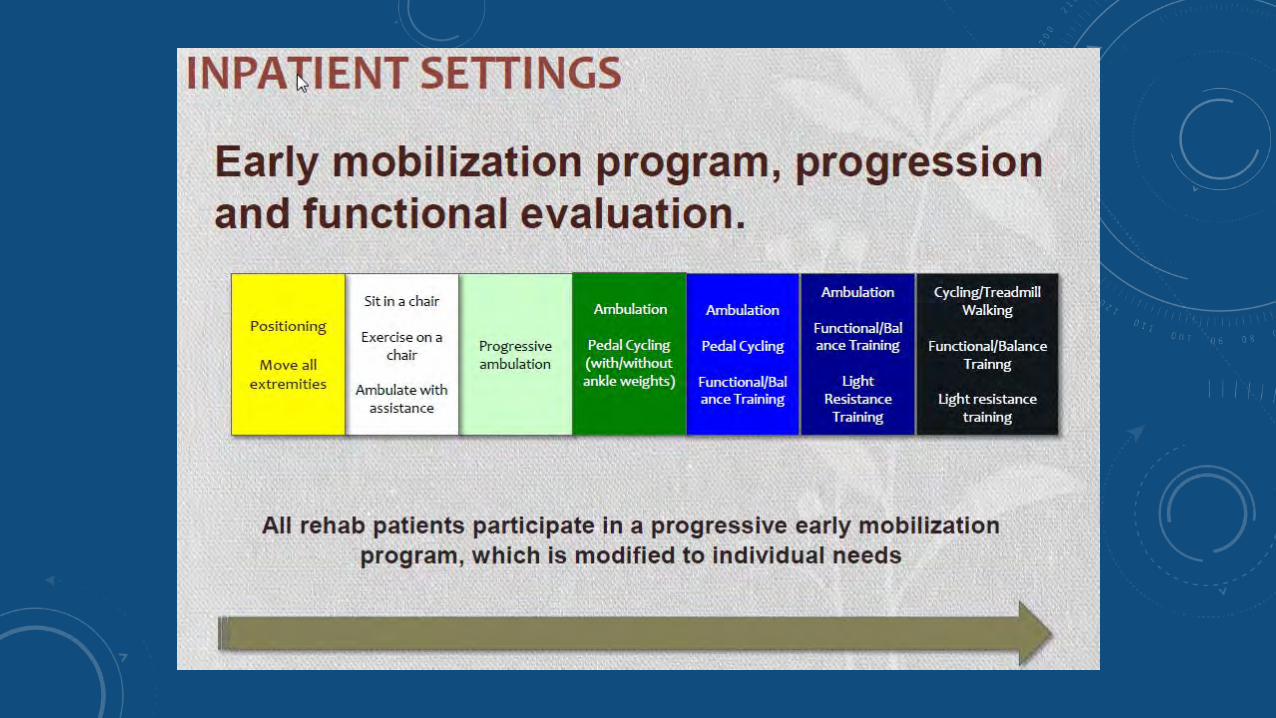
CARDIAC REHABILITATION PHASE I (ICU/ WARDS/ GYM)
• Inpatient recovery program
• Post MI start 2-4 days after hospitalized
• Post surgery start 1-2 days after surgery
• Lasts for 2-3 weeks
• Intensive medical supervision
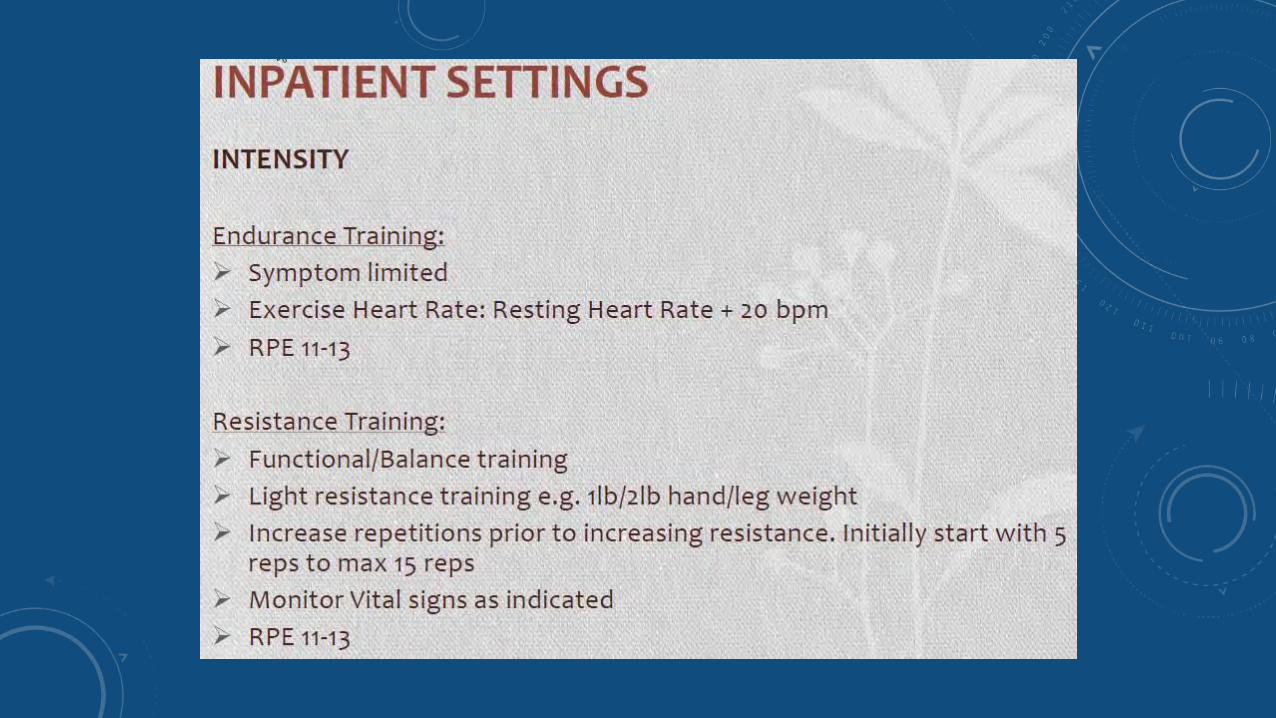
• Low intensity exercise (1.5 - 2.5 METS)
• 60% - 70% of MHR
• Exercise done daily- shoulder and arm exercises, gentle trunk exercises, ambulating short distances, gym & a flight of stairs without adverse symptoms
CARDIAC REHABILITATION PHASE II (IJN)
• Out patient convalescence program
• Starts within 2-3 weeks of discharge
• Lasts for 3 months
• Referred by physician and medically supervised
• Light to moderate exercise (2 - 5 METS)
• 65% - 75% of MHR
• 3 times per week14/11/2016 24

PHYSIOTHERAPY & REHABILITATION DEPT., IJN, CRP PHASE II
1. Strengthening Exercises
2. Endurance Exercise
(stationary bike or treadmill)
3. Exercise Tolerance( step
board)
4. Exercise tolerance
(walking for 6 mins)
5. Stretching and Cool down
Circuit
TrainingAssessment
Re-assessment
Patient Education 14/11/2016 25
CRP PHASE II -IJN
• Warm up/Cool down
- A gradual and progressive warm-up of 10 to 15 mins. incorporating mobility and stretching
*Strenuous exertion without
previous warm up produces
Ischaemic ST segment changes
and arrhythmias & reduction of left
Ventricular ejection fraction, even
In healthy individuals.
(BACR, 1995 pg. 84)14/11/2016 26
EXERCISE IN CARDIAC REHABILITATION
• Exercise, the cornerstone of CR esp. Phase II & III.
• Prescribe with the same precision as any medication.
• The ex. dose is the combination of intensity, frequency and duration of physical activity.
• Sufficient to produce a conditioning, but not enough to provoke complication.
• Aimed at enhancing cardiovascular fitness, strength, endurance and flexibility.
PATIENT EDUCATION (CRP I & II)
Group Education
One to one home
counselingOR
CR EFFECTIVENESS IS DETERMINED BY A MULTIDISCIPLINARY APPROACH
• Cardiothoracic Surgeon
• Cardiologist
• Psychologist
• Physiotherapist/Exercise Physiologist
• Nurses/ Cardiac Nurse
• Dietician
• Pharmacist
• Diabetic Counselor
• Quit Smoking Counselor
• Patient and family
Provide Smoking-cessation Advice And Support To All Patients Who Smoke
Smoking is one of the most significant risk factors for cardiovascular disease, including myocardial infarction (MI).
Stopping smoking is associated with a substantial reduction in risk of all-cause mortality among patients with coronary heart disease.
Quitting smoking reduces the likelihood of a repeat cardiac event and the chances of developing other forms of cardiovascular disease.
There is a rapid reduction in the risk of coronary heart disease within one year of quitting smoking.
Brief educational interventions of 3–5 minutes have been shown to increase quitting rates compared with no intervention.
CATEGORY OF CLIENTS:
Referral case
Referred by IJN Doctors ( in patient/outpatient)
referral form doctor required
cardiac Rehab Nurse will see patient and conduct counselling
Self referred
Patient call IJN for appointment
slot will be given to client
will be seen in clinic for counselling
New referral - Outpatient / in patient
( We will see on the same day )
QUIT SMOKING CLINIC IJN
WHY IS SMOKING HARMFUL TO THE CARDIOVASCULAR SYSTEM ?
• Increased tendency for vasoconstriction
• Increases level of bad cholesterol ie. LDL
• Reduces level of good cholesterol ie. HDL
• Reduces beneficial effects of medications eg. Statins, Aspirin
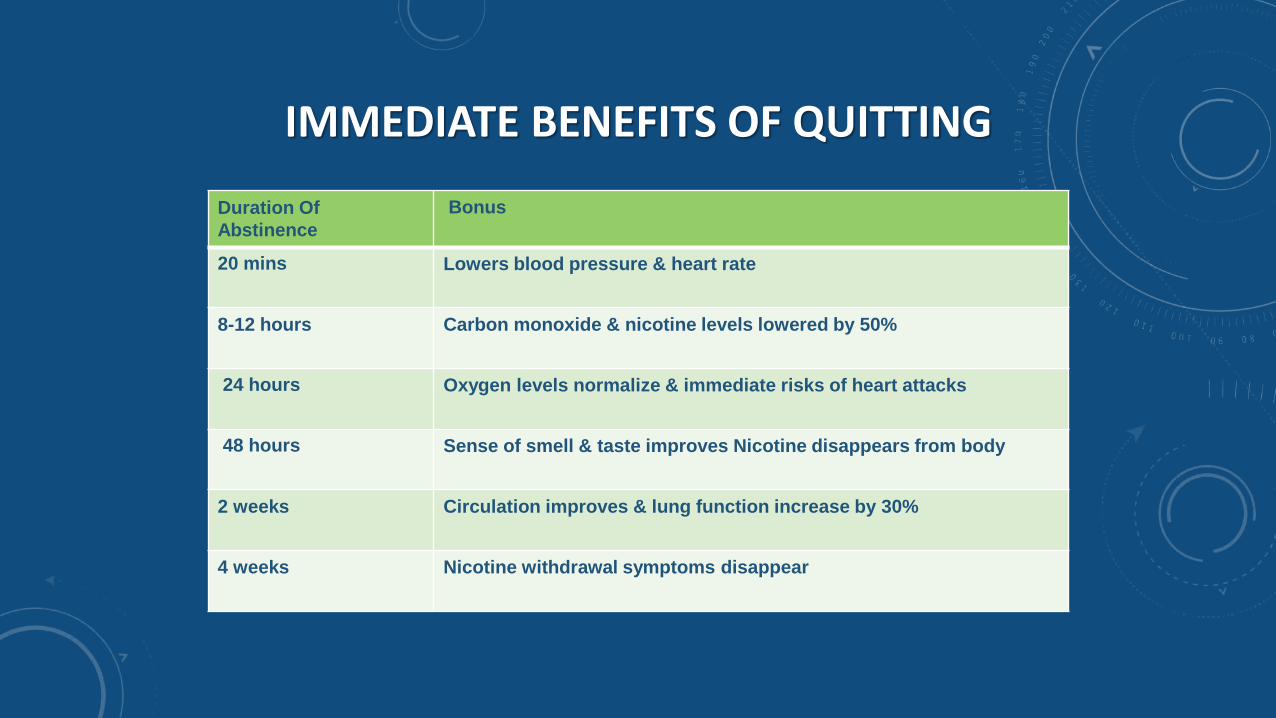
IMMEDIATE BENEFITS OF QUITTING
Duration Of
Abstinence
Bonus
20 mins Lowers blood pressure & heart rate
8-12 hours Carbon monoxide & nicotine levels lowered by 50%
24 hours Oxygen levels normalize & immediate risks of heart attacks
48 hours Sense of smell & taste improves Nicotine disappears from body
2 weeks Circulation improves & lung function increase by 30%
4 weeks Nicotine withdrawal symptoms disappear
CONT..The Right Way of Quitting
• Fix a date , be confident and look forward• Always be positive and get support • Fight your urge to smoke or use nicotine replacement therapy• Drink lots of water – to flush chemical• Exercise > 5 minutes (stretching )or exercise• Wash faces & keep hand wet• Take shower more frequent• Do chew gum with sugar free or vitamin C• Avoid caffeine drink change to fruit juice • Stop thinking about cigarette , divert to other things • Distract yourself from situations which encourages smoking• Do pray

TREATMENT AVAILABLE (PHARMACOLOGIC APPROACH)
Non nicotine treatment (Non - NRT) in IJN1.Champix tablet (varenicline)
Nicotine treatment (NRT) buy from other companies
1.Nicorette tablet 2.Nicotine patch3.Nicotin gum
If patient request for NRT, send prescription slip to retail pharmacy, purchase and call patient.
CONT..
• Choosing the right pharmacologic agent
• Patient preference
• Patient ‘s previous experience with medication, either positive or negative
• Ease of administration
• Compliance
• Health care professional’s familiarity with medications
CONT....
1. (Non NRT – TAB CHAMPIX – VARENICLINE TARTRATE )Doses :0.5 mg DLY x 3 /70.5 mg BD x 4/71.0 mg BD x 11/52
2. Treatment for 12 weeksAm dose - After light breakfast
Or 11/2- 2 hours after heavy breakfastPm dose - 1.5 hrs. - 2 hrs. after dinner(To prevent from nausea or vomiting)NRT can take with others medication
COMMUNICATE MANAGEMENT PLAN TO THE PATIENT, CARERS AND THE COMMUNITY HEALTHCARE PROVIDERS
• Effective communication between the hospital, patients and their families/carers, and community healthcare providers enhances long-term adherence with prescribed therapies and lifestyle changes. Include the patient’s GP and, as applicable, community pharmacists, community nurses and other outpatient services.
Adherence to Therapy Improves Survival
Patients discontinuing their medicines after an MI is common, often soon after discharge. Minimise this by:
Educating patients about their medicines. This is likely to improve their understanding and knowledge and thus adherence.
Starting patients on secondary preventive therapies and lifestyle changes before they leave hospital. This significantly improves long-term adherence.
Involving family members in educational efforts. Smoking cessation, weight loss and increased physical activity are enhanced by enlisting the support of family members.
Communicating risk of future cardiovascular events.
Long-Term Management
A discharge letter/summary should include:
A complete list of medicines. Document why guideline medicines have not been prescribed and alternative medicine(s) used.
Any changes to medicines being taken at admission.
A plan for required dose titration (include who is responsible).
Recommendations for monitoring and management of medicine-related adverse effects.
Treatment goals including blood pressure, blood lipid levels, weight, HbA1c.
Referral for cardiac rehabilitation.
Advice given on lifestyle modifications (e.g. smoking cessation as applicable).
Recommendations for use of dose-administration aids, carer support and referral for a Home Medicines Review.

Thank you


















