Texas HIV Medication Program Dwayne Haught, MSN, ACRN May 31, 2007.
date post
21-Dec-2015Category
view
217download
3
Prevention with Prevention with Positives:Positives:
Promoting Change Promoting Change While the Clock TicksWhile the Clock Ticks … …
Robert T. Carroll, PhC, RN, ACRNWashington State Education Coordinator,
Northwest AIDS Education and Training Center
U NIVERSITY OF WASHINGTON 2U NIVERSITY OF WASHINGTON 2
Today’s GoalsToday’s Goals• Describe the theoretical and
practical underpinnings of Prevention with Positives programs
• Provide a brief overview of the Motivational Interview process for promoting behavior change
• Describe the key elements of a brief motivational intervention focusing on prevention with PLWH/A
U NIVERSITY OF WASHINGTON 3U NIVERSITY OF WASHINGTON 3
Why the Emphasis on Why the Emphasis on Prevention with Prevention with
Positives?Positives?Every person
infected with HIV was exposed by
a person who was HIV-Positive.
U NIVERSITY OF WASHINGTON 4U NIVERSITY OF WASHINGTON 4
• New generation of prevention programs targeting individuals who
• Current emphasis arises from
What is Prevention What is Prevention with Positives (PwP)?with Positives (PwP)?
• Have already tested positive for HIV
• May be at risk of transmitting the disease
• CDC 5-year plan to reduce rates of infection by 1/2 over the next 5 years
U NIVERSITY OF WASHINGTON 5U NIVERSITY OF WASHINGTON 5
Why the New Focus on Why the New Focus on Prevention with Prevention with
Positives?Positives?Advancing HIV Prevention (AHP)New Strategies for a Changing Epidemic
• September 2003
• CDC initiative to reduce barriers to early diagnosis of HIV and increase access to quality medical care, treatment, and ongoing prevention services for PLWH/A
U NIVERSITY OF WASHINGTON 6U NIVERSITY OF WASHINGTON 6
Why a New Initiative Why a New Initiative for HIV Prevention?for HIV Prevention?
• 40,000 new HIV infections still occur in the United States each year
• One-quarter of the 850,000 - 950,000 PLWH/A in the U.S. do not yet know they are infected
• Recent increases in syphilis diagnoses among men who know they are HIV-infected suggests an increase in risk behaviors among PLWH/A and their partners
U NIVERSITY OF WASHINGTON 7U NIVERSITY OF WASHINGTON 7
Local TrendsLocal Trends
Insert local/regional epidemiological charts and/or graphs which provide evidence of increases in new infections related to engagement in high risk activities (i.e., increase/spikes in other STI rates)
U NIVERSITY OF WASHINGTON 8U NIVERSITY OF WASHINGTON 8
AHP Initiative AHP Initiative Strategies Strategies
Make HIV testing a routine part of medical care when and where patients receive care
• Use new models to diagnose HIV infection outside of traditional medical settings
• Prevent new infections by working with HIV positive people and their partners
• Continue to decrease mother-to-child HIV transmission
U NIVERSITY OF WASHINGTON 9U NIVERSITY OF WASHINGTON 9
Prevent New Infections Prevent New Infections by Working with by Working with PLWH/APLWH/A
• Publish Recommendations for Incorporating HIV Prevention into the Medical Care of Persons with HIV Infection (CDC, HRSA, NIH, and IDSA)
• Fund demonstration projects to provide PCM for people with HIV who have ongoing high-risk behavior
• Fund demonstration projects of new models of PCRS
• In 2004, implement these services
U NIVERSITY OF WASHINGTON 10U NIVERSITY OF WASHINGTON 10
Incorporating HIV Prevention Incorporating HIV Prevention into the Medical Care of into the Medical Care of
PLWH/APLWH/ARRecommendations of CDC, the Health Resources and Services Administration, the National
Institutes of Health, and the HIV Medicine Association of the
Infectious Diseases Society of America
MMWR 2003 July 18; 52
U NIVERSITY OF WASHINGTON 11U NIVERSITY OF WASHINGTON 11
How Does it Work?How Does it Work?Individual-focused PwP interventionshelp PLWH/A reduce their transmission rates through theoretically-based interventions which--
• Help PLWH/A feel better about themselves
• Decrease the stigma associated with HIV
• Help PLWH/A take responsibility for their lives and for stopping the spread of HIV
U NIVERSITY OF WASHINGTON 12U NIVERSITY OF WASHINGTON 12
How is this How is this Accomplished?Accomplished?
•Peer-based workshops and focus groups•One-on-one transmission risk counseling•Psycho-social assessment and supportive interventions•Case management•HIV status support groups
Prevention with Positives programs aim to build self-esteem and enrich coping skills through supportive services such as
U NIVERSITY OF WASHINGTON 13U NIVERSITY OF WASHINGTON 13
PwP Programs in the PwP Programs in the U.S. U.S.
• CA office of AIDS EIP programPrevention integrated with care & treatment Prevention Case Management
• HIV Stops with me: LA, SF, BostonSocial marketing approach
• Prevention for HIV-Infected Person’s Project (PHIPP)
Multi-site CDCP demonstration project
• Positive Power (Seattle & WA State)
Targeting gay and bisexual men through individual and group work
• Partnership for Health (USC)2-day TOT program to implement4-hour individual intervention
U NIVERSITY OF WASHINGTON 14U NIVERSITY OF WASHINGTON 14
I know there must be a I know there must be a theory in there theory in there somewhere…somewhere…
Yup.
Most PwP programs are based on one or many of the seven most popular theoretical models of (HIV) health promotion/risk behavior change
U NIVERSITY OF WASHINGTON 15U NIVERSITY OF WASHINGTON 15
Seven Theoretical ModelsSeven Theoretical Models (HIV) Health Promotion & Risk Behavior (HIV) Health Promotion & Risk Behavior
ChangeChange
1. Health Belief model2. AIDS Risk Reduction Model3. Trans-theoretical model4. Social Cognitive Theory model5. Theory of Reasoned Action6. Theory of Planned Behavior7. Information-Motivation-Behavioral
Skills model
U NIVERSITY OF WASHINGTON 16U NIVERSITY OF WASHINGTON 16
What do these What do these Theories have in Theories have in
Common?Common?KNOWLEDGE +
SKILLS +MOTIVATION +
RESOURCES +SUPPORT =
Behavior Change!
U NIVERSITY OF WASHINGTON 17U NIVERSITY OF WASHINGTON 17
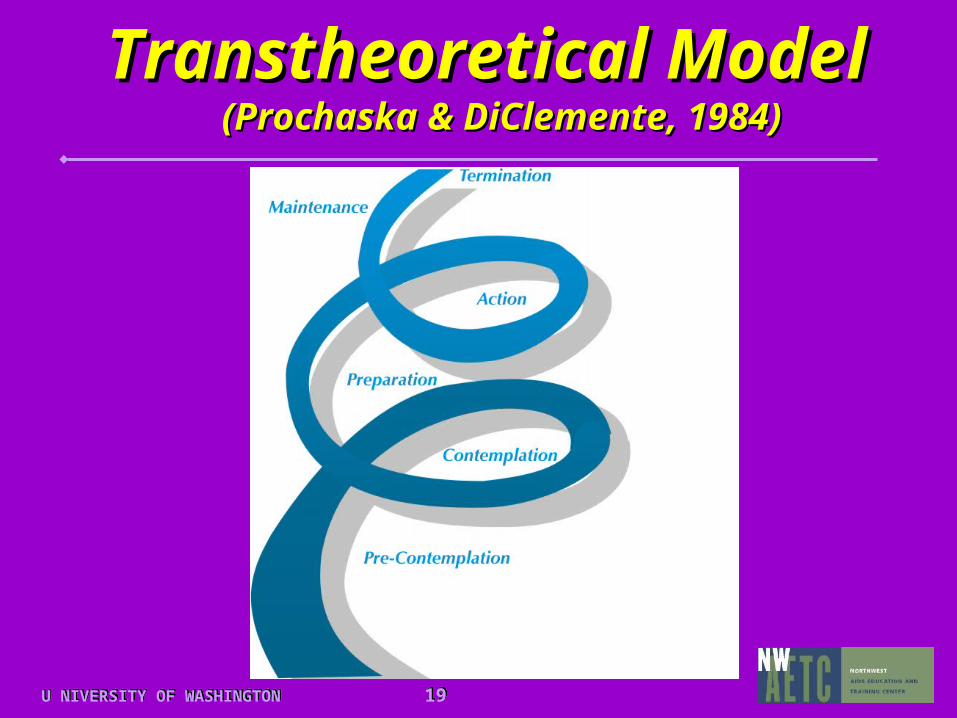
Transtheoretical ModelTranstheoretical Model (Prochaska & DiClemente, 1984)(Prochaska & DiClemente, 1984)
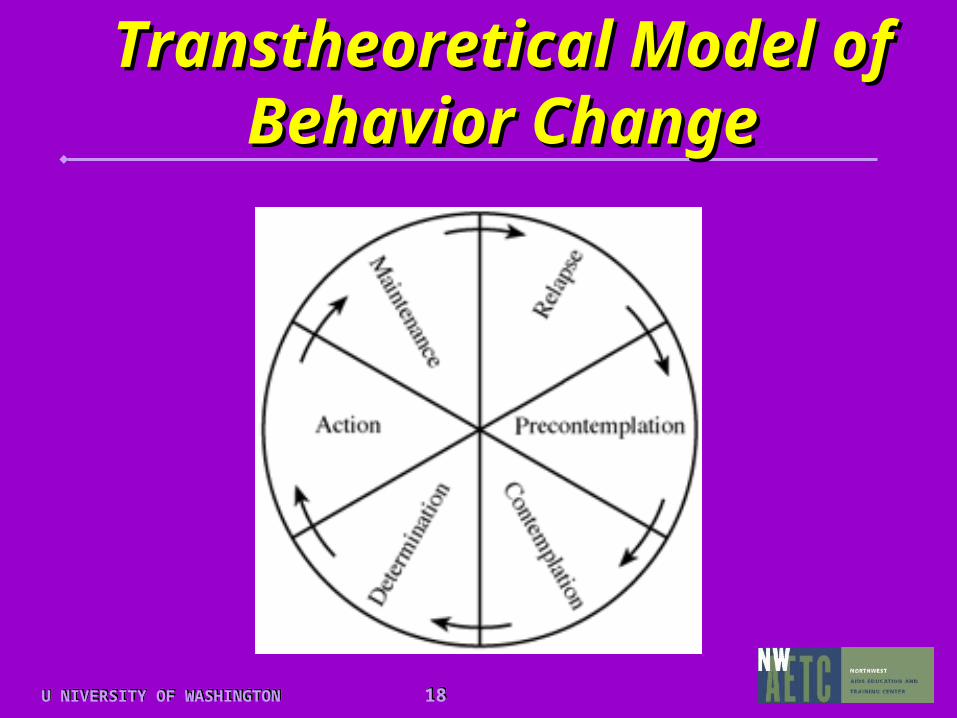
1. Precontemplation: Not even thinking about it
2. Contemplation: Thinking about it
3. Determination/Preparation: Taking steps to start behavior
4. Action: Person tries behavior
5. Maintenance: Person does behavior regularly
6. Relapse: Person slips up & needs to make adjustments
Six stages of behavior change
U NIVERSITY OF WASHINGTON 18U NIVERSITY OF WASHINGTON 18
Transtheoretical Model Transtheoretical Model of Behavior Changeof Behavior Change
U NIVERSITY OF WASHINGTON 19U NIVERSITY OF WASHINGTON 19
Transtheoretical Transtheoretical ModelModel
(Prochaska & DiClemente, 1984)(Prochaska & DiClemente, 1984)
U NIVERSITY OF WASHINGTON 20U NIVERSITY OF WASHINGTON 20
Transtheoretical ModelTranstheoretical Model (Prochaska & DiClemente, 1984)(Prochaska & DiClemente, 1984)
• Change is an incremental process and not a discrete outcome
• Change takes time• Harm/risk reduction is a good goal• Relapse is the rule, not the exception• Two dimensions: stages and
processes
Key assumptions of the model
U NIVERSITY OF WASHINGTON 21U NIVERSITY OF WASHINGTON 21
But it must have But it must have structure and structure and
purpose…purpose…
Brief Motivational Brief Motivational Interviewing Works!Interviewing Works!
U NIVERSITY OF WASHINGTON 22U NIVERSITY OF WASHINGTON 22
First Things First!First Things First!
• Work with the patient to identify a behavior to be targeted for change
• Identify where the patient stands on the readiness-to-change continuum
• Establish with the patient incremental goals – appropriate to their readiness - to move toward the desired change
U NIVERSITY OF WASHINGTON 23U NIVERSITY OF WASHINGTON 23
• Document, Document, Document!
• Ensure full staff understanding of, buy-in for, and consistency in delivery of the plan.
Remember…Remember…
Initial plan, subsequent encounters, outcomes, and changes to the plan
U NIVERSITY OF WASHINGTON 24U NIVERSITY OF WASHINGTON 24
FRAMES:FRAMES: Active Ingredients of Active Ingredients of the Effective Brief Motivational the Effective Brief Motivational InterviewInterview
F : FeedbackR : ResponsibilityA : AdviceM : MenuE : EmpathyS : Self-Efficacy
(Miller & Rollnick, 1991)
U NIVERSITY OF WASHINGTON 25U NIVERSITY OF WASHINGTON 25
Key ingredient which supports
the client’s ability to change.
MOTIVATIONMOTIVATION
U NIVERSITY OF WASHINGTON 26U NIVERSITY OF WASHINGTON 26
General Principles of General Principles of Motivational Motivational InterviewingInterviewing
• Express empathy
• Develop discrepancy
• Avoid argumentation
• Roll with resistance
• Support self-efficacy
U NIVERSITY OF WASHINGTON 27U NIVERSITY OF WASHINGTON 27
Phases of the Phases of the Motivational Interview Motivational Interview
Practice Practice I. Build motivation for change
Sensitive questioning and reflection encourage the person to articulate self-motivational statements and the arguments for change
II. Strengthen commitment to change
Motivation-building moves to key questions designed to evoke problem-solving and commitment to change
U NIVERSITY OF WASHINGTON 28U NIVERSITY OF WASHINGTON 28
But What Can I Do in But What Can I Do in a Brief Period of a Brief Period of
Time?Time?If all you have is a short time in
which to make an impact-- seek at least
not to do any damagenot to do any damage
by entrenching resistance and discouraging change.
(Miller & Rollnick, 1991)
U NIVERSITY OF WASHINGTON 29U NIVERSITY OF WASHINGTON 29
Five Key Five Key Communication SkillsCommunication Skills
1. Framing communication messages
2. Understanding the patient perspective
3. Active listening
4. Redirecting
5. Cocktail Party

U NIVERSITY OF WASHINGTON 30U NIVERSITY OF WASHINGTON 30
Brief Intervention Brief Intervention Talking PointsTalking Points
(adapted from the Partnership for Health Program, PAETC, University of Southern
California)
• Compliment any protective behavior
• Ask a question/s about sexual behavior and disclosure
• Discuss sexual behavior and disclosure
U NIVERSITY OF WASHINGTON 31U NIVERSITY OF WASHINGTON 31
PwP Internet PwP Internet ResourcesResources
• www.aidspartnershipca.org/pfp.html• www.paetc.com/partnershipforhealth.
htmlPAETC, Partnership for Health Program
• www.aegis.com/pubs/woalive/2001/WO2001-0607.htmlPrevention with Positives: What Is It?
Women Alive, Summer 2001. Cathy Olufs.
• www.hivstopswithme.org
U NIVERSITY OF WASHINGTON 32U NIVERSITY OF WASHINGTON 32
PwP Internet ResourcesPwP Internet Resources
• www.omhrc.gov/OMH/aids/impact/HIV_march2002.pdfPrevention with Positives: Reducing
Further Transmission of HIV/AIDS.HIV Impact, March/April, 2002. Aimee Swartz.
• http://www.thebody.com/treat/prevpos.htmlArchived online articles
U NIVERSITY OF WASHINGTON 33U NIVERSITY OF WASHINGTON 33
Contact InformationContact Information
Robert T. Carroll, PhD (c), RN, ACRN
WA State Education CoordinatorNW AIDS Education & Training
Center901 Boren Ave., Suite 1100
UW Box #359932Seattle, WA 98104-3508