
Prevention of Syncope through Permanent Cardiac...
21
DOI: 10.1161/CIRCEP.112.975102 1 Prevention of Syncope through Permanent Cardiac Pacing in Patients with Bifascicular Block and Syncope of Unexplained Origin: The PRESS Study Running title: Santini et al.; Prevention of syncope using pacemaker Massimo Santini, MD 1 ; Antonio Castro, MD 2 ; Franco Giada, MD 3 ; Renato Ricci, MD 1 ; Giuseppe Inama, MD 4 ; Germano Gaggioli, MD 5 ; Leonardo Calò, MD 6 ; Serafino Orazi, MD 7 ; Miguel Viscusi, MD 8 ; Leandro Chiodi, MD 9 ; Angelo Bartoletti, MD 10 ; Giovanni Foglia- Manzillo, MD 11 ; Fabrizio Ammirati, MD 12 ; Maria Luisa Loricchio, MD 2 ; Claudio Pedrinazzi, MD 4 ; Federico Turreni, MD 2 ; Gianni Gasparini, MD 3 ; Francesco Accardi, MS 13 ; Giovanni Raciti, MS 13 ; Antonio Raviele, MD 3 1 Azienda Ospedaliera S. Filippo Neri; 2 Ospedale Sandro Pertini, Roma; 3 Ospedale Umberto I, Mestre; 4 Azienda Ospedaliera Ospedale Maggiore, Crema; 5 Azienda Ospedaliera Villa Scassi, Sampierdarena; 6 Policlinico Casilino, Roma; 7 Ospedale Civile G. De Lellis, Rieti; 8 Azienda Ospedaliera San Sebastiano, Caserta; 9 Ospedale Santa Maria Annunziata, Bagno a Ripoli; 10 Nuovo Ospedale S. Giovanni di Dio, Firenze; 11 Ospedale Valduce, Como; 12 Ospedale GB Grassi, Ostia; 13 Boston Scientific, Milano, Italy Corresponding author: Massimo Santini, MD Cardiovascular Department San Filippo Neri Hospital via G. Martinotti 20 00135 Roma, Italy Tel: +39 06 33062294 Fax: + 39 06 33062489 E-mail: [email protected] Journal Subject Code: [120] Pacemaker D ; Serafino Orazi zi, , M M M M MD D D D 10 10 10 10 ; ; ; ; Gi Gi Gi Giov ov ov ovan an an anni n n ni F Fog og og ogl li li li MD 2 ; ; Cl Cl Cl Clau au au audi di di dio o o o Pe Pe Pe Pedr dr dr drin i D e O a o s D 11 12 13 D 4 ; ; ; ; Fe Fe Fe Fed d deri ri ri r co co T T T Tu ur u u reni , MD 2 ; Gianni Gaspa a ari ini, MD 3 ; Fr r r ran a ce e e es sc s s o Accardi , MS 13 ; Gi Gi iov ov o ovan an an anni ni ni ni R R Rac c c cit it t ti, M MS 13 13 1 ; An n nto oni i i io o o Ra a a av vi v el l le e e, M M MD D D 3 Ospe e eda da da d li lier er e a a a S. S. S. F F Fil il ilip ip ip po po po N N Ner r r eri; i; i; i; 2 Ospe pe pe da da dale le le S S San n ndr dr dr d o o o Pe Pe Pert tin in ini, i i, R R Rom om oma; a a; 3 3 3 Os Os Ospe pe pe da da a dale le l le U U U Umb mb mber r rto to to I I I, , M e Ospe pe pe p da da da dal li l er er era a a Os Os Os O pe pe pe peda da da dale le le le M M Mag ag aggi gi gi ior o o e, , , C C C Cre re rema ma ma ma; ; ; 5 Az Az Azie ie ie i nd nd nd nda a a Os Os Os Ospe pe peda da da dali li l er e er e a a a Vi Vi Vi Vill ll ll l a a a a Sc Sc Sc cas as as assi si si si, Sa Sa Sa Samp mp mp ie ie ie ierda o o o Ca Ca Casi si sili li lino no no, Ro Ro Roma ma ma; ; ; 7 Os Os Ospe pe peda da dale le le C C Civ iv ivil il ile e e G G G. D D De e e Le Le Lell ll llis is is, Ri Ri Riet et eti; i; i; 8 Az Az Azie ie iend nd nda a a Os Os Ospe pe peda da dali li lier er era a a Sa Sa San n n Se Se Seba ba bas s s 9 Ospe dale e e e S S S San an an nta ta ta a M M M Mar ar ar aria ia a ia A A A An nn n un un un unzi zi zi z at at at a a, a a, a B B B Bag ag ag a no no no n a a a R R R Rip ip ip ipol o ol o i; i; i; i; 10 10 10 0 Nu Nu Nu Nuov ov ov ovo o o o Os Os Os Ospe pe pe peda da da ale le le e S S S S. Gi Gi Gi Gio o ov o anni di D 11 12 13 by guest on June 30, 2018 http://circep.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://circep.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://circep.ahajournals.org/ Downloaded from
Transcript of Prevention of Syncope through Permanent Cardiac...

DOI: 10.1161/CIRCEP.112.975102
1
Prevention of Syncope through Permanent Cardiac Pacing in Patients with
Bifascicular Block and Syncope of Unexplained Origin: The PRESS Study
Running title: Santini et al.; Prevention of syncope using pacemaker
Massimo Santini, MD1; Antonio Castro, MD2; Franco Giada, MD3; Renato Ricci, MD1;
Giuseppe Inama, MD4; Germano Gaggioli, MD5; Leonardo Calò, MD6; Serafino Orazi, MD7;
Miguel Viscusi, MD8; Leandro Chiodi, MD9; Angelo Bartoletti, MD10; Giovanni Foglia-
Manzillo, MD11; Fabrizio Ammirati, MD12; Maria Luisa Loricchio, MD2; Claudio Pedrinazzi,
MD4; Federico Turreni, MD2; Gianni Gasparini, MD3; Francesco Accardi, MS13;
Giovanni Raciti, MS13; Antonio Raviele, MD3
1Azienda Ospedaliera S. Filippo Neri; 2Ospedale Sandro Pertini, Roma; 3Ospedale Umberto I, Mestre;4Azienda Ospedaliera Ospedale Maggiore, Crema; 5Azienda Ospedaliera Villa Scassi, Sampierdarena;
6Policlinico Casilino, Roma; 7Ospedale Civile G. De Lellis, Rieti; 8Azienda Ospedaliera San Sebastiano, Caserta; 9Ospedale Santa Maria Annunziata, Bagno a Ripoli; 10Nuovo Ospedale S. Giovanni di Dio, Firenze; 11Ospedale Valduce, Como; 12Ospedale GB Grassi, Ostia; 13Boston Scientific, Milano, Italy
Corresponding author:
Massimo Santini, MD
Cardiovascular Department
San Filippo Neri Hospital
via G. Martinotti 20
00135 Roma, Italy
Tel: +39 06 33062294
Fax: + 39 06 33062489
E-mail: [email protected]
Journal Subject Code: [120] Pacemaker
D ; Serafino Orazizi, , ,, M
MMMMDDDD10101010;;;; GiGiGiGiovovovovananananninnni FFogogogogllilili
MD2;; ClClClClauauauaudidididio o o o PePePePedrdrdrdrini
D
eO ao s
D11 12 13
D4;;;; FeFeFeFeddderiririr coco TTTTuuruu reni, MD2; Gianni Gaspaaariini, MD3; Frrrrana ceeeesscss o Accardi, MS13;
GiGiiovovoovanananannininini RRRaccccitittti, MMS13131 ; Annntooniiiio oo Raaaavviv ellleee, MMMDDD3
Ospeeedadadad lilierere aaa S.S.S. FFFilililipipipppopopop NNNerrreri;i;i;i; 2Ospepepep dadadalelele SSSannndrdrdrd ooo PePePerttininini,ii, RRRomomoma;aa; 333OsOsOspepepep dadaadalelelle UUUUmbmbmberrrtototo III,, MeOspepepep dadadadallil ererera aa OsOsOsO pepepepedadadadalelelele MMMagagaggigigiioroo e,,, CCCCrereremamamama;;; 5AzAzAzieieiei ndndndnda aa OsOsOsOspepepedadadadalilil ereere a aa ViViViVilllllll a aaa ScScSccasasasassisisisi, SaSaSaSampmpmppieieieierdaooo CaCaCasisisilililinonono, RoRoRomamama;;; 7OsOsOspepepedadadalelele CCCivivivililileee GGG. DDDeee LeLeLellllllisisis, RiRiRieteteti;i;i; 8AzAzAzieieiendndndaaa OsOsOspepepedadadalililierereraaa SaSaSannn SeSeSebababasss9Ospep daleeee SSSSanananntatataa MMMMarararariaiaaia AAAAnnnn ununununziziziz atatata a,aa,a BBBBagagaga nononon aaa RRRRipipipipoloolo i;i;i;i; 1010100NuNuNuNuovovovovoooo OsOsOsOspepepepedadadaalelelee SSSS. GiGiGiGiooovo anni di D11 12 13
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
2
Abstract:
Background - Syncope in patients with bifascicular block (BFB) is a common event whose
causes might be difficult to assess.
Methods and Results - PRESS is a multicenter, prospective, randomized, single blinded study
designed to demonstrate a reduction in symptomatic events in patients with BFB and syncope of
undetermined origin implanted with permanent pacemaker. Device programming at DDD with a
lower rate of 60 ppm is compared to backup pacing at DDI with a lower rate of 30 ppm. The
endpoint consisted of: 1) syncope; 2) symptomatic pre-syncopal episodes associated with a
device intervention (ventricular pacing); 3) symptomatic episodes associated with intermittent or
permanent atrio-ventricular block (any degree). 101 patients were enrolled and randomized.
Primary endpoint events at two years were observed in 23 patients, with a significant lower
incidence in the study group (HR: 0.32; 95% CI: 0.10 – 0.96; p=0.042). Reduction of any
symptoms, associated or not with device intervention, was superior in DDD60 compared to
DDI30 (HR: 0.4; 95% CI: 0.25 – 0.78; p=0.0053). Fourteen patients developed other rhythm
diseases and met class I indication for pacing. The annual incidence of rhythm disease
development was 7.4%.
Conclusions - In patients with BFB and syncope of undetermined origin, the use of a dual
chamber pacemaker programmed to DDD60 led to a significant reduction of syncope or
symptomatic events associated with a cardio-inhibitory origin, compared to DDI30
programming. Symptoms associated with a new onset of rhythm disease were found in 15% of
the population at 2 years.
Clinical Trial Registration Information – clinicaltrials.gov; Identifier: NCT01463358.
Key words: pacemakers; syncope; Bifascicular Block; randomized controlled trial
oooolllllllledededed aaaandndndnd rrrranananandodododomimimimizezezz dddd
th a ssigigigigninininifififif cacacacantntntn lololooweweww r
n
associated or not with device intervention, was superior in DDD60 compared to
R h
n
e
n p y p g ,
n tttthehehe sstututudydydydy grororoouupuu (HR: 0.32; 95% CI: 0.101010 – 0.96; p=000.042222))). Reduction of any
aaasa sssociated ooorrr nnot tt wiwiwiwithththt ddddevee icicicce e e e inininnteervenenntion,, wawawaw sss susuuuppep rirr ooor iiiin nn DDDDDDD6D6D6D60000 cocococ mpmpmpararara ededede to
R: ::: 0.00.0 4;44 95%%%% CI: 0.22255 – 00.0 77787 ; pppp=0000..0. 0555333). FoFourrrrttteeeeennn n papap tiieeene ts deeeveelee ooopo edddd ooothheer rhyhyhyth
nd meemeet tt class sss I indididicacacation ffffor pacing.gg TTTTheeee aaannnnnnn ual ininincidence ofoo rhyyyththhthm diddd sease
nt was 77.7 4%4%4%.
nnss - InIn ppatatattieiei nttnts s wiwiithththth BFBFBFBFBBB anand dd d syssyncncoppopee ofoff uundnddetteterermimimiminened dd d ororigigi inini , , tttthehehh uusese oof f a a dudualal by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.112.975102
3
Introduction
Bifascicular block (BFB) is a conduction disturbance with reported prevalence of 1–1.5%, with
up to 25% of adult patients presenting with syncope1-6. The cause of syncope in these patients is
difficult to assess and may be due in part to transitory conduction disturbances at the pre-sinus,
sinus, or atrio-ventricular node level6-8. These patients may also present with ventricular
tachycardia9,10. Patients with BFB and syncope represent a heterogeneous population which is
difficult to stratify and where the selection of an appropriate therapy may be challenging6, 11-14.
Different techniques are used in clinical practice to investigate the cause underlying
syncope, including either invasive (Electrophysiological study) or noninvasive (ECG, Holter
monitoring, Tilt Table Test). These methods, despite useful in identifying specific causes often
lack in specificity10, 13,14-18. Therefore, the current evidence led the ACC-AHA-HRS committee
to consider permanent pacemaker implantation as a class IIA indication for BFB patients
presenting with syncope of undetermined origin11,12,19. However, the guidelines do not state
which pacing modality should be chosen for these patients (single vs dual chamber). Limited
information is available on the recurrences of syncopal episodes, hospitalizations and quality of
life for these patients after pacemaker implantation. The PRESS study (PREvention of Syncope
through permanent cardiac pacing in patients with bifaScicular block) was designed to
investigate the role of pacemaker in preventing symptom recurrences in patients with bifascicular
block and history of syncope of unknown origin.
Methods
PRESS (study registration: NCT01463358) is a multicenter, prospective, randomized, single-
blinded study designed to investigate the role of pacemakers in reducing symptoms recurrences
in patients with bifascicular block who experienced syncope, whose origin was undetermined in
the cause underlylyyyinininingg
ninvaasiisiiveve ((((ECECECECG,GGG, HHHHololololtete
g o
c
r
e
ng modalit sho ld be chosen for these patients (single s d al chamber) Limite
g, TiTiTiltltltlt TTTabababablelelele TTTesesesest). These methods, despiiiitetete uuseful in ideeentifffyiyiying specific causes oa
ccccififififiiici ity10, 13,14-188. Thhheerefffororre, tttthheheh cccuurreenttt evviddencnnce e e e lllel dd thhheee ACCCC-AHAHAHAHA-HRHRHRH SS commmmmm
r permmmmannananeent pacemakkkker immmmplplplplantatititiononono aaas a llclass s IIIIIIIIAAA A inininindididid cacacac tititit on for BBBBFBFBFBFB p ttatiiienttts
withh h syyyncopppe ee ofofofof u ddndeter imiiined ddd origigigiinii 11,11122,2 19199. HHoH wever, tttthheheh ggguiuiuiuideddd lililines doddd nnnnotototo sstate
dod lalitit hsh ldld bb hch ff tthhe tatiie tnt ((siin lgl dd ll hch bbe )r) LiLi imitte
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
4
nature after screening for causes with the currently indicated diagnostic techniques. The
objective of the study was to demonstrate that permanent dual chamber (DDD) pacing is
effective in reducing the recurrence of symptoms including syncope or pre-syncopal episodes
associated with a cardio-inhibitory origin (including symptomatic temporary or permanent atrio-
ventricular block). The study was approved by the institutional Ethics Committee of the
participating centers.
All patients enrolled into the study were implanted with a dual chamber pacemaker
(InsigniaTM, Boston Scientific Corporation) and randomized to two parallel arms. The treatment
arm included devices programmed to DDD pacing mode with a 60 ppm lower rate and AV
interval 200 msec (DDD60). The control arm included those programmed with to DDI mode
and 30 ppm lower rate (DDI30). Device programming in the control arm was aimed at
minimizing pacing as much as possible, while providing a safety backup stimulation. The
primary endpoint of the study was to demonstrate at two years after implant a reduction in the
treatment group of the following composite: 1) syncopal episodes of any origin; 2) symptomatic
pre-syncopal episodes (including dizziness, and near-syncope without loss of consciousness)
associated with a documented device intervention (ventricular pacing) and 3) symptomatic
episodes associated with documented episodes of intermittent, or permanent atrio-ventricular
block (any degree) or to sustained ventricular tachycardia. Pre-syncopal episodes with symptoms
and without loss of consciousness were included as primary endpoints only if associated either
with a documented bradycardia at ECG or with consistent ventricular pacing >1% detected by
pacemaker diagnostics. Other symptoms were classified as primary endpoint only in the presence
of documented evidence of AV block of any degree.
Secondary endpoint included: 1) comparison of each of the three separate components of
rallel arms. The trtrrreaeaeaeatmt
m lowowerer rrattatte e anand d AVAVAVAV
o
m
g
t
f h f ll i i 1) l i d f i i 2)
00000 msmsmsmsecec ((((DDDD D6DDD 0). The control arm inclllludududded those proooogrammmmmed with to DDI mo
mmmm looowo er rate (DDDDI30330). DDDeeevice prrroggrammmm inngg in tttthehehehe cconnntrrrol aarmm wwwas aiiaiimmem d at
g pacicicing as mu hhch as possibibblle, whilille prppp ovididining a safffety bbbackkup stimimimulululatioii n. ThTThe
dpppoint of the ssstudy yy was to demonstrate at two yeyy ars afteteeer impmpmplant a reducccctitititiononon in tr
f h f ll i i 1) l i d f i i 2)
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
5
the primary endpoint in the two study groups; 2) comparison of symptomatic episodes of any
origin between the two study groups; 3) rhythm disease progression in the entire cohort of
patients (AV block, bradycardia, atrial fibrillation); 4) comparison of documented atrial
fibrillation in the two study groups; 5) recurrence of symptoms after device reprogramming from
DDI30 to DDD60. This study included patients with BFB and a history of syncope of unknown
origin, currently indicated to permanent pacing according to ACC-AHA-HRS guidelines (class
IIA). Subjects were eligible to participate in the study if they met the following inclusion criteria:
ECG documentation of BFB defined as complete Left Bundle Branch Block or complete Right
Bundle Branch Block associated with Left Anterior Hemiblock or Left Posterior Hemiblock with
at least 1 episode of syncope in a period of 6 months preceding enrollment. All eligible patients
underwent complete laboratory screening including ECG, Holter monitoring, tilt test, carotid
sinus massage, EP study, to rule out any possible preexisting cause of syncope. Patients were
excluded if the cause of syncope was identified among the following: 1) vasovagal syncope; 2)
carotid sinus syndrome; 3) persistent or permanent atrial fibrillation 3) sinus node dysfunction or
Brady-Tachy syndrome; 4) 2nd or 3rd degree atrio-ventricular block (AVB), diagnosed at ECG or
during EP study; 5) spontaneous or inducible sustained ventricular tachycardia; 6) minimal
nocturnal heart rate inferior to 35 bpm documented at Holter monitoring. Patients with
significant structural heart disease (EF <40%) were also excluded. Detailed description for the
diagnostic examinations to assess these criteria are detailed in appendix.
After signing informed consent, patients underwent dual chamber pacemaker
implantation; randomization occurred at patient discharge post implant (block randomization
with block size = 4 allocation, ratio 1:1). Medical therapy was prescribed according to physician
discretion. The use of Beta blockers was not recommended during the course of the study unless
Block or complp ette e e e RRRR
ft Poststttererioiiior r HHHeHemimiblblblblooocockk
pisode of syncope in a period of 6 months preceding enrollment. All eligible pat
complete laboratory screening including ECG, Holter monitoring, tilt test, carot
a e
f e
s s ndrome; 3) persistent or permanent atrial fibrillation 3) sin s node d sf nct
pisosososodededed oof fff syssynccccoopoo e in a period of 6 monthhhhsss ppreceding ennnrolllllmmemm nt. All eligible pat
cccoc mmmpm lete labororatooryy screrereeninnng iniinccluddiiing EECG,GG,G HHHHollterrr mmmonnittoririririnng, tiiiltltll teestt, caararot
age, EEEEPPP stststs dudy, ttto rulllle outtt aaaannny possssisisis blbblble prpreexistststininining g ccccaususseeee offf syncoopepepepe. Patititientstt we
f the cause ofofof ssssynyy copepp was iiidenttifififieii dddd amonggg ttheh ffff llollowiwiwiwingngg: 1)1)1)) vasovagggalll ssssynynyny cccoc peppddd
dnd 3)3) isi tst tt tnt ttriiall fifibbrililllatiti 33)) isi dde dd ff tt
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.112.975102
6
needed for other reasons. Amiodarone or other antiarrhythmic drugs were not discontinued
during the study.
Each enrolled patient was followed for two years after enrollment with standard in-clinic
visit programmed at one month and every 3 months after randomization.
Both pacing mode and lower rate stimulation were required to remain unchanged unless
specific symptomatic episodes occurred and the endpoint reached. Primary endpoint analysis was
completed according to an “intention-to-treat” protocol with respect to device programming. In
the case of device reprogramming after the occurrence of the primary endpoint, recurrences of
episodes in the remaining follow-up period were also collected. At the end of the follow-up
period, for each patient, the pacing mode and rate could be programmed at physician’s
discretion.
Sample size and statistical analysis
The PRESS study was designed to demonstrate an absolute reduction of at least 20% of events
between the study group and the control group, assuming 30% of events in the control group at 2
years. Aiming at alpha of 0.05, a 80% power and a 10% attrition per year, the study required a
sample size of 101 patients. Descriptive statistics are used to describe collected data: absolute
numbers and proportions for discrete data; mean, standard deviation, median and quartiles for
continuous data, according to distribution. Primary and secondary endpoints were analyzed with
a survival analysis techniques and the Kaplan-Meier method. Log-rank test was also used to
analyze the primary endpoint. Additionally, Cox model with robust standard errors was used to
analyze both primary and secondary endpoints to account for intra site correlation.
Results
A total of 101 patients were enrolled in the study and randomized (52 to DDD60 group, 49 to
endpop int,, recurreencncncnceese
e end ddd offfof ttthhehhe ffff llolollololl w-w-w-w-uuupup
S study was designed to demonstrate an absolute reduction of at least 20% of eve
e st d gro p and the control gro p ass ming 30% of e ents in the control gro
eaaaachchhch pppattatieieieientnn , thththhe pacing mode and rate cccououo ld be prograaammmmmeeed at physician’s
e anddd d sttstatatatatiiistiiiicalll an lllalysis
S st duddy yy was dededeesiiiigngg dedd to dded monstrate an abbbsolllutte redudd ctctttiioioi n ofofoff att lell ast 20202020% %%% ofofoff eve
tst dd dd thth tnt ll iin 3030%% fof tnt iin tthhe ttr lol
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.112.975102
7
DDI30) from March 2005 to February 2009. Patient characteristics are shown in table 1. During
the two years-follow-up, two patients withdrew from the study, 3 were lost to follow up, and 4
died before the end of follow up (causes of death: 1 undetermined during sleep; 1 cerebral
hemorrhage; 1 respiratory failure in patient with COPD ; 1 myocardial infarction), yielding to a
total of 93 patients at the end of the follow up period.
The composite primary endpoint occurred in 23 patients (22.8%) at two years with
median time to event of 5.4 months, of which 16 (32.6%) in the DDI30 group and 7 (13.5%) in
DDD60 group (HR: 0.32 [0.10 - 0.96], P=0.042). Kaplan-Meier curves (figure 1) showed a
significant reduction of events in the treatment group (with a NNT=5.23). The first event
occurred in these 23 patients was syncope in 14 (13.9%), pre-syncope in 6 (5.9%) and AV block
in 3 (3%) patients. Additionally, the proportion of patients presenting with syncope, pre-syncope
and AV block alone, considered as independent events, were compared in the two study groups
(table 2), indicating that a significant difference is still preserved between the DDD60 and
DDI30 for pre-syncope and AV block events separately but not for syncope alone.
A total of 19 syncopal episodes occurred in 14 patients, with 5 patients having a second
episode (3 randomized in the control and 2 in the treatment arm). The total number of pre-
syncopal episodes due to a documented cardio-inhibition was 34 in 22 patients (21.8%): 9
patients had recurrences after the first episode with 6 patients having one recurrence and 3
patients with two recurrences. All patients with pre-syncope recurrences were originally
programmed in the DDI30 (control group). Reprogramming of pacing mode from DDI30 to
DDD60 occurred in 15 patients following the first event of syncope or pre-syncope. In 13 of
these cases the event has been adjudicated as primary endpoint. Among the 9 patients originally
programmed at DDI30 and with recurrent pre-syncope, only 2 had the device reprogrammed to
s ((figug re 1) ) showweeeed d d d aa
23). ThThThThe e fifififirsrsttt t evevennnntt t t
n these 23 patients was syncope in 14 (13.9%), pre-syncope in 6 (5.9%) and AV b
p y
ock alone, considered as independent events, were compared in the two study gro
n
pre s ncope and AV block e ents separatel b t not for s ncope alone
n thhhesesesesee ee 232333 pppatieieienntnn s was syncope in 14 (13.3.3.9%99 ), pre-syncocc peeee iiin 6 (5.9%) and AV
paaaatiiiients. Addittioonaallyy, thhheee propoporrrtiion ooof paattiennntstss ppppreeseeenttting wwithththh syncncnccoopo e,e, preee---sy
ock aalolololoneenene, considididder ddded as inininindeddedependndndndenenene t tt eventtts, weweweweree ccccommmpapapap reddd iniii tthehehehe tttwo stttudydd gro
ndicatiini g gg thhhatatat aaaa sigigigi niiifififica tnt dddifffefff rence is s iitillll pppreservedddd bbbbetweeeeeene thehh DDDDDDDDDDDD60606060 aaaand
dnd AAVV blbl kk tts tat lel bb tt tt ffo lal
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
8
DDD60 after the first episode.
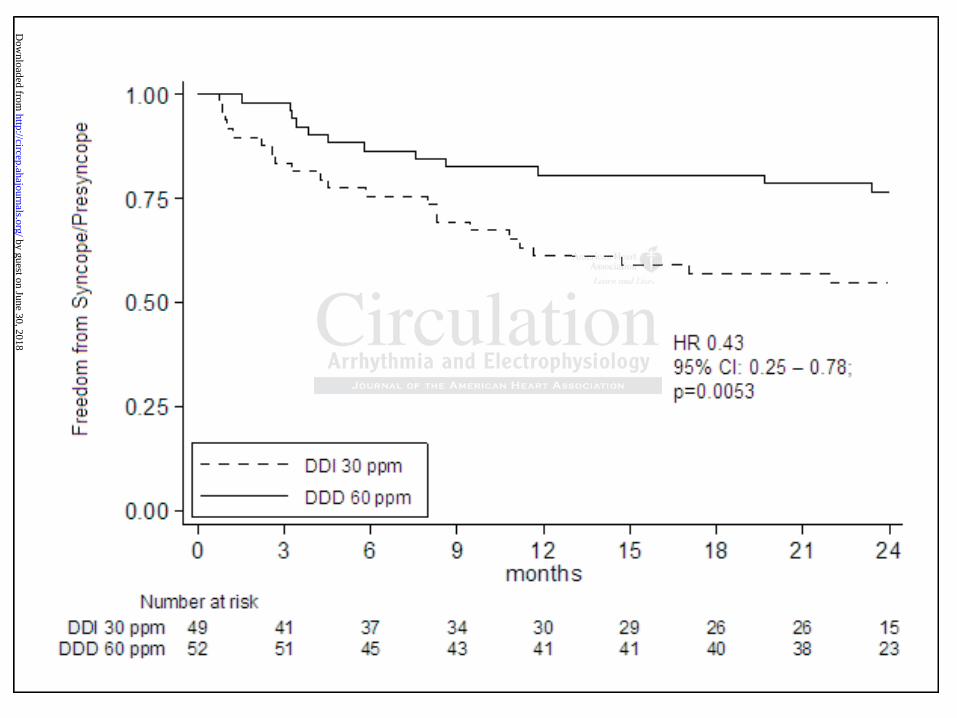
Overall, a symptomatic episode (syncope or pre-syncope), regardless of its origin,
occurred in 35 patients (34.6%) of which 22 (44.9%) in the control (DDI30) group and 13 (25%)
in the treatment (DDD60) group (HR: 0.43 [0.25 - 0.78], P=0.0053). Kaplan-Meier curve (Figure
2) showed a significant reduction in the event rates in the treatment group.
14 patients developed a Class I indication for permanent pacing during the course of the
study (10 symptomatic AV block, 2 Brady-Tachy, 1 sinus bradycardia, 1 permanent AF with
slow ventricular response), accounting for an overall incidence of 7.4% per year of new class I
indication for permanent pacing (the most prevalent being AV block, with 5.38%). With regard
to the 10 patients who showed a complete AV block during the follow-up, 8 of them were in the
control group (16.3%) and 2 (3.8%) in the treatment group. Fourteen patients had at least one
hospitalization for symptomatic Heart Failure, associated or not with AV block, yielding an
annual incidence of 3.7%. In DDD60 group median pacing rate was: 26% for atrium (IQR: 1%-
48%) and 23% for ventricle (IQR:1%-35%). 10 patients (9.9%) had a history of paroxysmal AF
before implant. During follow up, a total of 44 episodes of atrial fibrillation were retrieved in
26/101 patients. Episodes were retrieved either at ECG or from implanted device diagnostics
Among the 26 patients with atrial fibrillation, 7 were patients with documented pre-implant atrial
fibrillation history and 19 were patients with new onset, post-implant, atrial fibrillation episodes.
The total annual incidence of atrial fibrillation in this sample was 13.1%. None of these patients
presented with ventricular tachycardia during the course of the follow up.
Discussion
Bifasicular block, defined as complete Left Bundle Branch Block or complete Right Bundle
% pep r yey ar of new w clclclclaa
with hhh 5555.38383838%)%)%)%). WiWiWiWithththth rre
atients who showed a complete AV block during the follow-up, 8 of them were i
oup 6.3% and 2 .8 in the treatment group. Fourteen patients had at least o
tion for symptomatic Heart Failure, associated or not with AV block, yielding an
idence of 3.7%. In DDD60 group median pacing rate was: 26% for atrium (IQR:
23% for entricle (IQR:1% 35%) 10 patients (9 9%) had a histor of paro sma
atienenenentsttst wwwhohohoho shohohowed a complete AV bloccck kkk dud ring the foloo low-w-w-w up, 8 of them were i
ouuuup (16.3%) anndd 2 (3(3(3.8%)%)%)) in ththththe trreatmmmentt ggrouuup.p.p.p FFFFoourrrteeeen paatieneents hhhadadada aat leaasttt t o
tion fofofoforrr ssssympmptttomatititic Hearararrttt FFFFailururrreee,e aaassociiiattett d ddd oooor nnnnoooot wwwwitititi h hhh AVAVAVV bbblolololockckckck, yiiiiellldddid ng an
idence of ff 3.33 7%7%7%%. InIII DDDDDDDDD6060600 gggrouppp m deddian papp iicinggg rate wawaaas: 2226%6%6%6% fffor atriuii m mmm (I(I(I( QRQRQRQ :
223%3% ff ttriiclle ((IQIQRR:1%1% 3535%)%) 1100 titi tts ((99 9%9%)) hhadd hihi tst ff a
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
9
Branch Block associated with Left Anterior Hemiblock or Left Posterior Hemiblock, is a
condition associated with increased mortality, whose mechanisms are not well understood6-8,20-22.
Syncope, associated or not with severe trauma or injuries, can be a frequent event in this
population. The underlying causes explaining loss of consciousness in bifascicular block
population are heterogeneous, the most frequent being neurally mediated syncope or intermittent
high degree atrio-ventricular (AV) block7,20,23,24. Additionally, several studies focusing on
follow-up of BFB patients with previous syncope reported consistent rates of temporary or
permanent AV block development over time8,11,25-28. Despite the high incidence of electric
disturbances of the conduction system, electro-physiological study (EPS) at the time of the
hospital observation has limited positive predictive value10, 14, 29,30. Accordingly, BFB patients
with both history of previous syncope and a negative EPS have been the subject of several
investigations involving pacemakers or loop recorders in order to identify the nature of
associated syncopal recurrences and consequently its most appropriate treatment5, 24, 27, 31, 32.
Current guidelines set in the last 10 years a class IIA recommendation for a pacemaker
implantation in patients with BFB and experiencing syncope of apparently unexplained origin; to
avoid the risk of syncopal recurrences and potential physical trauma19. The PRESS study was
designed to assess the role of dual chamber pacing in preventing symptom recurrences in these
patients and demonstrated that the use of a pacemaker programmed with a lower rate of 60 ppm
(DDD60) resulted in a significant reduction of the combination of symptomatic events including
syncope, pre-syncope or AV block when compared to a substantially negligible electrical
treatment. Indeed, the programming to DDI-30 bpm of the control group patients was chosen in
order to avoid as much as possible any paced beat, considering that the Holter screening criteria
before implant included only patients with a spontaneous heart rate always higher than 30 bpm
incidence of electrtrtrricicicic
PS) atattt ttthehehh ttttiimimi e e ofofff tttthehehehe
b 10 14 29 30 e
h
o
2
idelines set in the last 10 ears a class IIA recommendation for a pacemaker
bserrrrvavavavatititiiononnn hhhhas lililiimited positive predictiveee vvvala ue10, 14, 29,30. Accccccocc rdingly, BFB patie
hiiiisttttory of prevvioous syncccopopope anand a negagaativee EPSPSPSPS hhhavaava e bebebeen tthhe sssuubu jectctctt ooof f seveeeraaal
ons iiinvnnvnvolollolvingng pacemakers ororor loop pp rererer cocco ddrdders inn oooo drdrdderererer to o idididi entititiifyfff ththhtheee nnature of fff
synyy copapp lll recuuurrrrr ences and dd conseqqque tntlyyy iiits mostt apppppproprprprriiatetete ttttre tatment5,55 2224,4,4,4 22227,7,7, 33331, 32
idid leliin tet ii thth lla tst 1100 lcl IIIIAA ddatiti ff kak
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.112.975102
10
during the 24 hours. The beneficial effect of permanent pacing is more striking if we consider the
rigid selection process that patients had undergone to be considered eligible for the study, ruling
out any evident rhythm disease at the time of enrollment. Despite this precise pre-selection of
patients, symptoms associated with new onset of a rhythm disease including AV block, brady-
tachy or bradycardias or chronic atrial fibrillation with slow ventricular response, with class I
indications for pacemaker implant emerged in up to 15% of the study population.
Notably, by analyzing the components of the primary endpoint, a significant difference
between the study group and controls is shown only with respect to pre-syncope and to
symptoms associated with AV block, but not to syncope alone, which did not show any
significant difference between DDD60 and DDI30. This result may be explained by the
mechanisms of syncope occurring in this selected BFB population when implanted with a
permanent pacemaker. Having device diagnostics that excluded ventricular arrhythmias and a
pacemaker that warranted the presence of adequate pacing in both groups to prevent a cardio-
inhibitory episode, syncope events that occurred in this sample were likely due to vasodepressor
syndrome, hypotension from non-cardiac etiology (e.g., excessive medications/postural
orthostasis) or a neurological issue not detected with the pre-enrollment tilt test screening.
Additionally, it is reasonable to hypothesize that patient with cardio-inhibitory episodes have
turned into most of the pre-syncope symptoms, especially in the control group. Additionally, the
fact that these syncopal recurrences occurred in patients implanted with pacemaker regardless of
device programming, rule out the possible placebo effect of pacing, as hypothesized in previous
studies 33. However, it should be noted that the study was not powered to separately evaluate
individual endpoint events.
PRESS is the first randomized study for a BFB population involving a very strict
e-syny copep and to
did nn totot sshhhohoww anany y y
m
n
i
episode s ncope e ents that occ rred in this sample ere likel d e to asodep
difffffferererereneencececec bbbettttwweww en DDD60 and DDI300. ThThTT is result maaay bebebe explained by the
mssss oooof syncope occcuuurrring gg inninin thhhisisisi seellecteddd BFBFB pppopopopopuuulu aatiooonnn whehen imimimi plannnntetetedd wwithhh aaa
paceemamammakekekek r. HHHavinii g dddeviciciciceee ddddiagnonononostststicicics ththth tttat excxcxcxclluludedededed veveveventtt iiricular arararar hhhrhytttthmhh iai s an
that warrantedededd tthhheh pppresence offff added quqq ate papp ciiinggg iiin bobb thththth gggroupupupps to pppreventntntt aaa a cccac rdi
iis dod tts thth tat dd iin tthihi lle lilikkell dd tt dde
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.112.975102
11
selection and screening process. Specifically, diagnostic criteria used for the patients selection
(including ECG, Holter, TTT, and EPS) were used to exclude other possible causes for syncopal
episodes. The fact that a subgroup of these patients still presented with syncopal recurrences
within a short time after implant (median of 5 months) supports the prevailing belief that these
tests have limited predictive value. One of the most notable aspects of this study was the choice
to implant a permanent pacemaker in both arms of the study. This was done for several reasons.
The existence of class IIA indications in this population led to the choice to implant a pacemaker
rather than to randomize one group to no therapy or to a loop recorder implant. Additionally, as
this study was mainly focused on patient symptoms, a more uniform therapy to all patients was
a means to maintain patient blinding and thus to rule out a placebo effect on patient perceived
symptoms that could have biased the results.
Previous studies have documented the incidence and new onset of either cardiac events or
AV block in patients with BFB, as well as those BFB with negative EPS20-27. Despite a thorough
assessment of AV block development (especially those of transient nature) was not possible in
our study, a conservative estimate for development of a class IA indication for pacemaker,
mainly due to AV block, was found in 13% of patients, with the event occurring most likely
within a year from their enrollment. Differences in symptomatic AVB occurrence between the
two groups showed that AVB was mainly recognized in the DDD30 group: this is explained by
the fact that in the DDD60 group all blocks of transitory origin were not detected.
This study also demonstrated the potential value of pacemaker to prevent symptoms in a
population where the diagnostic chain to exclude current class IA pacemaker indication
(including EPS, tilt testing, Holter monitoring and Echo) is often burdensome to perform in
current practice. As noted in this study, despite the reliable determination of a bradyarrhyhtmia
impplant. Additiononnnalalaa l
therapappy y ttotot aallllllll ppppatattieieieiennntnt
v
v e
i
t of AV block de elopment (especiall those of transient nat re) as not possibl
maamamaininintaatainininn pppaatieieienntnn blinding and thus to ruuulelelele oout a placebo oo effffefefef ct on patient perceiv
tttht aaata could havvee biiiased tttthhehh resesullltss.
vioususss sstuututudddid es hhhave ddddocumememeenttntnted thehehehe iiiincnn ididddence aaandndndn nnnnew oooons ttet of eieiiiththththeer ca ddrdiaiii c eve
in papp tiiients wititithhh h BFBFBFB BB,B as w lelll as thhoh se BBBBFBFBFB wiiithhhh negggattivvvve EPEPEPSSSS2020200-272727. DDeDD spppitititite eee a aaa tho
tt ff AVAV bbllo kck dd lel tnt ((e iiallll thth fof tt iie tnt tat )e) tot isiblbl
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.112.975102
12
and its origin can be difficult in these patients, an annual incidence of 7.4% of indications for
pacing together with a clinically significant reduction of symptomatic episode with a dual
chamber pacemaker, suggests that in a patient with a compelling history of sudden syncope
empiric pacing therapy could be appropriate. This could be also supported by the consideration
that, the mean age of this population (75 yrs), together with prevalence of AF (25% in this
group), would lead to requiring the use of AA drugs that contribute to the deterioration of
intraventricular conduction in BFB patients
Although sustained high-rate ventricular tachyarrhythmias can also be the cause of
syncope in patients with BFB, in none of our cases a repetitive ventricular tachycardia has been
detected by the device which is provided by a special algorithm for arrhythmia detection and
storage. This result may be explained by careful selection of the patient population with
exclusion of patients with significant structural heart disease and a consequent mean left
ventricular ejection fraction of 57 ±10.
Limitations
The main limitations of the present study are related to specific choices made in the design. The
endpoint was driven by patient symptoms, with no possibility to accurately assess cardiac rhythm
disease development, especially when related to transient episodes of atrio-ventricular block.
Accordingly, using only pacemaker diagnostics to detect occurrence of a block allowed us to
detect only a conservative estimate for assessing the AV block development in this population.
Additionally, the study was single blinded and a registry of patients excluded (i.e. positive to any
of the screening test) was not kept.
Conclusion
The present study demonstrated that the use of dual chamber permanent pacing (DDD 60) in
also be the causee ofofofo
ular tttacachyhhhycaca ddrdrdiaiaii hhhhaaasas bb
y the device which is provided by a special algorithm for arrhythmia detection an
h
o
y thhhe e e e dedededevivivivicecece wwwhihihih ch is provided by a speccciaiaiaiall ll algorithm fofoor arrrrrhrhrhythmia detection an
hiiisi rrrresult may bee expxxplainnneedee bbby y caaarrefuul sseleecctioonn n ofofoff ttthe ppatientt popopoppup latittt oono wwithhh
of patatatatieieienttntnts wiiiiththth siiigngnifififificantttt stststs ructurururrallalal hhhhea ttrt ddddisiii eaeaeaease aaaa ddndd aaaa consequenenenentttt mean lelll ftftfft
ejjjectiiion fffractctctiioioi n ffof 555777 ±1±1100.00
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
13
BFB patients with syncope of undiagnosed origins after diagnostic screening, results in a
significant reduction of the combination of syncope/pre-syncopal episodes or other symptomatic
episode of cardio-inhibitory origin. Although further randomized studies would be necessary to
address some of the remaining questions on the nature of event recurrences in this population,
this study suggests that the use of a dual chamber pacemaker in this patient population might be
considered as a means for prevention of symptomatic event recurrences.
Funding Sources: The PRESS study has been sponsored by Boston Scientific Corporation.
Conflict of Interest Disclosures: F. Accardi and G. Raciti are Boston Scientific employee.
References:
1. Scheinman MM, Peters RW, Morady F, Sauve MJ, Malone P, Modin G. Electrophysiologic studies in patients with bundle branch block. Pacing Clin Electrophysiol. 1983;6:1157–1165.
2. Schneider JF, Thomas HE Jr, Kreger BE, McNamara PM, Kannel WB. Newly acquired left bundle-branch block: the Framingham study. Ann Intern Med. 1979;90:303–310.
3. McAnulty JH, Rahimtoola SH. Bundle branch block. Prog Cardiovasc Dis. 1984; 26: 333–354.
4. Scheinman MM, Peters RW, Suave MJ, Desai J, Abbott JA, Cogan J, Wohl B, Williams K. Value of the H-Q interval in patients with bundle branch block and the role of prophylactic permanent pacing. Am J Cardiol. 1982;50:1316–1322.
5. Brignole M, Menozzi C, Moya A, Garcia-Civera R, Mont L, Alvarez M, Errazquin F, Beiras J, Bottoni N, Donateo P. International Study on Syncope of Uncertain Etiology (ISSUE) Investigators: Mechanism of syncope in patients with bundle branch block and negative electrophysiological test. Circulation. 2001;104:2045–2050.
6. McAnulty JH, Rahimtoola SH, Murphy E, DeMots H, Ritzmann L, Kanarek PE, Kauffman S. Natural History of “HIGH RISK” Bundle-Branch-Block. N Engl J Med. 1982;307:137-143.
7. Dhingra RC, Denes P, Wu D, Chuquimia R, Amat-y-Leon F, Wyndham C, Rosen KM. Syncope in patients with chronic bifascicular block. Significance, causative mechanisms and clinical implications. Ann Intern Med. 1974;81:302-306.
8. De Pasquale NP, Bruno ME. Natural history of combined right bundle branch block and left
p
n Scieentnttifififificiiic ememplpplployoyyyeeeeee
s
m op 6
en
s:
maaaan MM, Peterrs RW,WW MMMorororo ady F, SSauvveee MMJ,, MaMaMalolololonenne P, MMModdinn G.G.G y Elecccctrropphhyssiooolopattieieieentntntssss wiwiwiwiththth bbbbununnndldldldle brbbb annnnchchch bbbblololockckckk. PaPaPaPacicicic ngngngn CCCClililiin nnn ElElElElecececectrtrtrt opopopophyhyhyyssis olololol. 1111989989 3;3;3;66:66 1111 575757–––1– 1611
er JFFJFJ , ThThThomomomasasas HHHHEE E E JrJrJr,,, KrKrKregeggegeere BBBBE,E,E, MMMMcNcNcNc amamama arararaa a a PPPPM,M,M,M, KKKananana nenenen lll WBWBWBB.... NeNeNeN wlwlwlw yyy acacaca quququq iriririred ncncnchh blblococock:k: ttthehe FFrararamimingngnghahammm stststududy.y.y. AnAnnnn InInteteternrnrn MMeded. 119797779;9;9 9090:3:30303 3–31010.
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
14
anterior hemiblock (bilateral bundle branch block). Am J Med. 1973;54: 297-303.
9. Peters RW, Scheinman MM, Modin C, O'Young J, Somelofski CA, Mies C. Prophylactic permanent pacemakers in chronic bundle brunch block. Circulation. 1979;66:978-985.
10. Ezri M, Lerman BB, Marchlinski FE, Buxton AE, Josephson ME. Electrophysiologic evaluation of syncope in patients with bifascicular block. Am Heart J. 1983;106:693-697.
11. Bergfeldt L, Edvardsson N, Rosenqvist M, Vallin H, Edhag O. Atrioventricular Block Progression in Patients with Bifascicular Block Assessed by Repeated Electrcardiography and a Bradycardia-Detecting Pacemaker. Am J Cardiol. 1994;74:1129-1132.
12. Scheinman MM, Peters RW, Suavé MJ, Desai J, Abbott JA, Cogan J, Wohl B, Williams K. Value of the H-Q Interval in Patients with Bundle Branch Block and the Role of Prophylactic Permanent Pacing. Am J Cardiol. 1982;50:1316-1322.
13. Rosen KM, Rahimtoola SH, Chuquimia R, Loeb HS, Gunnar RM. Electrophysiological Significance of the First Degree Atrioventricular Block with Intraventricular Conduction Disturbance. Circulation. 1971;43:491-502.
14. Kaul U, Dev V, Narula J, Malhotra AK, Talwar KK, Bhatia ML. Evaluation of Patients with Bundle Branch Block and “Unexplained” Syncope: A Study Based on Comprehensive Electrophysiologic Testing and Ajmaline Stress. Pacing Clin Electrophysiol.. 1988;11:289-297.
15. Englund A, Fredrikson M, Rosenqvist M. Head-up Tilt Test. Circulation. 1997;95: 951-954.
16. Sheldon R, Rose S,Koshman ML. Comparison of Patients with Syncope of Unknown Cause Having Negative or Positive Tilt-Table Test. Am J Card. 1997;80:581-585.
17. Sheldon R, Splawinski J, Killam S. Reproducibility of isoproterenol tilt-table tests in patients with syncope. Am J Cardiol. 1992;69:1300-1305.
18. Grubb BP, Wolfe D, Temesy-Armos P, Hahn H, Elliott L. Reproducibility of head upright tilt table test in patients with syncope. Pacing Clin Electrophysiol.1992;15:1477-1481.
19. Gregoratos G, Abrams J, Epstein AE, Freedman RA, Hayes DL, Hlatky MA, Kerber RE, Naccarelli GV, Schoenfeld MH, Silka MJ, Winters SL, Gibbons RJ, Antman EM, Alpert JS, Gregoratos G, Hiratzka LF, Faxon DP, Jacobs AK, Fuster V, Smith SC J. ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices: Summary Article. Circulation. 2002;106:2145-2161.
20. McAnulty JH, Rahimtoola SH, Murphy E, DeMots H, Ritzmann L, Kanarek PE, Kauffman S. Natural history of ‘highrisk’ bundle- N Engl J Med. 1982;307:137–143.
21. Dhingra RC, Palileo E, Strasberg B, Swiryn S, Bauernfeind RA, Wyndham CR, Rosen KM.
Elecctrtrtt opophyhyhh isisiiolllologogoggicicicicalalricularararar CCCConononondududuductctctctioioioionnnn
c
U say
n
n R Rose S Koshman ML Comparison of Patients ith S ncope of Unkno n C
e. CiCiCiCircrcrcr ululullatatata iionnn.... 1971;43:491-502.
U, DDDeD v V, Naruulaa J, MMMalhohohootra AKAKAKA , Talwlwwar KKK, BBBhahahahattia MLMM . EvEvalllluuationnnn ooof f PPatienenentsancncnch h h Block k kk annd “UUUnnexppplalalainii edddd”” SySySyncopopope: AA SSStututut dyyyy BBassseeede onn CoCooompmpmpm reheheheh nssivve ysiolllogogogogiciicic TTTTestititit ng andddd AAAjmmalalala iiinine Stttrerereresssss. PPPPa iicing CCCClililil n n EEElE eccccttrtrt ophhhysiololll.. 11198888888 1;111:11 28282828999
nd A,AAA FFFredrdd ikikiksososoon MMM,M RRRosenqvqq ist t MM.M HHHHead-ddd uppp TTTililillt TTTeT stt. CiCiCC rcululullaaata iiioi n. 19191997979797;99995:5:5:5 951
RR RR SS KKo hsh MLML CCo iis ff PPatiti tts itithh SS fof UU knk CC
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
15
Circulation.1981;64:1265–71.
22. Denes P, Dhingra RC, Wu D, Wyndham CR, Amat-y-Leon F, Rosen KM. Sudden death in patients with chronic bifascicular block. Arch Intern Med. 1977;137:1005–1010.
23. Moya A, Brignole M, Menozzi C, Garcia-Civera R, Tognarini S, Mont L, Botto G, Giada F,Cornacchia D. International Study on Syncope of Uncertain Etiology (ISSUE) Investigators.Mechanism of syncope in patients with isolated syncope and in patients with tilt-positive syncope. Circulation. 2001;104:1261-1267.
24. Brignole M, Sutton R, Menozzi C, Garcia-Civera R, Moya A, Wieling W, Andresen D, Benditt DG, Vardas P. International Study on Syncope of Uncertain Etiology 2 (ISSUE 2) Group. Early application of an implantable loop recorder allows effective specific therapy in patients with recurrent suspected neurally mediated syncope. Eur Heart J. 2006;27:1085-1092.
25. Tabrizi F, Rosenqvist M, Bergfeldt L, Englund A. Time relation between a syncopal event and documentation of atrioventricular block in patients with bifascicular block: clinical implications. Cardiology. 2007;108:138-143.
26. Martí-Almor J, Cladellas M, Bazán V, Delclós J, Altaba C, Guijo MA, Vila J, Mojal S, Bruguera J. Novel predictors of progression of atrioventricular block in patients with chronic bifascicular block. Rev Esp Cardiol. 2010;63:400-408.
27. Israel CW. Syncope and bifascicular block: who needs a pacemaker? Rev Esp Cardiol.2010;63:385-386.
28. Gaggioli G, Bottoni N, Brignole M. Progression to second and third-degree atrioventricular block in patients electrostimulated for bundle branch block: a long –term study. G Ital Cardiol.1994; 24:409-416.
29. Tabrizi F, Rosenqvist M, Bergfeldt L, Englund A. Long-term prognosis in patients with bifascicular block-the predictive value of noninvasive and invasive assessment. J Intern Med.2006;260:31-38.
30. Englund A, Bergfeldt L, Rehnqvist N, Astrom H, Rosenqvist M. Diagnostic value of programmed ventricular stimulation inpatients with bifascicular block: a prospective study of patients with and without syncope. J Am Coll Cardiol. 1995; 26:1508–1515.
31. Da Costa A, Gulian JL, Romeyer-Bouchard C, Messier M, Zarqane N, Samuel B, Khiel A, Isaaz K. Clinical predictors of cardiac events in patients with isolated syncope and negative electrophysiologic study. Int J Cardiol. 2006;109:28-33.
32. Brignole M. International study on syncope of uncertain aetiology 3 (ISSUE 3): pacemakertherapy for patients with asystolic neurally-mediated syncope: rationale and study design.Europace. 2007;9:25-30.
rt J. 2006;2; 7JJ :10885-5-5-5-101
etweeenen aa ssynyncocopapapallll eeevevlar blocococock:k:k:k: cccclilililininininicacacacallll
n
Almor J, Cladellas M, Bazán V, Delclós J, Altaba C, Gui MA, Vila J, M al S,. Novel edictors of ression of atrioventricular block in atients with chronr
C8
ns. CaCaCaCardrdrdr ioioioolololologyyyy... . 2007;108:138-143.
AAAAlmmmmor J, Cladeellas MMM, BBBaaazán VVVV, DDelcclóóós JJ, AAlttttabababa a a a CC, GGGuuuijo MMAAA,A Vilaa aa JJ,J MMojaaal S,. NoNoNovel prededede icctoors oof prrrogogogresssssioioioi nnn of aaatttrioveventtttriririculallal r bbbloooco k inn patatata ieiii ntsss s wiwiw thh chhhrooonr blockckckck. RReReR v EsEEE p CaCCC ddrdiollll. 2020202010;66663:3:3:3 4040404000-00 4040404 88.88
CW. SySySyncopppe aaana ddd d bibibifaff scicii ulllar bbbblllockkkk: hwhhho ne ddeds a papp ceemammm kekeker?r?r?r? RRReR v EEsEE ppp CaCaCaCardrdrdrdiol.85-386. by guest on June 30, 2018
http://circep.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCEP.112.975102
16
33. Raviele A, Giada F, Menozzi C, Speca G, Orazi S, Gasparini G, Sutton R, Brignole M. Vasovagal Syncope and Pacing Trial Investigators. Randomized, double-blind, placebo-controlled study of permanent cardiac pacing for the treatment of recurrent tilt-induced vasovagal syncope. The vasovagal syncope and pacing trial. Eur Heart J. 2004;25:1741-1748.
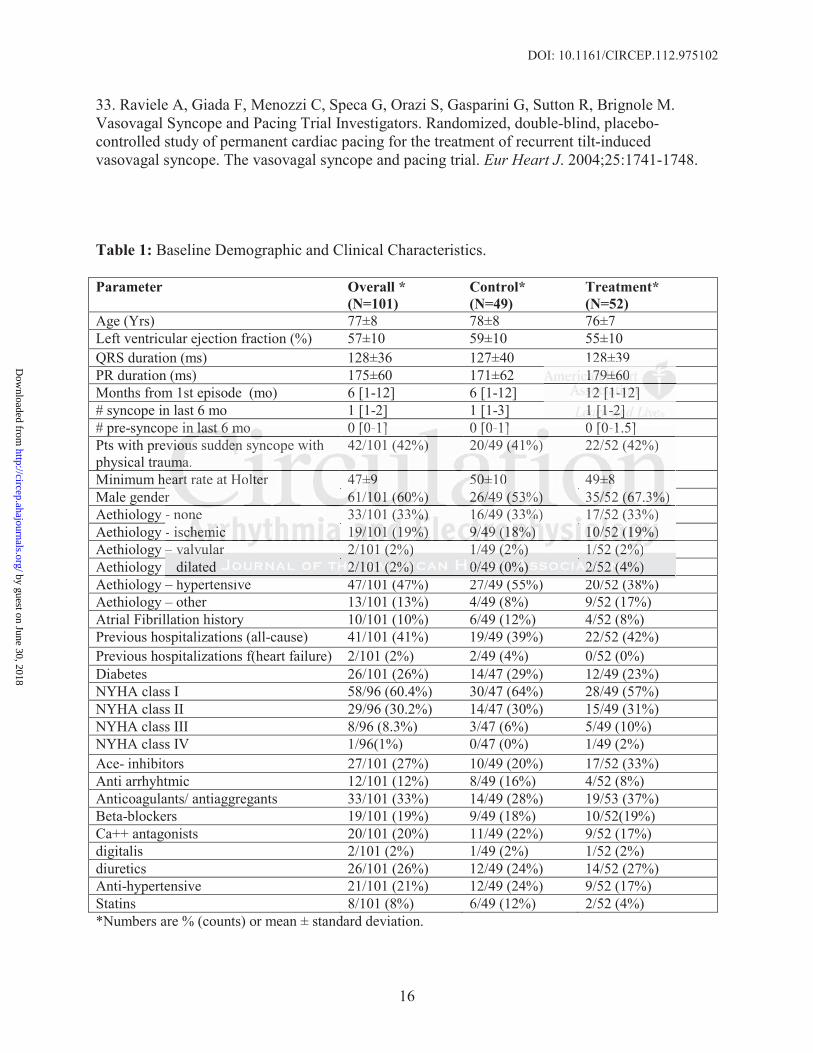
Table 1: Baseline Demographic and Clinical Characteristics.
Parameter Overall *(N=101)
Control*(N=49)
Treatment*(N=52)
Age (Yrs) 77±8 78±8 76±7Left ventricular ejection fraction (%) 57±10 59±10 55±10QRS duration (ms) 128±36 127±40 128±39PR duration (ms) 175±60 171±62 179±60Months from 1st episode (mo) 6 [1-12] 6 [1-12] 12 [1-12]# syncope in last 6 mo 1 [1-2] 1 [1-3] 1 [1-2]# pre-syncope in last 6 mo 0 [0-1] 0 [0-1] 0 [0-1.5]Pts with previous sudden syncope with physical trauma.
42/101 (42%) 20/49 (41%) 22/52 (42%)
Minimum heart rate at Holter 47±9 50±10 49±8Male gender 61/101 (60%) 26/49 (53%) 35/52 (67.3%)Aethiology - none 33/101 (33%) 16/49 (33%) 17/52 (33%)Aethiology - ischemic 19/101 (19%) 9/49 (18%) 10/52 (19%)Aethiology – valvular 2/101 (2%) 1/49 (2%) 1/52 (2%)Aethiology – dilated 2/101 (2%) 0/49 (0%) 2/52 (4%)Aethiology – hypertensive 47/101 (47%) 27/49 (55%) 20/52 (38%)Aethiology – other 13/101 (13%) 4/49 (8%) 9/52 (17%)Atrial Fibrillation history 10/101 (10%) 6/49 (12%) 4/52 (8%)Previous hospitalizations (all-cause) 41/101 (41%) 19/49 (39%) 22/52 (42%)Previous hospitalizations f(heart failure) 2/101 (2%) 2/49 (4%) 0/52 (0%)Diabetes 26/101 (26%) 14/47 (29%) 12/49 (23%)NYHA class I 58/96 (60.4%) 30/47 (64%) 28/49 (57%)NYHA class II 29/96 (30.2%) 14/47 (30%) 15/49 (31%)NYHA class III 8/96 (8.3%) 3/47 (6%) 5/49 (10%)NYHA class IV 1/96(1%) 0/47 (0%) 1/49 (2%)Ace- inhibitors 27/101 (27%) 10/49 (20%) 17/52 (33%)Anti arrhyhtmic 12/101 (12%) 8/49 (16%) 4/52 (8%)Anticoagulants/ antiaggregants 33/101 (33%) 14/49 (28%) 19/53 (37%)Beta-blockers 19/101 (19%) 9/49 (18%) 10/52(19%)Ca++ antagonists 20/101 (20%) 11/49 (22%) 9/52 (17%)digitalis 2/101 (2%) 1/49 (2%) 1/52 (2%)diuretics 26/101 (26%) 12/49 (24%) 14/52 (27%)Anti-hypertensive 21/101 (21%) 12/49 (24%) 9/52 (17%)Statins 8/101 (8%) 6/49 (12%) 2/52 (4%)*Numbers are % (counts) or mean ± standard deviation.
128±39171717179±9±9±9±6060606012121212 [[[[1111---12121212]]]]1111 [1[1[1[1--2]2]2]2]
pe in last 6 mo 0 [0 1] 0 [0 1] 0 [0 1 5]eu
r
––
h i 47/101 (47%) 27/49 (55%) 20/52 (38%)
pe innn lllasasastt 6 6 6 momm 0 [0-1] 0 [0-1] 0 [0-1.5]eviiiououuus suddddenenee syncope with umumumumaaa.a
42/101 (42%)) 20/49 (4(4(4( 1%))) 22/52 (42%)
eeeearaa ttt t rate at Holteer 47±±±9 5050505 ±±1000 49±8±8±8±r 61666 /1111010101 ((((606060%)%)%) 2626266/4444999 (5(5(553%3%3%) 3555/5/5/5/52 (6(6(67.7 3%3%%%)))- nonenenee 33/101 (((3333 %)%)%) 161616/49 (33%%%%) 17/5/5/52 (33%)- ischchchhemememicicic 19999/1/1/1/ 01010101 ((((119%)%)%)% 9/99/4949499 ((((18181818%)%)%) 10101010/5/5/52222 (1(1(119%9%9%%))))– vavavalvlvlvulululararar 2/2/2/101010111 (2(2(2%)%)%) 1/1/1/494949 (((2%2%2%%))) 1/1/1/525252 (((2%2%2%%))))– dilated 2/2/22/1001001111 (2(22(2%)%)%)% 0/0/0/0/49494949 (((0%0%0%%))) 2/2//2/52525252 ((((4%)
h i 47/101 (47%) 27/49 (55%) 20/52 (38%)
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.112.975102
17
Table 2: Two-years development of syncope, pre-syncope and AV block alone
Total DDI30 DDD60 P value
Syncope 14 (13.9%) 7 (14.3%) 7 (13.5%) 0.89
Presyncope 22 (21.8%) 16 (32.6%) 6 (11.5%) P<001
Symptomatic AV block 10 (9.9%) 8 (16.3%) 2 (3.8%) P<001
Figure Legends:
Figure 1. Kaplan Meier curves - Primary endpoint. HR: Hazard Ratio
Figure 2. Kaplan Meier curves – patient symptoms (Syncope or pre-syncope of any origin) HR:
Hazard Ratio
K
K n
t
KaKaKaplplplplan MMMeieiee er curves - Primary endpoint. HHR: Hazardddd RRRRatioii
Kapllplanaaa Meieieie er curururvevv s – papappatient syyympmpmpptott msmsmms ((((Syyyncopopope or pppreeree-s-s- yny cococopepeppe oooof ff any yy origin
tttioio
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

Gianni Gasparini, Francesco Accardi, Giovanni Raciti and Antonio RavieleFoglia-Manzillo, Fabrizio Ammirati, Maria Luisa Loricchio, Claudio Pedrinazzi, Federico Turreni,
Leonardo Calò, Serafino Orazi, Miguel Viscusi, Leandro Chiodi, Angelo Bartoletti, Giovanni Massimo Santini, Antonio Castro, Franco Giada, Renato Ricci, Giuseppe Inama, Germano Gaggioli,
and Syncope of Unexplained Origin: The PRESS StudyPrevention of Syncope through Permanent Cardiac Pacing in Patients with Bifascicular Block
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2013 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Arrhythmia and Electrophysiology
published online February 6, 2013;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/early/2013/02/06/CIRCEP.112.975102World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org/content/suppl/2013/02/06/CIRCEP.112.975102.DC1Data Supplement (unedited) at:
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answerinformation about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Arrhythmia and Electrophysiology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

SUPPLEMENTAL MATERIAL
Appendix
The required diagnostic examination, that has been performed to verify the exclusion criteria
listed above are the following: Electrocardiogram (ECG): to exclude any ongoing rhythm
disturbance. Tilt Table Test (TTT): A 30 minutes TTT 60°/70° had to be performed to look for
occurrence of syncope. If no syncope occurred in that timeframe Natispry was administered
(0.30mg) and the test was prolonged for other 15 minutes. TTT was judged positive in case of
syncope occurrence associated with bradycardia, hypotension, or both. Carotid sinus massage
testing: the test was done for at least 10 seconds or until episode occurrence, both in supine and
standing positon. ECG and pressure were monitored during the test. The test was judged positive
if a syncope occurred during or immediately after the test together with asystole (≥3 sec.) and/or
hypotension (≤50 mmhg). Electrophysiologic study (EPS): EPS was be done to exclude
ventricular, supraventricular arrhythmias and AV conduction disturbances. The test was judged
be positive if: 1) basal HV interval was ≥100ms or 2) an AV Block superior to 1st degree was
induced with atrial incremental stimulation; or 3) monomorphic sustained VT was induced; or 4)
sustained and symptomatic SVT were induced or 5) recovery time was ≥525 msec. 24 hour
Holter monitoring: a minimum of 20 hour recoding was required with recording available during
nighttime. Patients were excluded if heart rate averaged hour trend during sleep felt below 35
bpm, or if non-sustained VT were recorded. Echocardiography: four chamber view was
performed to measure the LVEF. Only patients with a LVEF >40% were enrolled in the study.


















