
Prevention of Alcohol Dependence: Strategies for Selective, Indicated, and Universal Prevention
10
This article was downloaded by: [University of West Florida] On: 09 October 2014, At: 22:54 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Substance Abuse Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/wsub20 Prevention of Alcohol Dependence: Strategies for Selective, Indicated, and Universal Prevention Narayana Manjunatha DPM, MD a , Sahoo Saddichha BA, MBBS, DPM, MD a , Christoday R. J. Khess MD b , Pratima Murthy DPM, MD a & Mohan K. Isaac DPM, MD, FRCPsych c a National Institute of Mental Health & Neurosciences (NIMHANS) , Bangalore , India b Central Institute of Psychiatry , Ranchi , India c School of Psychiatry and Clinical Neurosciences , University of Western Australia , Perth , Australia Published online: 08 Jun 2011. To cite this article: Narayana Manjunatha DPM, MD , Sahoo Saddichha BA, MBBS, DPM, MD , Christoday R. J. Khess MD , Pratima Murthy DPM, MD & Mohan K. Isaac DPM, MD, FRCPsych (2011) Prevention of Alcohol Dependence: Strategies for Selective, Indicated, and Universal Prevention, Substance Abuse, 32:3, 135-143, DOI: 10.1080/08897077.2011.562736 To link to this article: http://dx.doi.org/10.1080/08897077.2011.562736 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions
Transcript of Prevention of Alcohol Dependence: Strategies for Selective, Indicated, and Universal Prevention

This article was downloaded by: [University of West Florida]On: 09 October 2014, At: 22:54Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Substance AbusePublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/wsub20
Prevention of Alcohol Dependence: Strategies forSelective, Indicated, and Universal PreventionNarayana Manjunatha DPM, MD a , Sahoo Saddichha BA, MBBS, DPM, MD a , Christoday R. J.Khess MD b , Pratima Murthy DPM, MD a & Mohan K. Isaac DPM, MD, FRCPsych ca National Institute of Mental Health & Neurosciences (NIMHANS) , Bangalore , Indiab Central Institute of Psychiatry , Ranchi , Indiac School of Psychiatry and Clinical Neurosciences , University of Western Australia , Perth ,AustraliaPublished online: 08 Jun 2011.
To cite this article: Narayana Manjunatha DPM, MD , Sahoo Saddichha BA, MBBS, DPM, MD , Christoday R. J. Khess MD ,Pratima Murthy DPM, MD & Mohan K. Isaac DPM, MD, FRCPsych (2011) Prevention of Alcohol Dependence: Strategies forSelective, Indicated, and Universal Prevention, Substance Abuse, 32:3, 135-143, DOI: 10.1080/08897077.2011.562736
To link to this article: http://dx.doi.org/10.1080/08897077.2011.562736
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Substance Abuse, 32:135–143, 2011Copyright c© Taylor & Francis Group, LLCISSN: 0889-7077 print / 1547-0164 onlineDOI: 10.1080/08897077.2011.562736
Prevention of Alcohol Dependence:Strategies for Selective,
Indicated, and Universal Prevention
Narayana Manjunatha, DPM, MDSahoo Saddichha, BA, MBBS, DPM, MD
Christoday R. J. Khess, MDPratima Murthy, DPM, MD
Mohan K. Isaac, DPM, MD, FRCPsych
ABSTRACT. Study of the chronology of criteria of dependence in alcohol dependence syndrome(ADS) can enable us to design strategies for the prevention for ADS, which takes into account pri-mary prevention (indicated, selective, and universal prevention) approaches and aims at reducing theoccurrence of ADS. The objective of this work is to study the age-wise and order-wise chronologiesof International Classification of Diseases Tenth Revision Diagnostic Criteria for Research (ICD-10DCR) dependence criteria in individuals with ADS. Consecutively admitted and consenting inpatientswith ICD-10 DCR diagnosis of ADS were evaluated in a structured interview after detoxification usingSemi-Structured Assessment for the Genetics of Alcoholism (SSAGA)-II. The total sample size was81. The mean ages at the first onset of alcohol use, development of the first criterion, and ICD-10 de-pendence was 18.72 years (SD: 6.84), 24.33 years (SD: 9.21), and 27.51 years (SD: 9.28), respectively.In age-wise chronology, tolerance, loss of control, and craving were present in 97.53%, 80.24%, and79%, respectively, of our study sample. In order-wise chronology, either craving (16%) or tolerance(71.6%) was present as the first criterion and the presence of craving (16%), tolerance (21%), or loss ofcontrol (18.5%) was observed as the first criterion in 55.5% of the subjects. Indicated prevention may beattempted by enquiring about craving, tolerance, and loss of control and use of anticraving medicationsor behavioral strategies. Selective prevention by using naltrexone for those genetically inclined anduniversal prevention by use of “clinical” labeling on alcoholic beverages can also be attempted.
KEYWORDS. Alcohol dependence, indicated prevention, selective prevention, universal prevention
Narayana Manjunatha, Sahoo Saddichha, and Pratima Murthy are affiliated with the National Institute ofMental Health & Neurosciences (NIMHANS), Bangalore, India.
Christoday R. J. Khess is affiliated with the Central Institute of Psychiatry, Ranchi, India.Mohan K. Isaac is affiliated with the School of Psychiatry and Clinical Neurosciences, University of
Western Australia, Perth, Australia.Address correspondence to: Dr. Sahoo Saddichha, Department of Psychiatry, National Institute of Men-
tal Health & Neurosciences (NIMHANS), Hosur Road, Bangalore 560029, India (E-mail: [email protected]).
The authors acknowledge the help of Dr. Victor Hesselbrock, PhD, University of Connecticut, Framington,who provided and permitted the authors to use the SSAGA-II. SSAGA-II has been developed by the Collab-orative Study on the Genetics of Alcoholism (COGA), supported by National Institute of Health (NIH) grantU10AA08401 from the National Institute of Alcohol And Alcoholism (NIAAA). The authors also thank theentire COGA team and lastly, but not the least, the patients who made this study possible.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4

136 SUBSTANCE ABUSE
INTRODUCTION
Alcohol dependence syndrome (ADS) hasgained public health importance and has stim-ulated research after Edwards and Gross (1) de-scribed typical behavioral clusters of ADS. Thesame criteria are used to diagnose ADS acrossthe world in both International Classification ofDiseases Tenth Revision (ICD-10) and Diagnos-tic and Statistical Manual of Mental DiseasesFourth Edition (DSM-IV), with some variations.In ICD-10, the presence of minimum 3 out of 6criteria is required to diagnose ADS (2). After di-agnosis, the management follows the establishedalgorithms of secondary and tertiary prevention.However, it is quite likely that the person has hadcontact with a primary health care setup beforethe development of ADS, where he may havereceived treatment for other alcohol-related con-ditions such as gastritis, hepatitis, etc. (3), andmay be targeted for prevention of alcohol depen-dence. This category of patients has been termed“diagnostic orphans” by Kaczynski and Martin(4) and others have adopted it (5, 6). These per-sons may have high risk to develop ICD-10 de-pendence syndrome and eventually present with3 or more criteria (5). Moreover, diagnostic or-phans are more likely to seek help for alcohol-related problems before developing full-fledgeddependence syndrome (7). It becomes pertinent,therefore, to know whether intervention strate-gies may help in progression to dependence inthis group, and the best time to implement suchstrategies.
Research on alcohol diagnostic orphans isscant when compared to ADS (8), although therehave been some recent attempts to address thisgap (4–6). This may be because of difficul-ties inherent in definition, terminology, measure-ment, and extent of causation for alcohol-relatedproblems (9). Further, the experience of depen-dence criteria has also been noted to be varyingacross the world (10). Because alcohol-relatedproblems are more common in nondependentdrinkers than in dependent drinkers (11), it be-comes essential to study the natural progres-sion of ADS to formulate effective strategiesof prevention in alcohol diagnostic orphans andfor those alcohol users without any dependencecriteria.
Secondary and tertiary prevention are cur-rently the predominating issues in the manage-ment of ADS, i.e., detoxification, relapse preven-tion, etc. However, there are obstacles towardsprimary prevention of ADS, such as the socialacceptance of alcohol use (12), cardioprotectivebenefit (13), legal and free availability (14), sta-tistically significant prevention programs (15),and an assumption that prevention is not pos-sible due to unknown etiology of alcohol de-pendence (16). These obstacles indicate that itis impossible to think of an alcohol-free societyalthough long-term alcohol use has been asso-ciated with many physical problems, e.g., my-ocardial infarction, strokes, etc. (13). Althoughan alcohol-free society may be an impossibility,primary prevention of dependence syndrome isboth realistic and feasible. There is, therefore, aneed to develop effective prevention strategies,for which identifying the right factors and dura-tion between onset and development of depen-dence in our population is required.
There is very little research on primary pre-vention of ADS. Ehlers et al. (17) carried outa community-based study on clinical course ofalcoholism with targeting the preventive strate-gies, but not formulated any preventive plan. Asystematic study and analysis of chronology ofdependence criteria has not been comprehen-sively carried out to date, although some at-tempts have been made to do so (18), includ-ing an earlier paper of ours (19). This mightbe helpful in designing a strategy for the pre-vention of ADS, and lowering the incidence ofADS. We report here a systematic study of thechronology (age-wise and order-wise) and theprevalence of each criterion of ICD-10 ADS ofin-patients, which may be helpful in designingstrategies of primary prevention for ADS andto better identify the “at-risk” population, espe-cially in routine primary care practice.
METHODS
The exact methodology has been detailed inan earlier paper (20). Briefly, patients admittedconsecutively into Centre for Addiction Psychi-atry, Central Institute of Psychiatry, Ranchi, and
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4

Manjunatha et al. 137
meeting a clinical diagnosis of ADS as per ICD-10 and who gave written informed consent wererecruited for this study. The study protocol wasapproved by the Institute’s “Ethics Committee.”Subjects who met criteria for other substancedependence, those who had other comorbid psy-chiatric disorders or general medical conditions,and patients with Mini-Mental Status Examina-tion (MMSE) (21) screening scores of less than24 were excluded from the study.
Patients who fulfilled study criteria were in-terviewed using the alcohol section of Semi-Structured Assessment for the Genetics ofAlcoholism-II (SSAGA-II) (22), after detoxifi-cation. SSAGA-II is a polydiagnostic instrumentdeveloped by Collaborative Study on the Genet-ics of Alcoholism team designed to assess thephysical, psychological, and social manifesta-tions of alcohol and other substances as well asother psychiatric disorder according to ICD-10and DSM-IV. It also has items related to each cri-terion of dependence of ICD-10. Reliability andvalidity of SSAGA has been established (22, 23).The alcohol section of SSAGA-II contains 45multipart items. SSAGA has good concordancewith Schedule for Clinical Assessment in Neu-ropsychiatry (24) and has good kappa value (κ =.63) for alcohol dependence (23). SSAGA-II per-mits detailed evaluation of first onset of eachcriterion of dependence according to ICD-10.
Since it was retrospective study, questionswere framed individually to trigger the recallusing anchor questions to personal and imper-sonal or important social events and definingthe technical terms (25). Relevant informationof patients was also corroborated from their re-spective case records completed at the time ofadmission. In case of discrepancy of any items,it was discussed with patient for consensus. Atthe end of interview, data were transferred tothe ICD-10 tally sheet of respective items in thealcohol section of SSAGA-II. Among the firstage(s) of appearance of items of each criterion,we considered the earliest age of appearance ofany item as age of first appearance of the respec-tive criterion of dependence (ICD-10 Diagnos-tic Criteria for Research [DCR]). We consideredthe age of development of ICD-10 dependencesyndrome as the age of onset of a third con-secutive criterion, with the simultaneous pres-
ence of other 2 criteria (among the 6 criteria ofICD-10).
The criteria of ICD-10 ADS (2) are (a) astrong desire or sense of compulsion to takealcohol (craving); (b) difficulties in controllingalcohol-taking behavior in terms of onset, ter-mination, or levels of use (loss of control);(c) physiological withdrawal state; (d) tolerance;(e) progressive neglect of alternative pleasures orinterests (salience), and (f) persistent use despiteovert physical or psychological harm. The keywords (in italics) of each criterion are used indiscussion of this study.
RESULTS
Total sample size of present study was 81.All subjects were males, with mean age 35.16years (SD: 10.20). Mean years of formal ed-ucation was 11.69 years (SD: 3.98). A 49.4%(N = 40) were engaged in skilled and semiskilledjobs, 27.2% (N = 22) were professionals, 8.6%(N = 7) were students, 8.6% (N = 7), wereunemployed and 6.2% (N = 5) were not in ac-tive employment. A 70.4% (N = 57) subjectswere married, 27.2% (N = 22) were single, and1.2% each (N = 1) were separated and divorced.Mean monthly income was INR 8451.23 (SD:7901.03) (approximately $187.8 [SD: $175.6])and their residence status were of urban 75.3%(N = 61) and rural 24.7% (N = 20) origins. A77.8% (N = 63) of our study samples had familyhistory of alcohol dependence.
This study analyzed the 2 types of chronol-ogy of ICD-10 dependence: age-wise chronol-ogy (for all criteria) and order-wise chronology(up to only the third criterion, because it metthe threshold criteria to diagnose ICD-10 depen-dence). The age-wise chronology was analyzedfor better understanding of course and progres-sion of the disorder, given as ages at which pa-tients experienced the first onset of each crite-rion of dependence and its frequencies (Table 1).The order-wise chronology of each criterion issummarized as its frequencies in their order ofappearance of the first, second, and third crite-ria at their life-time first appearance (Table 1).However, age-wise chronology of each criterionhas important shortcomings. Firstly, not every
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4

TAB
LE1.
Res
ults
ofP
rese
ntS
tudy
and
Com
paris
onw
ithE
hler
set
al.(
2004
)
Ehl
ers
etal
.,20
04(1
7)P
rese
ntst
udy
(N=
81)
Age
atw
hich
the
crite
rion
was
Pat
ient
sA
geat
whi
chth
efir
stex
perie
nced
who
expe
ri-th
ecr
iterio
nw
asP
atie
nts
who
(age
-wis
eO
rder
-wis
ech
rono
logy
ofea
chcr
iterio
nen
ced
the
first
expe
rienc
edex
perie
nced
chro
nolo
gy)
crite
rion
(yea
rs)
the
crite
rion
(yea
rs)
Firs
tS
econ
dT
hird
ICD
-10
crite
riaof
depe
nden
cen
%M
ean
SD
n%
Mea
nS
Dn
%n
%n
%
Cra
ving
7029
21.3
95.
9264
79.0
026
.71
8.05
1316
.013
16.0
1619
.8To
lera
nce
211
8720
.41
5.99
7997
.53
25.1
59.
3758
71.6
1721
.02
02.5
Loss
ofco
ntro
l19
781
21.0
96.
4065
80.2
427
.76
9.39
303
.715
18.5
2227
.2S
alie
nce
106
4420
.78
5.98
3138
.27
29.6
77.
730
101
.29
11.1
With
draw
alsy
mpt
oms
8133
23.1
27.
3175
92.6
27.0
49.
786
07.4
2935
.821
25.9
Per
sist
use
desp
iteha
rm33
1424
.09
6.60
7187
.65
27.6
17.
731
01.2
607
.411
13.6
138
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4

Manjunatha et al. 139
TABLE 2. Notable Age of Onset of DifferentChronology of Present Study
Age of onset(in years)
Criteria (mean ± SD)
Age at onset of alcohol use 18.72 ± 6.84Age at onset of first criterion 24.33 ± 9.21Age at onset of second criterion 25.86 ± 9.45Age at onset of ICD-10 dependence 27.51 ± 9.28Duration from onset of alcohol use to first
criterion5.61 ± 6.2
Duration from onset of alcohol use todependence
8.78 ± 6.7
Duration from first criterion todependence
3.17 ± 3.23
patient experiences each criterion of depen-dence, which is evident in the present study aswell as in other studies (18), and secondly, theage of onset of dependence may not be the ap-pearance of any criterion of dependence (18).The order-wise chronology of each criterion isvery important in overcoming the shortcomingsof age-wise chronology. The ages of life-timefirst appearance of the first, second, and third cri-teria as a whole and the time duration betweenimportant milestones that are important in for-mulating the prevention plan of ADS are givenin Table 2. This can help in better understandingof individual criterion in alcoholic diagnostic or-phans for the purposes of primary prevention ofADS.
DISCUSSION
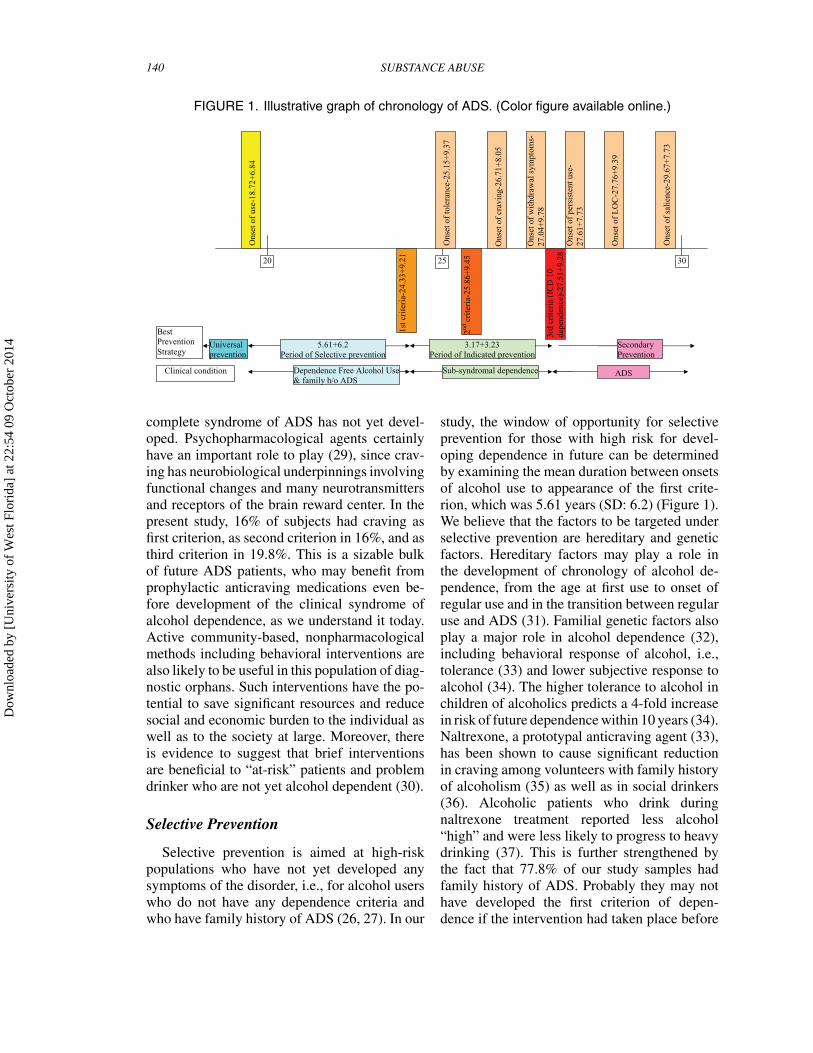
The time-gap between onset of alcohol useand appearance of the first criterion and fromonset of alcohol use to ICD-10 dependence was5.61 years (SD: 6.2) and 8.78 years (SD: 6.7),respectively (Table 2). On an average, a personuses alcohol for about 6 years before developingthe first criterion of dependence. Thus, criterion-free (or social) drinking lasts for 6 years approx-imately, and if alcohol use continues, then inabout 3 to 4 years, ICD-10 dependence developsclinically. This time frame can be useful for insti-tuting strategies for prevention in this population(Figure 1).
Indicated Prevention
Indicated prevention is directed at the pop-ulation not just with high risk but with mini-mal and detectable symptoms that do not meetthe diagnostic criteria (26). In our study, theages at onsets of the first criterion and ICD-10 dependence were 24.33 years (SD: 9.21) and27.51 years (SD: 9.28) (Figure 1). Duration be-tween onset of the first criterion and ICD-10dependence was 3.17 years (SD: 3.23). A per-son therefore uses alcohol for about 3 to 4 yearsfrom the appearance of the first criterion to de-velopment of ICD-10 dependence. These per-sons are referred to as “alcoholic diagnostic or-phans,” as has been mentioned before, and aretherefore the best target for indicated preven-tion of ADS (27), because these groups are rel-atively more motivated for intervention at thisstage (7) and can be targeted individually by aclinician.
At this stage, analyzing the data of both age-wise and order-wise chronologies can give usa path towards indicated prevention by deter-mining the questions to be asked. In order-wise chronology, either craving or tolerance waspresent in 87.6% as first criterion and presence ofeither of craving (16%), tolerance (21%), or lossof control (18.5%) was seen as second criterionin 55.5% of the subjects. Moreover, in age-wisechronology, tolerance, loss of control, and crav-ing were present in 97.53%, 80.24%, and 79% ofour study sample, respectively. In both age-wiseas well as order-wise chronologies, craving, tol-erance, and loss of control emerged as the mostfrequently occurring criteria during predepen-dence stage of alcohol dependence. These cri-teria are hence to be enquired from all personswho are “alcoholic diagnostic orphans.” If theseare routinely enquired by all clinicians in all al-cohol users, it may help in earlier detection andpossible indicated prevention of ADS in diag-nostic orphans and reduce the increased risk ofprogression to dependence from any predepen-dence criteria (28).
Possible methods for indicated prevention areuse of anticraving medications that may be use-ful in alcohol diagnostic orphans (as prophylaxisfor prevention of ADS rather than as merelyfor relapse prevention) when craving has de-veloped as first or second criterion, even if the
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4
140 SUBSTANCE ABUSE
FIGURE 1. Illustrative graph of chronology of ADS. (Color figure available online.)
Ons
et o
f us
e-18
.72+
6.84
1st c
rite
ria-
24.3
3+9.
21
Ons
et o
f cr
avin
g-26
.71+
8.05
Ons
et o
f to
lera
nce-
25.1
5+9.
37
2nd c
rite
ria-
25.8
6+9.
45
Ons
et o
f sa
lien
ce-2
9.67
+7.
73
Ons
et o
f L
OC
-27.
76+
9.39
Ons
et o
f pe
rsis
tent
use
-27
.61+
7.73
3rd
crit
eria
(IC
D 1
0
depe
nden
ce)-
27.5
1+9.
28
Ons
et o
f w
ithd
raw
al s
ympt
oms-
27
.04+
9.78
5.61+6.2 Period of Selective prevention
3.17+3.23 Period of Indicated prevention
Secondary Prevention
Universal prevention
Dependence Free Alcohol Use& family h/o ADS
Sub-syndromal dependence
20 25 30
ADS
Best Prevention Strategy
Clinical condition
complete syndrome of ADS has not yet devel-oped. Psychopharmacological agents certainlyhave an important role to play (29), since crav-ing has neurobiological underpinnings involvingfunctional changes and many neurotransmittersand receptors of the brain reward center. In thepresent study, 16% of subjects had craving asfirst criterion, as second criterion in 16%, and asthird criterion in 19.8%. This is a sizable bulkof future ADS patients, who may benefit fromprophylactic anticraving medications even be-fore development of the clinical syndrome ofalcohol dependence, as we understand it today.Active community-based, nonpharmacologicalmethods including behavioral interventions arealso likely to be useful in this population of diag-nostic orphans. Such interventions have the po-tential to save significant resources and reducesocial and economic burden to the individual aswell as to the society at large. Moreover, thereis evidence to suggest that brief interventionsare beneficial to “at-risk” patients and problemdrinker who are not yet alcohol dependent (30).
Selective Prevention
Selective prevention is aimed at high-riskpopulations who have not yet developed anysymptoms of the disorder, i.e., for alcohol userswho do not have any dependence criteria andwho have family history of ADS (26, 27). In our
study, the window of opportunity for selectiveprevention for those with high risk for devel-oping dependence in future can be determinedby examining the mean duration between onsetsof alcohol use to appearance of the first crite-rion, which was 5.61 years (SD: 6.2) (Figure 1).We believe that the factors to be targeted underselective prevention are hereditary and geneticfactors. Hereditary factors may play a role inthe development of chronology of alcohol de-pendence, from the age at first use to onset ofregular use and in the transition between regularuse and ADS (31). Familial genetic factors alsoplay a major role in alcohol dependence (32),including behavioral response of alcohol, i.e.,tolerance (33) and lower subjective response toalcohol (34). The higher tolerance to alcohol inchildren of alcoholics predicts a 4-fold increasein risk of future dependence within 10 years (34).Naltrexone, a prototypal anticraving agent (33),has been shown to cause significant reductionin craving among volunteers with family historyof alcoholism (35) as well as in social drinkers(36). Alcoholic patients who drink duringnaltrexone treatment reported less alcohol“high” and were less likely to progress to heavydrinking (37). This is further strengthened bythe fact that 77.8% of our study samples hadfamily history of ADS. Probably they may nothave developed the first criterion of depen-dence if the intervention had taken place before
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4

Manjunatha et al. 141
becoming alcoholic diagnostic orphans and ulti-mately preventing ADS.
Universal Prevention
This is aimed at the general population irre-spective of risk, e.g., school programs, mass me-dia campaigns, etc. (26, 27). Innovative strate-gies may be tried for universal prevention suchas detailing criteria of dependence or “clinicallabeling” on the labels of alcoholic beverages ina simple, commonly used language, along withthe label that “Alcohol is injurious to health.” Inaddition, routine enquiries about alcohol use interms of criteria of dependence by primary carephysicians in all patients irrespective of diag-nosis could help in universal prevention. In theauthors’ opinion, the above technique should becombined with routine questions on the use ofalcohol, its frequency and quantity, such as “Doyou drink alcoholic beverages? How often? Howmuch?” (38).
A recent report of the Institute of Medicine(IOM) recommended that preventive interven-tions, earlier described as primary prevention,are to be subdivided into 3 subcategories (i.e.,universal, selective, and indicated prevention)designed for populations before the onset offull-blown mental disorders (i.e., ADS) that areaimed at reducing the incidence of any mentaldisorder (39). Therefore, all 3 types of primaryprevention (universal, selective, and indicated)may be possible in ADS when we know thechronology of dependence criteria (Figure 1).Among the 3 types of primary prevention,studies of interventions on indicated preventionhave shown reduction in the incidence of mentaldisorders, whereas insufficient data exist onselective and universal prevention on reducingthe incidence of mental disorders (15). However,Cuijpers (15) opines that synergistic effect ofcombining the interventions of all 3 types ofprimary prevention may be superior to eachindividual type of prevention alone. We suggestthat the term “alcohol predependence” be usedfor an alcohol user when there is any evidenceof socio-occupational dysfunction in the periodof onset of the first criterion to onset of thethird criterion. Further, the term “subsyndromealcohol dependence” may be used for alcoholrelapse and those who have not achieved full
dependence, as relapses are very common evenafter abstinence (40).
We also believe that using the preven-tion approaches will also prevent withdrawalsymptoms, especially life-threatening deliriumtremens and withdrawal seizure, since with-drawal symptoms are a sure sign of onset ofICD-10 dependence, seen in our study as thenear-simultaneous onset of both withdrawal as acriterion and dependence as a syndrome (27.04and 27.5 years, respectively). Our study find-ings are also similar to an earlier study (17) ina community sample in terms of tolerance andloss of control. The difference in the prevalenceof withdrawal symptoms can be attributed to theorigin of the sample—hospital versus commu-nity population (41). The differences in criteriaof “persistent use despite harm” may be becauseof cultural variations in attribution of harm toalcohol as appearance of different criteria (10).In spite of these differences, we believe that ourfindings and suggestions are significant enoughto be initiated on a large-scale basis that mayform part of the National Mental Health Pro-gram in India.
Strengths
The descriptions of order-wise chronologyalong with age-wise chronology of each crite-rion of dependence are unique in this study. Tothe best of our knowledge, this is the first studyconducted on chronologies of dependence crite-ria. Prevalence of each criterion in our study ismore or less consistent with other studies. Thisis also the first study to discuss a strategy forprimary prevention of ADS rather than just al-cohol use, which is more realistic in reducingthe incidence of ADS in the society at large.Even though this is a retrospective study, ade-quate care has been taken to minimize the in-evitable recall bias, by using more reliable andvalid instruments (SSAGA-II), MMSE screen-ing before interview, corroboration from CaseRecord Form as well as questions in interviewbeing individually framed.
Limitations
There are inherent limitations in this studydesign such as inclusion of only male patients,
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4

142 SUBSTANCE ABUSE
historical cohort study, recall bias even thoughit is reduced to great extent, and lack of general-izability (in terms of ages of onset) to a generalpopulation. However, our study gives the broadframework for prevention of ADS.
Future Directions
We suggest future studies in different targetpopulations in different countries in order to for-mulate individual respective plans for primaryprevention of ADS with the help of the broadframework derived in our study, since our find-ings may not be applicable to other culture interms of ages of onset of different criteria be-cause of cultural variations of meanings in cri-teria of dependence such as salience, tolerance,etc. Prospective studies may also concentrate onthe effectiveness of preventive interventions ofpredependence alcohol users.
CONCLUSIONS
The chronology of dependence criteria givesus an opportunity for intervention as a step to-wards primary prevention of ADS. Adequatetraining of primary care personnel and early psy-chiatric referral may be helpful. All 3 types ofprimary prevention are possible for ADS. En-quiring about presence of craving, tolerance,withdrawal symptoms, and loss of control rou-tinely in every alcohol user presenting to healthcare would be beneficial for indicated preven-tion. Describing criteria of dependence in a sim-ple language as mode of public education in massmedia as well as on all alcohol beverages androutine enquiry by primary care physicians aboutdependence criteria may be useful as strategiesof universal prevention. Prospective studies oneffectiveness of the suggested interventions inalcohol user are required.
REFERENCES
1. Edwards G, Gross MM. Alcohol dependence:provisional description of a clinical syndrome. BMJ.1976;1:1058–1061.
2. World Health Organization. ICD-10 Classificationof Mental and Behavioural Disorders. Diagnostic Criteria
for Research (DCR). Geneva: World Health Organization;1993.
3. Chand PK, Issac MK. Management of substanceuse disorder in primary care. In: Lal R, ed. Substance UseDisorder—Manual for Physicians. New Delhi: NationalDrug Dependence Treatment Centre, All India Institute ofMedical Sciences; 2005:1–12.
4. Kaczynski-Pollock N, Martin CS. Diagnostic or-phans: adolescent with alcohol symptoms who do not qual-ify for DSM IV abuse or dependence diagnoses. Am J Psy-chiatry 1999;156:897–901.
5. Eng MY, Schuckit MA, Smith TL. A five-yearprospective study of diagnostic orphans for alcohol usedisorders. J Stud Alcohol. 2003;64:227–234.
6. Hasin D, Paykin A. Dependence symptoms butnon-problem drinkers: diagnostic ‘orphans’ in a 1992national sample. Drug Alcohol Depend. 1999;53:215–222.
7. Sarr M, Bucholz KK, Phelps DL. Using cluster anal-ysis of alcohol use disorders to investigate ‘diagnostic or-phans’: subjects with alcohol dependence symptoms but nodiagnosis. Drug Alcohol Depend. 2000;60:295–302.
8. Drummond DC. The relationship between alcoholdependence and alcohol-related problems in a clinical pop-ulation. Br J Addict. 1990;85:357–366.
9. Room R. Measuring alcohol consumption in theUnited States: methods and rationales. In: Kozlowski LT,Annis HM, Cappell HD, et al., eds. Research Advances inAlcohol and Drug Problems. Vol. 10. New York: PlenumPress; 1990:39–80.
10. Schmidt L, Room R. Cross-cultural applicability ininternational classifications and research on alcohol depen-dence. J Stud Alcohol. 1999;60:448–462.
11. Marshall J. Alcohol dependence and alcohol prob-lems. In: Gelder MG, Lopez-Ibor JJ, Andreasen N, eds.New Oxford Textbook of Psychiatry. Oxford, UK: OxfordUniversity Press; 2000:482–488.
12. Park K. Mental health. In: Park K, ed. Park’s Text-book of Preventive and Social Medicine. Jabalpur, India:Banarsidas Bhanot Publishers; 2005:632–637.
13. Friedman GD, Klatsky AL. Is alcohol good for yourhealth? N Engl J Med. 1993;329:1882–1883.
14. Room R. Prevention of alcohol-related problems. In:Gelder MG, Lopez-Ibor JJ, Andreasen N, eds. New OxfordTextbook of Psychiatry. Oxford, UK: Oxford UniversityPress; 2000:514–518.
15. Cuijpers P. Examining the effects of preventionprograms on the incidence of new cases of mental dis-orders: the lack of statistical power. Am J Psychiatry.2003;160:1385–1391.
16. Raphael B. Prevention in psychiatry: Australian con-tributions. Aust N Z J Psychiatry. 2000;34, S6–S13.
17. Ehlers CL, Wall TL, Betancourt M, Gilder DA. Theclinical course of alcoholism in 243 Mission Indians. Am JPsychiatry. 2004;161:1204–1210.
18. Mattoo SK, Basu D. Clinical course of alcohol de-pendence. Indian J Psychiatry. 1997;39:294–99.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4

Manjunatha et al. 143
19. Sahoo S, Majunatha N, Baxi BNP, Khess CRJ. Whyis alcohol excluded and opium included in NDPS Act,1985? Indian J Psychiatry. 2007;49:126–128.
20. Manjunatha N, Saddichha S, Sinha BNP, Khess CRJ,Isaac MK. Chronology of alcohol dependence: implicationsin prevention. Indian J Community Med. 2008;33:233–237.
21. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State—a practical method for grading the cogni-tive state of patients for the clinician. J Psychiatr Res.1975;12:189–198.
22. Bucholz KK, Cadoret R, Cloninger CR, et al. A new,semi-structured psychiatric interview for the use in geneticlinkage studies: a report on the reliability of the SSAGA.J Stud Alcohol. 1994;55:149–158.
23. Hesselbrock M, Easton C, Bucholz KK, et al. Avalidity study of the SSAGA: a comparison with the SCAN.Addiction. 1999;94:1361–1370.
24. Wing JK, Babor T, Brigha T, et al. SCAN—Schedules for Clinical Assessment in Neuropsychiatry.Arch Gen Psychiatry. 1990;47:589–593.
25. Carlat DJ. Asking questions III: tricks for improv-ing patient recall. In: Carlat DJ, ed. The Psychiatric Inter-view: A Practical Guide. 2nd ed. Philadelphia: LippincottWilliams & Wilkins; 2005:27–29.
26. Reddy MS. Primary prevention in psychiatry [edito-rial]. Indian J Psychol Med. 2009;31:1–2.
27. Gordon RS. An operational classification of diseaseprevention. Public Health Rep. 1983;98:107–109.
28. De Brujin C, van de Brink W, de Graaf R, VolleberghWAM. Alcohol abuse and dependence criteria as predictorsof a chronic course of alcohol use disorders in the generalpopulation. Alcohol Alcohol. 2005;40:441–446.
29. George MS, Anton RF, Bloomer C, et al. Activa-tion of prefrontal cortex and anterior thalamus in alcoholicsubjects on exposure to alcohol-specific cues. Arch GenPsychiatry. 2001;58:345–352.
30. Fiellin DA, Reid MC, O’Connor PG. New therapiesfor alcohol problems: application to primary care. Am JMed. 2000;108:227–237.
31. Liu I, Blacker DL, Xu R, et al. Genetic and en-vironmental contributions to the development of alco-hol dependence in male twins. Arch Gen Psychiatry.2004;61:897–903.
32. Numberger JI, Wiegand R, Bucholz K, et al. A fam-ily study of alcohol dependence coaggregation of multipledisorders in relatives of alcohol-dependent probands. ArchGen Psychiatry. 2004;61:1246–1256.
33. O’Brien CP. Anti-craving medications for re-lapse prevention: a possible new class of psychoac-tive medications. Am J Psychiatry. 2005;162:1423–1431.
34. Schuckit MA. Low level of response to alcoholas a predictor of future alcoholism. Am J Psychiatry.1994;151:184–189.
35. King AC, Volpicelli JR, Frazer A, et al. Effect of nal-trexone on subjective alcohol response in subjects at highand low risk for future alcohol dependence. Psychophar-macology (Berl). 1997;129:15–22.
36. Davidson D, Swift RM, Fitz E. Naltrexone increasesthe latency to drink alcohol in social drinkers. Alcohol ClinExp Res. 1996;20:732–739.
37. Volpicelli JR, Watson NT, King AC, et al. Effect ofnaltrexone on alcohol “high” in alcoholics. Am J Psychiatry.1995;152:613–615.
38. Kitchens JM. Does this patient have an alcohol prob-lem? JAMA. 1994;272:1782–1787.
39. Mrazek D, Mrazek PJ. Prevention of psychiatric dis-orders in children and adolescents. In: Sadock BJ, SadockVA, eds. Kaplan & Sadock’s Comprehensive Textbook ofPsychiatry. 8th ed. Philadelphia: Lippincott Williams &Wilkins; 2005:3513–3519.
40. Vallant GE. A long term follow-up of male alcoholabuse. Arch Gen Psychiatry. 1996;53:243–249
41. Schuckit MA, Smith TL, Daeppen JB, et al. Clinicalrelevance of the distinction between alcohol dependencewith and without a physiological component. Am J Psychi-atry. 1998;155:733–740.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 2
2:54
09
Oct
ober
201
4







![Selective serotonin reuptake inhibitors [SSRIs] and ... SSRIs SNRIs prevention... · Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine ... and tension-type](https://static.fdocuments.net/doc/165x107/5ce01be988c99399558de41a/selective-serotonin-reuptake-inhibitors-ssris-and-ssris-snris-prevention.jpg)










