Hepatic Steatosis in Rats Fed Diets With Varying Concentrations of Sucrose

35
ORIGINAL ARTICLE
Acta Medica Indonesiana - The Indonesian Journal of Internal Medicine
Prevalence of Hepatic Steatosis in Chronic Hepatitis B Patients and Its Association with Disease Severity
Laurentius A. Lesmana1,2, C. Rinaldi A. Lesmana1,2, Levina S. Pakasi2, Ening Krisnuhoni3 1 Department of Internal Medicine, Faculty of Medicine, University of Indonesia - dr. Cipto Mangunkusumo Hospital. Jl. Diponegoro no. 71, Jakarta Pusat 10430, Indonesia. Correspondence mail: [email protected]. 2 Digestive Disease Center, Medistra Hospital, Jakarta, Indonesia. 3 Department of Anatomical Pathology, Faculty of Medicine, University of Indonesia - dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia.
ABSTRAKTujuan: untuk mengetahui prevalensi steatosis hepatis pada pasien hepatitis B kronik (HBK) dan meneliti
apakah hal tersebut berkaitan dengan penyakit yang lebih progresif. Metode: penelitian dengan desain potong lintang dilaksanakan di Rumah Sakit Cipto Mangunkusumo dan Rumah Sakit Medistra, Jakarta terhadap pasien dengan hepatitis B kronik dari tahun 2007 hingga 2009. Data yang diteliti meliputi data demografi pasien, antropometri, uji fungsi hati dan uji serologi Hepatitis B. Diagnosis steatosis hepatis dinilai berdasarkan biopsi hati dan dinilai derajat keparahannya sebagai derajat ringan (<33%), sedang (33-66%), atau berat (>66%). Derajat fibrosis dan aktivitas nekroinflamasi dinilai berdasarkan sistem METAVIR. Hasil: seratus tujuh puluh empat pasien ikut serta dalam penelitian ini; 99 (56,9%) di antaranya adalah laki-laki. Usia rata-rata pasien berkisar antara 39,9 + 10,69 tahun. Sekitar 56% kasus menunjukkan hasil HBeAg negatif. Prevalensi steatosis hepatis adalah sebesar 29,9%. Pasien dengan steatosis hepatis secara bermakna mempunyai indeks massa tubuh (25,1 + 3,3 vs. 22,7 + 3,33 kg/m2, p<0,001) dan lingkar pinggang (88,3 vs. 79,0 cm; p<0,001) yang lebih tinggi. Tidak ada keterkaitan antara steatosis hepatis dan status HBeAg (p=0,736). Tidak ada perbedaan antara log kadar HBV DNA (5,72+1,993 vs. 6,07+2,077; p=0,675) dan kekakuan hati (8,3+6,28 vs. 9,5+10,18 kPa) antara pasien dengan dan tanpa steatosis hepatis. Fibrosis (61,5% vs. 69,7%; p=0,295) dan nekroinflamasi (63,5% vs. 65,6%; p=0,789) yang tampak jelas ternyata tidak berbeda antara pasien dengan dan tanpa steatosis hepatis Kesimpulan: steatosis hepatis ditemukan pada 30% pasien dengan hepatitis B kronik. Keberadaannya paling sering dikaitkan dengan obesitas sentral. Tidak seperti hepatitis C kronik, steatosis hepatis pada hepatitis B kronik tidak berhubungan dengan penyakit yang lebih progresif.
Kata kunci: steatosis hepatis, hepatitis B kronik, fibrosis hati.
ABSTRACTAim: to know the prevalence of liver steatosis in chronic hepatitis B (CHB) patients and evaluate whether
its presence was associated with a more progressive disease. Methods: a cross-sectional study was conducted in Cipto Mangunkusumo and Medistra Hospitals, Jakarta on CHB patients between 2007 and 2009. Data on patients’ demography, anthropometry, liver function test and hepatitis B serology were collected. Hepatic steatosis was assessed by liver biopsy and graded as mild (<33%), moderate (33-66%) or severe (>66%). Fibrosis stage and necroinflammatory activity were assessed according to the METAVIR system. Results: one-hundred and seventy four patients were enrolled; 99 (56.9%) among them were men. Patients’ mean age was 39.9+10.69 years. About 56% of cases were HBeAg negative. The prevalence of liver steatosis was 29.9%. Patients with liver steatosis had significantly higher body mass index (25.1+3.3 vs. 22.7+3.33 kg/m2, p<0.001) and waist circumference (88.3 vs. 79.0 cm; p<0.001). No association between liver steatosis and HBeAg status (p=0.736). There were no differences of log HBV-DNA levels (5.72+1.993 vs. 6.07+2.077; p=0.675) and liver stiffness (8.3+6.28 vs.

36
Laurentius A. Lesmana Acta Med Indones-Indones J Intern Med
INTRODUCTIONHepatic steatosis is the accumulation of
lipid droplets in hepatocytes characterized by microvesicular and/or macrovesicular steatosis.1
Hepatic steatosis is a common finding in patients with chronic hepatitis B (CHB) with prevalence varies from less than 20%2,3, 30-40%4,5 to more than 55%.6,7 There is no explanation why the prevalence varies greatly among studies. Altogether, the presence of hepatic steatosis in CHB was considered low compared to those occurring in chronic hepatitis C (CHC); in which viral factors contributes directly to the development of insulin resistance and fat accumulation in the liver.8
The impact of hepatic steatosis on the natural course of CHB is less recognized compared to those known in chronic hepatitis C patients. While CHB patients have increased risk of developing cirrhosis and hepatocellular carcinoma (HCC), recently non-alcoholic fatty liver (NAFLD) has also been regarded as a risk factor for HCC.9 Therefore, it is tempting to know whether the presence of hepatic steatosis is associated to a more progressive disease, such as liver fibrosis and cirrhosis.
The prevalence of hepatic steatosis in CHB patients and its impact has not been studied in Indonesia. Therefore, this study was primarily aimed to find the prevalence of hepatic steatosis in CHB patients and secondarily to evaluate whether its presence was associated with disease severity in terms of serum alanine aminotransferase (ALT) and hepatitis B virus deoxyribonucleic acid (HBV-DNA) levels, hepatitis B e antigen (HBeAg) status, liver fibrosis and necroinflammatory grade.
METHODS
Study Design and SubjectsA cross-sectional study was done in Cipto
Mangunkusumo Hospital and Medistra Hospital,
Jakarta on CHB patients between 2007 and 2010. Patients were included if they were willing to undergo liver biopsy. Data on patients’ demography, anthropometry, liver function test and hepatitis B serology were collected. Body mass index (BMI) was calculated as body weight in kilograms divided by body height in meter square (kg/m2). Obesity was defined by a body mass index of more than 25 kg/m2 for Asian population, according to the World Health Organization.
Laboratory ProceduresBlood chemistry test was done by using
automated blood analyzer (Advia Hematology Analyzer, Siemens Diagnostics, Bad Nauheim, Germany). Hepatitis B serology markers, i.e. HBsAg, HBeAg, and anti-HBe were checked using the enzyme-linked immunosorbent assay (ELISA) with commercial kits. Quantitative serum HBV-DNA level was measured using the polymerase chain reaction technique (COBAS®
TaqMan HBV Test, Roche Diagnostics, Basel, Switzerland). The lower detection limit was 4.700 copies/mL. Genotype analysis was performed using specific primers.
Liver BiopsyLiver biopsy was performed using a 16-gauge
Menghini needle (Hepafix, Braun, Melsungen AG, Germany) under local anesthesia. The specimens then were fixed in formalin and embedded in paraffin blocks. A 4-μm thick of the specimens were cut and stained with hematoxylin eosin. Fibrosis was assessed with Masson trichrome staining. Histopathology assessment was done by an experienced pathologist, who was blinded to the patients’ clinical history. Adequate specimens should be at least 15 mm long and includes 5 portal systems. The degree of steatosis was graded 1 to 3, according to the percentage of cells with fatty droplets (grade 1: (mild) 0-33%, grade 2 (moderate): 34-66%, grade 3 (severe): 67-100%). The stage of fibrosis
9.5+10.18 kPa) between patients with and without liver steatosis. The presence of significant fibrosis (61.5% vs. 69.7%; p=0.295) and necroinflammation (63.5% vs. 65.6%; p=0.789) was not differed between patients with and without liver steatosis. Conclusion: liver steatosis was found in 30% of chronic hepatitis B patients. Its presence was mostly associated with central obesity. Unlike chronic hepatitis C, liver steatosis in chronic hepatitis B was not related to a more progressive disease.
Key words: liver steatosis, chronic hepatitis B, liver fibrosis.
37
Vol 44 • Number 1 • January 2012 Prevalence of Hepatic Steatosis in Chronic Hepatitis B Patients
was measured based on the METAVIR scoring system (F0 = normal connective tissue; F1 = foci of perivenular and/or perisinusoidal fibrosis in zone 3; F2 = perivenular or pericellular fibrosis affecting zones 3 and 2; F3 = septal or bridging fibrosis; and F4 = cirrhosis).11,12
Liver Stiffness MeasurementThe l iver s t i ffness was measured
using Fibroscan (Echosens, Paris, France). Examination procedure was done according to the previous technical description.13 Ten successful measurements were performed on each patient. The success rate was calculated as the number of validated measurements divided by the total number of measurements. The results were expressed in kilopascals (kPa). The median value of successful measurements was considered representative of the liver stiffness in a given patient, according to the manufacturer’s recommendation (interquartile range [IQR] less than 30% of the median value and success rate >60%.14
Statistical AnalysesCharacteristics of the study subjects
were presented descriptively; continuous variables were expressed as mean + standard deviation or median (range) while categorical variables were presented as frequency and percentage. The association between liver steatosis and disease severity (serum alanine aminotransferase, serum HBV-DNA levels, fibrosis stage and necroinflammatory grade according to METAVIR Score) was analyzed statistically. Mean comparison was tested using the Mann-Whitney U test. A p value of <0.05 was considered significant. Statistical analysis was performed using the software Statistical Program for Social Studies version 13.0 for Windows PC (SPSS Inc, Chicago, IL, USA).
RESULTSThere were 174 cases eligible for analyses; 99
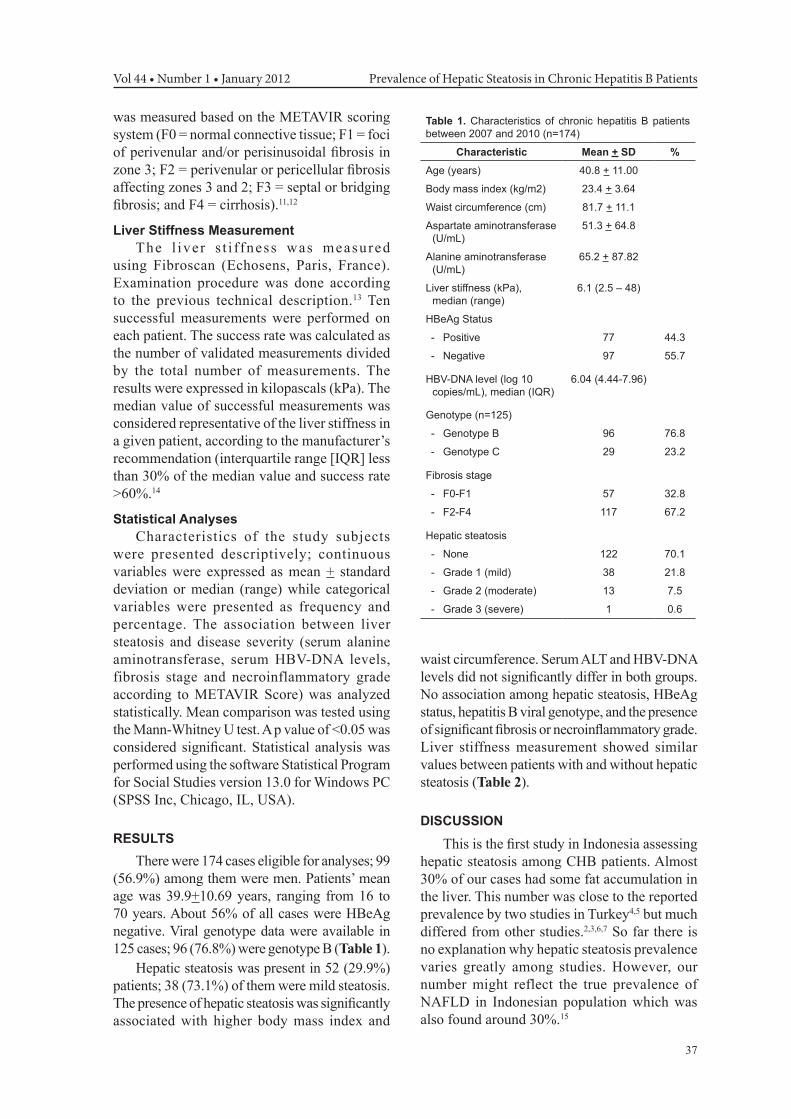
(56.9%) among them were men. Patients’ mean age was 39.9+10.69 years, ranging from 16 to 70 years. About 56% of all cases were HBeAg negative. Viral genotype data were available in 125 cases; 96 (76.8%) were genotype B (Table 1).
Hepatic steatosis was present in 52 (29.9%) patients; 38 (73.1%) of them were mild steatosis. The presence of hepatic steatosis was significantly associated with higher body mass index and
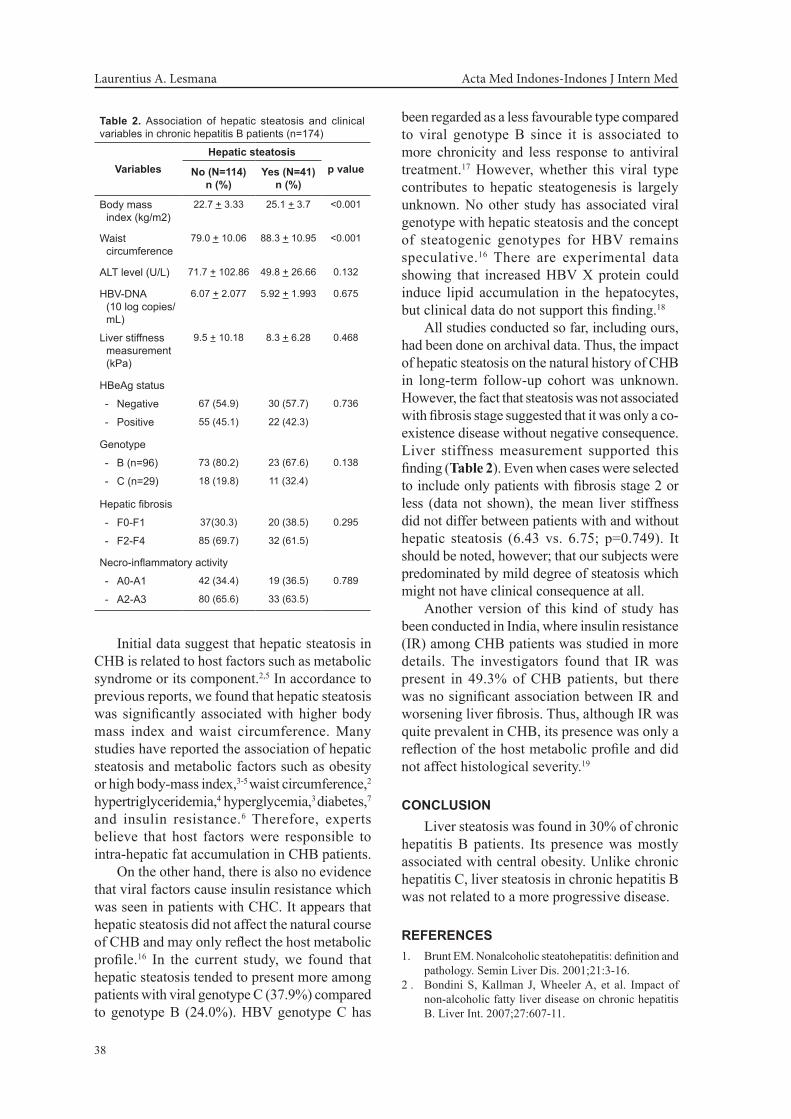
waist circumference. Serum ALT and HBV-DNA levels did not significantly differ in both groups. No association among hepatic steatosis, HBeAg status, hepatitis B viral genotype, and the presence of significant fibrosis or necroinflammatory grade. Liver stiffness measurement showed similar values between patients with and without hepatic steatosis (Table 2).
DISCUSSION
This is the first study in Indonesia assessing hepatic steatosis among CHB patients. Almost 30% of our cases had some fat accumulation in the liver. This number was close to the reported prevalence by two studies in Turkey4,5 but much differed from other studies.2,3,6,7 So far there is no explanation why hepatic steatosis prevalence varies greatly among studies. However, our number might reflect the true prevalence of NAFLD in Indonesian population which was also found around 30%.15
Table 1. Characteristics of chronic hepatitis B patients between 2007 and 2010 (n=174)
Characteristic Mean + SD %Age (years) 40.8 + 11.00
Body mass index (kg/m2) 23.4 + 3.64
Waist circumference (cm) 81.7 + 11.1
Aspartate aminotransferase (U/mL)
51.3 + 64.8
Alanine aminotransferase (U/mL)
65.2 + 87.82
Liver stiffness (kPa), median (range)
6.1 (2.5 – 48)
HBeAg Status
- Positive 77 44.3
- Negative 97 55.7
HBV-DNA level (log 10 copies/mL), median (IQR)
6.04 (4.44-7.96)
Genotype (n=125)
- Genotype B 96 76.8
- Genotype C 29 23.2
Fibrosis stage
- F0-F1 57 32.8
- F2-F4 117 67.2
Hepatic steatosis
- None 122 70.1
- Grade 1 (mild) 38 21.8
- Grade 2 (moderate) 13 7.5
- Grade 3 (severe) 1 0.6
38
Laurentius A. Lesmana Acta Med Indones-Indones J Intern Med
Initial data suggest that hepatic steatosis in CHB is related to host factors such as metabolic syndrome or its component.2,5 In accordance to previous reports, we found that hepatic steatosis was significantly associated with higher body mass index and waist circumference. Many studies have reported the association of hepatic steatosis and metabolic factors such as obesity or high body-mass index,3-5 waist circumference,2 hypertriglyceridemia,4 hyperglycemia,3 diabetes,7 and insulin resistance.6 Therefore, experts believe that host factors were responsible to intra-hepatic fat accumulation in CHB patients.
On the other hand, there is also no evidence that viral factors cause insulin resistance which was seen in patients with CHC. It appears that hepatic steatosis did not affect the natural course of CHB and may only reflect the host metabolic profile.16 In the current study, we found that hepatic steatosis tended to present more among patients with viral genotype C (37.9%) compared to genotype B (24.0%). HBV genotype C has
been regarded as a less favourable type compared to viral genotype B since it is associated to more chronicity and less response to antiviral treatment.17 However, whether this viral type contributes to hepatic steatogenesis is largely unknown. No other study has associated viral genotype with hepatic steatosis and the concept of steatogenic genotypes for HBV remains speculative.16 There are experimental data showing that increased HBV X protein could induce lipid accumulation in the hepatocytes, but clinical data do not support this finding.18
All studies conducted so far, including ours, had been done on archival data. Thus, the impact of hepatic steatosis on the natural history of CHB in long-term follow-up cohort was unknown. However, the fact that steatosis was not associated with fibrosis stage suggested that it was only a co-existence disease without negative consequence. Liver stiffness measurement supported this finding (Table 2). Even when cases were selected to include only patients with fibrosis stage 2 or less (data not shown), the mean liver stiffness did not differ between patients with and without hepatic steatosis (6.43 vs. 6.75; p=0.749). It should be noted, however; that our subjects were predominated by mild degree of steatosis which might not have clinical consequence at all.
Another version of this kind of study has been conducted in India, where insulin resistance (IR) among CHB patients was studied in more details. The investigators found that IR was present in 49.3% of CHB patients, but there was no significant association between IR and worsening liver fibrosis. Thus, although IR was quite prevalent in CHB, its presence was only a reflection of the host metabolic profile and did not affect histological severity.19
CONCLUSIONLiver steatosis was found in 30% of chronic
hepatitis B patients. Its presence was mostly associated with central obesity. Unlike chronic hepatitis C, liver steatosis in chronic hepatitis B was not related to a more progressive disease.
REFERENCES1. Brunt EM. Nonalcoholic steatohepatitis: definition and
pathology. Semin Liver Dis. 2001;21:3-16.2 . Bondini S, Kallman J, Wheeler A, et al. Impact of
non-alcoholic fatty liver disease on chronic hepatitis B. Liver Int. 2007;27:607-11.
Table 2. Association of hepatic steatosis and clinical variables in chronic hepatitis B patients (n=174)
VariablesHepatic steatosis
p valueNo (N=114)n (%)
Yes (N=41)n (%)
Body mass index (kg/m2)
22.7 + 3.33 25.1 + 3.7 <0.001
Waist circumference
79.0 + 10.06 88.3 + 10.95 <0.001
ALT level (U/L) 71.7 + 102.86 49.8 + 26.66 0.132
HBV-DNA (10 log copies/mL)
6.07 + 2.077 5.92 + 1.993 0.675
Liver stiffness measurement (kPa)
9.5 + 10.18 8.3 + 6.28 0.468
HBeAg status
- Negative 67 (54.9) 30 (57.7) 0.736
- Positive 55 (45.1) 22 (42.3)
Genotype
- B (n=96) 73 (80.2) 23 (67.6) 0.138
- C (n=29) 18 (19.8) 11 (32.4)
Hepatic fibrosis
- F0-F1 37(30.3) 20 (38.5) 0.295
- F2-F4 85 (69.7) 32 (61.5)
Necro-inflammatory activity
- A0-A1 42 (34.4) 19 (36.5) 0.789
- A2-A3 80 (65.6) 33 (63.5)

39
Vol 44 • Number 1 • January 2012 Prevalence of Hepatic Steatosis in Chronic Hepatitis B Patients
3. Thomopoulos KC, Arvaniti V, Tsamantas AC, et al. Prevalence of liver steatosis in patients with chronic hepatitis B: a study of associated factors and of relationship with fibrosis. Eur J Gastroenterol Hepatol. 2006;18:233-7.
4. Cindoruk M, Karakan T, Unal S, et al. Hepatic steatosis has no impact on the outcome of treatment in patients with chronic hepatitis B infection. J Clin Gastroenterol. 2007;41:513-7.
5. Altiparmak E, Koklu S, Yalinkilic M, et al. Viral and host causes of fatty liver in chronic hepatitis B. World J Gastroenterol. 2005;11:3056-9.
6. Wang CC, Hsu CS, Liu CJ, Kao JH, Chen DS. Association of chronic hepatitis B virus infection with insulin resistance and hepatic steatosis. J Gastroenterol Hepatol. 2008;23:779-82.
7. Tsochatzis E, Papatheodoridis GV, Manesis EK, et al. Hepatic steatosis in chronic hepatitis B develops due to host metabolic factors: a comparative approach with genotype 1 chronic hepatitis C. Dig Liver Dis. 2007;39:936-42.
8. Czaja AJ, Carpenter HA, Santrach PJ, Moore SB. Host- and disease-specific factors affecting steatosis in chronic hepatitis C. J Hepatol. 1998;29:198-206.
9. Starley BQ, Calcagno CJ, Harrison SA. Nonalcoholic fatty liver disease and hepatocellular carcinoma: a weighty connection. Hepatol. 2010;51:1820-32.
10. World Health Organization, Western Pacific Region. The Asia-Pacific perspective: redefining obesity and its treatment. International Association for the Study of Obesity, 2000.
11. The French METAVIR Cooperative Study Group. Intraobserver and interobserver variations in liver biopsy interpretation in patients with chronic hepatitis C. Hepatol. 1994;20:15-20.
12. Bedossa P, Poynard T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR cooperative study group. Hepatol. 1996;24:289-93.
13. Sandrin L, Fourquet B, Hasquenoph JM, et al. Transient elastrography: a new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med Biol. 2003;29:1705-13.
14. Castera L, Forn X, Alberti A. Non-invasive evaluation of liver fibrosis using transient elastography. J Hepatol. 2008;48:835-47.
15. Hasan I, Gani RA, Machmud R, et al. Prevalence and risk factors for nonalcoholic fatty liver in Indonesia. J Gastroenterol Hepatol. 2002;17(suppl):S154.
16. Fan JG, Chittur S. Hepatitis B and fatty liver: causal or coincidental? J Gastroenterol Hepatol. 2008;23:679-86.
17. Lin CL, Kao JH. The clinical implications of hepatitis B virus genotype: Recent advances. J Gastroenterol Hepatol. 2011;26(Suppl 1):123-30.
18. Kim KH, Shin HJ, Kim K, et al. Hepatitis B virus X protein induces hepatic steatosis via transcriptional activation of SREBP1 and PPAR gamma. Gastroenterol. 1997;132:1955-67.
19. Kumar M, Choudhury A, Manglik N, et al. Insulin resistance in chronic hepatitis B virus infection. Am J Gastroenterol. 2009;104:76-82.