Prevalence and Parkinson's · nal signs (resting tremor, rigidity, bradykine-sia, and impaired...
6
16ournal of Neurology, Neurosurgery, and Psychiatry 1997;62:10-15 Department of Epidemiology and Biostatistics, Erasmus University Medical School, Rotterdam, The Netherlands M C de Rijk M M B Breteler Department of Neurology, University Hospital Rotterdam, The Netherlands M C de Rijk INSERM Unite 360, H6pital de La Salpetriere, Paris, France C Tzourio A Alperovitch Department of Neurology, Pellegrin Hospital, University of Bordeaux II, France J F Dartigues INSERM Unite 360, University of Bordeaux II, France J F Dartigues Department of Neurology, University of Florence, Florence, Italy L Amaducci Department of Neurology, Santa Caterina Hospital, Girona, Spain S Lopez-Pousa Department of Neurology, University of Navarra, Pamplona, Spain J M Manubens-Bertran Department of Health Sciences Research, Mayo Clinic and Mayo Foundation, Rochester, Minnesota, USA W A Rocca Correspondence to: Dr A Alperovitch, INSERM Unite 360, Hopital La Salpetriere, 75651 Paris Cedex 13, France. Received 18 March 1996 and in revised form 15 July 1996 Accepted 27 August 1996 *AIl collaborators are listed at the end of the manuscript Prevalence of parkinsonism and Parkinson's disease in Europe: the EUROPARKINSON collaborative study M C de Rijk, C Tzourio, M M B Breteler, J F Dartigues, L Amaducci, S Lopez-Pousa, J M Manubens-Bertran, A Alperovitch, W A Rocca, for the EUROPARKINSON Study Group* Abstract Objectives-To assess and compare the prevalence of parkinsonism and Parkinson's disease in five European pop- ulations that were surveyed with similar methodology and diagnostic criteria. Methods-Joint analysis of five commu- nity surveys-Gironde (France), eight centres in Italy, Rotterdam (The Netherlands), Girona (Spain), and Pamplona (Spain)-in which subjects were screened in person for parkinson- ism. Overall, these surveys comprised 14 636 participants aged 65 years or older. Results-The overall prevalence (per 100 population), age adjusted to the 1991 European standard population, was 2-3 for parkinsonism and 1 6 for Parkinson's disease. The overall prevalence of parkin- sonism for the age groups 65 to 69, 70 to 74, 75 to 79, 80 to 84, and 85 to 89 years was respectively, 0-9, 1 5, 37, 50, and 5 1. The corresponding age specific figures for Parkinson's disease were 0-6, 1-0, 27, 36, and 3 5. After adjusting for age and sex, the prevalence figures did not differ sig- nificantly across studies, except for the French study in which prevalence was lower. Prevalence was similar in men and women. Overall, 24% of the subjects with Parkinson's disease were newly detected through the surveys. Conclusions-Prevalence of both parkin- sonism and Parkinson's disease increased with age, without significant differences between men and women. There was no convincing evidence for differences in prevalence across European countries. A substantial proportion of patients with Parkinson's disease went undetected in the general population. (7 Neurol Neurosurg Psychiatry 1997;62:10-15) Keywords: Parkinson's disease; parkinsonism; preva- lence Parkinson's disease is one of the most com- mon chronic neurodegenerative diseases in elderly people. Prevalence estimates of Parkinson's disease vary widely across studies and countries' but the interpretation of this geographic variation is hampered by differ- ences in methodology and diagnostic criteria. Consequently, it remains unclear whether a true variation exists. As part of the European Community Concerted Action on the Epidemiology of Parkinson's disease (EUROPARKINSON),2 we conducted a col- laborative comparison of five European preva- lence surveys of all types of parkinsonism, including Parkinson's disease. Methods EUROPARKINSON is a collaborative effort to study the prevalence, incidence, and deter- minants of Parkinson's disease in Europe comprising five studies, one each from France,3 Italy,4 and the Netherlands,5 and two from Spain. All five studies are community surveys of both independently living and insti- tutionalised elderly subjects 55 years of age or older, with a sample size of at least 1000. Table 1 summarises the characteristics of the five study populations. CASE FINDING PROCEDURES All studies used a two phase design to assess the prevalence of parkinsonism and Parkinson's disease. In phase 1, participants were screened in person using a symptom Table 1 Characteristics of the study populations Geographic Urban or Size of study Response Years of Population Investigators location rural population rate (%) Age (y) Type of sample survey France Dartigues Gironde region Urban and 3149 71 65 + Stratified random 1988-9 Gironde et al rural sample Italy Amaducci Eight provinces Urban and 4510 80 65 + Stratified random 1992-4 Eight centres et al across Italy rural sample The Netherlands Breteler City of Rotterdam, Urban 6969t 68 55 + Complete 1990-3 Rotterdam et al Ommoord district enumeration Spain Lopez-Pousa Group of villages Rural 1450 84 70 + Complete 1990-1 Girona et al in Girona province enumeration Spain Manubens- City of Pamplona Urban 1127 82 70 + Stratified random 1991 Pamplona Bertran et al sample tIn the present comparison, persons aged 55 to 64 years (n = 2569) who participated in the Rotterdam study were excluded. 10 on May 26, 2020 by guest. Protected by copyright. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.62.1.10 on 1 January 1997. Downloaded from
Transcript of Prevalence and Parkinson's · nal signs (resting tremor, rigidity, bradykine-sia, and impaired...

16ournal ofNeurology, Neurosurgery, and Psychiatry 1997;62:10-15
Department ofEpidemiology andBiostatistics, ErasmusUniversity MedicalSchool, Rotterdam,The NetherlandsM C de RijkM M B BretelerDepartment ofNeurology, UniversityHospital Rotterdam,The NetherlandsM C de RijkINSERM Unite 360,H6pital de LaSalpetriere, Paris,FranceC TzourioA AlperovitchDepartment ofNeurology, PellegrinHospital, University ofBordeaux II, FranceJ F DartiguesINSERM Unite 360,University ofBordeauxII, FranceJ F DartiguesDepartment ofNeurology, Universityof Florence, Florence,ItalyL AmaducciDepartment ofNeurology, SantaCaterina Hospital,Girona, SpainS Lopez-PousaDepartment ofNeurology, UniversityofNavarra, Pamplona,SpainJ M Manubens-BertranDepartment of HealthSciences Research,Mayo Clinic and MayoFoundation,Rochester, Minnesota,USAW A RoccaCorrespondence to:Dr A Alperovitch, INSERMUnite 360, Hopital LaSalpetriere, 75651 ParisCedex 13, France.
Received 18 March 1996and in revised form15 July 1996Accepted 27 August 1996
*AIl collaborators are listedat the end of the manuscript
Prevalence of parkinsonism and Parkinson'sdisease in Europe: the EUROPARKINSONcollaborative study
M C de Rijk, C Tzourio, M M B Breteler, J F Dartigues, L Amaducci, S Lopez-Pousa,J M Manubens-Bertran, A Alperovitch, W A Rocca, for the EUROPARKINSONStudy Group*
AbstractObjectives-To assess and compare theprevalence of parkinsonism andParkinson's disease in five European pop-
ulations that were surveyed with similarmethodology and diagnostic criteria.Methods-Joint analysis of five commu-nity surveys-Gironde (France), eightcentres in Italy, Rotterdam (TheNetherlands), Girona (Spain), andPamplona (Spain)-in which subjectswere screened in person for parkinson-ism. Overall, these surveys comprised14 636 participants aged 65 years or older.Results-The overall prevalence (per 100population), age adjusted to the 1991European standard population, was 2-3for parkinsonism and 1 6 for Parkinson'sdisease. The overall prevalence of parkin-sonism for the age groups 65 to 69, 70 to74, 75 to 79, 80 to 84, and 85 to 89 yearswas respectively, 0-9, 1 5, 37, 50, and 5 1.The corresponding age specific figures forParkinson's disease were 0-6, 1-0, 27, 36,and 3 5. After adjusting for age and sex,the prevalence figures did not differ sig-nificantly across studies, except for theFrench study in which prevalence waslower. Prevalence was similar in men andwomen. Overall, 24% of the subjects withParkinson's disease were newly detectedthrough the surveys.Conclusions-Prevalence of both parkin-sonism and Parkinson's disease increasedwith age, without significant differencesbetween men and women. There was no
convincing evidence for differences inprevalence across European countries. Asubstantial proportion of patients withParkinson's disease went undetected inthe general population.
(7 Neurol Neurosurg Psychiatry 1997;62:10-15)
Keywords: Parkinson's disease; parkinsonism; preva-lence
Parkinson's disease is one of the most com-mon chronic neurodegenerative diseases inelderly people. Prevalence estimates ofParkinson's disease vary widely across studiesand countries' but the interpretation of thisgeographic variation is hampered by differ-ences in methodology and diagnostic criteria.Consequently, it remains unclear whether atrue variation exists. As part of the EuropeanCommunity Concerted Action on theEpidemiology of Parkinson's disease(EUROPARKINSON),2 we conducted a col-laborative comparison of five European preva-
lence surveys of all types of parkinsonism,including Parkinson's disease.
MethodsEUROPARKINSON is a collaborative effortto study the prevalence, incidence, and deter-minants of Parkinson's disease in Europecomprising five studies, one each fromFrance,3 Italy,4 and the Netherlands,5 and twofrom Spain. All five studies are communitysurveys of both independently living and insti-tutionalised elderly subjects 55 years of age orolder, with a sample size of at least 1000.Table 1 summarises the characteristics of thefive study populations.
CASE FINDING PROCEDURESAll studies used a two phase design to assess
the prevalence of parkinsonism andParkinson's disease. In phase 1, participantswere screened in person using a symptom
Table 1 Characteristics of the study populations
Geographic Urban or Size of study Response Years ofPopulation Investigators location rural population rate (%) Age (y) Type of sample survey
France Dartigues Gironde region Urban and 3149 71 65 + Stratified random 1988-9Gironde et al rural sample
Italy Amaducci Eight provinces Urban and 4510 80 65 + Stratified random 1992-4Eight centres et al across Italy rural sample
The Netherlands Breteler City of Rotterdam, Urban 6969t 68 55 + Complete 1990-3Rotterdam et al Ommoord district enumeration
Spain Lopez-Pousa Group of villages Rural 1450 84 70 + Complete 1990-1Girona et al in Girona province enumeration
Spain Manubens- City of Pamplona Urban 1127 82 70 + Stratified random 1991Pamplona Bertran et al sample
tIn the present comparison, persons aged 55 to 64 years (n = 2569) who participated in the Rotterdam study were excluded.
10 on M
ay 26, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.62.1.10 on 1 January 1997. Dow
nloaded from
Prevalence ofparkinsonism and Parkinson's disease in Europe: the EUROPARKINSON collaborative study
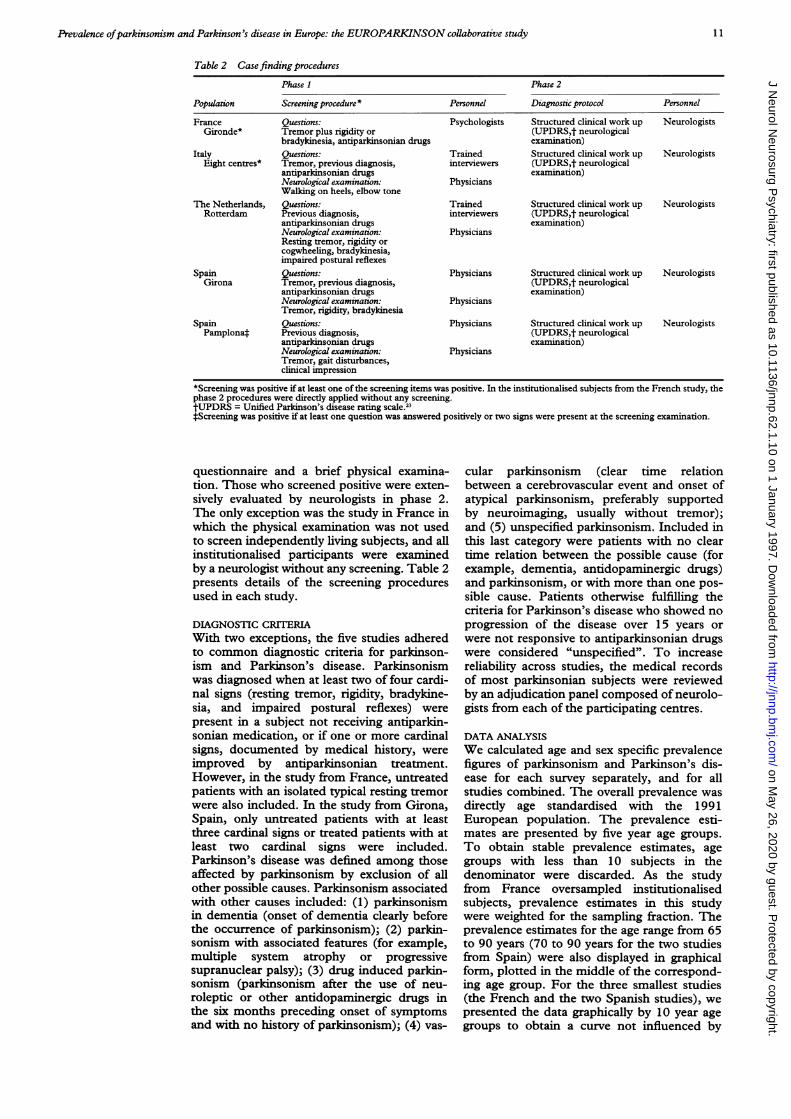
Table 2 Casefinding procedures
Phase I Phase 2
Population Screening procedure * Personnel Diagnostic protocol Personnel
France Questions: Psychologists Structured clinical work up NeurologistsGironde* Tremor plus rigidity or (UPDRS,t neurological
bradykinesia, antiparkinsonian drugs examination)Italy Questions: Trained Structured clinical work up Neurologists
Eight centres* Tremor, previous diagnosis, interviewers (UPDRS,t neurologicalantiparkinsonian drugs examination)Neurological examination: PhysiciansWalking on heels, elbow tone
The Netherlands, Questions: Trained Structured clinical work up NeurologistsRotterdam Previous diagnosis, interviewers (UPDRS,t neurological
antiparkinsonian drugs examination)Neurological examination: PhysiciansResting tremor, rigidity orcogwheeling, bradykinesia,impaired postural reflexes
Spain Questions: Physicians Structured clinical work up NeurologistsGirona Tremor, previous diagnosis, (UPDRS,t neurological
antiparkinsonian drugs examination)Neurological examination: PhysiciansTremor, rigidity, bradykinesia
Spain Questions: Physicians Structured clinical work up NeurologistsPamplonat Previous diagnosis, (UPDRS,t neurological
antiparkinsonian drugs examination)Neurological examination: PhysiciansTremor, gait disturbances,clinical impression
*Screening was positive if at least one of the screening items was positive. In the institutionalised subjects from the French study, thephase 2 procedures were directly applied without any screening.tUPDRS = Unified Parkinson's disease rating scale.23*Screening was positive if at least one question was answered positively or two signs were present at the screening examination.
questionnaire and a brief physical examina-tion. Those who screened positive were exten-sively evaluated by neurologists in phase 2.The only exception was the study in France inwhich the physical examination was not usedto screen independently living subjects, and allinstitutionalised participants were examinedby a neurologist without any screening. Table 2presents details of the screening proceduresused in each study.
DIAGNOSTIC CRITERIAWith two exceptions, the five studies adheredto common diagnostic criteria for parkinson-ism and Parkinson's disease. Parkinsonismwas diagnosed when at least two of four cardi-nal signs (resting tremor, rigidity, bradykine-sia, and impaired postural reflexes) werepresent in a subject not receiving antiparkin-sonian medication, or if one or more cardinalsigns, documented by medical history, wereimproved by antiparkinsonian treatment.However, in the study from France, untreatedpatients with an isolated typical resting tremorwere also included. In the study from Girona,Spain, only untreated patients with at leastthree cardinal signs or treated patients with atleast two cardinal signs were included.Parkinson's disease was defined among thoseaffected by parkinsonism by exclusion of allother possible causes. Parkinsonism associatedwith other causes included: (1) parkinsonismin dementia (onset of dementia clearly beforethe occurrence of parkinsonism); (2) parkin-sonism with associated features (for example,multiple system atrophy or progressivesupranuclear palsy); (3) drug induced parkin-sonism (parkinsonism after the use of neu-roleptic or other antidopaminergic drugs inthe six months preceding onset of symptomsand with no history of parkinsonism); (4) vas-
cular parkinsonism (clear time relationbetween a cerebrovascular event and onset ofatypical parkinsonism, preferably supportedby neuroimaging, usually without tremor);and (5) unspecified parkinsonism. Included inthis last category were patients with no cleartime relation between the possible cause (forexample, dementia, antidopaminergic drugs)and parkinsonism, or with more than one pos-sible cause. Patients otherwise fulfilling thecriteria for Parkinson's disease who showed noprogression of the disease over 15 years orwere not responsive to antiparkinsonian drugswere considered "unspecified". To increasereliability across studies, the medical recordsof most parkinsonian subjects were reviewedby an adjudication panel composed of neurolo-gists from each of the participating centres.
DATA ANALYSISWe calculated age and sex specific prevalencefigures of parkinsonism and Parkinson's dis-ease for each survey separately, and for allstudies combined. The overall prevalence wasdirectly age standardised with the 1991European population. The prevalence esti-mates are presented by five year age groups.To obtain stable prevalence estimates, agegroups with less than 10 subjects in thedenominator were discarded. As the studyfrom France oversampled institutionalisedsubjects, prevalence estimates in this studywere weighted for the sampling fraction. Theprevalence estimates for the age range from 65to 90 years (70 to 90 years for the two studiesfrom Spain) were also displayed in graphicalform, plotted in the middle of the correspond-ing age group. For the three smallest studies(the French and the two Spanish studies), wepresented the data graphically by 10 year agegroups to obtain a curve not influenced by
1 1 on M
ay 26, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.62.1.10 on 1 January 1997. Dow
nloaded from

Rijk, Tzourio, Breteler, Dartigues, Amaducci, Lopez-Pousa, et al
Table 3 Age and sex specific prevalence (per 100 population) ofparkinsonism * and overall age and sex adjustedprevalence ratios
Age group (y)jt Prevalenceratio
Population 65-69 70-74 75-79 80-84 85-89 90-94 95-99 (95% CI)
France Women 0 6 1.2 2-8 3-2 3-8 5-3 28-6Girondet (4/667) (8/656) (14/507) (16/496) (13/340) (6/113) (8/28) 0 7 (0 5-0 9)
Men 0-8 0-6 2-1 3-2 3 9 4-5(5/641) (3/473) (6/285) (6/190) (5/129) (1/22) -
Italy Women 1 4 2-4 4-1 5-7Eight centres (8/568) (13/538) (22/541) (31/542)
Men 1.2 1-8 5-3 7 0 - - - 1-3 (1 0-1 7)(7/585) (11/602) (30/571) (39/555)
The Women 0-9 1-3 3-7 5-6 6-9 4-4 10 0Netherlands (6/705) (9/684) (20/544) (22/396) (17/245) (4/91) (2/20) Reference
Rotterdam Men 0-8 2-1 2-9 5-6 5-1 4-5 _(5/613) (10/477) (10/341) (10/180) (4/79) (1/22) -
Spain Women - 1-5 5 0 4-1 4-4 500Girona (5/328) (13/256) (7/170) (4/90) (1/20)
Men - 0-4 4-0 2-6 6-7 - 1-0 (0-7-1-3)(1/262) (6/150) (3/114) (3/45) - -
Spain Women - 1-3 3-8 2-0 3-6 6 8Pamplona (1/75) (6/159) (3/150) (5/137) (3/44)
Men - 4-2 2-6 6-6 7 0 8-9 - 0 9 (0-6-1-3)(3/71) (4/152) (10/152) (10/142) (4/45)
Total Women 0 9 1-6 3-7 4-5 4-8 5-2 29-8(18/1940) (36/2281) (75/2007) (79/1754) (39/812) (14/268) (10/48)
Men 0 9 1-5 3-7 5-7 5-6 6 7(17/1839) (28/1885) (56/1499) (68/1191) (22/395) (6/89)
*Numbers in parentheses indicated the actual numerator and denominator.tDashes indicate age groups that were not included in the survey or for which prevalence estimates were not computed because ofsmall numbers.tPrevalence estimates of the French study were weighted according to the sampling procedure; the denominators reported in thetable were artificially computed by dividing the observed number of cases by the weighted prevalence.
unstable estimates due to small numbers. Thelikelihood ratio test was performed to test forheterogeneity across centres. To investigatewhether age and sex adjusted prevalence fig-ures of Parkinson's disease differed across
studies, we calculated prevalence ratios andthe corresponding 95% confidence intervals(95% CIs) by Poisson regression analyses withthe Rotterdam study (the largest) as referencefor comparison. We also used Poisson regres-sion analysis to determine whether the overallage adjusted prevalence was significantly dif-ferent between men and women.
ResultsThe overall study population comprised17 205 elderly subjects, of whom 14 636 were
65 years of age and older (table 1). Theresponse rates ranged from 68% in the surveyfrom The Netherlands to 84% for the surveyfrom Girona, Spain (table 1). Tables 3 and 4and figs 1 and 2 show prevalence values andthe prevalence ratios of parkinsonism andParkinson's disease for the individual studiesand overall. The overall age standardisedprevalence (per 100 population) in subjects 65years of age or older was 2 3 for parkinsonism
Table 4 Age and sex specific prevalence (per 100 population) ofParkinson's disease * and overall age and sex adjustedprevalence ratios
Age group (y)t Prevalenceratio
Population 65-69 70-74 75-79 80-84 85-89 90-94 95-99 (95% CI)
France Women 0-2 0-2 1-8 1.0 2-2 1-9 7-1Girondet (1/500) (2/974) (9/487) (5/493) (7/324) (2/113) (2/28)
Men 0 7 0-5 1-3 2-9 1-6 4.5 - 04 (0-3-0 6)(4/556) (2/399) (4/308) (5/173) (2/125) (1/22)
Italy Women 0-9 2-2 3-0 41 - -Eight centres (5/568) (12/538) (16/541) (22/542)
Men 0 5 1.0 3-7 5 0 - - - 1.2 (0-9-1 6)(3/585) (6/602) (21/571) (28/555)
The Women 0-6 1.0 2-4 4-8 5-3 3.3 5 0Netherlands (4/705) (7/684) (13/544) (19/396) (13/245) (3/91) (1/20) Reference
Rotterdam Men 0-8 1-7 2-3 3-9 3-8(5/613) (8/477) (8/341) (7/180) (3/79) (0/22) -
Spain Women - 1-5 4-7 3-5 4.4 5 0Girona (5/328) (12/256) (6/170) (4/90) (1/20) -
Men - 0 4 4-0 2-6 6-7 - 0 7 (0-5-1-1)(1/262) (6/150) (3/114) (3/45) - -
Spain Women - 3-1 1-3 2-2 2-2Pamplona (0/75) (5/159) (2/150) (3/137) (1/44)
Men - 1-4 1-3 4-6 4-9 2-2 - 1 1 (0-8-1-6)(1/71) (2/152) (7/152) (7/142) (1/45)
Total Women 0-6 1 0 2-8 3-1 3-4 2-6 6 3(10/1773) (26/2599) (55/1987) (54/1751) (27/796) (7/268) (3/48)
Men 0 7 1.0 2-7 4-3 3-8 2-2(12/1745) (18/1811) (41/1522) (50/1174) (15/391) (2/89) -
*Numbers in parentheses indicate the actual numerator and denominator.tDashes indicate age groups that were not included in the survey or for which prevalence estimates were not computed because ofsmall numbers.tPrevalence estimates of the French study were weighted according to the sampling procedure; the denominators reported in the tablewere artificially computed by dividing the observed number of cases by the weighted prevalence.
12 on M
ay 26, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.62.1.10 on 1 January 1997. Dow
nloaded from

Prevalence ofparkinsonism and Parkinson's disease in Europe: the EUROPARKINSON collaborative study
Figure 1 (A) Agespecific prevalence, for bothsexes combined, ofparkinsonism in fiveEuropean surveys. Theprevalence estimates areplotted in the middle of thecorresponding age groups:for the studies from Italyand The Netherlands byfive year age groups, forthe studies from Franceand Spain by 10 year agegroups. (B) Overall agespecific prevalence forwomen and men.
6Italyc0.7 5
0.
co4L
00
C-C';6
a)
2
c
> 1
France
65 70 75 80 85 90Age (y)
BMen
Women
65 70 75 80 85 90Age (y)
and 1 6 for Parkinson's disease. Prevalencefigures of parkinsonism increased from 0 9 forthose aged 65 to 69 years to 5-1 for those aged85 to 89 years. The prevalence figures forParkinson's disease increased from 0-6 forthose aged 65 to 69 years to 3-5 for those aged85 to 89 years. The prevalence of both parkin-sonism and Parkinson's disease increased withage, after a similar pattern in all studies, withno decrease in extreme ages. After adjustmentfor age and sex, there were no significant dif-ferences across surveys except for the Frenchstudy, in which prevalences were consistentlylower. The likelihood ratio test showed hetero-geneity across centres when the survey fromFrance was included (P < 0001). When thesurvey from France was excluded, there wereno statistically significant differences acrosscentres (P = 0-21). Figures 1 and 2 show theoverall age and sex specific prevalences ofparkinsonism and Parkinson's disease. Theprevalences for men and women were not sig-nificantly different; for parkinsonism thewomen:men ratio was 0-96 (95% CI:0-80-1-16), and for Parkinson's disease 0 94(95% CI: 0-75-1-18).The frequency distribution by type of
parkinsonism for all studies combined was asfollows: Parkinson's disease 68%, parkinson-ism in dementia 9%, drug induced parkinson-ism 5%, parkinsonism with associated features1 %, vascular parkinsonism 3%, and unspeci-
fied parkinsonism 14%. The proportion ofsubjects with Parkinson's disease who werenewly diagnosed through the surveys variedfrom 11% in France and 13% in TheNetherlands, to 26% in Girona, Spain, 31% inItaly, and 52% in Pamplona, Spain. In all sur-veys, the percentage of newly diagnosedpatients with Parkinson's disease increasedwith age. For all studies combined, this per-centage increased from 18% for those aged 65to 70 years to 36% for those aged 80 to 85years.
DiscussionMETHODOLOGICAL CONSIDERATIONSThe striking variation in prevalence estimatesof Parkinson's disease reported from variousstudies and different populations, rangingfrom 10 to 405 cases per 100 000 population,'may be caused, partly or completely, by varia-tion in the methods used. The three mostimportant methodological elements are thecase finding strategy,6 the diagnostic criteriafor parkinsonism and Parkinson's disease, andthe degree of coverage of the target population(response rate).
Studies that rely on existing medical recordsexclude from the prevalence estimate thosepatients who failed to seek medical attentionfor their symptoms, those who were incor-rectly diagnosed, and those whose records
Figure 2 (A) Agespecific prevalence, for bothsexes combined, ofParkinson's disease in fiveEuropean surveys. Theprevalence estimates areplotted in the middle of thecorresponding age groups:for the studies from Italyand The Netherlands byfive year age groups, forthe studiesfrom Franceand Spain by 10 year agegroups. (B) Overall agespecific prevalence forwomen and men.
c0
Cu
0.
0.0
r-
0)Qm
C.)CD
a)gu
5
4
3
2
1
o
A
TheNetherlands
Spain,/,' * Girona
Italy / ,aSpain,Pamplona
/'~/France
65 70 75 80 85 90Age (y)
C
0
0._.-
Q
030
CL'
C)C'6
>
2
Cu
CD
a-
Men
Women
65 70 75 80 85 90Age (y)
7' A
6
5
4
3
2
C
._
00.m
0
Q
Cl'
a
CuClSC)
C)gCuCu
13
I
on May 26, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.62.1.10 on 1 January 1997. D
ownloaded from

Rijk, Tzourio, Breteler, Dartigues, Amaducci, Lopez-Pousa, et al
were not retrieved. The alternative case find-ing approach involves the direct or indirectcontact of all subjects in the study populationto assess their disease status. This approachshould eliminate the underestimation of preva-lence and should be more suitable for interna-tional comparisons as it reduces the variationdue to differences in access to and quality ofmedical care in various populations.
Our study is the first comparison of resultsfrom several prevalence surveys of Parkinson'sdisease which used similar case finding strat-egy and diagnostic criteria. Although the fiveEUROPARKINSON surveys were notdesigned as a multicentre study, the investiga-tors met and exchanged their methods anddata collection instruments early in the plan-ning of the surveys. Therefore, we havereached an unprecedented level of method-ological homogeneity. To increase compara-bility across centres, the medicaldocumentation of most parkinsonian patientsunderwent a centralised review by an adjudi-cation panel.
Despite this effort to homogenise ourmethodology, the five surveys still presentsome variation. The screening procedureswere different in number of items tested andpersonnel involved. In the French study, nophysical examination was performed as part ofthe screening, whereas in the four remainingstudies it was. Also, the use of diagnostic crite-ria for parkinsonism varied somewhat with abroadening of the criteria in the French studyand a restriction in the Girona study. Therewere variations in the differential diagnosis ofparkinsonism by specific aetiology.Parkinson's disease represented 70% to 96%of all parkinsonisms in Italy, The Netherlands,and Girona, Spain, whereas Parkinson's dis-ease was only 59% of all parkinsonisms inPamplona, Spain, and 48% in France. A largepercentage of parkinsonian subjects in theFrench study had concurrent dementia withno clear time relation between onset ofdementia and onset of extrapyramidal signs.These subjects were classified as "unspecifiedparkinsonism". In addition, a high percentageof subjects in France were receiving anti-dopaminergic agents, and were classified as"drug induced parkinsonism". It was againdifficult in these patients to isolate the role ofantidopaminergic drugs from the independentoccurrence of Parkinson's disease.
In a two phase survey, failure to study alarge segment of the target population (non-response) due to refusal or other obstaclesmay cause an underestimation or an overesti-mation of prevalence.7 Unfortunately, the fivesurveys had different response rates, and theimpact of this variation on our findings isunknown.
AGEThe prevalence of parkinsonism andParkinson's disease increased with age in allfive surveys for both men and women, with nodecrease at higher ages. This suggests that theprevalence, and probably also the incidence, ofParkinson's disease continues to increase
beyond the age 85 or 90 years. Various othersurveys based on direct68 or indirect9 10 contactof all subjects in the population also showed acontinuing increase in the prevalence ofParkinson's disease with age. By contrast,other prevalence studies based on existingmedical records showed a peak in prevalencefollowed by a decline among the oldest old."1-14We speculate that these contrasting patternsare due to the underascertainment ofParkinson's disease among older subjectswhich occurs when patients are detectedthrough medical records only. Our five surveysshowed that the percentage of subjects withParkinson's disease who had not been previ-ously diagnosed increases with advancing agein the general population.
SEXMost prevalence studies that indicated higherprevalences of Parkinson's disease inmen82 517 or in women, Il4 were based on
medical records, whereas most surveys with apersonal screening for parkinsonism, such asour study, found no significant sex differ-ences.6 9 10 18 These findings suggest that therisk of Parkinson's disease is equal in men andwomen, but the referral to medical servicesvaries by sex across populations.
GEOGRAPHIC COMPARISONIt has been postulated that geographic differ-ences in the prevalence of Parkinson's diseasemay yield aetiological clues.'9-2' After adjustingfor the effect of age and sex using Poissonregression models, our data did not suggestsignificant differences in prevalence acrossEuropean countries, with the exception of theFrench survey. Morgante et al showed that asubstantial proportion of parkinsonian sub-jects go undetected when only a questionnairescreening, as in the French survey, is used.6We think that the differences in methodologyand in diagnostic criteria discussed may atleast partly account for the lower prevalenceestimates of Parkinson's disease in the Frenchsurvey. Therefore, our overall impression isthat there is no evidence for the prevalence ofParkinson's disease being different acrossEuropean countries.
Although the overall prevalences were similarin our five surveys, there was a wide variation inthe percentage of newly diagnosed patientswith Parkinson's disease who were detectedthrough the screening. This may be due to dif-ferences in referral pattern and in access tomedical services across the four countries.These findings emphasise the importance of adirect screening when assessing the prevalenceof Parkinson's disease.
Comparing our findings with those fromother recent surveys based on a similar casefinding approach, we found striking similari-ties with the Sicilian study.6 This comparisonstrengthens our overall impression of limitedgeographic variation in prevalence when meth-ods are homogeneous.Some authors reported that persons living
in a rural environment have a higher risk ofdeveloping Parkinson's disease than persons
14
on May 26, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.62.1.10 on 1 January 1997. D
ownloaded from

Prevalence ofparkinsonism and Parkinson's disease in Europe: the EUROPARKINSON collaborative study
living in towns, and suggested an environmen-tal cause for Parkinson's disease.I822 In ourstudy, the more rural population (Girona) ormixed populations (France, Italy) did not havea higher prevalence of Parkinson's diseasethan the more urban populations (Pamplona,Rotterdam).
ConclusionsTo allow comparisons across countries, aneffort was made in EUROPARKINSON toincrease the homogeneity of case finding strat-egy and diagnostic criteria in five Europeansurveys on the prevalence of Parkinson's dis-ease. Allowing for the French study-whichdeviated somewhat from the common meth-ods-our findings suggest that the prevalenceof Parkinson's disease is similar acrossEuropean countries. The prevalence of bothparkinsonism and Parkinson's diseaseincreases steeply with age, and is similar inmen and women.
This research was supported by theEuropean Community Concerted Action"Incidence and Risk Factors for Parkinson'sdisease: a European Collaborative Study"(Contract BMH1 CT92 1101).
We thank Dr Paul G H Mulder for his advice on statistics.
List of all collaborators ofEUROPARKINSONFrance: JF Dartigues, F Tison, L Letenneur, P Henry(Bordeaux); A Alperovitch, C Tzourio, M Gautier(Paris).
Italy: A Amaducci, M Baldereschi, D Inzitari, AGhetti (Florence); F Grigoletto, L Battistin, G Enzi(Padova); A Capurso, P Livrea (Barn); L Motta(Catania); S Bonaiuto (Fermo); C Loeb, C Gandolfo(Genova); N Canal (Milano); F Rengo (Napoli).The Netherlands (Rotterdam): MMB Breteler, MC
de Rijk, GA Graveland, A Ott, FGA van der Meche, AHofman.
Spain (Girona): S Lopez-Pousa, J Vilalta-Franck, JLlinis-Regla, M Lozano-Gallego.
Spain (Pamplona): JM Martinez-Lage, JMManubens-Bertran, R Larumbe, J Muruzabal, PMartinez-Lage, C Guarch, T Urrutia, P Sarrasqueta, FLacruz, P Quesada, C Lopez.USA (Rochester): WA Rocca.
1 Zhang Z, Roman GC. Worldwide occurrence ofParkinson's disease: an updated review. Neuro-epidemiology 1993;12:195-208.
2 Breteler MMB, Alperovitch A, Lopez-Pousa S, Manubens-Bertran JM, Rocca WA. EUROPARKINSON: aEuropean concerted action on incidence and risk factors
for Parkinson's disease [abstract]. Neuroepidemiology1993;12:17.
3 Tison F, Dartigues JF, Dubes L, Zuber M, Alperovitch A,Henry P. Prevalence of Parkinson's disease in the elderly:a population study in Gironde, France. Acta Neurol Scand1994;90:111-5.
4 Maggi S, Zucchetto M, Grigoletto F, Baldereschi M,Candelise L, Scarpini E, et al. The Italian LongitudinalStudy on Aging (ILSA): design and methods. Aging ClinExp Res 1994;6:463-71.
5 de Rijk MC, Breteler MMB, Graveland GA, Ott A,Grobbee DE, van der Meche FGA, et al. Prevalence ofParkinson's disease in the elderly: the Rotterdam Study.Neurology 1995;45:2143-6.
6 Morgante L, Rocca WA, Di Rosa AE, De Domenico P,Grigoletto F, Meneghini F, et al. Prevalence ofParkinson's disease and other types of parkinsonism: adoor-to-door survey in three Sicilian municipalities.Neurology 1992;42:1901-7.
7 Grigoletto F, Anderson DW, Rocca WA, Meneghini F,Morgante L, Reggio A, et al. Attrition and use of proxyrespondents and auxiliary information in the SicilianNeuroepidemiologic Study. Am J Epidemiol 1994;139:219-28.
8 Li SC, Schoenberg BS, Wang CC, Wang C, Cheng X, RuiD, et al. A prevalence survey of Parkinson's disease andother movement disorders in the People's Republic ofChina. Arch Neurol 1985:42:655-7.
9 Schoenberg BS, Anderson DW, Haerer AF. Prevalence ofParkinson's disease in the biracial population of CopiahCounty, Mississippi. Neurology 1985;35:841-5.
10 Barucha NE, Barucha EP, Barucha AE, Bhise AV,Schoenberg BS. Prevalence of Parkinson's disease in theParish Community of Bombay, India. Arch Neurol 1988;45:1321-3.
11 Marttila RJ, Rinne UK. Epidemiology of Parkinson's dis-ease in Finland. Acta Neurol Scand 1976;53:81-102.
12 Rosati G, Granieri E, Pinna L, Aiello I, Tola R, DeBastiani P, et al. The risk of Parkinson disease inMediterranean people. Neurology 1980;30:250-5.
13 D'Alessandro R, Gamberini G, Granieri E, Benassi G,Naccarato S, Manzaroli D. Prevalence of Parkinson'sdisease in the Republic of San Marino. Neurology 1987;37:1679-82.
14 Okada K, Kobayashi S, Tsunematsu T. Prevalence ofParkinson's disease in Izumo City, Japan. Gerontology1990;36:340-4.
15 Mutch WJ, Dingwall-Fordyce I, Downie AW, Paterson JG,Roy SK. Parkinson's disease in a Scottish city. BMJ'1986;292:534-6.
16 Mayeux R, Denaro J, Hemenegildo N, Marder K, Tang M,Cote U, et al. A population-based investigation ofParkinson's disease with and without dementia. ArchNeurol 1992;49:492-7.
17 Mayeux R, Marder K, Cote U, Denaro J, Hemenegildo N,Mejia H, et al. The frequency of idiopathic Parkinson'sdisease by age, ethnic group, and sex in northemManhattan. AmJ Epidemiol 1995;142:820-7.
18 Ho SC, Woo J, Lee CM. Epidemiologic study ofParkinson's disease in Hong Kong. Neurology 1989;39:1314-8.
19 Schoenberg BS, Osuntokun BO, Adeuja AOG, Bademosi0, Nottidge V, Anderson DW, et al. Comparison of theprevalence of Parkinson's disease in black populations inthe rural United States and in rural Nigeria: door-to-doorcommunity studies. Neurology 1988;38:645-6.
20 Lux WE, Kurtzke JF. Is Parkinson's disease acquired?Evidence from geographic comparison with multiple scle-rosis. Neurology 1987;37:467-71.
21 Kurtzke JF, Goldberg ID. Parkinsonism death rates byrace, sex, and geography. Neurology 1988;38:1558-61.
22 Koller W, Vetere-Overfield B, Gray C, Alexander C, ChinT, Dolezal J, et al. Environmental risk factors inParkinson's disease. Neurology 1990;40:1218-21.
23 Fahn S, Elton RL, Members of the UPDRS DevelopmentCommittee. Unified Parkinson's disease rating scale. In:Fahn S, Marsden CD, Calne DB, eds. Recent develop-ments in Parkinson's disease. Vol 2. Florham Park, NJ:MacMillan Healthcare information, 1987:153-63.
15
on May 26, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.62.1.10 on 1 January 1997. D
ownloaded from