
Pressure Injuries: Prevention That Works - NPUAP€¦ · incorporate into your PIP program. ......
18
3/11/2017 1 ©2017 National Pressure Ulcer Advisory Panel | www.npuap.org Pressure Injuries: Prevention That Works Joyce Pittman PhD, ANP-BC, FNP-BC, CWOCN Indiana University Health Indianapolis, IN [email protected] Ann N. Tescher, APRN CNS, CCRN, CWCN, FCCM Clinical Nurse Specialist – Surgical/Trauma/CV Surgery ICU, Hyperbaric Therapy, Vascular Wound Center Mayo Clinic, Rochester MN [email protected] Pressure Injuries: Prevention That Works Disclosures: Joyce Pittman • AACN grant recipient- Research Impact grant Unavoidable pressure injuries in critical care • Smith & Nephew- consultant • JWOCN Deputy Editor Ann Tescher None
Transcript of Pressure Injuries: Prevention That Works - NPUAP€¦ · incorporate into your PIP program. ......

3/11/2017
1
©2017 National Pressure Ulcer Advisory Panel | www.npuap.org
Pressure Injuries: Prevention That Works
Joyce Pittman PhD, ANP-BC, FNP-BC, CWOCN
Indiana University Health
Indianapolis, IN
Ann N. Tescher, APRN CNS, CCRN, CWCN, FCCM
Clinical Nurse Specialist – Surgical/Trauma/CV Surgery
ICU, Hyperbaric Therapy, Vascular Wound Center
Mayo Clinic, Rochester MN
Pressure Injuries: Prevention That Works
Disclosures:
Joyce Pittman
• AACN grant recipient- Research Impact grant
Unavoidable pressure injuries in critical care
• Smith & Nephew- consultant
• JWOCN Deputy Editor
Ann Tescher
None

3/11/2017
2
Objectives
• Describe components of a sustainable
pressure injury program.
• Name 2 exemplars of successful
Pressure Injury prevention programs.
• Describe innovative methods to
incorporate into your PIP program.
Essentials Components of Pressure Injury (PI) Prevention
1. Pressure injury admission assessment
2. Daily pressure injury risk assessment
3. Daily (routine) skin assessment
4. Moisture management
5. Maximize nutrition
6. Minimize pressure
Educate staff, provider, patient, family
3/11/2017
3
Essential Components of PI Prevention
1. Evaluate the individual’s clinical condition and
pressure ulcer risk factors
2. Define and implement interventions that are
consistent with individual needs, goals and
recognized standards of practice
3. Monitor and evaluate the impact of the
interventions
4. Revise the approaches as appropriate
(NPUAP, 2010; CMS)
SWOT Model
• Strengths
• Weaknesses
• Opportunities
• Threats
3/11/2017
4
Structure- Process- Outcomes
To achieve and sustain the lowest possible
HAPI rates, you should ask:
1. What structure needs to be in place
2. What process should be implemented
and monitored
3. How should outcomes be measured and
reports
Pressure Injuries: Prevention That Works
STRUCTURE- PROCESS- OUTCOMES
4 Magnet Model Domains:
1. Transformational leadership
2. Structural empowerment
3. Exemplary professional practice
4. New knowledge; innovation and improvement.
Successful implementation of these elements yields measurable positive outcomes (W. V. Padula, Mishra MK, Makic MB, Valuck RJ, 2014 Apr).

3/11/2017
5
Transformational Leadership
• Key leader stakeholder (VP) appointed to
facilitate/support PIP initiatives
• PIP clinical program facilitator
appointed/designated
• Sets clear expectations for benchmarking,
outcomes, and accountability.
• Removes barriers
Transformational Leadership
• Clear reporting structure and bidirectional
communication for the PIP program in the
nursing organizational framework identified.
Board level (Safety and Risk Board) Nurse Executive
Council PPS committee WOC/PIP committee Facility
PPC Facility PIP Unit
Time and resources for group meetings and projects is
supported
Supports use of FTE to do the work- system facility
unit, and communicates those expectations to all levels.
Supports interdisciplinary team development.

3/11/2017
6
Structural empowerment
• PIP Team established: system, facility, unit level, multi-
disciplinary Bi-directional reporting/ accountability
Multidisciplinary: WOC, CNS, RN, RT, PT, RD, Risk, Social Work,
Educator (staff/patient), Ethics, Supply Chain, IT
Continuum of care:- Acute care, Home Care, Long term care, LTAC
Recognition of excellence- system, facility, unit, individual
PIP Member role/responsibilities/expectations was established and
approved by NEC
•PIP Education expectations/opportunities- Embedded annual/orientation staff education/competencies,
WTA program
CAP
• Conference presentations/attendance
Exemplary professional Practice
• Evidence-based PIP protocol, plan of care, order sets developed and
embedded into EMR.
• PIP is hard-wired into care at the bedside but also ancillary areas-
OR, ED, transportation- safe handoff, order sets, triggers, etc..
• HAPI prevalence/processes benchmarking Monthly rather than
quarterly. Transparent at unit level.
• PI integration into IT- quality data reports, triggers, e-measures– EMR design triggers specific nursing interventions based on risk assessment
– EMR generates daily/real time PU occurrences
• Moving toward meaningful data- incidence rather than prevalence
• Culture of Safety through standardized Root Cause Analysis process – NPUAP RCA template
– Avoidable versus unavoidable HAPI

3/11/2017
7
Assess skin
Complete Braden
risk and skin
assessment
Implement skin/
wound
interventions/
orders based on
risk
Evaluate skin
based on
implemented
interventions
Risk or skin
integrity
changed
Continue skin plan
of care
Document POA
within 24 hrsNo
Process Measures:
1. 100% skin assessment completed and documented POA within 24 hours
2. 100% accuracy with wound order set completion based on risk
Standard Work Requirement (discussed in huddles/bedside report, etc)
1. Skin wound orderset included in admission packet and placed on every chart
2. Assess risk with Braden and anytime change in status
3. Complete skin wound orderset based on risk
Pressure Ulcer Prevention
Do No Harm through Elimination of Hosptial Acquired Pressure Ulcers
Braden < 18 or
POA
Initiate Phase 1
and 2 of skin care
prevention PPOC
Risk or skin
integrity
changed
Continue PU
prevention plan of
care
No
No
Initiate Phase 1
and 2 of skin care
prevention PPOC
Evaluate skin
Surface selection
Keep turning
Incontinence/
moisture
management
Nutrition
Yes
Yes
3/11/2017
8
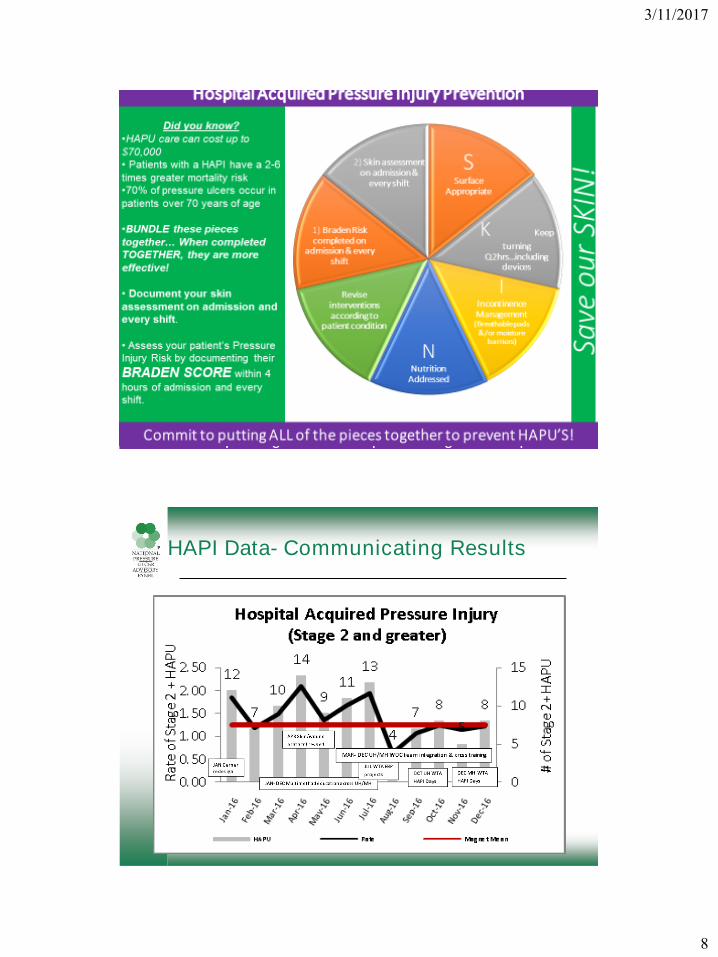
Did you know?
•HAPU care can cost up to
$70,000
• Patients with a HAPI have a 2-6
times greater mortality risk
•70% of pressure ulcers occur in
patients over 70 years of age
•BUNDLE these pieces
together… When completed
TOGETHER, they are more
effective!
• Document your skin
assessment on admission and
every shift.
• Assess your patient’s Pressure
Injury Risk by documenting their
BRADEN SCORE within 4
hours of admission and every
shift.
Commit to putting ALL of the pieces together to prevent
HAPU’S!
S Surface
Appropriate
K Keep turning
Q2hrs…including devices
IIncontinence Management
(Breathable pads &/or moisture
barriers)
NNutrition
Addressed
Revise interventions according to
patient condition
1) Braden Risk completed on admission & every shift
2) Skin assessment on
admission & every shift
Save o
ur
SK
IN!
HAPI Data- Communicating Results
3/11/2017
9
New knowledge; innovation and improvement
• Research activities-
– WOCN grant recipient x 3- BMS RCT, BMS translation into practice, PIPI
– Device-related HAPI- AACN grant recipient/webinar Nov 2014
– Soft silicone dsg as prevention- cost savings of $271,000- $1,972,100
– WOC Team redesign- IUH Quality award
• Supports EBP projects to improve PIP- WTA program EBP projects
– PIP and linen use
– PIP and progressive mobility
– PIP and Braden risk assessment
– PIP and support surface
• Supports publication of clinical work- journal articles, abstract
submissions, poster presentations, podium presentations.
• Recognizes innovation- standing agenda item (tests of change)
• Promotes PIP beyond organization, into the community- WTA Community
Program
Greetings from Mayo Clinic Rochester

3/11/2017
10
One Size Does NOT Fit All
Structure Elements
• Stability of Clinical Staff
• Experts near the Front Lines
• Presence and Sophistication of
Electronic Health Record
• Materials Management and Purchasing
Department
• Administrative Support
• Legal Department liaison

3/11/2017
11
Process Elements
• Assessment
– CWOCN/CWCN/CNS
– Wound Therapy Technicians
– Expert Staff Nurses
• Skin Savers Teams on the Units
• Availability of Educational Offerings
– Physical Therapy Wound Specialists (CWS)
– Staging (Are we all speaking the same
language?)
Process Elements
• Communication
– Electronic Notifications through the EHR
– Types of Notifications
• Braden Scores for high risk patients
• Certain types of skin alterations
– Clinical Cameras
• Data security
• Technical expertise
• Accessibility
– Multidisciplinary Team Notification

3/11/2017
12
Process Elements
• Materials Management and Purchasing
– Contracts
– Nursing Supply Value Analysis Committee
• Multi-disciplinary
• Administrative Support
– Resource Commitment (It Takes a Village)
• Pressure Ulcer Prevention Work Group
• Event Analysis
• Personnel
• Support for Education
Process Elements
• Interventions
– Skin Care Bundles for Prevention
• Risk and skin assessments
• Progressive mobility
• Moisture management
• Nutrition
– Treatment Algorithms
– Process Measures Monitoring
• Standardized but customizable care plans
• Follow up compliance reports

3/11/2017
13
Process Elements
• Interventions
– Evidence Based Practice (the never-ending
story)
• Dressings
– Silicone border
• Bed Surfaces
– Support Surface Standards Initiative (S3I)
• Building the Body of Evidence
– Non-Contact Ultrasonic Mist Therapy
– Turning schedules and reminders
Process Elements
• Event Data Analysis
– Medical Device
Related Pressure
Injuries
• Compression Wraps
• Continuous Positive
Airway Pressure
(CPAP) masks
• Cervical Collars
– Translational
Research

3/11/2017
14
Research and QI: Pay it Forward
• Cervical Collars
• Braden Scale Scores
• Anti-Shear Technology
– CPAP Masks
– Pre-hospital Transport
Tescher AN, Rindflesch AB, Youdas JW, Jacobson TM, Downer LL, Miers AG, Basford JR, Cullinane DC, Stevens SR, Pankratz VS, Decker PA. Range-of-motion restriction and craniofacial tissue-interface pressure from four cervical collars. J Trauma. 2007 Nov; 63(5):1120-6. PMID:17993960.
DOI:10.1097/TA.0b013e3180487d0f.
Tescher AN, Branda ME, Byrne TJ, Naessens JM. All at-risk patients are not created equal: analysis of Braden pressure ulcer risk scores to identify specific risks. J Wound Ostomy Continence Nurs. 2012 May-Jun; 39(3):282-91. PMID:22552104. DOI:10.1097/WON.0b013e3182435715.
Anti-Shear Technology – CPAP Masks

3/11/2017
15
Anti-Shear Technology – Pre-Hospital Transport
There’s got to be a pony in here somewhere…

3/11/2017
16
Conclusion
An effective and sustainable PIP program can be developed using the four Magnet Model domains of:
• Transformational leadership
• Structural empowerment
•
• Exemplary professional practice
• New knowledge; innovation and improvement.
Successful implementation of these elements yields measurable positive outcomes.(W. V. Padula, Mishra MK, Makic MB, Valuck RJ, 2014 Apr)
References
• Agency for Healthcare Research and Quality (AHRQ). (2011 July). AHRQ toolkit helps to prevent hospital-acquired pressure ulcers: Research Activities. Rockvill, MD: AHRQ.
• Berwick, D. M., Calkins DR, McCannon CJ, Hackbarth AD. (2006 Jan). The 100,000 lives campaign: setting a goal and a deadline for improving care quality. JAMA, 295(3), 324-327.
• Black, J. M. (2005). National Pressure Ulcer Advisory Panel: Moving toward consensus on deep tissue injury and pressure ulcer staging. Adv Skin Wound Care, 18, 415.
• Clark, M. L. (2006 Jun). The Magnet Recognition Program and evidence-based practice. J Perianesth Nurs, 21(3), 186-189.
• Creehan, S.; Cuddigan,J.; Gonzales, D.; Nix, D.; Padula, W.; Pittman,J.; Pontieri-Lewis, V.; Walden, C.; Wells, B.; Wheeler, R. The VCU Pressure Ulcer Summit-Developing Centers f Pressure Ulcer Prevention Excellence: A Framework for Sustainability. J Wound Ostomy Continence Nurs. 2016;43(2):121-128
• Donabedian, A. (1992). Quality assurance. Structure, process and outcome. Nurs Stand, 7(11 Suppl QA), 4-5.
• Duncan, K. (2007). Preventing Pressure Ulcers: The Goal is Zero. The Joint Commission Journal on Quality and Patient Safety, 33(10).
• Kelleher, A. D., Moorer, A., & Makic, M. F. (2012). Peer-to-peer nursing rounds and hospital-acquired pressure ulcer prevalence in a surgical intensive care unit: a quality improvement project. J Wound Ostomy Continence Nurs, 39(2), 152-157. doi: 10.1097/WON.0b013e3182435409
• LeMaster, K. (2007). Reducing Incidence and Prevalence of Hospital-Acquired Pressure Ulcers at Genesis Medical. The Joint Commission Journal on Quality and Patient Safety, 33(10).
• Lyder, C. H., Grady J, Mathur D, Petrillo MK, Meehan TP. (2004). Preventing pressure ulcers in Connecticut hospitals by using the plan-do-study-act model of quality improvement. Jt Comm J Qual Safe, 30(4), 205-214.
• Morton, A., Mengersen K, Waterhouse M, Steiner S. (2010). Analysis of aggregated hospital infection data for accountability. J Hosp Infection, 76(4), 287-291.
• National Database of Nursing Quality Indicators; Pressure Injury Training Modules, version 5; Retrieved February 9, 2017. https://members.nursingquality.org/ndnqipressureulcertraining/

3/11/2017
17
References
• National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel. Prevention
and treatment of pressure ulcers: clinical practice guideline. Washington DC: National Pressure
Ulcer Advisory Panel; 2009.
• Padula, W. V., Mishra MK, Makic MB, Sullivan PW. (2011 Apr). Improving the Quality of Pressure
Ulcer Care with Prevention: a cost-effectiveness analysis. Med Care, 49(4), 385-392.
• Padula, W. V., Mishra MK, Makic MB, Valuck RJ. (2014 Apr). A Framework of Quality Improvement
Interventions to Implement Evidence-Based Practices for Pressure Ulcer Prevention. Adv Skin
Wound Care, (In Press).
• Padula, W. V., Mishra MK, Weaver CD, Yilmaz T, Splaine ME. (2012 Jun). Building Information for
Systematic Improvement of the Prevention of Hospital-acquired Pressure Ulcers with Statistical
Process Control Charts and Regression. BMJ Quality & Safety, 21(6), 473-480.
• Padula, W. V., Wald, H. M., & Makic, H. M. (2013). Pressure ulcer risk assessment and prevention.
Ann Intern Med, 159(10), 718. doi: 10.7326/0003-4819-159-10-201311190-00016
• Pappas, S. (2008). The Cost of Nurse-Sensitive Adverse Events. JONA, 38(5), 230-236.
• Ratliff, C. R., Bryant DE. (2003). Guideline for prevention and management of pressure ulcers
WOCN clinical practice guideline; no. 2 (Vol. 2, pp. 52). Glenview, IL: Wound, Ostomy, and
Continence Nurses Society (WOCN).
• Ratliff, C. R., & Tomaselli, N. (2010). WOCN update on evidence-based guideline for pressure
ulcers. J Wound Ostomy Continence Nurs, 37(5), 459-460. doi: 10.1097/WON.0b013e3181f17cae
• Centers for Medicare and Medicaid Services (CMS). Overview of hospital-acquired conditions
(present on admission indicator). Retrieved 3/13/2012 from:
http://www.cms.gov/hospitalacqcond/01_overview.asp#topofpage
References
• Armour-Burton, T., Fields, W., Outlaw, L., Deleon, E. The Healthy Skin Project: Changing Nursing
Practice to Prevent and Treat Hospital-Acquired Pressure Ulcers. Critical Care Nurse. June 2013.
33(3): 32-40.
• Bergstrom, N., Horn, S., Rapp, MP, Stern, A., Barrett, R., Watkiss, M. Turning for Ulcer ReductioN: A
Multisite Randomized Clinical Trial in Nursing Homes. JAGS. October 2013. 61(10):1705-1713.
• Call, E., Pedersen, J., Bill, B., Black, J., et al. Enhancing Pressure Ulcer Prevention Using Wound
Dressings: What are the Modes of Action?. INT WOUND J. Aug2015; 12(4):408-413.
• Chaboyer, W., Gillespie, BM. Understanding nurses’ views on a pressure ulcer prevention care
bundle: a first step towards successful implementation. Journal of Clinical Nursing. February 2014.
23, 3415-3423, doi:10.1111/jocn.12587.
• Chou, R., Dana, T., Bougatsos, C., Blazina, I., et al. Pressure Ulcer Risk Assessment and
Prevention. Annals of Internal Medicine. 2 JUL 2013. 159(1): 28-39.
• Coyer, F., Gardner, A., Doubrovsky, A., Cole, R., et al. Reducing Pressure Injuries in Critically Ill
Patients by Using a Patient Skin Integrity Care Bundle (InSPiRE). American Journal of Critical Care.
May 2015. 24(3): 199-210.
• Crawford, B., Corbett, N., Zuniga, A. Reducing Hospital-Acquired Pressure Ulcers: A Quality
Improvement Project Across 21 Hospitals. J Nurs Care Quality. 29(4):303-310.
• Dellefield, ME, Magnabosco, JL. Pressure Ulcer Prevention in Nursing Homes: Nurse Descriptions
of Individual and Organization Level Factors. Geriatric Nursing. 35 (2014) 97-104.
• Gillespie, BM, Chaboyer, W., Sykes, M., O’Brien, J., Brandis, S. Development and Pilot Testing of a
Patient-Participatory Pressure Ulcer Prevention Care Bundle. J Nurs Care Qual. 29(1): 74-82.
• Hopper, MB, Morgan, S. Continuous Quality Improvement Initiative for Pressure Ulcer Prevention. J
WOCN. March/April 2014;41(2):178-180.

3/11/2017
18
References
• Olsho, LEW, Spector, WD, Williams, CS, et al. Evaluation of AHRQ’s On-Time Pressure Ulcer
Prevention Program: A Facilitator-assisted Clinical Decision Support Intervention for Nursing
Homes. Mecal Care. March 2014;52(3):258-266.
• Padula, WV, Makic, MB, Mishra, MK, et al. Comparative Effectiveness of Quality Improvement
Interventions for Pressure Ulcer Prevention in Academic Medical Centers in the United States.
Joint Commission Journal on Quality and Patient Safety. June 2015;41(6):246-256.
• Padula, WV, Valuck, RJ, Makic, MB, Wald, HL. Factors Influencing Adoption of Hospital-
Acquired Pressure Ulcer Prevention Programs in US Academic Medical Centers. J WOCN.
July/August 2015;42(4):327-330.
• Santamaria, N., Gerdtz, M., Sage, S., McCann, J., et al. A Randomized Controlled Trial of the
Effectiveness of Soft Silicone Multi-layered Foam Dressings in the Prevention of Sacral and
Heel Pressure Ulcers in Trauma and Critically Ill Patients: The Border Trial. INT WOUND J.
2015; 12:302-308.
• Tayyib, N., Coyer, F., Lewis, PA. A Two-Arm Cluster Randomized Control Trial to Determine the
Effectiveness of a Pressure Ulcer Prevention Bundle for Critically Ill Patients. Journal of Nursing
Scholarship. 2015;47(3):237-247.
• Yap, TL, Kennerly, SM, Simmons, MR, et al. Multidimensional Team-Based Intervention Using
Musical Cues to Reduce Odds of Facility-Acquired Pressure Ulcers in Long-Term Care: A Paired
Randomized Intervention Study. JAGS. 2013;61(9):1552-1559.
Prevention That Works


















