
Presented by Keya Bala(90) Sutapa Das(93) Azma Parhin(91)
69
-
Upload
homer-pope -
Category
Documents
-
view
230 -
download
3
Transcript of Presented by Keya Bala(90) Sutapa Das(93) Azma Parhin(91)


Case Presentation Presented by
Keya Bala(90)Sutapa Das(93)
Azma Parhin(91)

Particulars Of The Patients
Name:Mrs.NurnaharHusband’s name:Mr.Mahbub Ali
Age:60 yearsSex:Female
Religion:IslamMarital status:MarriedOccupation:Housewife
Address:Anowara,ChittagongContact no:01643125434
Date of admission:02.11.13 at 3.00 pmDate of examination:05.11.13 at 7.00 pm
Ward no:24 ,Bed no:46Surgical unit:24

Presenting Complaints1.Pain in left breast for last 1 month2. Progressive swelling in the left breast for last 1 year.

History of Present Illness

According to the patient’s statement she was relatively well 1 year back.Then she developed a swelling on her left breast which was gradually progressive in size.The skin overlying the lump was reddish in colour.She also complained of mild pain in the swelling for last 1 month.Pain was not associated with fever,chills and rigor.She also complained that her body weight decreased 1/5th of previous weight since last month.Then she went to doctor and diagnosed as a case of invasive duct cell carcinoma of left breast.She has no history of chest pain,haemoptysis,haematemesis,melaena,jaundice,bone pain.Her bowel and bladder habits are normal.With this complaints she got admitted in CMCH for better management

History of past illness
She has no history of same type of problem before.She has no history of hypertention,diabetes,asthma.

Personal historyShe is non smoker,non alcoholic,she gave history of taking betel leaf and betel nuts.

Family History She has four children, all children are breast fed. None of her first degree relatives is suffering from this disease.

Drug history
She took no medication for lump.

Blood transfusion history She has no history of previous blood transfusion.
Immunization history She can not give history of specific immunization.

.
History of contraception :She gave no history of taking contraceptive pill during her reproductive age.Menstrual history : She is a post menopausal woman for 10 years.Her menarche started at 13 years.Her menstrual cycle was regular.

Systemic Enquiry :
Cardiorespiratory :
Chest pain – Absent Intermittent claudication – Absent Palpitation – Absent Ankle swelling – Absent Orthopnoea – Absent Nocturnal dyspnoea – Absent Shortness of breath – Absent Cough with or without sputum –Absent Haemoptysis - Absent

Gastrointestinal : Abdominal pain – Absent Dyspepsia – Absent Dysphagia – Absent Nausea and/or vomiting – Absent Changes in appetite – Absent Weight loss – Absent Change in bowel pattern – Absent Rectal bleeding – Absent Jaundice – Absent

Genito-urinary : Haematuria – Absent Nocturia – Absent Frequency – Absent Dysuria – Absent
Neurological : Seizure – Absent Dizziness and loss of balance – Absent Paraesthesia – Absent Muscle weakness – Absent Muscle wasting – Absent Spasm and involuntary movement – Absent Pain in limb and back - Absent

General Examination :Appearance : AnxiousBuild :Below averageCo-operation : Co-operativeDecubitus : On choiceAnaemia : Mildly anaemicJaundice : AbsentCyanosis : AbsentEdema : AbsentAsicitis :AbsentDehydration : AbsentNutrition : AverageBlood pressure : 110/70
mmHgPulse :72beats/minuteRespiratory rate : 17breaths
per minuteNeck vein :Not engorged Neck gland :Not palpableHernial orifices : IntactPeripheral Lymph nodes: All
accessible peripheral lymph node are not palpable including axillary lymph node.

::
Systemic Examination :
A. Abdominal Examination :
1. Inspection :-
Shape – Normal
Umbilicus –Centrally placed, inverted
No visible peristalsis
No engorged vein and scar mark
2. Palpation :-
a. Superficial –
Temperature – Not raised
Tenderness – Absent
Hyperasthesia – Absent
Muscle guard – Absent
b. Deep – Liver, spleen and kidneys are not palpable. 3. Percussion :- Percussion note - Tympanic 4. Auscultation :- Bowel sound - Present

::
B. Cardio-respiratory Examination 1. Inspection :-
Chest :- Shape – Normal Movement with respiration – In both side normal Scar mark – Absent There is a lump in upper and inner quadrant of left breast Left nipple is retracted Visible engorged vein over the lump
2. Palpation :- Position of trachea – Central Apex beat – in left fifth intercostals space, 10cm from the lateral border of sternum

::
Vocal fremitus – NormalChest expansion – NormalRib tenderness – AbsentApex beat – Palpable in left fifth intercostals space, 9.5 cm from left lateral border of sternum
3. Percussion :- Percussion note – Resonant Area of liver dullness – In fifth intercostals space 4. Auscultation :- Breath sound – Vesicular Vocal resonance – Normal First and second heart sound - Normal

::
Local examination :1.Inspection :
Right breast : Normal in appearance No scar mark Nipple – Not retracted
Left breast : Upwards in comparison to right breast Site - There is a visible lump in the central portion of the breast Size:5cm 5cm Shape - Irregular Overlying skin – Not ulcerated Nipple – Retracted Areola:Thickened and blakish

::
2.Palpation : Local temperature – Slightly increased Tenderness – Mildly tender Consistancy – Hard Size –5x5 cm Surface - Irregular Border – ill-defined Fixation – Fixed with overlying skin and not fixed with underlying pectoralis major muscle Movement is possible in all direction . Axillary group of lymph node: Not palpable in both side. Supraclavicular lymph node : Not palpable in both sides.

::
Salient feature
Mrs. Jakia Khatun, 70 years old, hypertensive, from Bohoddarhat, Chittagong presented to me with the complaint of-Lump in left breast for one yearAccording to her, she noticed a lump in her left breast one year ago, at first small in size, but gradually it is increasing in size,not associated with pain. She has no anorexia, weight loss, bone pain, jaundice, itching, melaena,haemoptysis.

::
On general examination, patient is pale, anxious. She is hypertensive, rest other vital signs are within normal limit.Systemic examination reveals no abnormality.On local examination, the lump is situated in upper and inner quadrant of left breast, non ulcerated, hard in consistency having irregular surface and ill defined border, with a size of 12x5x3 cm. There is local rise of temperature. It is not fixed with overlying skin, or underlying pectoralis major muscle, where movement in all direction is possible.

::
Provisional Diagnosis :
Carcinoma of breast. Differential Diagnosis :
Fibroadenoma of breastLipoma

Investigation Profile
Cytopathology report
Specimen:Left breast lump
Aspiration note:Blood mixed material came out on aspiration
M/E:Smear showed many irregular clusters and scattered malignant ductal epithelial cells with large hyper chromatic and pleomorphic nuclei in a blood mixed necrotic background.
Impression:Left breast lump(FNA): Duct cell carcinoma


Report: Ultra sonogram of whole abdomen
Liver: is normal in size, shows homogenous parenchymal echo texture. No focal or diffuse lesion is seen. IHBCs are not dilated.
Gallbladder: is well distended with normal wall thickness. No calculus is seen.
Common bile duct: is not dilated.
Pancreas: visualized portion of pancreas appears normal.
Spleen: is normal in size with homogenous echo texture.
Kidneys: are normal in size, shape and position. Cortico-medullary differentiation is maintained. Pelvi-calyceal systems are not dilated.
Urinary bladder: is well distended with normal wall thickness. No intravesical lesion is seen.
Impression: Normal study.


Report: Chest X-ray P/A view
Diaphragm: Normal in position.Heart: Normal in transverse diameter.Lungs: Both lung fields are clear.Bony thorax: Appears normal.Impression: Normal chest X-ray.

ECG Report

Name of the investigation Result
Complete blood countHaemoglobin 10.5g/dlESR 75mm in 1st hourWBC 9500/cu mm
Urine Routine ExaminationEpithelial cells 2-4/HPFPus cells 2-3/HPF

Investigation Profile
FBS (Fasting blood sugar) 85mg/dl2hrs ABF 126mg/dlSerum creatinine 0.8mg/dlSerum albumin 4.3g/dlBlood group “ A ” positive Cytopathology report:Left breast lump (FNA). Duct cell carcinoma.USG of whole abdomen: NormalChest X-ray P/A view: Normal
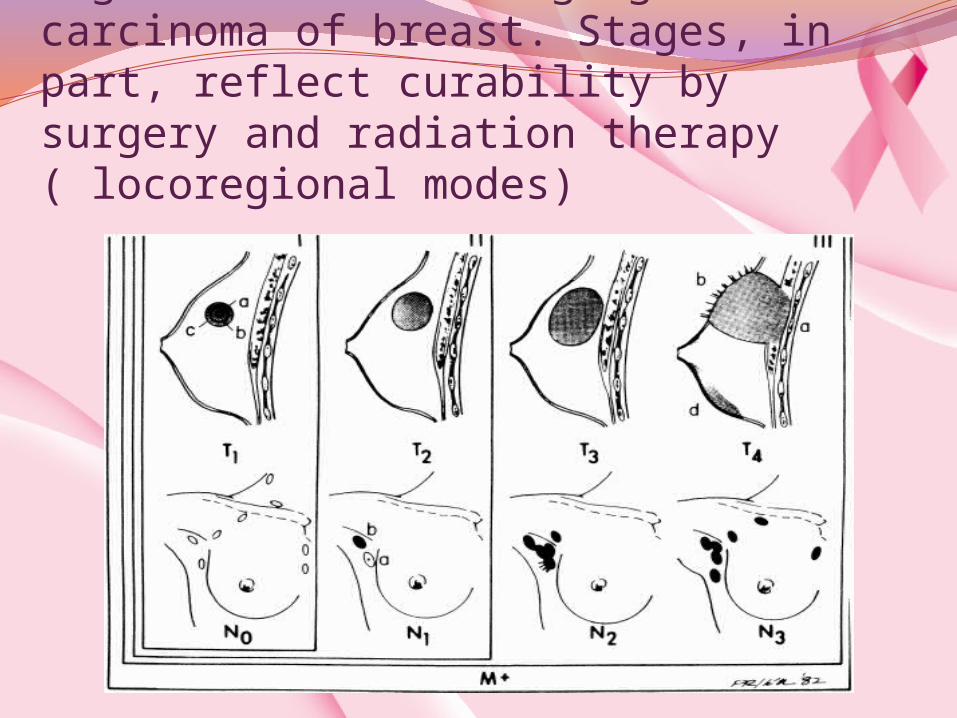
Figure :Clinical staging of carcinoma of breast. Stages, in part, reflect curability by surgery and radiation therapy ( locoregional modes)

Staging by IUAC : TNM Staging T (Tumour size)T 0 =No evidence of primary tumourTis = Carcinoma in situT1 = Tumour < 2 cmT2 = Tumour 2-5 cmT3 = Tumour > 5 cm T4 = Any size involving skin or chest wall

N (Nodal involvement)N0 = No nodal metastasis N1 = Mobile palpable axillary lymph node N2 = Fixed axillary lymph nodeN3 = Ipsilateral palpable supraclavicular lymph node Ipsilateral palpable infraclavicular lymph
node
M (metastasis) M0 = No metastasis M1 = Distant metastasis

Manchester staging Stage I= Tumour < 2cm in diameter Stage II = Tumour 2- 5cm in diameter with or without palpable
mobile lymph node in ipsilateral axillaStage IIIa = Tumour > 5 cm in diameter with or
without fixed palpable axillary lymph node. Stage IIIb = Skin involvement. Skin involvement wide than tumour Peaud’ orange Fixation to underlying muscle Palpable supraclavicular lymph node Oedema of arm Stage IV = Distant metastasis

Combination of Manchester and TNM staging Tis : No palpable lump detected in mamography. No palpable lymph node. Stage I : T1 : Size < 2 cm in diameter No : No palpable lymph node M0 : No metastasis Stage II : T2 : 2-5 cm in diameter N1 : Mobile axillary lymph node Mo : No metastasis Stage IIIa : T3 : > 5cm in diameter N2 : Fixed axillary lymph node M0 : No metastasis Stage IIIb : T4 : Irrespective of size if there is any cutaneous
ulceration or fixity with underlying structure N3 : Other than axillary lymph node involvement with ipsilateral supraclavicular lymph node
involvement Mo : No metastasis Stage IV : M1 : Metastasis is present No consideration about T and M

Confirmatory DiagnosisAccording to the staging of combination
Manchester and TNM the confirmatory diagnosis is Carcinoma of breast stage IIIa.
Treatment Left sided simple mastectomy with axillary
clearance.

Pre –requisite for surgeryProper councellingInformed written consent

Pre-operative OrderKeep the patient nothing by mouth from
11pm today.Take informed written consent from the
patient or patient’s attendant for operation under G/A.
Clean and shave the operative field with right axilla.
Send the patient to the patient to the OT at 8am on 10-10-2012.
Inf.Hartsol (1000cc) I/V at 30 drops/min from 7am on 10-10-2012.

SurgeryWith all aseptic condition left part chest wall
is opened by doing left eliptical incision.The excised mass is composed of The whole left breast All the fat and fascia and lymph node of ipsilateral axilla

Post operative orderNothing by mouth – till further orderInf. 5% DNS (2000cc)Inf.N/S (1000cc) I/V at 30 drops/minInf.Furocef (750 mg) -1 vial I/V stat 8hourlyInf.Flubex (500 mg) - 1 vial I/V stat 6 hourlyInj.Pethedine (100 mg) -3/4th ampule (75 mg)I/MInj.Phenerex (50 mg) -1/2 ampule I/M with
Inj.Pethedine I/M 8 hourly for 24 hoursInj.Pantonix (40 mg) -1 vial I/V stat 12 hourlyInj.Rolac (30 mg) - 1 ampule I/V statDrainage tube in situ is given (collection is 1000cc/24
hours)Dressing condition is examined properly (dressing is
dry)Specimen sent for cytopathology examination reveals
duct cell carcinoma.

Follow UpAccording to cytopathology report there is
duct cell carcinoma in situ ( non invasive).Post operative radiotherapyRegular checkup 6 month interval for 3 years12 months interval for rest of lifeIf any complaints-Clinical examination : local and sysytemicInvestigation : Mamography

Outline
Female Breast Anatomy
Breast Cancer
Mammography
Computer-Aided Diagnosis of Breast Cancer
46

Female Breast Anatomy
47

Lymphatic System
48
Lymph ducts: Drain fluid that carries white blood cells (that fight disease) from the breast tissues into lymph nodes under the armpit and behind the breastbone
Lymph nodes: Filter harmful bacteria and play a key role in fighting off infection
A network of vessels
Lymph ductLymph node

Normal Breast
Breast profile
A ducts
B lobules
C dilated section of duct to hold milk
D nipple
E fat
F pectoralis major muscle
G chest wall/rib cage
49
Enlargement
A normal duct cells
B basement membrane (duct wall)
C lumen (center of duct)
Illustration © Mary K. Bryson

Range of Ductal Carcinoma in situ
50
Illus
trat
ion
© M
ary
K.
Bry
son

Invasive Lobular Carcinoma (ILC)
51Illustration © Mary K. Bryson
Lobular cancer cells breaking
through the wall

Mammography
Use a low-dose x-ray system to examine breasts
Digital mammography replaces x-ray film by solid-state detectors that convert x-rays into electrical signals. These signals are used to produce images that can be displayed on a computer screen (similar to digital cameras)
Mammography can show changes in the breast up to two years before a physician can feel them
52

Computer-Aided Diagnosis
Mammography allows for efficient diagnosis of breast cancers at an earlier stage
Radiologists misdiagnose 10-30% of the malignant cases
Of the cases sent for surgical biopsy, only 10-20% are actually malignant
53
National Cancer Institute
CAD systemscan assist
radiologists toReduce these
problems

Risk factorsBreast Cancer (BC)Etiology:The variation of incidence amongdifferent populations: Environmental factors: e.g. highconsumption of dietary fat, sugar. Genetic factors especially in youngerwomen.

Other risk factors:Gross cystic disease, atypical hyperplasiaand multiple papillomatosis,- Most forms of benign breast diseasedo not predispose BCLobular carcinoma in situ carries a 30percent risk of invasive cancer.

Factors known to decrease risk:Asian ancestry.Term pregnancy before age 18 years.Early menopause , Surgical castrationbefore the age of 37 years.
Factors having no effect on risk(previously thought to be risk factors):Multiparty.Lactation.Breast feeding

Clinical breast exam Mammogram - to check breast tissue
Other tests
Computer-aided detection (CAD) Digital mammography Magnetic resonance imaging (MRI) Breast ultraasound (ultrasonography)
Experimental procedures
Ductal lavage Molecular breast imaging (MBI)

Diagnostic procedures Ultrasound Biopsy – Fine-needle aspiration biopsy, core needle biopsy, sterotactic
biopsy, wire localization biopsy, surgical biopsy Estrogen and progesterone receptor tests Staging tests – Stage 0 to IV Genetic stage

TreatmentAdvanced metastatic disease:(any T, any N, M1)Palliative intent.Factors affecting treatment decision:– Menstrual states.– Site of metastases (vital organs).– Extent of the disease.– Performance status and age.Treatment:– Systemic therapy, RT, Surgery, trials of new therapyand supportive treatment.

Role of RT in Breast CancerPreoperative RT.Post-mastectomy RT.Conservative surgery + RT.Palliative RT.
PORT ( Post opertive radiotherapy)Indications:Patients with T3 and T4 tumors.> 4 Positive axillary lymph nodes.Residual disease

TREATMENT OPTION In addition to coping with a potentially life-
threatening illness – must make complex decisions about treatment.
Treatments exist for every type and stage of breast cancer.
Most women will have surgery and an additional (adjuvant) therapy such as radiation, chemotherapy or hormone therapy.
Experimental treatments are also available at cancer treatment centers.

SURGERY
Lumpectomy Partial or segmental mastectomy Simple mastectomy Modified radical mastectomy
Sentinel lymph node biopsy Axillary lymph node dissection Radiation therapy Chemotherapy

Reconstructive surgery
Reconstruction with implants Reconstruction with a tissue flap Deep inferior epigastric perforator (DIEP)
reconstruction Reconstruction of the nipple and areola

Hormonal therapy Selective estrogen receptor modulators (SERMs) Aromatase inhibitors
Biological therapy
Trastuzumab (Herceptin) Bevacizumab (Avastin) Lapatinib (Tykerb)

COPING SKILLS Telling others Maintaining a strong support system Dealing with intimacy Self-care taking

Epidemiology
Breast cancer, the second-leading cause of cancer deaths in women, is the disease women fear most.
Breast cancer can also occur in men, but it's far less common.
Yet there's more reason for optimism than ever before.
In the last 30 years, doctors have made great strides in early diagnosis and treatment of the disease and in reducing breast cancer deaths.

80% of breast cancers occur in women older than age 50. In 30s, have a one in 233 chance of developing breast cancer. By age 85, chance is one in eight.
In 1975, a diagnosis of breast cancer usually meant radical mastectomy – removal of the entire breast along with underarm lymph nodes and muscles underneath the breast.
Today, radical mastectomy is rarely performed. Instead, there are more and better treatment options, and many women are candidates for breast-sparing operations.

Thank you

Thank you


















