Presentation to Advisory Council Boston, MA August 25, 2011.
16
Presentation to Advisory Council Boston, MA August 25, 2011
-
Upload
timothy-houston -
Category
Documents
-
view
219 -
download
0
Transcript of Presentation to Advisory Council Boston, MA August 25, 2011.

Presentation to Advisory Council
Boston, MAAugust 25, 2011

2
Review research framework and provide updates on progress
Meeting Purpose
Introduce Manatt/Mercer
Discuss next steps

3
Manatt Health Experience
$$
States
Payers
Providers
Foundations and Other Stakeholders
$$

4
Mercer Health Experience
Health Exchange
Uninsured
Health Plan Reviews
Actuarial Rate Setting
$$

55
Transition Planning
Leverage the Commonwealth’s strong foundation
Ensure compliance with ACA requirements
Facilitate integration between MassHealth and the Connector
Strengthen the role of the Connector in the Insurance Market
Leverage the Commonwealth’s strong foundation
Ensure compliance with ACA requirements
Facilitate integration between MassHealth and the Connector
Strengthen the role of the Connector in the Insurance Market
The Strategic Plan must:The Strategic Plan must:
. . . to successfully support health care delivery system reform in the Commonwealth. . . to successfully support health care delivery system reform in the Commonwealth
The Commonwealth seeks to evaluate the options for providing subsidized coverage, Exchange (i.e., Health Connector) structure, and operations in light of federal health reform.
Massachusetts is operating major elements of federal health reform and today operates a mature and successful health benefit exchange (HBE).

6
Transition Goals and Priorities
• Comply with or, seek waiver from, specific ACA
requirements related to coverage and eligibility
• Maximize continuity of coverage from as-is to to-be
– Minimize harm to transitioning populations
• Maximize continuity of coverage among to-be coverage
options
• Leverage federal dollars to provide state fiscal relief
• Leverage purchasing power of the Connector and MassHealth
• Identify and optimize administrative simplification
opportunities

7
High Level Timeline
Exchange must be operational – January 1
Exchange must be operational – January 1
Fu
nd
ing
O
pp
ort
un
itie
sFu
nd
ing
O
pp
ort
un
itie
sR
ep
ort
ing
R
eq
uir
em
en
tsR
ep
ort
ing
R
eq
uir
em
en
tsK
ey F
ed
era
l D
ate
sK
ey F
ed
era
l D
ate
sS
tate
M
ilesto
nes
Sta
te
Milesto
nes
HHS Exchange Establishment
Grants awarded – May 23
HHS Exchange Establishment
Grants awarded – May 23
CMS to issue initial Exchange and Medicaid eligibility regulations – July, August
CMS to issue initial Exchange and Medicaid eligibility regulations – July, August
HHS Approval that Exchange will be operational by 1/1/14 – January 1
HHS Approval that Exchange will be operational by 1/1/14 – January 1
State must spend grant funds -
September 30
State must spend grant funds -
September 30
Early Innovator Grant Awards – February 15(Applications due 12/22/10)
Early Innovator Grant Awards – February 15(Applications due 12/22/10)
Early Innovator Grant period ends – February
Early Innovator Grant period ends – February
Exchange must be self-
sustained – January 1,
2015
Exchange must be self-
sustained – January 1,
2015
HHS Exchange Establishment Grants RFP –
February
HHS Exchange Establishment Grants RFP –
February
Final report & Federal Financial Report due – 90 days within project end date
Final report & Federal Financial Report due – 90 days within project end date
Project Kick-Off –June 13
Project Kick-Off –June 13
Quarterly report – January
Quarterly report – January
Quarterly report – April
Quarterly report – April
Quarterly report – July
Quarterly report – July
Exchange must be “soft-launched” – July 1
Exchange must be “soft-launched” – July 1
Quarterly report – October
Quarterly report – October
CMS to issues second set of Exchange regulations –September
CMS to issues second set of Exchange regulations –September
HHS Exchange Establishment Grants Level 1
and Level 2 deadline –
September 30
HHS Exchange Establishment Grants Level 1
and Level 2 deadline –
September 30HHS Exchange Establishment
Grants Level 1 and Level 2 deadline –
June 30
HHS Exchange Establishment
Grants Level 1 and Level 2 deadline –
June 30
HHS Exchange Establishment Grants
Level 1 and Level 2 deadline –December 30
HHS Exchange Establishment Grants
Level 1 and Level 2 deadline –December 30
HHS Exchange Establishment Grants
Level 2 deadline – June 29
HHS Exchange Establishment Grants
Level 2 deadline – June 29
HHS Exchange Establishment Grants
Level 2 deadline – March 30
HHS Exchange Establishment Grants
Level 2 deadline – March 30
2014Jan2011
Feb2011
Mar 2011
Apr2011
May2011
Jun2011
Jul2011
Sept2011
Oct2011
Nov2011
Dec2011
Aug2011 2012 2013
ACA Sec. 1321(e) provides that HHS will provide assistance to existing Exchanges for coming into compliance with the ACA
and a presumption of compliance after this process

8
Research Approach
• Analyzed State statute, regulations, and administrative guidance:
• Analyzed Federal statute, regulations, and guidance
• Developed preliminary gap analysis
• Conducted key informant interviews
• Identified policy questions/issues for further research
• Developing high-level transition roadmap and assessment
• Developing modeling framework and assumptions
June July August September
• Conduct additional federal and state statutory, regulatory, and administrative guidance research
• Conduct modeling
• Evaluate transition options
• Conduct gap analysis
• Assess coverage options balancing the interests of multiple stakeholders
• Present findings and recommendations to Subsidized Insurance Workgroup, Advisory Council, Executive leadership, and stakeholders

9
Individual CoverageTransition Options

10
Findings: As-Is Takeaways
Coverage of 98% of Commonwealth residents has been achieved through a patchwork of programs.
98% Programs vary in:
Eligibility levels and requirementsBenefit packagesCost-sharing Funding sourcesResponsible agencies/entities
1
2
3
4
5

11
Findings: As-Is Takeaways
400%400%
FPL
FPL
300%300%
200%200%
100%100%
Children
< 1
(35,185)
Children
< 1
(35,185)
PopulationPopulationChildren
1 – 18
(449,687)
Children
1 – 18
(449,687)
Parents
(191,060)
Parents
(191,060)
Preg.
Women
(pending)
Preg.
Women
(pending)
BCCTP
(351)
BCCTP
(351)
Childless Adults
MH
(12,511)
Childless Adults
MH
(12,511)
Childless Adults
LTU
(88,283)
Childless Adults
LTU
(88,283)
HIV+
(1,262)
HIV+
(1,262)
Indiv.
Unempl. Comp
(pending)
Indiv.
Unempl. Comp
(pending)
Small Biz
Empl.
(5,226)
Small Biz
Empl.
(5,226)
Imm. 5 yr Bar
(15,474)
Imm. 5 yr Bar
(15,474)
Imm. GF
(pending)
Imm. GF
(pending)
Indiv Inelig
for MassHealth
(195,984)
Indiv Inelig
for MassHealth
(195,984)
Disabled
Adults & Children
(20,419)
Disabled
Adults & Children
(20,419)
Non- qual
Aliens
(58,365)
Non- qual
Aliens
(58,365)
Non- qual
Aliens
Children
(26)
Non- qual
Aliens
Children
(26)
MassHealth Standard MassHealth Standard
Family Assistance
Family Assistance
Medical Security
Plan
Medical Security
Plan
MassHealth Essential
MassHealth Essential
MassHealth Basic
MassHealth Basic
Common wealth
Care Bridge
Common wealth
Care Bridge
Common wealth
Care
Common wealth
Care
Common wealth Choice
Common wealth Choice
MassHealth CommonHealth
MassHealth CommonHealth
Family Assistance
Family Assistance
MassHealth Limited
MassHealth Limited
Children’s Medical Security
Plan
Children’s Medical Security
Plan
Health Safety Net
Health Safety Net
Insurance PartnershipInsurance
Partnership
12
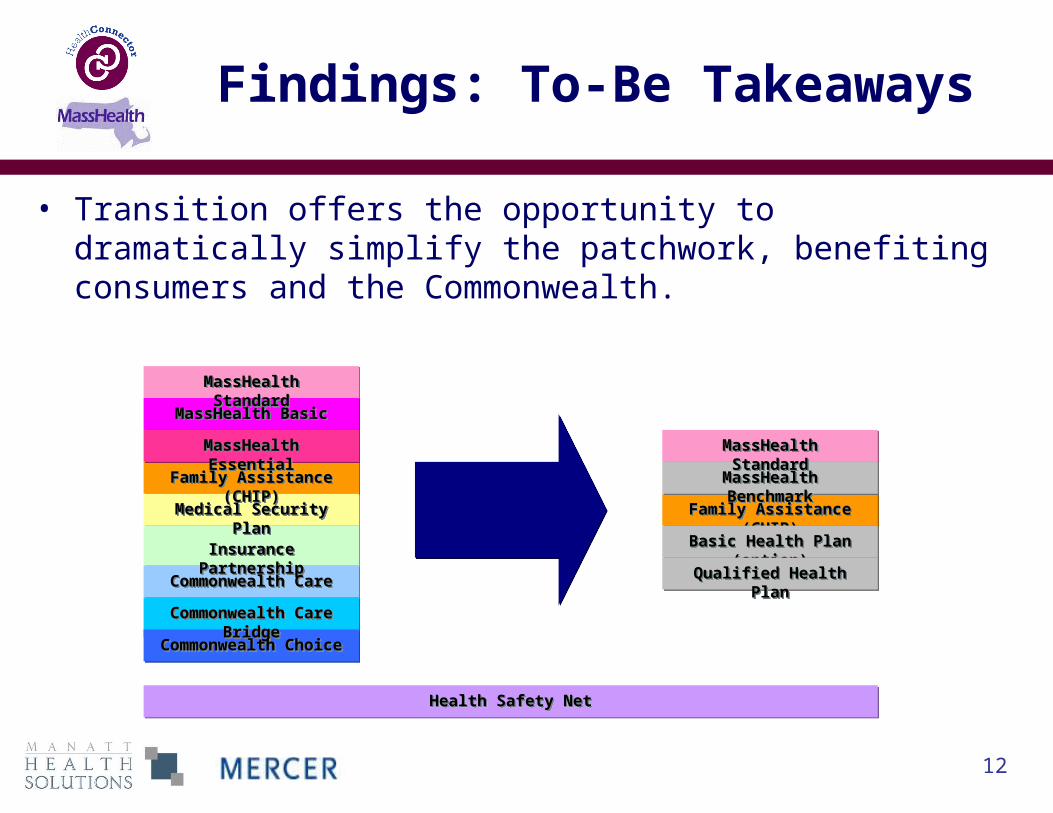
Findings: To-Be Takeaways
• Transition offers the opportunity to dramatically simplify the patchwork, benefiting consumers and the Commonwealth.
MassHealth BasicMassHealth Basic
MassHealth EssentialMassHealth Essential
Family Assistance (CHIP)Family Assistance (CHIP)
MassHealth StandardMassHealth Standard
Medical Security PlanMedical Security Plan
Insurance PartnershipInsurance Partnership
Commonwealth CareCommonwealth Care
Commonwealth Care BridgeCommonwealth Care Bridge
Commonwealth ChoiceCommonwealth Choice
MassHealth BenchmarkMassHealth Benchmark
Family Assistance (CHIP)Family Assistance (CHIP)
MassHealth StandardMassHealth Standard
Basic Health Plan (option)Basic Health Plan (option)
Qualified Health PlanQualified Health Plan
Health Safety NetHealth Safety Net

13
Transition from As-Is to To-Be:First Level Assessment
As-Is To-Be
2014 Benefit Change
Consumer Cost Sharing Change
Federal Financial Participation
State Financing
First level assessment
14
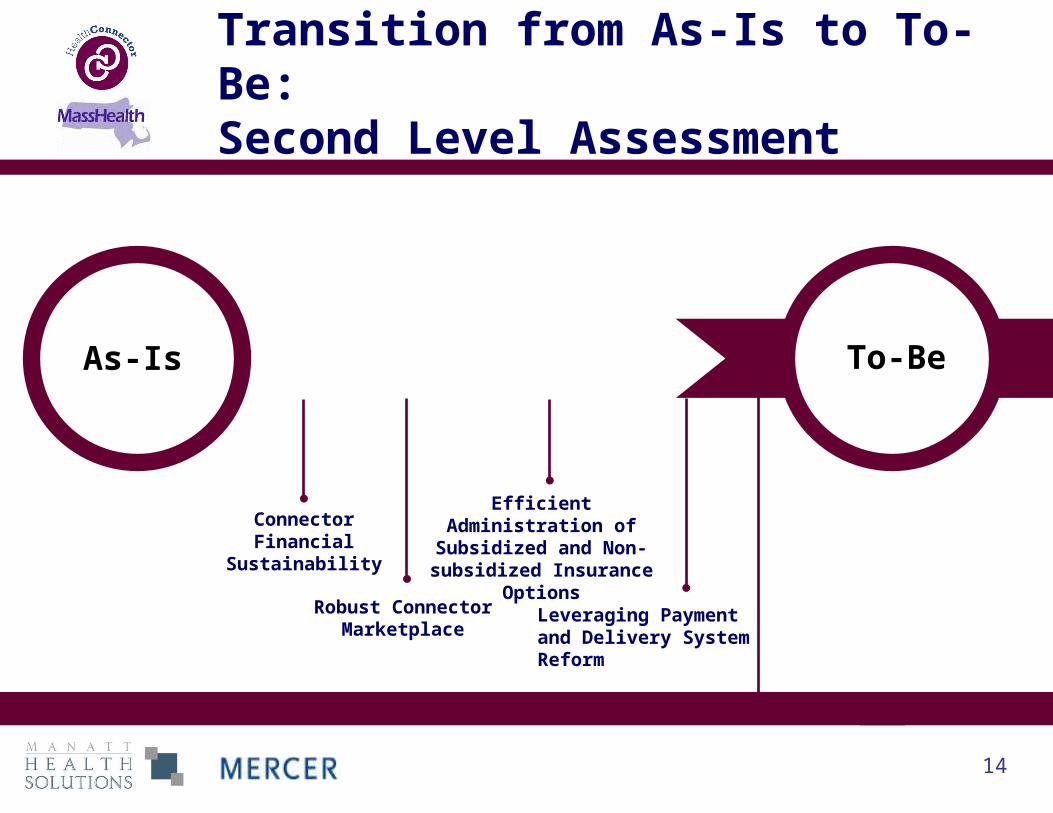
Transition from As-Is to To-Be:Second Level Assessment
As-Is To-Be
Connector Financial
Sustainability
Robust ConnectorMarketplace
Efficient Administration of
Subsidized and Non-subsidized Insurance
OptionsLeveraging Paymentand Delivery SystemReform
Second level assessment

15
In Summary
Effective administration of preferred options is the final question
Implications for Connector
scale and sustainability
Implications of the
potentially divergent delivery
models in MassHealth (MCO, PCC)
and the Connector delivery model
(health plans)
Balancing scope of benefits, consumer
cost-sharing, access to federal
financing, and impact
on state expenditures
Balancing the advantages,
disadvantages and risks
Final Transition Decisions will be Informed by:
Delivery Model
Basic Health Program
Cost - Benefit Analysis
Connector Sustainability
Optimizing to advance
payment and delivery system reform
Purchasing Leverage

16
• Conduct additional federal and state statutory, regulatory, and administrative guidance research
• Conduct modeling
• Evaluate transition options
• Conduct gap analysis
• Assess coverage options balancing the interests of multiple stakeholders
• Present to Subsidized Insurance Workgroup, Advisory Council, Executive leadership, and stakeholders
Next Steps