
Presentation on Expenditure Management in Health · Nine hypothetical hospitals. ... Needs of the...
34
Expenditure management and efficiency in the health system Health Dialogue 10 July 2012 Nairobi
Transcript of Presentation on Expenditure Management in Health · Nine hypothetical hospitals. ... Needs of the...
Expenditure management
and efficiency in the
health system
Health Dialogue
10 July 2012
Nairobi

Overview – hypotheses and
questions
1. Critical to improve health service delivery and outcomes in Africa
2. While more funding is required, efficiency of spending or value for money is the key issue
3. Budget reform (or improved expenditure management) is a key element for enhancing value for money
2
key element for enhancing value for money
4. Despite widespread implementation of budget reform in Africa, success (especially if measured as sustained improvement in service delivery and social outcomes) seems to have been limited?
5. What are the blockages?
6. How can the dialogue between health and finance help with a way forward?

2. The need for efficiency
Some illustrations

2.1 Technical efficiency
4
Source: Osei et al. (2005): “Technical efficiency …in Ghana”
“… 47% of [district] hospitals [in Ghana] were technically inefficient”; 56% of health centres in Kenya; 70% of PHC clinics in KZN, South Africa
Nine hypothetical hospitals

2.2 Need for efficiency: Aids Spending
5
Zeng, et al. (2012) How much can we gain from improved efficiency?
“there may be substantial room for improving HIV/AIDS services at
the country level with the existing resources … where the efficiency
of HIV/AIDS services is low, priority should be given to interventions
to overcome barriers … where performance is already high, efforts
should be geared towards mobilizing more resources”
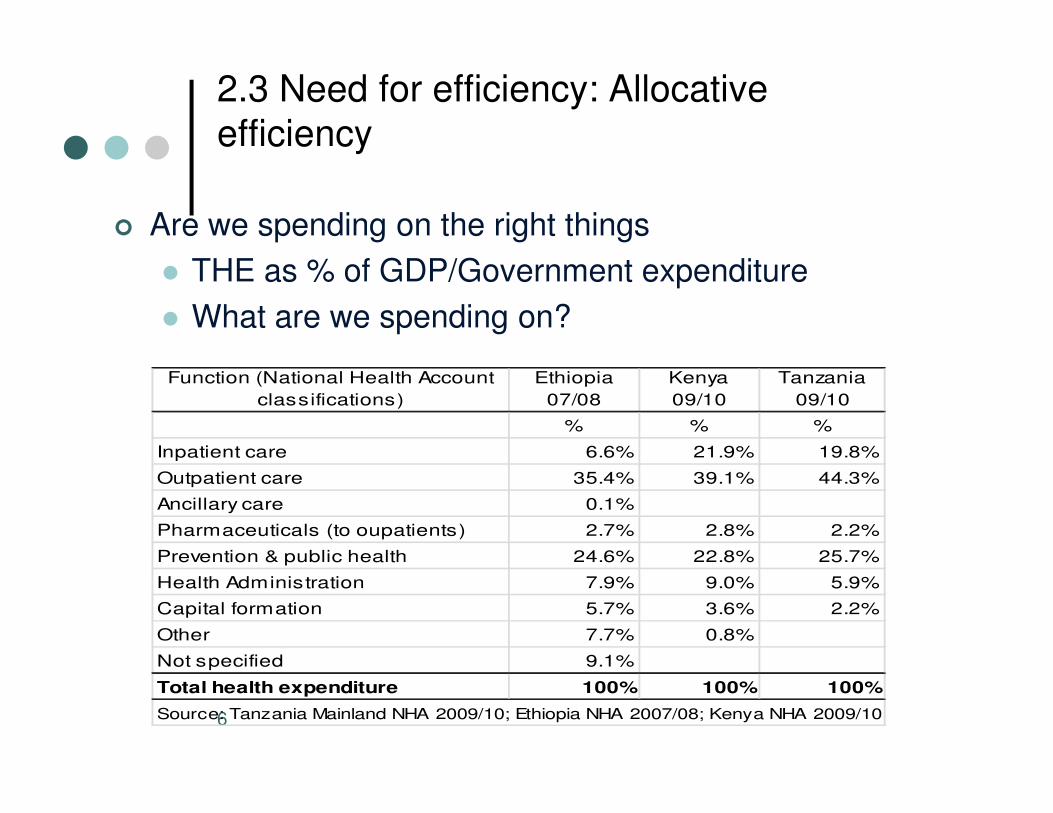
2.3 Need for efficiency: Allocative
efficiency
� Are we spending on the right things
� THE as % of GDP/Government expenditure
� What are we spending on?
Function (National Health Account
classifications)
Ethiopia
07/08
Kenya
09/10
Tanzania
09/10
6
classifications) 07/08 09/10 09/10
% % %
Inpatient care 6.6% 21.9% 19.8%
Outpatient care 35.4% 39.1% 44.3%
Ancillary care 0.1%
Pharmaceuticals (to oupatients) 2.7% 2.8% 2.2%
Prevention & public health 24.6% 22.8% 25.7%
Health Administration 7.9% 9.0% 5.9%
Capital formation 5.7% 3.6% 2.2%
Other 7.7% 0.8%
Not specified 9.1%
Total health expenditure 100% 100% 100%
Source: Tanzania Mainland NHA 2009/10; Ethiopia NHA 2007/08; Kenya NHA 2009/10
3. Expenditure management/ budget reform and efficiency
The promise

3.1 Value chain in health
8

3.2 Accountability relationships
9
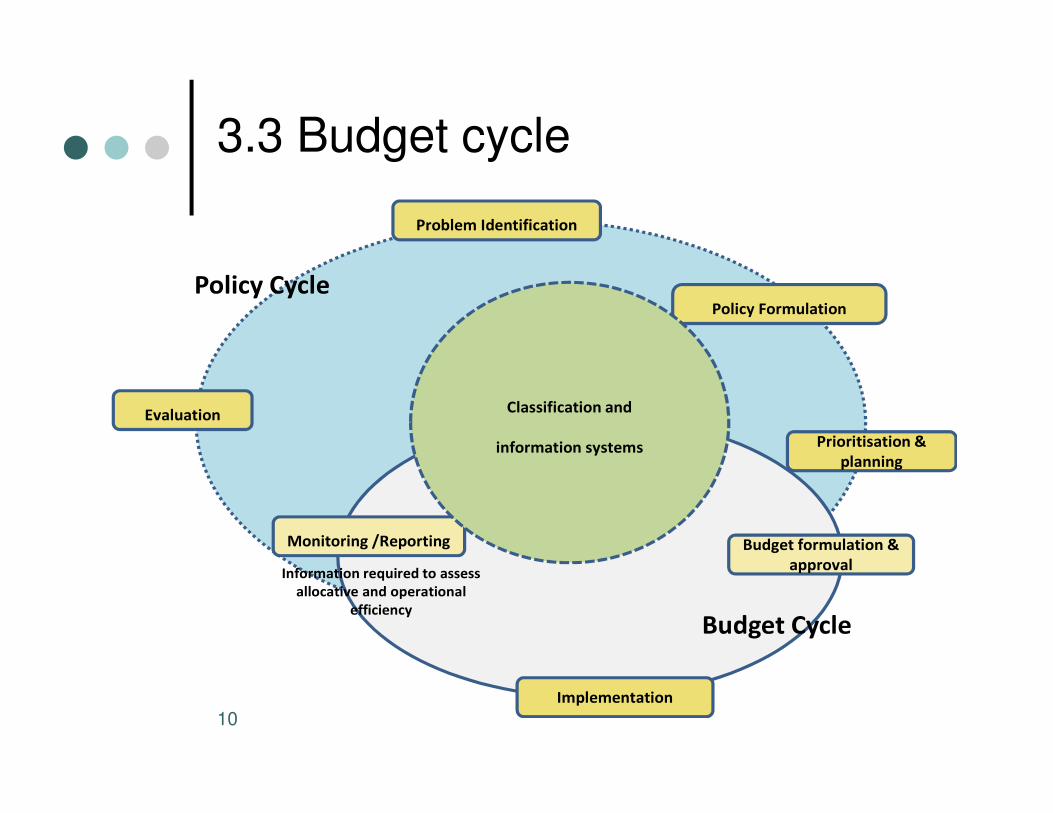
3.3 Budget cycle
Problem Identification
Evaluation
Policy Formulation
Policy Cycle
Classification and
10
Evaluation
Budget formulation &
approval
Budget Cycle
Monitoring /Reporting
Prioritisation &
planning
Implementation
Information required to assess
allocative and operational
efficiency
Classification and
information systems

3.4 Budget cycle and efficiency
Macroeconomic
framework/Macro-
expenditure control
Aggregate fiscal
discipline
Budget
11
formulation/
expenditure
programming)
Allocative efficiency
Budget execution/
implementation &
monitoring
Operational
efficiency
Source: Shall 2010

4. Components of budget reform
The tools

4.1 The package?
� Change of classification systems & programme budgeting
� Use of performance information
� Medium-term budgeting/Multi-year perspective and costing
13
� Relative autonomy of managers and units: incentives
� Execution aspects: management & control; tracking
� A focus on reporting & accountability through range of
mechanisms (audit institutions; Parliament; citizens)

4.2 Classification systems
� Different needs and different budget classifications:
� Historical analysis and policy analysis (international comparative) -
Functional classification such as COFOG
� Accountability and administering the budget – Organisational or
administrative classification
� Compliance controls and internal management - Line-item classification
Policy formulation and performance accountability/policy review -
14
� Policy formulation and performance accountability/policy review -
Programme classification. (see Allen & Tomasi 2001/Shall 2010)
� Continue to need line-item for control but emphasis shifting from
“planning for inputs” to planning for outputs (and results and outcomes)

4.3 The Classification of Functions of Government (COFOG)
7 Health
7.1 Medical products, appliances and equipment
07.1.1 Pharmaceutical products
07.1.2 Other medical products
07.1.3 Therapeutic appliances and equipment (IS)
7.2 Outpatient services
07.2.1 General medical services (IS)
07.2.2 Specialized medical services (IS)
15
07.2.2 Specialized medical services (IS)
07.2.3 Dental services (IS)
07.2.4 Paramedical services (IS)
7.3 Hospital services
07.3.1 General hospital services (IS)
07.3.2 Specialized hospital services (IS)
07.3.3 Medical and maternity centre services (IS)
07.3.4 Nursing and convalescent home services (IS)
7.4 Public health services
7.5 R&D Health
7.6 Health n.e.c.
Source: http://unstats.un.org/unsd/cr/registry/regdnld.asp?Lg=1

4.4 Programme & economic
classification
Programme R billion % Economic classification R billion %
Administration 2.9 3% Compensation of employees 59.1 58%
District Health Services 43.6 43% Goods and services 30.8 30%
Emergency Medical Services 4.3 4% Transfers and subsidies 3.9 4%
Health spending - South Africa (Provincial depts.) - '2010/11
16
Provincial Hospital Services 23.2 23% Payments for capital assets 8.1 8%
Central Hospitals 14.8 15%
Health Sciences and Training 3.4 3%
Health Care Support Services 1.6 2%
Health Facilities Management 8.3 8%
Total 102.0 100% Total 102.0 100%
Source: National Treasury, 2011 Provincia l database
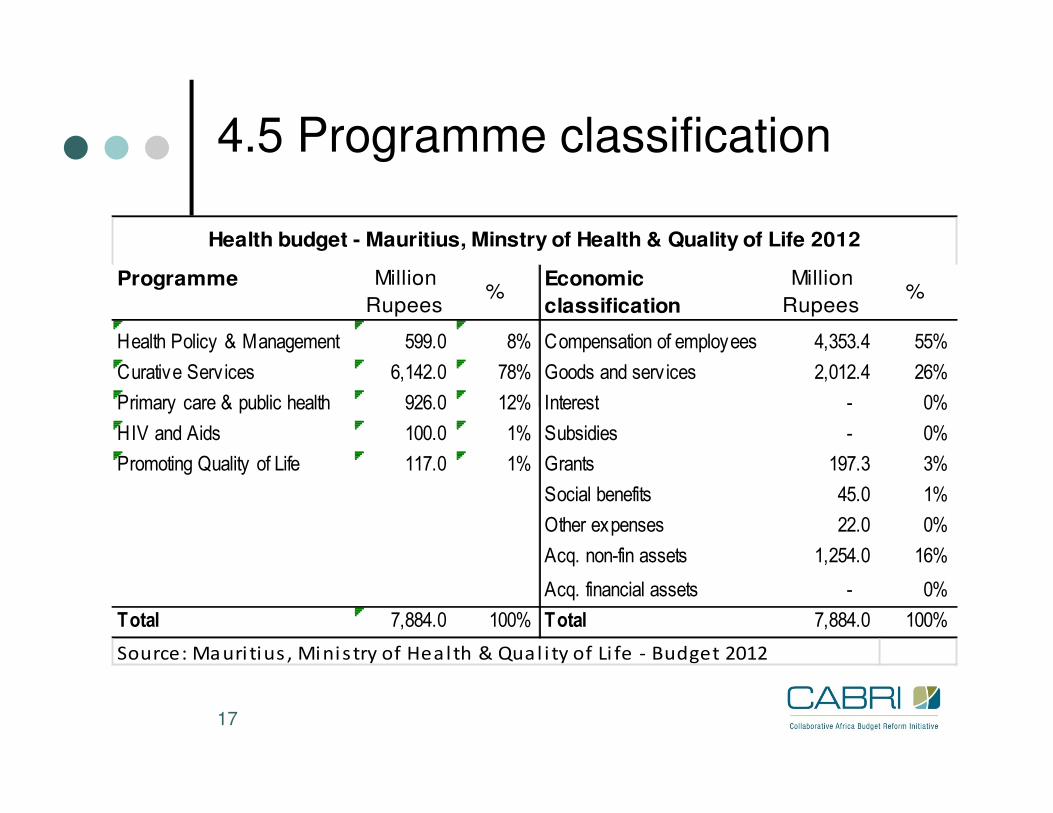
4.5 Programme classification
Programme Million
Rupees%
Economic
classification
Million
Rupees%
Health Policy & Management 599.0 8% Compensation of employees 4,353.4 55%
Curative Serv ices 6,142.0 78% Goods and serv ices 2,012.4 26%
Primary care & public health 926.0 12% Interest - 0%
Health budget - Mauritius, Minstry of Health & Quality of Life 2012
17
Primary care & public health 926.0 12% Interest - 0%
HIV and Aids 100.0 1% Subsidies - 0%
Promoting Quality of Life 117.0 1% Grants 197.3 3%
Social benefits 45.0 1%
Other expenses 22.0 0%
Acq. non-fin assets 1,254.0 16%
Acq. financial assets - 0%
Total 7,884.0 100% Total 7,884.0 100%
Source: Mauri tius , Minis try of Heal th & Qual i ty of Li fe - Budget 2012

4.6 Use of performance information
� Performance information needed for resource allocation and management
� Inputs, quantity (output), quality of services, outcome
� Different ways of using in budget process: background information versus actual
basis for allocation
� Challenge of developing useful performance measures – definitional and
18
� Challenge of developing useful performance measures – definitional and
measurement issues
� Challenge of building systems to track – health information systems
� Substantial scrutiny through Health Metrics Network: assessment of no of countries on
resources, processes, outputs
� Need: “a policy, a comprehensive plan, coordination mechanisms, sufficient investment,
and a health information workforce”

4.7 Rwanda – performance framework
19

4.8 Medium-term budgets
(MTEFs)
� “Multi-year perspective in fiscal planning, expenditure policy and budgeting”
� Predictability as key principle of sound budgeting
� MTEF provides 3 to 5-year forward estimates of expenditureGives more certainty in funding
20
� Gives more certainty in funding
� “tool for improving allocation of resources to strategic priorities”
� Integrates policy-making, planning & budgeting� (Top-down) forward estimates of what is affordable (ceiling)
� (Bottom-up) costing of policy
� Process to prioritise and match – balance needs against availability
� Costing as key components. � Estimates of “demand” and cost drivers (population profile; disease patterns)
� Activities and costs going forward

4.9 Autonomy & decentralisation
� Let the manager manage & keep them accountable for outputs
� Local knowledge
� Incentive to innovate & save or extend services
21
Incentive to innovate & save or extend services
� Risk of decentralisation and need for monitoring
� Both Rwanda & Ethiopia interesting cases� In both decentralisation identified as political imperative
� Needed public finance reform to ensure oversight
� Positive assessments of progress
• Ethiopia – high ranking in terms of PFM systems
• Rwanda – improvement in health service delivery and achievements – see case study

4.10 Execution aspects
22 From: Lawson et al. (2009) adaptation of PEFA criteria for Mozambique health

4.11 Accounting, recording &
reporting
23
From: Lawson et al. (2009) adaptation of PEFA criteria for Mozambique health
5. The impact of reform
Some assessments

5.1 Measuring impact of reform
• Anticipated impact:
• Budget decisions and resource allocations
• Technical or operational efficiency
25
• Technical or operational efficiency
• Service delivery outcomes
• Transparency and accountability
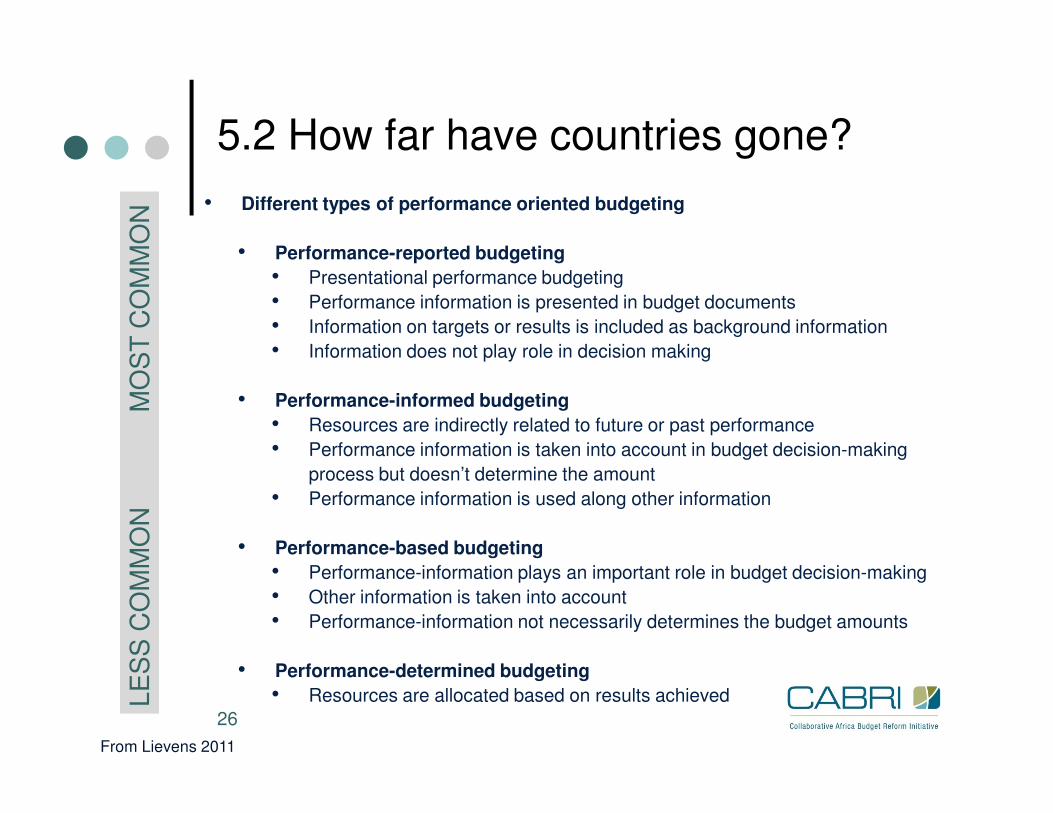
5.2 How far have countries gone?L
ES
S C
OM
MO
N M
OS
T C
OM
MO
N
• Different types of performance oriented budgeting
• Performance-reported budgeting
• Presentational performance budgeting
• Performance information is presented in budget documents
• Information on targets or results is included as background information
• Information does not play role in decision making
• Performance-informed budgeting
26
LE
SS
CO
MM
ON
M
OS
T C
OM
MO
N
• Performance-informed budgeting
• Resources are indirectly related to future or past performance
• Performance information is taken into account in budget decision-making
process but doesn’t determine the amount
• Performance information is used along other information
• Performance-based budgeting
• Performance-information plays an important role in budget decision-making
• Other information is taken into account
• Performance-information not necessarily determines the budget amounts
• Performance-determined budgeting
• Resources are allocated based on results achieved
From Lievens 2011

5.3 Ranking expenditure management (PEFA): scores for out-turn against approved budget
Ethiopia
27
Kenya
Botswana
DRC
http://www.pefa.org/en/dashboard/charts/multicountry

5.4 Impact? the state of health information
28Health Metrics Network (2012) …Current situation & trends

5.5 Assessments of impact
� Lievens (2011)
� Government-wide• Little hard evidence / mostly qualitative evidence
• Empirical focus mostly in OECD
• Mixed results
• Picture emerging: hypothesis is not rejected that if investments are made it can enhance …
efficiency
� Perhaps more sector-specific evidence but impact depends on mechanism & � Perhaps more sector-specific evidence but impact depends on mechanism &
context/Attribution an issues
� Peterson (2010) on Ethiopia:
� Hails Ethiopian success but argues that “”successful public reform is rare in
Africa … Reform of PFM has los its way”
� Andrews (2010) on Africa� “Budgets are made better than they are executed … & practice lags behind
the creation of processes and laws … an implementation deficit”
� The case of South Africa?
� Top the Open Budget Index 2010 (92%)
� Health service delivery and outcomes struggling (for some time)

5.6 Assessments of impact
� Fölscher (6 mini case studies for CABRI 2012):� Burkina Faso: impact “seen by many authors as limited”/”low impact in the first
ten years …”
� Ghana: “ … weak performance budgeting”/ “slow progress to a performance
orientation”
� Mali: by end of the decade “impact of programme budgeting was still seen as
limited”/”monitoring and evaluation remained weak”/”capacity in Supreme
30
limited”/”monitoring and evaluation remained weak”/”capacity in Supreme
Audit Institution … poor”
� Mauritius: “need for further work (costing of baselines …)” but “more
collaborative relationships between finance and line”/”budget submissions
have improved”/”budgets more transparent”
� Morocco: improved “quality of budget negotiations” and “particular cases of
service delivery improvement”/in some cases “improved discussions with the
finance ministry in terms of technical content and tenor” – “… ensured that the
focus was on the improvement of service delivery”
� Mozambique: Finance/Planning split “perpetuates weak linkages between
priorities”/ “Warren-Rodriguez identified “weak coordination and weak
planning”

5.7 Assessment of health information systems
� Heath Metrics Network 2011:
� “The findings … on country health information systems are not unexpected.
But they are nevertheless shocking.”
� “We are … realizing that our information systems are not equipped for
accurately tracking to what extent we are on course.”
� “… the basic foundations of a good health information system, i.e.
are inadequate in many countries.”
31
are inadequate in many countries.”
6. Identifying blockages and the way forward
How to structure the dialogue between health & finance going forward

6.1 What are the blockages?
� Suggestions form the literature
� Too much focus on change (& too many cooks)
(Peterson)
� Too little focus on support and training (Peterson?)
33
� Technique over context/too much similarity
(Andrews)
� Too much “concentration”/focus on the centre
(Andrews)
� Needs of the centre/centralisation

6.2 Way forward?
� Is the assessment correct?
� Is the assessment useful?
� Do we need to do things differently going forward?
� How?
� Some possible suggestions:
34
� Some possible suggestions:
� Working country and sectoral context into reform (recognise/improve/sustain – sometimes change - Peterson)
OR “addressing a locally defined problem” (USAID 2010)
� Respond to the needs of providers
� (An absolute commitment to decentralisation)?
� Focus on political imperatives & respond to those
� Start with the basics
� Not going far enough? RBF or P4P – Case study focus on Rwanda


















