
Presentation on Dyslipidemia on 20.11.13
56
Statin Evolution— Evidence, Efficacy, and Experience SENIOR GP CONSULTANT S1
-
Upload
drnasim20088171 -
Category
Documents
-
view
44 -
download
2
description
latest guidelies for dyslipidemia
Transcript of Presentation on Dyslipidemia on 20.11.13

Statin Evolution— Evidence, Efficacy, and Experience
SENIOR GP CONSULTANT
S1

DYSLIPIDEMIA
THE SILENT KILLER
DR. MOHAMMAD NASIM
SENIOR GP CONSULTANT
BADRUDDIN MEDICAL GROUP

WHAT IS DYSLIPIDEMIA?
DYSLIPIDEMIA IS A RANGE OF DISORDERS THAT INCLUDE ABNORMALLY HIGH AND LOW LEVELS OF LIPOPROTEINS AS WELL AS DISORDERS IN THE COMPOSITION OF THESE PARTICLES.

CAUSES
PRIMARY---
1.POLYGENIC HYPERCHOLESTROLEMIA
2.FAMILIAL HYPERCHOLESTEROLEMIA
3.FAMILIAL HYPERTRIGLYCERIDEMIA
4.CHYLOMICRONEMIA
5.FAMILIAL COMBINED DYSLIPIDEMIA

SECONDARY
1. TYPE 2 DYSLIPIDEMIA
2.EXCESSIVE ALCOHOL CONSUMPTION
3.CHOLESTATIC LIVER DISEASES
4.NEPHROTIC SYNDROME
5.CHRONIC RENAL FAILURE
6.HYPOTHYROIDISM
7.CIGARETTE SMOKING
8.OBESITY
9.DRUGS—RETINOIDS,ESTEROGENS/CONTRACEPTIVE PILLS,CORTICOSTEROIDS,CICLOSPORINS,DIURETICS,NON SELECTIVE BETA BLOCKER
10.SEDENTARY LIFESTYLE & EXCESSIVE INTAKE OF FATTY FOODS

SIGNS AND SYMPTOMS-
DERMATOLOGIC SIGNS
The most common dermatologic manifestation of dyslipidemia is xanthomas and xanthelasma.Xanthomas are firm and nontender cutaneous deposits of cholesteryl ester-enriched foam cells are most commonly observed with high levels of LDL. Xanthomas deposit in ligaments and tendons, although they may also be detected in periosteum and fascia. They are classified as tendinous, tuberous, tuberoeruptive, and planar. The most common location for tendinous xanthomas is the Achilles tendon[9] followed by the hands, feet, elbows, and knees

OPHTHALMOLOGIC SIGNS
Corneal Arcus
Corneal arcus is a grayish white opacification at the periphery of the cornea (Figure 1).[1] It is a particularly sensitive sign of familial hypercholesterolemia (FH), especially when detected in persons less than age 50 years, in which case it is also referred to as arcus juvenalis
Corneal Opacification
Patients with very low high-density lipoprotein (HDL) cholesterol because of mutations in regulatory genes may also exhibit ocular findings like corneal opacification.

Retinal Findings
In addition to the eruptive xanthomas that may accompany marked chylomicronemia, another important clinical sign is lipemia retinalis or a "milky-white" appearance of the retina.

MANAGEMENT-The management of lipid disorder greatly depends on the age, signs/symptoms of the affected persons. The following are remedies / treatment may apply to lower the level of LIPIDS in the body including:
Eat well-balanced diet – Almost fifteen (15) percent of cholesterol may decrease when strictly controlled. Eating foods that are naturally low in fat (whole grains, fruits, vegetables, etc.) a good sources of soluble fiber to prevent other health complications.
Weight Management
Exercise Regularly – (walking, yoga, dancing, etc.) – Exercise for at least thirty (30) minutes everyday. Maintain this habit and you will see the desired result.
Quit smoking – An important treatment to reduce the risk of heart disease and stroke.
Healthy Lifestyle – It is recommended that patients should eat fish, vegetables, in order to lower their cholesterol level.
Medicines / Drug Treatment – Available drugs for lowering cholesterol includes statins, bile acid, nicotinic acid, cholesterol absorption inhibitors. Helps in preventing the fastening of fatty deposits to arterial walls

MMNMM
MEDICAL MANAGEMENT—
1.STATIN– SIMVASTATIN,ATORVASTATIN,ROSUVASTATIN
2.FIBRATES
3.BILE ACID RESINS
4.NIACIN
5.NICOTINIC ACID
6.EZITIMIBE
7.FISH OIL

INCII
INCIDENCE IS MORE THAN HYPERTENSION AND DIABETES
RULE OF HALF APPLIES TO DYSLIPIODEMIA ALSO---HALF OF THE DYSLIPIDEMIA CASES ARE DIAGNOSED,HALF OF DIAGNOSED CASES BEING TREATED,HALF OF THE TREATED CASES ARE UNCONTROLLED

MANAGEMENT
The new guideline,ISSUED AT 12 NOV.,2013 BY ACC AND AHA, recommends moderate- or high-intensity statin therapy for these four groups:
Patients who have cardiovascular disease;
Patients with an LDL, or “bad” cholesterol level of 190 mg/dL or higher;
Patients with Type 2 diabetes who are between 40 and 75 years of age; and
Patients with an estimated 10-year risk of cardiovascular disease of 7.5 percent or higher who are between 40 and 75 years of age (the report provides formulas for calculating 10-year risk).

Atherosclerosis Timeline
Phase I: InitiationLDL-C plays a major role in initiating the development of atherosclerotic plaque.
Libby P. In: Heart Disease: A Textbook of Cardiovascular Medicine. 6th ed. Philadelphia, Pa: WB Saunders Co; 2001:995-1009; Libby P. J Intern Med. 2000;247:349-358.
Media
Intima
Phase II: ProgressionDisease progression results in the remodeling of the vascular wall so that the size of the lumen does not change significantly.
LDL-C
Phase III: ComplicationExtensive lipid accumulation and a greater inflammatory component can pose the threat of plaque rupture.
Lumen Unstable
Stable
S2

Lipid-lowering Goals
Joint European Societies1 LDL-C Goal
Established CHD, other atherosclerotic <115 mg/dL (3.0 mmol/L)
disease, or high absolute risk
US NCEP ATP III2
0-1 CHD risk factors <160 mg/dL (4.1 mmol/L)
>2 CHD risk factors <130 mg/dL (3.4 mmol/L)
CHD or CHD risk equivalent <100 mg/dL (2.6 mmol/L)
1 Wood D, et al. Atherosclerosis. 1998;140:1434-1503; 2 NCEP Expert Panel. JAMA. 2001;285:2486-2497. S3

Statin Evolution
• Evidence
• Efficacy
• Experience
S4

Statin Evidence: Landmark Statin Trials
*Extrapolated to 5 years
Adapted from Kastelein JP. Atherosclerosis. 1999;143(suppl 1):S17-S21.
S = statin treated P = placebo treated
Secondary prevention ( )Primary prevention ( )
Pravastatin
Lovastatin
Simvastatin
Atorvastatin
5.4 (210)2.3 (90) 2.8 (110) 3.4 (130) 3.9 (150) 4.4 (170) 4.9 (190)
0
5
10
15
20
25
AFCAPS-S
WOSCOPS-S
WOSCOPS-PCARE-S
LIPID-P
4S-P
LIPID-S
CARE-P
4S-S
AFCAPS-P
% w
ith
CH
D e
ven
t
LDL-C, mmol/L (mg/dL)
ASCOT-S*
ASCOT-P*
S5

Statin Evidence: Expanding Benefits
Acute coronary event
4S
CARE/LIPID
4 mo
No history of CAD Unstable CAD
3 mo
t = 0
6 mo
Stable CAD
Secondary preventionPrimary prevention
AFCAPS / TexCAPS/WOSCOPS
MIRACL
Hypertension
ASCOT-LLA
HPS
S6

Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22.
Hypertensionn = 8457 (41%)
with CHD1458 (7%)
no CHD1822 (9%)
with CHD4042 (20%)
no CHD2701 (13%)
with CHD1978 (10%)
no CHD3982 (19%)
no CHDno CHD2860 (2860 (14%)%)
with CHD5595 (27%)
with MI8510 (41%)
no MI4876 (24%)
20,536patients
PATIENT POPULATION
Statin Evidence: Heart Protection Study
CHDn = 13,379 (65%)
Diabetesn = 5963 (29%)
PVDn = 6748 (33%)
CVDn = 3280 (16%)
S7
Dr. J. Genest

Vascular event
Major coronary eventNonfatal MICoronary death
Stroke
Revascularization
ANY MAJOR VASCULAR EVENT
27% risk reductionP <.0001
25% risk reductionP <.000124% risk reductionP <.000124% risk reductionP <.0001
Simvastatin Placebo
better better
0.4 0.6 0.8 1.0 1.2 1.4
Risk ratio and 95% CI
Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22.
Statin Evidence: Heart Protection Study
S8

Statin Evidence: Heart Protection Study
24% risk reductionP < .0001
Simvastatin Placebo
better betterBaseline level
LDL-C (mg/dL)<100 (2.6 mmol/L)>100 < 130>130 (3.4 mmol/L)
ALL PATIENTS
0.4 0.6 0.8 1.0 1.2 1.4
Risk Ratio and 95% CI
Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22. S9

Statin Evidence: ASCOT-LLA
ASCOT is a multicenter, international trial that involves 2 treatment comparisons in a factorial design:
• A Prospective, Randomized, Open, Blinded End point (PROBE) design comparing 2 antihypertensive regimens
• A double-blind, placebo-controlled trial of atorvastatin 10 mg in a large prospective cohort of those hypertensive patients studied (lipid-lowering arm [ASCOT-LLA])
ASCOT is composed of almost 20,000 hypertensive patients with multiple risk factors for CHD
S10

Statin Evidence: ASCOT-LLA
R
9000 beta-blocker ± diuretic
9000 CCB ± ACEI
5000 TC <250 mg/dL(<6.5 mmol/L)
4000 TC >250 mg/dL (>6.5 mmol/L)
4000 TC >250 mg/dL (>6.5 mmol/L)
5000 TC <250 mg/dL(<6.5 mmol/L)
R
500 open lipid lowering
4500
2250 statin
2250 placebo
2250 placebo
2250 statin
R
4500500
open lipid lowering
+
8000 open lipid lowering
18,000 patientsR=Randomized
These are the target numbers of patients.
CCB=calcium channel blocker, ACEI=angiotensin converting enzyme inhibitor S11

Statin Evidence: ASCOT-LLA
Eligibility criteria for ASCOT-LLA
• SBP >160 mm Hg and/or DBP >100 mm Hg (untreated) or SBP >140 mm Hg and/or DBP >90 mm Hg (treated)
• TC <250 mg/dL (<6.5 mmol/L) and triglycerides <400 mg/dL (<4.5 mmol/L)
• 40-79 years of age
• 3+ CVD risk factors
• No history of CHD
Sever PS, et al. Lancet. 2003;361:1149-1158. S12
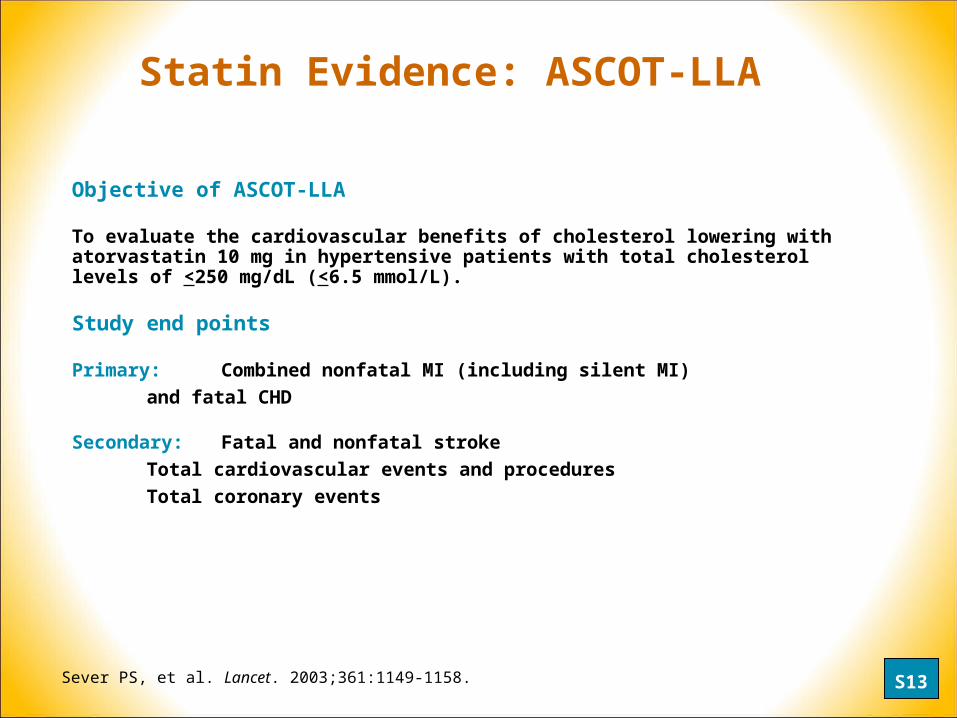
Objective of ASCOT-LLA
To evaluate the cardiovascular benefits of cholesterol lowering with atorvastatin 10 mg in hypertensive patients with total cholesterol levels of <250 mg/dL (<6.5 mmol/L).
Study end points
Primary: Combined nonfatal MI (including silent MI)
and fatal CHD
Secondary: Fatal and nonfatal stroke
Total cardiovascular events and procedures
Total coronary events
Statin Evidence: ASCOT-LLA
Sever PS, et al. Lancet. 2003;361:1149-1158. S13

September 2002
• The DSMB reported that in ASCOT-LLA there was a highly significant reduction in the primary end point as well as a significant reduction in stroke
• The DSMB recommended that the double-blind, cholesterol-lowering study treatment arm be terminated since the results were outside of the stopping rules of the trial
• The Steering Committee endorsed the recommendation of the DSMB, and the lipid arm was closed after a median follow-up period of 3.3 years; the blood pressure-lowering arm of the study is expected to complete in 2005
Statin Evidence: ASCOT-LLA
Sever PS, et al. Lancet. 2003;361:1149-1158. S14

19,342 patients randomized to antihypertensive treatment
10,305 randomized in lipid-lowering arm
5168 atorvastatin
4928 alive with complete information
185 dead with complete information
Incomplete information: 39 alive after Oct 1, 2002 4 alive before Oct 1, 2002 5 withdrew consent 7 lost to follow-up
212 dead with complete information
5137 placebo
4861 alive with complete information
Incomplete information: 42 alive after Oct 1, 2002 3 alive before Oct 1, 2002 9 withdrew consent 10 lost to follow-up
Complete information obtained on 98.8% of patients
Patient Inclusion and Follow-Up Status
Statin Evidence: ASCOT-LLA
S15

Atorvastatin 10 mgPlacebo
Baseline 164/95 mm HgTreated 138/80 mm Hg
130
140
150
160
170
0 1 2 3
SB
P (
mm
Hg
)
LLA Close-out
DB
P (
mm
Hg
)
75
80
85
90
95
100
0 1 2 3Years
LLA Close-out
Sever PS, et al. Lancet. 2003;361:1149-1158.
Blood Pressure Changes
Statin Evidence: ASCOT-LLA
S16

Statin Evidence: ASCOT-LLAT
ota
l ch
ole
ster
ol
(mm
ol/L
)L
DL
ch
ole
ster
ol
(mm
ol/L
)6
0 1 2 3
200
150
100
(mg
/dL
)50 mg/dL (1.3 mmol/L)
38.7 mg/dL (1.0 mmol/L)
2
4
Atorvastatin 10 mg
Placebo
150
75
125
100 (mg
/dL
)
YearsLLA Close-out
1
2
3
4
0 1 2 3
Sever PS, et al. Lancet. 2003;361:1149-1158.
38.7 mg/dL (1.0 mmol/L)
46.5 mg/dL (1.2 mmol/L)
S17

Atorvastatin 10 mg Number of events 89
Placebo Number of events 121
0
1
2
3
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
Years
Cu
mu
lati
ve I
nci
den
ce (
%)
HR = 0.73 (0.56-0.96)P = .0236
27% reduction
Statin Evidence: ASCOT-LLA
Primary Endpoint:
Nonfatal MI and Fatal CHD
Secondary Endpoint:
Fatal and Nonfatal Stroke
0
1
2
3
4
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
Years
Cu
mu
lati
ve
Inc
ide
nc
e (
%)
Atorvastatin 10 mg Number of events 100
Placebo Number of events 154
36% reduction
HR = 0.64 (0.50-0.83)P = .0005
Sever PS, et al. Lancet. 2003;361:1149-1158. S18

Statin Evidence: ASCOT-LLA
Secondary Endpoint:
All CV Events and Procedures
Secondary Endpoint:
All Coronary Events
0
2
4
6
8
10
12
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
Years
Cu
mu
lati
ve
In
cid
en
ce
(%
) 21% reduction
HR = 0.79 (0.69-0.90)P = .0005
Atorvastatin 10 mg Number of events 389
Placebo Number of events 486
Atorvastatin 10 mg Number of events 178
Placebo Number of events 247
0
1
2
3
4
5
6
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
Years
Cu
mu
lati
ve
In
cid
en
ce
(%
) 29% reduction
HR = 0.71 (0.59-0.86)P = .0005
Sever PS, et al. Lancet. 2003;361:1149-1158. S19

Safety
• No significant difference between atorvastatin and placebo in:
• Incidence of fatal cancers• Incidence of serious adverse events• Incidence of liver enzyme abnormalities
Statin Evidence: ASCOT-LLA
Sever PS, et al. Lancet. 2003;361:1149-1158. S20

• Large given the short follow-up time (median 3.3 years) and emerged earlier than in many other statin trials
• Not significantly different among prespecified subgroups
• Unrelated to baseline cholesterol levels
• Occurred in the absence of any significant increase in adverse events.
Statin Evidence: ASCOT-LLA
The benefits of atorvastatin therapy in well-managed hypertensive patients at modest risk of cardiovascular events and with normal to mildly elevated cholesterol levels were:
S21

Schwartz GG, et al. JAMA. 2001;285:1711-1718.
Statin Evidence: MIRACL Study
Placebo plus usual care
Initial
hospitalization
Randomization(1-4 days)
3086 patients
Double-blind period
Atorvastatin 80 mg/day
16-week treatment phase
S22

Statin Evidence: MIRACL Study
Relative risk = 0.84P = .04895% CI 0.701-0.999
Atorvastatin
Placebo
0
5
10
15
0 4 8 12 16
Time Since Randomization (weeks)
Cu
mu
lati
ve In
cid
ence
(%
)
Time to first occurrence of:• Death (any cause)• Nonfatal MI• Resuscitated cardiac arrest• Worsening angina with new
objective evidence and urgent rehospitalization
17.4%
14.8%
Primary Efficacy Measure
Schwartz GG, et al. JAMA. 2001;285:1711-1718. S23

Statin Evidence: MIRACL Study
0
0.5
1
1.5
2
0 4 8 12 16
Time Since Randomization (weeks)
Cu
mu
lati
ve In
cid
ence
(%
)
Relative risk = 0.49P = .0495% CI 0.24-0.98
Atorvastatin
Placebo
Fatal and Nonfatal Stroke
Waters DD, et al. Circulation. 2002;106:1690-1695. S24

Αthyros VG, et al. Curr Med Res Opin. 2002;18:220-228.
Statin Evidence: GREACE Study
Begin recruitment January 1998
End recruitment November 1999
End of study December 2001
Mean follow-up, 3 years
Structured care (n = 800)Atorvastatin 10 to 80 mg/dGoal: LDL-C < 100 mg/dL
Usual care (n = 800)
1600 hypercholesterolemic patients with CHD
(LDL-C > 100 mg/dL[ > 2.59 mmol/L] after 6-week
trial of lipid-lowering diet)
S25

-4
-36
-5
-46
-3
-31
27
-3
-32
-6
-44
-60
-50
-40
-30
-20
-10
0
10
Total-C LDL-C TG HDL-C VLDL-C Non-HDL-C
Statin Evidence: GREACE Study
Athyros VG, et al. Curr Med Res Opin. 2002;18:220-228.
**
**
** **
**
††
Mea
n %
Ch
ang
e F
rom
Bas
elin
e
Usual Care
Structured Care
*P < .0001; †P = .0028. Mean atorvastatin dose, 24 mg/day.
S26
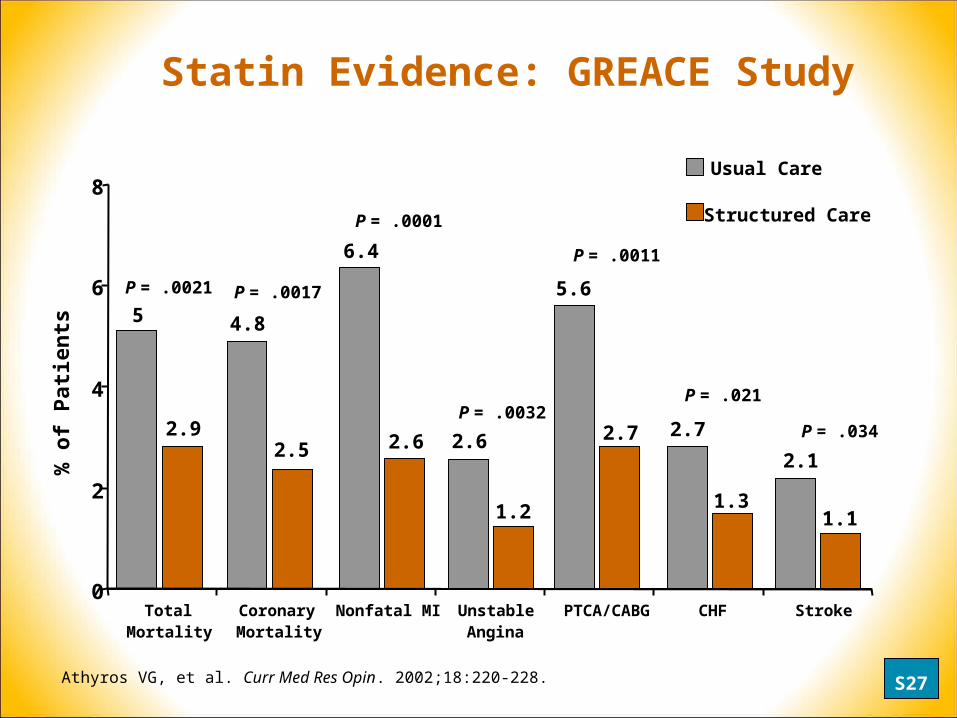
5
2.9
4.8
2.5
6.4
2.6 2.6
1.2
5.6
2.7 2.7
1.3
2.1
1.1
0
2
4
6
8
TotalMortality
CoronaryMortality
Nonfatal MI UnstableAngina
PTCA/CABG CHF Stroke
Statin Evidence: GREACE Study
P = .0021 P = .0017
P = .0011
P = .034
Athyros VG, et al. Curr Med Res Opin. 2002;18:220-228.
% o
f P
atie
nts
P = .0001
P = .0032P = .021
Usual Care
Structured Care
S27

Statin Evidence: GREACE Study
Structured Care Group
• 95% of patients reached the NCEP LDL-C goal
• Mean dose of atorvastatin 24 mg/day
• 96% of patients reached the European LDL-C goal
• Mean dose of atorvastatin was 22 mg/day
Usual Care Group
• 3% of patients reached the NCEP LDL-C goal
• 5.5% of patients reached the European LDL-C goal
Athyros VG, et al. Curr Med Res Opin. 2002;18:220-228; Athyros VG, et al. Data on file. S28

Statin Evidence: Benefits
• The statin trials have demonstrated significant decreases in
CVD morbidity and mortality.
• Reduction in CVD events has been demonstrated in patients
with stable CHD as well as acute coronary syndrome patients.
• Additionally, lowering LDL-C to target levels has beneficial
effects in patients with normal or moderately elevated LDL-C.
S29
Statin Evolution
• Evidence
• Efficacy
• Experience
S30

Drug Class LDL-C HDL-C Triglycerides
Statins* 18% to 60%*** 5% to 15% 7% to 37%***
Bile Acid 15% to 30% 3% to 5% No change or
Sequestrants increase
Nicotinic Acid 5% to 25% 15% to 35% 20% to 50%
Fibric Acids 5% to 20%** 10% to 20% 20% to 50%
Statin Efficacy: Lipid Lowering
*Lovastatin (20 to 80 mg), pravastatin (20 to 40 mg), simvastatin (20 to 80 mg), fluvastatin (20 to 80 mg), atorvastatin (10 to 80 mg), and rosuvastatin (10 to 40 mg).
**May be increased in patients with high triglycerides.
***Up to 60% reduction in LDL-C, and 37% reduction in triglycerides, as indicated in the atorvastatin PI.
Adapted from NCEP Expert Panel. JAMA. 2001;285:2486-2497. S31
v
v
v
v
v
v
v
v
v
v
v

Statin Efficacy: LDL-C Reduction
*Simvastatin 80 mg not available at time of study. **Significantly greater than mg-equivalent doses of comparative agents (P <.01). †Significantly less than atorvastatin 10 mg (P <.02). ‡Significantly less than atorvastatin 20 mg (P <.01).
Jones P, et al, for the CURVES Investigators. Am J Cardiol. 1998;81:582-587.
Atorvastatin
Simvastatin*
Pravastatin
Lovastatin
Fluvastatin
0 -60-50-40-30-20-10
10 mg (n = 73)
20 mg (n = 51)
40 mg (n = 61)
10 mg (n = 70)
20 mg (n = 49)
40 mg (n = 61)
10 mg (n = 14)
20 mg (n = 41)40 mg (n = 25)
20 mg (n = 16)40 mg (n = 16)
40 mg (n = 12)
20 mg (n = 12)
-38%**-46%**
-51%**
-28%†
-35%‡
-41%‡
-19%†
-24%†
-34%‡
-29%†
-31%†‡
-17%†
-23%†‡
80 mg (n = 10) -54%
80 mg (n = 11) -48%
% LDL-C reduction
S32

Primary efficacy parameter:
Reduction in plasma LDL-C from baseline
Men and women
With or without CHD and/or PAD
Type IIa/IIb
TG < 400 mg/dL (4.5 mmol/L)
~ 70% with CHD and/or PAD
Atorvastatin 10 to 80 mg
Simvastatin 10 to 40 mg
Pravastatin 10 to 40 mg
Lovastatin 10 to 80 mg
Fluvastatin 20 to 80 mg
54 week open-label treatment
Statin Efficacy: ACCESS
Andrews TC, et al. Am J Med. 2001;111:185-191. S33
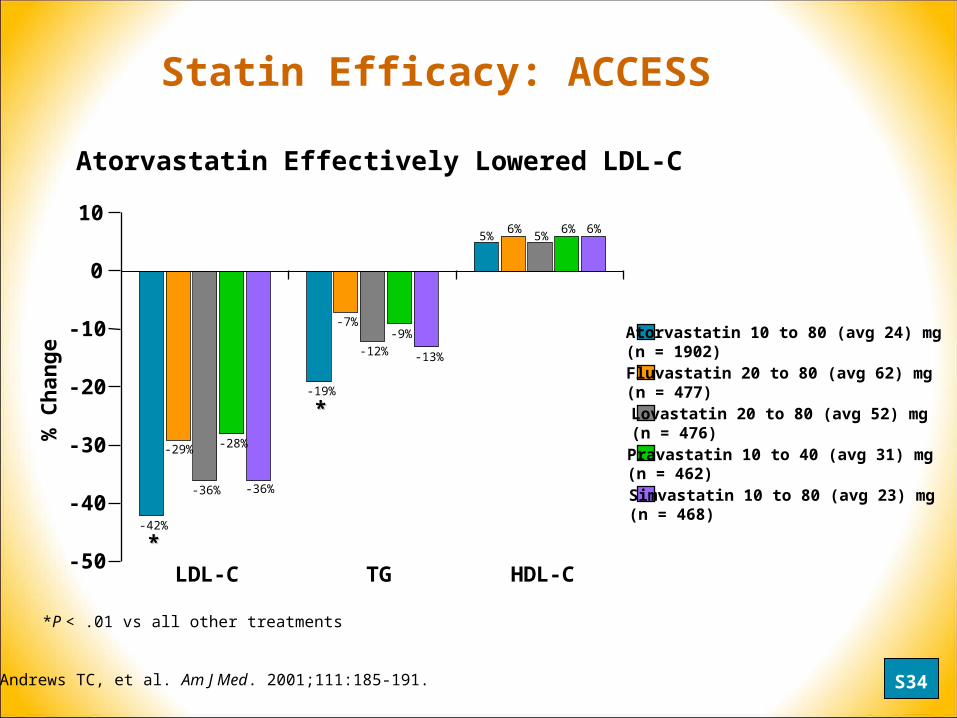
Andrews TC, et al. Am J Med. 2001;111:185-191.
*P < .01 vs all other treatments
Atorvastatin Effectively Lowered LDL-C
% C
han
ge
LDL-C TG HDL-C
**
**
-42%
-29%
-36%
-28%
-36%
-19%
-7%
-12%
-9%
-13%
5%6%
10
0
-10
-20
-30
-40
-50
5%6% 6%
Atorvastatin 10 to 80 (avg 24) mg (n = 1902)Fluvastatin 20 to 80 (avg 62) mg (n = 477)
Simvastatin 10 to 80 (avg 23) mg (n = 468)
Lovastatin 20 to 80 (avg 52) mg(n = 476) Pravastatin 10 to 40 (avg 31) mg (n = 462)
Statin Efficacy: ACCESS
S34

Statin Efficacy: ACCESS
*Significant difference vs atorvastatin (P < 0.05)
*
**
*
0
25
50
100
Atorvastatin10 to 80 mg
Per
cen
t o
f p
atie
nts
ach
ievi
ng
go
al
75
Simvastatin10 to 80 mg
Pravastatin10 to 40 mg
Lovastatin20 to 80 mg
Fluvastatin20 to 80 mg
NCEP ATP II LDL-C Goals< 2 CHD risk factors is < 160 mg/dL (4.1 mmol/L)
> 2 CHD risk factors is < 130 mg/dL (3.4 mmol/L)Andrews TC, et al. Am J Med. 2001;111:185-191.
NCEP Goal Attainment
S35
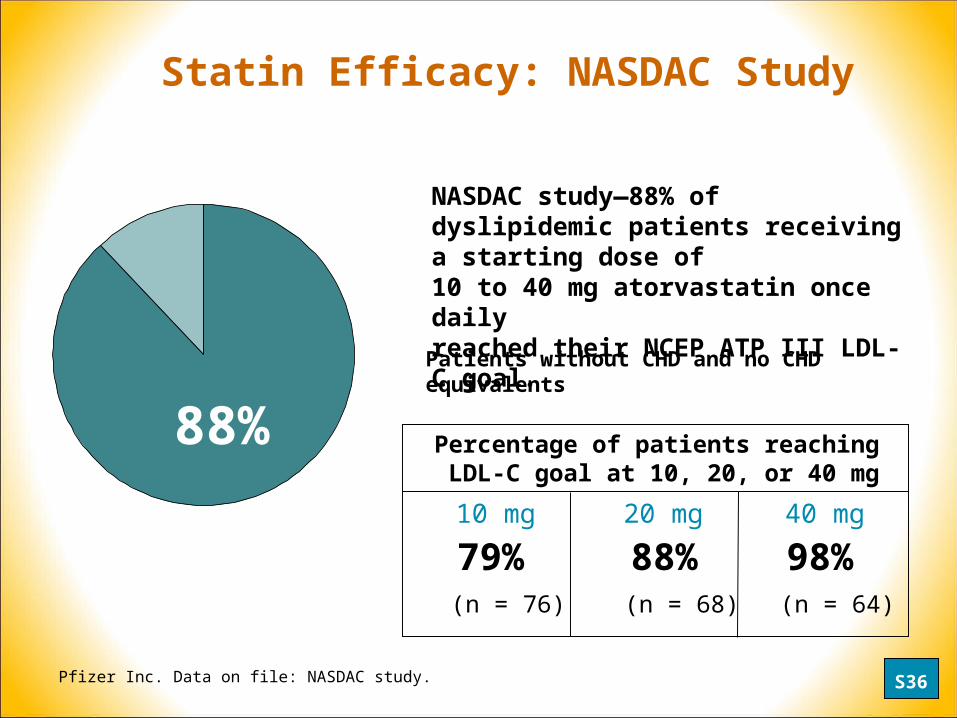
Statin Efficacy: NASDAC Study
NASDAC study—88% of dyslipidemic patients receiving a starting dose of 10 to 40 mg atorvastatin once daily reached their NCEP ATP III LDL-C goal.
88% Percentage of patients reaching LDL-C goal at 10, 20, or 40 mg
10 mg 20 mg 40 mg
79% 88% 98%(n = 76) (n = 68) (n = 64)
Patients without CHD and no CHD equivalents
Pfizer Inc. Data on file: NASDAC study. S36

Statin Efficacy: Atorvastatin
• Excellent efficacy across the dose range for all lipid parameters:
LDL-C -39% to -60%
Triglycerides -19% to -37%
HDL-C +5% to +9%
• In clinical trials, the vast majority of patients onatorvastatin reached LDL-C goal.
Pfizer Inc. Data on file. S37

Statin Evolution
• Evidence
• Efficacy
• Experience
S38

Atorvastatin Experience: Clinical Safety Data
• Safety of atorvastatin derived from analysis of 44 completed
clinical trials in 9416 patients:
• Involved many different patient types:
• eg, mixed dyslipidemia, diabetes, postmenopausal women, FH
Source: Pfizer Inc. Data on file. Review of 44 completed clinical trials.
Atorvastatin (all doses) 9416
Other statins 5290
Placebo 1789
n
S39

Source: Pfizer Inc. Data on file. Review of 44 completed clinical trials.
Atorvastatin Experience: Clinical Safety Data
Digestive 4 8 9Body as a whole 5 5 6Musculoskeletal 1 3 4Nervous 2 3 3Skin and appendages 1 2 2Metabolic/Nutritional 1 1 1Special senses < 1 1 < 1Urogenital 1 1 1Cardiovascular 2 1 1
Body system
Placebon = 1789
Atorvastatin(all doses)n = 9416
All other statins combined
n = 5290
(%)
Treatment-Associated AEs > 1% of Patients
(%) (%)
S40

Patient Withdrawal due to Treatment-Associated AEs
Atorvastatin(all doses)
n = 241/9416
2.6%
5
4
3
2
0All other
statins combined n = 188/5290
3.6%
1
Pat
ien
ts w
ith
dra
win
g d
ue
to t
reat
men
t-as
soci
ated
ad
vers
e ev
ents
(%
)
0.9%
Placebo n = 16/1789
Source: Pfizer Inc. Data on file. Review of 44 completed clinical trials.
Atorvastatin Experience: Clinical Safety Data
S41

Atorvastatin Experience: Clinical Safety Data
• ALT/AST elevations > 3x ULN:
• 0.5% of patients treated with atorvastatin 10 to 80 mg experienced ALT/AST elevations > 3x ULN.
• Myalgia
• Incidence of myalgia across all the atorvastatin doses was low (1.9%) and directly comparable to the incidence of myalgia observed in patients receiving other statins combined.
Source: Pfizer Inc. Data on file. Review of 44 completed clinical trials. S42

Atorvastatin Experience: Summary
Source: Pfizer Inc. Data on file. Review of 44 completed clinical trials.
• A recent analysis of 44 completed clinical trials demonstrated
that atorvastatin is well tolerated and has excellent safety
across the 10 mg to 80 mg atorvastatin dose range.
• The overall incidence of AEs with atorvastatin in clinical trials
does not increase across the dose range, and is similar to
that observed with placebo, and in patients treated with other
statins.
• Specific analysis of musculoskeletal and hepatic AEs showed
that these occurred infrequently and rarely resulted in
treatment discontinuation.
S43

Atorvastatin Clinical Trial Program (> 44,000 Patients)
Atorvastatin Evolution: Future
2003 2004
TNT
4D
SAGE
BONES
SPARKS
BELLES
CARDS
ASPEN
ASCOT
REVERSAL LEADe
S44

Atorvastatin Evolution
• Evidence
• Efficacy
• Experience
When choosing a statin consider:
S45










![Treating Diabetes and Dyslipidemia: Achieving …1]Part_2_Treating... · Treating Diabetes and Dyslipidemia: Achieving Therapeutic Targets: Goals for Diabetes and Dyslipidemia Treatment](https://static.fdocuments.net/doc/165x107/5bc182c709d3f2c7178dc2a1/treating-diabetes-and-dyslipidemia-achieving-1part2treating-treating.jpg)







