
PRESENTATION Diabetes and the Eye - CAO Diabetes and the Eye . Public Health Concern 1. Diabetes...
50
PRESENTATION Diabetes and the Eye
Transcript of PRESENTATION Diabetes and the Eye - CAO Diabetes and the Eye . Public Health Concern 1. Diabetes...

PRESENTATION
Diabetes and the Eye

Public Health Concern
1. Diabetes Canada. 2017. Diabetes Statistics in Canada2. CDA Clinical Practice Guideline Expert Committee. CDA clinical practice guidelines for theprevention and management of diabetes in Canada. Can J Diabetes. 2003;27(Suppl 1):S1-S152.
• Type 1 and 2 Diabetes Mellitus is a growingpublic health concern in Canada
• Projected prevalence to reach 5.0 million in20251
• In Canada, only 32% of DM2 have annual examsfor diabetic eye disease2

Diabetes and the Eye
1. J.H. Kempmen B.J. O'Colmain M.C. Leske The prevelance of diabetic retinopathy amongadults in the United States Arch Opthlalmology 122 2004 552 563
• Diabetes is the most commoncause of new cases of legalblindness in people of workingage1
• Diabetes can cause changes tovirtually all structures of the eye
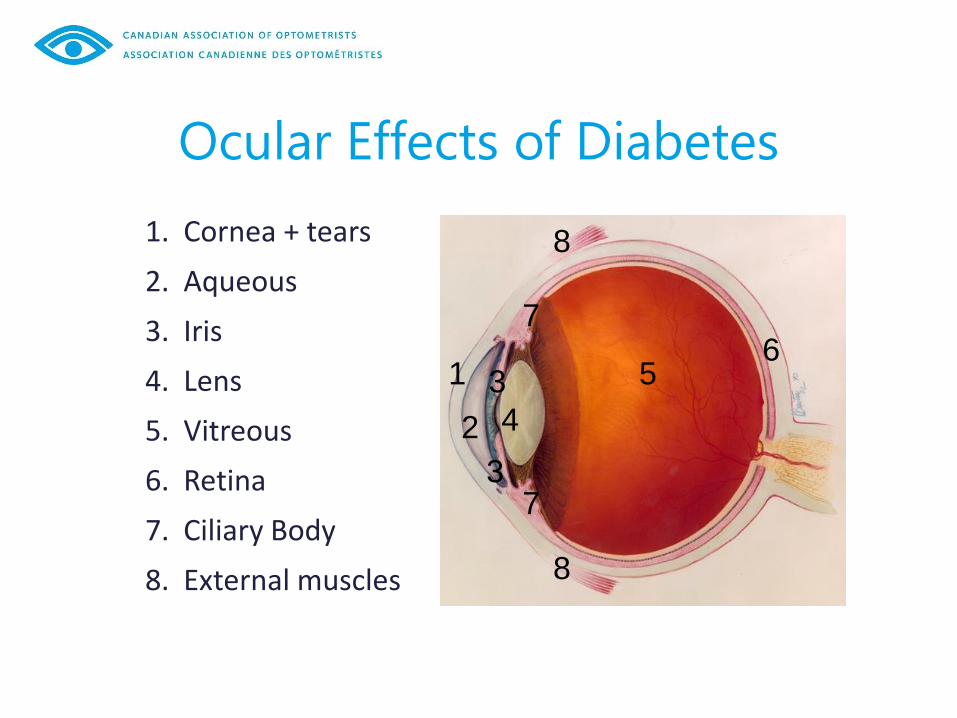
Ocular Effects of Diabetes
1. Cornea + tears
2. Aqueous
3. Iris
4. Lens
5. Vitreous
6. Retina
7. Ciliary Body
8. External muscles
6 1 3
3
5
8
8
7
7
4 2

Fluctuating Vision
Diabetes can cause large shifts in refractive error (nearsightedness and farsightedness) as blood sugar levels fluctuate

Anterior Segment: Dry Eye • More than 50% of patients with diabetes will
suffer from dry eye disease1
• Autonomic neuropathy – affects nerves thatcontrol the lacrimal gland resulting indecreased tear production
• Leads to corneal damage andsymptoms of dryness, irritation, etc.
• Reduced corneal sensation over time• Delayed healing• Reduced tear film – tear proteins
altered, increased MGD• Increase Demodicosis (Demodex)
1. Manaviat MR,Rashidi M,Afkhami-Ardekani M,Shoja MR.Prevalence of dry eye syndrome anddiabetic retinopathy in type 2 diabetic patients.BMC Ophthalmol. 2008;8:10.

Cataracts Major cause of vision impairment in patients with diabetes: • Earlier development in patients with diabetes1
• Suggested that patients with DM have higher complication rate following cataract surgery1
1. P. E. Stanga, S. R. Boyd, and A. M. P. Hamilton, “Ocular manifestations of diabetes mellitus,” Current Opinion in Ophthalmology, vol. 10, no. 6, pp. 483–489, 1999

Cranial Nerve Palsies
Common Presentation
• Acute onset diplopia• Gaze restrictions and eye deviation• 3rd nerve: ptosis, usually pupil sparing• Unilateral headache• Often resolves in a few months
6th nerve palsy
3rd nerve palsy with ptosis
• Isolated 3rd nerve (Ocular Motor Nerve)and 6th nerve (Abducens) are mostcommon
• 4th nerve palsy (Trochlear) is lesscommon
• Poorly controlled diabetes• Usually with comorbity of HTN,
cardiovascular disease

Glaucoma
Link between DM and Glaucoma is still not fully understood • Generally accepted that patients with poorly controlled
DM are more likely to develop glaucoma

Diabetic Retinopathy Prevalence
1. Diabetes Canada. 2017. Eye Damage (Diabetic Retinopathy)
It is estimated that almost all people with diagnosed diabetes have some form of diabetic retinopathy
• Retinopathy affects 23% of people with type 1 diabetes and 14% of people with type 2 diabetes on insulin therapy1

Risk Factors for Retinopathy
Non-Modifiable:
• Type of Diabetes (IDDM higher risk
than NIDDM)
• Ethnicity
• Aboriginal, Hispanic, South Asian,
Asian, and African are at higher risk
• Sex (male higher risk)
• Puberty (type 1)
• Pregnancy

Risk Factors for Retinopathy
Modifiable:
• Hyperglycemia
• High blood pressure
• Reduction of BP decreases risk of DR
and macular edema in Type 2 DM
• Elevated Lipid Serum Levels
• High levels of triglycerides, high LDL,
very-low density lipoproteins may lead to
macular edema
• Smoking

What is Diabetic Retinopathy?
Over time, diabetes will affect the
circulatory system of the retina
• Non-proliferative diabetic retinopathy can
proceed to vision threatening
proliferative diabetic retinopathy
• End organ response to systemic disease

What is Diabetic Retinopathy?

Development of Diabetic Retinopathy
• Basement membrane thickening
• Pericyte loss
• Smooth muscle cell depletion
• Vascular endothelial cell loss
• Vascular occlusion and re-canalization
• Neovascularization

Development of Diabetic Retinopathy

Types of Diabetic Retinopathy
• Macular Edema
• Non-proliferative Diabetic Retinopathy
• Proliferative Diabetic Retinopathy

Diabetic Macular Edema (DME) Mechanism for the development of macular edema is
similar to that for tissue edema elsewhere in the body
• Increased intravascular hydrostatic pressure drives
fluid across the vascular wall, causing fluid
accumulation in the macula
• Can occur at any stage of Diabetic Retinopathy:
• Causes a decrease in visual acuity
• Usually treated with focal laser photocoagulation an/or anti-VEGF intravitreal injections

Non-Proliferative Diabetic Retinopathy
Ischemic blood vessel changes
• Microaneurysms
• Intraretinal hemorrhages
• Cotton wool spots
• Vascular tortuosity and malformation
• Patients are often asymptomatic

Non-Proliferative Diabetic Retinopathy
Flame and blot hemorrhages and microaneurysms
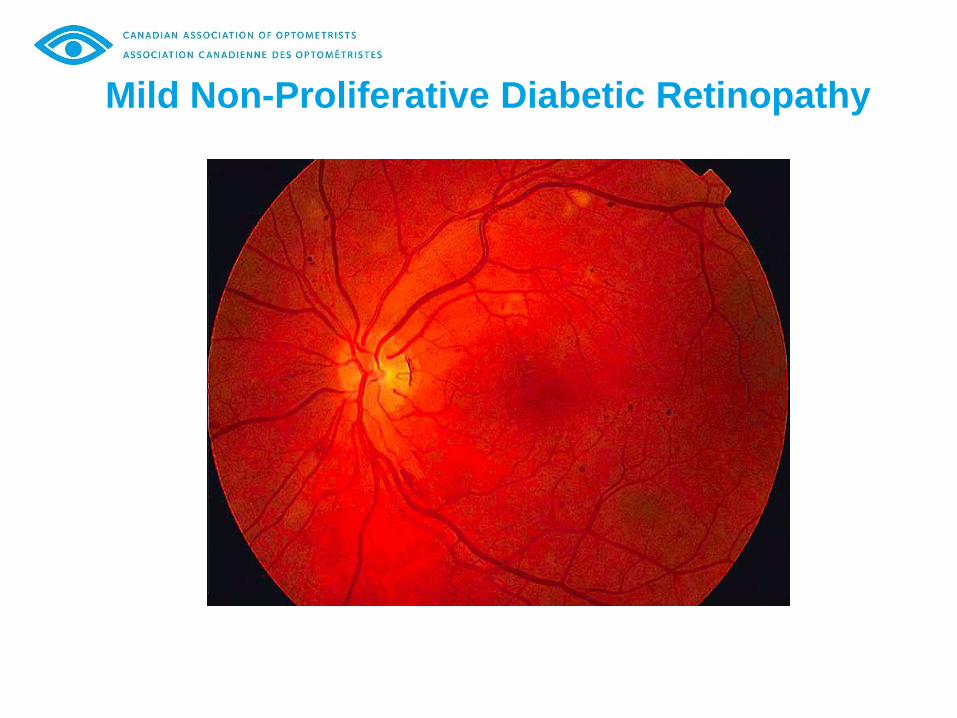
Mild Non-Proliferative Diabetic Retinopathy

Moderate Non-Proliferative Diabetic Retinopathy

Severe Non-Proliferative Diabetic Retinopathy

Omega Loop
Omega Loop
• From severe localized retinal
ischemia
• Seen in very severe NPDR
• Should be monitored within 3
months as can quickly
progress to PDR

Proliferative Diabetic Retinopathy
Ischemia leads to neovascularization in the retina
• Abnormal blood vessel growth
• These new vessels tend to leak
• Vitreous hemorrhages, Tractional Retinal Detachments
• High risk of severe irreversible vision loss

Proliferative Diabetic Retinopathy
Normal Neovascularization of the disc (NVD)

Proliferative DR
Neovascularization Pre-retinal (sub-hyaloid heme)

Proliferative DR
Vitreous Hemorrhage
Pre-retinal fibrosis/tractional RD

When is 20/20 Vision Lost?
When does a diabetic stop seeing 20/20 vision?
A.Moderate Non-Proliferative DR
B.Severe Non-Proliferative DR
C.Proliferative DR without macular edema
D.None of the above
One can still see 20/20 in advanced stages
if the macula is still intact

Example of Referral Guideline
To Retinal Specialist Immediate Referral Endophthalmitis
Intraocular foreign body
Ruptured globe – send to General Ophthalmologist that is On-Call
Central Retina Artery Occlusion (CRAO) – if acute (<6 hours)
Within 24 Hours Retinal Detachment
Retinal Tear
Vitreous Hemorrhage
Neovascular Glaucoma
Branch or Central Retinal Artery Occlusion
Papilledema – Swelling of Optic Disc

Retina Referral Guideline (cont'd) Within 1 Week Choroidal Neovascular Membrane (wet AMD, myopia, Histoplasmosis)
Sub retinal Hemorrhage (AMD, Trauma, Retina Arterial Macroaneurysm)
Uveitis – that threatens the disc or macula
Proliferative Diabetic Retinopathy
Dislocated Crystalline or Intraocular Lens
Within 2 Weeks Diabetic Macular Edema
Retinal Vein Occlusion (BRVO,CRVO)
Central Serous Chorioretinopathy (CSCR)
PVD – No Symptoms
Full Thickness Macular Hole (FTMH)
Posterior Segment Tumors (Melanoma)
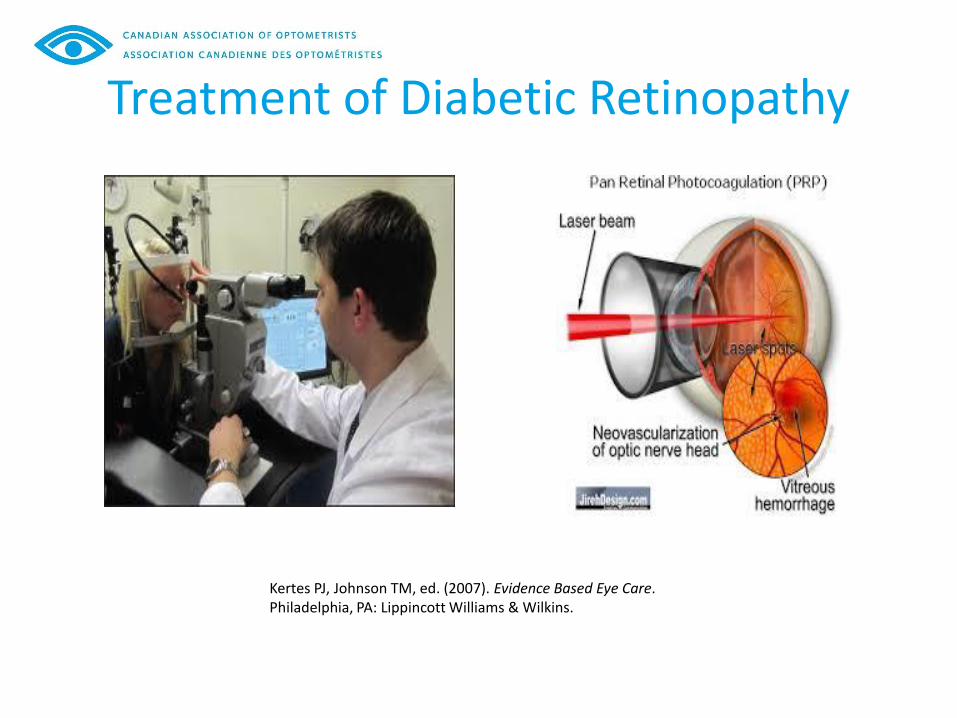
Treatment of Diabetic Retinopathy
Kertes PJ, Johnson TM, ed. (2007). Evidence Based Eye Care. Philadelphia, PA: Lippincott Williams & Wilkins.

Laser Treatment for DR
Panretinal Photocoagulation (PRP): AKA “Scatter” • Gold standard for proliferative diabetic
retinopathy• Decreases VEGF levels and causes resorption
of new blood vessels and stops new bloodvessels from forming

Laser Treatment for DR
1. F.L. Ferris 3rd How effective are treatments for diabetic retinopathy? JAMA 269 1993 12901291
2. Photocoagulation treatment of proliferative DR: the second report of the DRS findingsOpthalmology 85 1978 82 106
3. F. Ferris Early photocoagulation in patients with either type I or type II diabetes Trans AmOpthalmol Soc 94 1996 505 537
• Multiple laser spots throughout the peripheral retina
needed
• Has been shown to reduce legal blindness by 90%
in those with severe NPDR or PDR1-3
• Will cause peripheral vision loss but save central
vision

PanRetinal PhotoCoagulation (PRP)

Laser Treatment for Macula
1. Early treatment diabetic retinopathy study (ETDRS)
Focal laser photocoagulation
• Small area of laser applied to retina
to decrease swelling from macular
edema
• 50% decrease in edema1

Intravitreal Injections
Anti-VEGF Therapy
• Helps prevent leakage of blood vessels causing
macular edema
• Helps prevent development of neovascularization
• Needs more than one treatment
• Often monthly until stabilized
• Usually done in conjuction with PRP
• May cause subconjunctival hemorrhages, mild
eye pain, floaters, inflammation of eye, visual disturbances
• Side effects can be managed by Optometrists

Intravitreal Injections

Vision Rehabilitation
In some unfortunate patients, vision loss is inevitable
• Many optometrists offer low vision services to help
with aids and vision rehabilitation

Intensive Insulin Therapy
1. UKPDS (United Kingdom Prospective Diabetes Study)
Type 1 DM:
• Intensive insulin therapy reduced
development and progression of retinopathy1
• 3 or more dailyType 2 DM:
• Intensive insulin therapy reduced microvascular
complication rate by 25%1
• Every percentage point decreased inbHbA1c (e.g., 9 to 8%), there was a 35%reduction in the risk of microvascularcomplications1

Targets for Prevention
The ABCDEs:1
A A1c -optimal glycemic control <7%
B BP -optimal blood pressure control <130/80 mmHG
C Cholesterol LDL-C <2.0mmol/L if decision made to treat D Drugs to protect the heart A-ACE or ARB, S-Statin, A-ASA
if indicated
E Exercise – regular physical activity and healthy diet S Smoking cessation
1. 2013 CDA Clinical Practical Guidelines

Prevention
Nutrition:
• High fiber diet, low fat = less proliferative diabetic
retinopathy
• Anti-Inflammatory nutrition
• GHA and EPA
• Vitamin D
• Anti-Oxidant nutrition• Carotenoids (lutein and zeaxanthin)

Prevention
Ensure patients are getting routine eye examinations
CLASSIFICATION RECOMMENDED INITIAL EXAM1
Type 1 5 years after onset >= 15 yrs old (not needed <15)
Type 2 At time of diagnosis
Pregnancy Prior to conception and early in 1st trimester
1. 2013 CDA Clinical Practice Guidelines

Diabetic Retinopathy Follow-up1
NO NPDR Q 1-2 years by Optometrist or General Ophthalmologist
Mild NPDR </= 1yr by Optometrist or General Ophthalmologist
Moderate NPDR </= 1yr by Optometrist or General Ophthalmologist Severe NPDR or Any PDR Referral to General Ophthalmologist or Retinal Specialist
DME Referral to General Ophthalmologist or Retinal Specialist
1. 2013 CDA Clinical Practice Guidelines

Co-management Communication is necessary to improve quality of care
and prevent blindness.
Helping prepare the patients for their eye exam:
• Name of primary care physician/NP
• List of medications
• Blood work results (at least las A1c)
• Educate them on a dilated eye exam
• Remind them to have the eye examination report sent to other eye health provider or physician

Diabetic Retinopathy
Screening and Diagnosis Method Retinal examination through a dilated pupil by an optometrist or ophthalmologist (ophthalmoscopy or indirect slit-lamp fundoscopy or fundus photography)

Telemedicine
IT IS NOT A SUBSTITUTE FOR A COMPREHENSIVE EYE EXAM
(WILL NOT DETECT SOME EYE DISEASES, SOME DME AND VISION REDUCTION)
• Digital retinal photographs performed and interpretedremotely by a trained reader
• Only should be used in rural areas where access to anoptometrist or ophthalmologist is unavailable for adilated retinal exam

Key Messages
• Early detection/treatment is important
• Improve communication of health care
team for earlier intervention and
management
• Tight control of BS, BP, Lipids
• Low vision services for permanent
vision loss

Optometry’s Role
75% OF BLINDNESS IS PREVENTABLE
• Optometrists can diagnose and stage DR and
refer timely to ophthalmologist (eg DME)• Many already have an Optometrist they see regularly• Optometrists also manage other concurrent optical
and ocular conditions• No referral to Optometrist needed
• Often longer wait for opthamologist, especially ifno diagnosis
• Optometrists can reinforce compliance

Diabetes and the Eye
Questions?


















