Kamerabaseret udpegning af svin TEST Torben Gregersen IHA/ASE
Upload
itinera-instituteCategory
view
554download
0
28/01/2014
Doctoral thesis in Biomedical Sciences, KU Leuven
Promoter: Prof. Dr. Walter Sermeus; Co-Promoters: Prof. Dr. Martin Euwema & Dr. Kris Vanhaecht
MAKING TEAMS WORK: Care pathways as a tool to improve teamwork and
prevent burnout
dr. Svin Deneckere

28/01/2014
MAKING TEAMS WORK
OUTLINE
Growing need for teamwork in healthcare
How could care pathways improve teamwork?
Setting of the PhD-study
Objectives, research questions and included studies
Study results
General discussion and recommendations

28/01/2014
Why teamwork in healthcare?
As many as 44.000 to 98.000
people die in hospitals each
year as the result of medical
errors.
Medical errors are the eighth
leading cause of death in
U.S. – much higher than
motor vehicle accidents
(43.458), breast cancer
(42.297), or AIDS (16.516).
About 10% of patients
hospitalized were harmed by
the care they received Kohn et al. (1999). To Err Is Human:
Building A Safer Health System.
Washington DC: National Academic Press.

28/01/2014
1
10
100
1000
10000
100000
1 10 100 1000 10000 100000 1000000 10000000
Number of encounters for each fatality
To
tal
liv
es l
os
t p
er
year
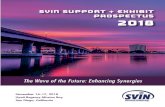
DANGEROUS
(> 1/1000)
REGULATED ULTRA-SAFE
(< 1/100K)
Bungee Jumping
Mountain
Climbing
Healthcare
Driving
Chartered Flights
Chemical Manufacturing
Scheduled Airlines
European
Railroads
Nuclear Power
Healthcare
(bron: L. Leape, 2/2001)

28/01/2014
Improving quality and safety of patient care is still an important issue:
– IOM-reports (1998, 2001): adverse events (AE)-rate in 3% to 4% of
patients hospitalized in the US
– Langelaan et al. (2008): 8% AEs; 2.9% preventable AEs; 5.5% preventable
deaths
– Levinson et al. (2010): 13.5 % AEs in hospitalized Medicare beneficiaries;
44% of AEs are preventable
Joint Commission (2007): poor communication among team members
was a contributing factor in almost 2/3 of AEs
“Patient care is a team sport. However healthcare is unique in that no other team sport has greater potential for catastrophic outcomes”. (Salas et al., 2008)
Why teamwork in healthcare?
MAKING TEAMS WORK

28/01/2014
Adverse Outcomes in Belgian Acute Hospitals
Wmean 32.3 12.4 14.0 13.8 12.7 6.7 8.2 6.2 P90/P10 4.5 3.6 2.4 3.6 5.7 3.0 5.4 1.7
95%CI [3.5;5.4] [2.9;4.2] [2.1;2.8] [2.9;4.2] [4.2;7.3] [2.4;3.5] [4.0;6.8] [1.5;1.8] CGain 15539 3194 3178 4226 5945 1991 3693 2320
Wmean 32.3 12.4 14.0 13.8 12.7 6.7 8.2 6.2 P90/P10 4.5 3.6 2.4 3.6 5.7 3.0 5.4 1.7
95%CI [3.5;5.4] [2.9;4.2] [2.1;2.8] [2.9;4.2] [4.2;7.3] [2.4;3.5] [4.0;6.8] [1.5;1.8] CGain 15539 3194 3178 4226 5945 1991 3693 2320
Wmean 17.6 12.2 13.5 13.2 5.2 5.3 3.6 3.4 14.7 9.0 7.9
P90/P10 5.1 4.0 3.3 3.0 6.5 2.4 7.9 3.5 4.0 4.7 3.5
95%CI [3.8;6.4] [3.1;4.9] [2.7;3.9] [2.4;3.5] [4.3;8.6] [2.0;2.8] [4.9;11.0] [2.7;4.2] [3.2;4.8] [3.5;5.8] [1.7;2.1]
CGain 5938 1943 5026 3016 1875 1336 1025 828 5983 3404 2786
Wmean 17.6 12.2 13.5 13.2 5.2 5.3 3.6 3.4 14.7 9.0 7.9
P90/P10 5.1 4.0 3.3 3.0 6.5 2.4 7.9 3.5 4.0 4.7 3.5
95%CI [3.8;6.4] [3.1;4.9] [2.7;3.9] [2.4;3.5] [4.3;8.6] [2.0;2.8] [4.9;11.0] [2.7;4.2] [3.2;4.8] [3.5;5.8] [1.7;2.1]
CGain 5938 1943 5026 3016 1875 1336 1025 828 5983 3404 2786
Each dot represents one of 123 Belgian acute hospitals. Risk adjustment was done via indirect standardization with APR-DRG and SOI and
Bayesian hierarchical modeling. Abbreviations: Wmean, weighted mean; 95% CI, 95% Credibility Intervals; CGain, centile gains; UTI,
urinary tract infection; PU, pressure ulcers; PNE, hospital, acquired pneumonia; SEP, hospital, acquired sepsis; CNS, central nervous
system complications; S/CA, shock or cardiac arrest; UGB, upper gastrointestinal bleeding; DVT, deep venous thrombosis; PF, pulmonary
failure; MD, metabolic derangement; WI, wound infection.
Medical patients:
Prevalence of 7.1%
Surgical patients :
Prevalence of 6.3%

28/01/2014
Cost of poor quality?
The Netherlands ‘Monitor Zorgerelateerde Schade
2011/2012’:
– Total cost for adverse events of €523 million per year and €126
million per year potentially preventable adverse events.
– 2,2% of yearly budget for hospital healthcare; 0,5% for potentially
preventable adverse events
Study on medical claims in USA:
– $17,1 billion in 2008
– 0,72% of total healthcare budget in USA
– Highest cost due to postoperative infections ($3,4 billion) and
pressure ulcers ($3,3 billion)
Langelaan M, Baines R, Broekens M, Siemerink K, van de Steeg L, Asscheman H et al. (2013). Monitor Zorggerelateerde Schade 2011/2012.
Dossieronderzoek in Nederlandse Ziekenhuizen. Amsterdam, NIVEL en EMGO+ Instituut.
Van Den Bos J., Rustagi K., Gray T., Halford M., Ziemkiewicz E., Shreve J. (2011) The $17.1 Billion Problem: The Annual Cost Of
Measurable Medical Errors. Health Affairs, 30, 4:596-603.

28/01/2014
Potential
Problem
Acc
iden
t
Problems with
legal procedures
Incomplete
Procedures Unclear roles
and tasks
Workload
Unclear
accountability
Inadequate
training
Divertion due to
other problems Inappropriate
maintenance Unstable
technology
Conflicts in Goals
System problems call for system solutions

28/01/2014
Why teamwork in healthcare?
WHO World Alliance for Patient Safety: lack of communication
and coordination as priority number one in patient safety
research for developed countries (Bates, D. 2009)

28/01/2014
Several barriers to effective teamwork in healthcare:
– Fragmented, disconnected organizational structures
– No incentives in financing system to collaborate
– Increasing job demands, high workload, different work schedules
– Low level of agreement and low level of predictability
– High specialization, high task interdependence, high functional
diversity
– Interprofessional boundaries, different educational backgrounds
– Power- and status differences, high competitive power
– Unclear leadership structures
– Temporary, ad hoc teams with low group identity, lack of role clarity
and poorly trained
Regular team conflicts: task /relation / process conflicts
Pseudo-teams in healthcare
Growing need for teamwork in healthcare

28/01/2014

28/01/2014
Nugus et al, 2010
Lack of informal
interaction
Power distributions

28/01/2014
Increasing job demands and high workload (RN4CAST-study KUL)
Within EU there will be shortage of one million healthcare workers
RN4CAST:
– Study on nurse staffing in which 61.168 nurses and 131.318 patients participated, in
more than 1.000 hospitals in 13 countries.
– Some Belgian results:
• Nurse staffing level: 11 patients for each nurse (US 5/1, the Netherlands 7/1)
• Number of nurses that are dissatisfied with their job: 22%
• Number of nurses that are intended to leave their job: 30%
• Number of nurses that report having a burnout: 24%
• Prevalence of nursing care left undone in Belgium: 58% comfort talks with
patients, 44% patient education and 43% update care plans
FOD Healthcare:
– 1198 medical doctors, 4635 nurses in 37 hospitals
– medical doctors (5,4% burnout; 17,8 risk of burnout), nurses (6,9% burnout; 12,4%
risk of burnout).
Aiken, L. H., Sermeus, W., Van den Heede, K., Sloane, D. M., Busse, R., McKee, M., … Kutney-Lee, A. (2012). Patient safety,
satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the
United States. British Medical Journal, 344, e1717.

28/01/2014
MAKING TEAMS WORK
OUTLINE
Growing need for teamwork in healthcare
How could care pathways improve teamwork?
Setting of the PhD-study
Objectives, research questions and included studies
Study results
General discussion and recommendations

28/01/2014
Team improvement interventions (Buljac-Samardzic et al. 2010)
(1) Teamwork training programs: these involve a
systematic process through which a team is trained to
master and improve team competencies (e.g. crew
resource management);
(2) Structured communication protocols: tools which seek
to improve the reliability of transferring critical information
(e.g. briefing and debriefing checklists)
(3) Organizational interventions: these are interventions
that seek to change work processes and structures so that
they support more effective communication.
MAKING TEAMS WORK

28/01/2014
Team training interventions: Crew Resource Management
‘Ferrari pit stops saves lives’ Prof. Martin Elliot

28/01/2014
Structured Communication Protocols: SBAR-Survey/Briefing
Adapted by Kaiser Permanente from a communication tool that
was adapted from the US Navy
An effective and efficient way to communicate important
information;
A simple way to help standardize communication
Allows parties to have common expectations related to what is to
be communicated and how the communication is structured.
S=Situation (a concise statement of the problem)
B=Background (pertinent and brief information related to the
situation)
A=Assessment (analysis and considerations of options —
what you found/think)
R=Recommendation (action requested/recommended — what
you want)

28/01/2014
What are care pathways?
A care pathway is a complex intervention for the mutual decision
making and organization of care processes for a well-defined
group of patients during a well-defined period.
Defining characteristics of care pathways include:
– An explicit statement of the goals and key elements of care based on
evidence, best practice, and patients’ expectations and their
characteristics;
– the facilitation of the communication among the team members and with
patients and families;
– the coordination of the care process by coordinating the roles and
sequencing the activities of the multidisciplinary care team, patients and
their relatives;
– the documentation, monitoring, and evaluation of variances and
outcomes
– the identification of the appropriate resources
Vanhaecht K, Sermeus W, van Zelm R, Panella M. Care pathways are defined as complex interventions. BMC Medicine 2010; 8:31.

28/01/2014
Care pathways as organisational interventions to improve teamwork
Deneckere S., Euwema, M, Van Herck P., Lodewijckx, C., Panella, M., Sermeus, W., and Vanhaecht, K. (2012). Care Pathways Lead to Better Teamwork: Results of a Systematic Review. Social Science & Medicine; 75(2):264-268.

28/01/2014
MAKING TEAMS WORK
OUTLINE
Growing need for teamwork in healthcare
How could care pathways improve teamwork?
Setting of the PhD-study
Objectives, research questions and included studies
Study results
General discussion and recommendations

28/01/2014
Setting: European Quality of Care Pathways (EQCP)-project
International multicentre research project launched by the European
Pathway Association (E-P-A) (http://www.E-P-A.org), supported with
unrestricted educational grant of Pfizer NV/SA
Objective: to study the effectiveness of CPs for COPD-exacerbation
and Proximal Femur Fracture (PFF)
Participating countries: Belgium, Ireland, Italy and Portugal
Three trials:
Trial 1: a cluster RCT on the impact of a CP for PFF on patient processes
and outcomes
Trial 2: a cluster RCT on the impact of a CP for COPD- exacerbation on
patient processes and outcomes
Trial 3: a cluster RCT on the impact of CPs on interprofessional teamwork
in which both COPD-exacerbation and PFF-clinical teams are included
MAKING TEAMS WORK

28/01/2014
Three research questions
RQ1: Which indicators can be used in order to study and
follow up interprofessional teamwork in care processes?
RQ2: What is the impact of care pathways on
interprofessional teamwork in an acute hospital setting?
RQ3: Which team and organizational conditions will
influence the successful implementation of care pathways
in an acute hospital setting?
MAKING TEAMS WORK

28/01/2014
Included studies
RQ1:
Team indicators
RQ2:
Impact of CPs on teamwork
RQ3:
CP conditions
Study 1 Study 2 Study 3 Study 4
Delphi-consensus
method to support
international expert panel
Systematic literature
review of articles on
CP-effectiveness on
teamwork
Stratified post-test-only
cluster randomized
controlled trial
Process evaluations of
the implementation
processes of the
developed CPs
• Each participant rated
an initial list of 44 team
indicators on a scale of 1
to 6.
• Consensus was sought
in two consecutive rounds
based on the content
validity index
• Literature search of
articles published
between 1999 and
2009
• Both effect and
exploratory studies
included
• Quality appraisal
• Intervention teams
developed CP
• Control teams
provided ‘usual care’
• Summative
evaluation of team
indicators
• Multi-level analysis
• Semi-structured, one-
to-one interviews with
key stakeholders of
each intervention team
• Normalization Process
Model used to guide the
inductive thematic
analysis
• Purposive sample of 36
experts: 19 scientific
researchers and 17
hospital managers
• 13 different countries
• 26 included studies
• Mixed settings and
patient groups
• 20 team indicators
used
• 30 teams caring for
COPD or PFF patients
• 17 intervention and
13 control teams
• 581 team members
• Purposive sample of
CP-facilitators,
management and team
members
• 75 representatives
DES
IGN
M
ETH
OD
S
SA
MPL
E

28/01/2014
RQ2 (study 3): Cluster RCT on impact of CPs on interprofessional teamwork:
methods

28/01/2014
Overall response rate was 78%: - 379 nurses - 94 allied health professionals - 75 medical doctors - 33 head nurses
Deneckere S, Euwema M, Lodewijckx C, Panella M, Mutsvari T, Sermeus W., and Vanhaecht, K. (2012). Better interprofessional teamwork, higher level of organized care and lower risk of burnout in acute healthcare teams using care pathways: A cluster randomized controlled trial. Medical Care 2012; In Press.
RQ2 (study 3): Cluster RCT on impact of CPs on interprofessional teamwork:
sample

28/01/2014
RQ2 (study 3): Cluster RCT on impact of CPs on interprofessional teamwork:
intervention

28/01/2014
Teams that developed a care pathway for COPD/PFF:
Perceived themselves more as being a real team (β=0.30 (0.91); 95% CI 0.11 to 0.49)
Better quality of work environment (β=0.40 (0.14); 95% CI 0.11 to 0.69)
Better management support (β=0.52 (0.11); 95% CI 0.29 to 0.74)
Better structured leadership (OR= 4.27; 95% CI 1.02 to 17.86)
More frequent team meetings (OR= 5.83; 95% CI 1.33 ; 25.68)
Better team composition (β=0.11(0.04); 95% CI 0.0.03 to 0.18]
No significant difference in team size
Better conflict management (β=0.30 (0.11); 95% CI 0.08 to 0.53)
Higher team climate for innovation (β=0.29 (0.10); 95% CI 0.09 to 0.49)
No significant differences in leadership qualities and relational coordination
Higher level of organization of care (β=5.56 (2.05); 95% CI 1.35; 9.76)
Lower emotional exhaustion (β= -0.57 (0.21); 95% CI -1.00 to -0.14)
Higher level of competence (β=0.147; 95% CI 0.147 to 0.640).
RQ2 (study 3): Cluster RCT: results of multilevel analysis
TEAM INPUTS
TEAM OUTPUTS
TEAM PROCESSES

28/01/2014
RQ2 (study 3): Cluster RCT: results of multilevel analysis
Intervention Group Control Group
N of team members with
risk of burnout
7,3% 12,5%
N of team members with
burnout
3,8% 6%
Deneckere S, Euwema M, Lodewijckx C, Panella M, Mutsvari T, Sermeus W., and Vanhaecht, K. (2012). Better
interprofessional teamwork, higher level of organized care and lower risk of burnout in acute healthcare teams
using care pathways: A cluster randomized controlled trial. Medical Care; 51(1):99 107.

28/01/2014
Job Demand Control model van Karasek
“Wie tegen problemen oploopt in zijn werk (dus regelbehoefte heeft),
moet die zelf kunnen oplossen (regelcapaciteit)”

28/01/2014
Principles of Innovative Work Organisation
MAKING TEAMS WORK

28/01/2014
Organizational model of a care pathway as a multiteam system aligning professionals and teams
within linked clinical microsystems (CM) with individual, team and system goals
Deneckere, S., Sermeus, W. (sup.), Vanhaecht, K. (cosup.), Euwema, M. (cosup.) (2012). MAKING TEAMS WORK. The impact of care pathways on interprofessional teamwork in an acute hospital setting: A cluster randomized controlled trial and evaluation of implementation processes.

28/01/2014
MAKING TEAMS WORK
OUTLINE
Growing need for teamwork in healthcare
How could care pathways improve teamwork?
Setting of the PhD-study
Objectives, research questions and included studies
Study results
General discussion and recommendations

28/01/2014
Implications for health services
CPs are an effective intervention for improving interprofessional
teamwork and conflict management, increasing the organizational level
of care processes, and decreasing risk of burnout for healthcare teams
in an acute hospital setting
CPs have the potential to tackle several barriers against effective
teamwork:
– Disconnected organizational structure: CPs build a structured care plan that will
improve information transfer between multiple teams and support the
interprofessional decision making process
– Professional boundaries: CPs can build an essential group identity, shared mental
model and a safe culture for innovation
– Unwarranted variation, high task uncertainty: organizing care and defining clear
team goals
– Increasing job demands: CPs seem to be able to create essential job resources
that can buffer the impact of these increasing job demands in the current healthcare
environment

28/01/2014
Some policy advice
Decentralization of decision processes
Deregularization on professional boundaries
Training in team competencies in education and
collaborative learning platforms
Financing system with incentives for collaboration: pay for
quality, bundled payment
Towards integrated care systems and service-line driven
organizational structures
Support care innovation and care process organization
Transparency of quality which leads to collective ambition
for change
MAKING TEAMS WORK

28/01/2014 MAKING TEAMS WORK The impact of care pathways on interprofessional teamwork in an acute hospital setting: A cluster randomized controlled trial and evaluation of implementation processes.
________________
dr. Svin Deneckere
Doctoral thesis in Biomedical Sciences Department of Public Health, KU Leuven
Leuven, 2012
“Talent wins games, but teamwork and intelligence wins
championships.”
(Michael Jordan)