
Preparing for Precipitous Vaginal Deliveries in the Emergency Department
4
PREPARING FOR PRECIPITOUS V AGINAL DELIVERIES IN THE EMERGENCY DEPARTMENT Author: Linda Robinson, RN, BSN, CEN, CFN, SANE, Covington, KY Section Editor: Faye P. Everson, RN, CEN O ne small Midwestern inner-city hospital has served its community since 1866. With the building of a suburban facility in this system, most of the inpa- tient services have moved to that location, including obstet- rics and pediatrics. Even though the facility is only 7 miles away, or 15 minutes away, the local community still relies heavily on the small inner-city facility for most of its health care needs. Much of this population is indigent, with ap- proximately 80% of the consumers receiving some type of federal funding or are paying out of pocket. Unfortunately, many of these patients and their families are of the mindset that any hospital can deliver a baby. This inner-city emergency department is a 14-bed unit and is adequately staffed by nurses, clerical coordinators, certified nursing assistants, and physicians. It is not the pre- ferred location, however, for a vaginal delivery for a variety of reasons, including the lack of an obstetric service and nursery. However, as a result of a seemingly special bond of trust between the community’s citizens and this hospital, patients still come to the site when they go into labor. This occurs despite our attempts to educate our community resi- dents and pregnant women, as well as directions from the obstetricians to their patients, to go to the suburban site for their deliveries. But they still come! Recently, there were 3 precipitous vaginal deliveries in this emergency department within a 2-month period. Each time this happens, even seasoned emergency nurses may feel tremendous anxiety and feel inadequately prepared, disorganized, uncomfortable with the equipment, and wor- ried that their documentation might not be adequate. Even my 11 years of experience in the emergency department rendered me a bit uneasy about this. So I decided to re- search the topic and develop a much-needed education program for the ED staff. This led me to our hospital medi- cal library, the Internet, the Maternal-Child Health Educa- tor at our suburban hospital, and our local EMS Paramedic Director. These combined resources played a vital role in the creation and implementation of this program. Problems Identified I identified 3 main problem areas related to imminent de- liveries in the emergency department: 1. Accessible equipment 2. Training in emergency deliveries 3. Specialized documentation First to be addressed was our equipment. The baby warmer and other delivery supplies were not located in a central location nor were they optimally organized. I met with the Maternal-Child Health Educator and dis- cussed the issues concerning the equipment. A decision was made to assemble precipitous birth packs. These packs contain items essential only for the vaginal delivery and ini- tial care of the newborn and mother. They also contain the wrist bracelets with matching numbers for mother and in- fant. Before the creation of these packs, the unit did not have the matching bracelets. The packs are bagged with an inventory list attached to the top. They are kept on the baby warmer along with the episiotomy tray. Every time a birth pack is used, 2 RNs are assigned to replace it. The unit now has multiple packs completed (Appendix A). The baby warmer was relocated to a more accessible location with its supplies inventoried, updated, and reorganized. Training needed to be addressed at several levels. Edu- cational updates needed to include the changes in equip- ment and in our documentation, as well as on the clinical care of a patient before, during, and after a vaginal delivery. The in-service program given to the ED staff began with a pretest to assess existing knowledge about vaginal deliveries. After the test, I reviewed the sections in the newly created “Precipitous Vaginal Deliveries” binder. First, we reviewed the section on equipment. It was explained that the precip- itous packs contained supplies used during an emergent vaginal delivery. We reviewed the use of each item in the pack and its location in the department. The entire in-service was very “hands on.” It is important for the nurses to feel Linda Robinson, Member, Chapter 261, is Team Leader, Emergency Depart- ment, St. Elizabeth Medical Center, Covington, KY. For correspondence, write: Linda Robinson, RN, BSN, CEN, CFN, SANE, Emergency Department, St Elizabeth Medical Center, 401 E 20th St, Covington, KY 41014; E-mail: [email protected]. J Emerg Nurs 2009;35:256-9. 0099-1767/$36.00 © 2009 Emergency Nurses Association. Published by Elsevier. All rights reserved. doi: 10.1016/j.jen.2009.02.007 NURSE EDUCATOR 256 JOURNAL OF EMERGENCY NURSING 35:3 May 2009
-
Upload
linda-robinson -
Category
Documents
-
view
214 -
download
1
Transcript of Preparing for Precipitous Vaginal Deliveries in the Emergency Department

PREPARING FOR PRECIPITOUS VAGINAL DELIVERIES
IN THE EMERGENCY DEPARTMENT
Author: Linda Robinson, RN, BSN, CEN, CFN, SANE, Covington, KYSection Editor: Faye P. Everson, RN, CEN
One small Midwestern inner-city hospital has servedits community since 1866. With the building of asuburban facility in this system, most of the inpa-
tient services have moved to that location, including obstet-rics and pediatrics. Even though the facility is only 7 milesaway, or 15 minutes away, the local community still reliesheavily on the small inner-city facility for most of its healthcare needs. Much of this population is indigent, with ap-proximately 80% of the consumers receiving some type offederal funding or are paying out of pocket. Unfortunately,many of these patients and their families are of the mindsetthat any hospital can deliver a baby.
This inner-city emergency department is a 14-bed unitand is adequately staffed by nurses, clerical coordinators,certified nursing assistants, and physicians. It is not the pre-ferred location, however, for a vaginal delivery for a varietyof reasons, including the lack of an obstetric service andnursery. However, as a result of a seemingly special bondof trust between the community’s citizens and this hospital,patients still come to the site when they go into labor. Thisoccurs despite our attempts to educate our community resi-dents and pregnant women, as well as directions from theobstetricians to their patients, to go to the suburban site fortheir deliveries. But they still come!
Recently, there were 3 precipitous vaginal deliveries inthis emergency department within a 2-month period. Eachtime this happens, even seasoned emergency nurses mayfeel tremendous anxiety and feel inadequately prepared,disorganized, uncomfortable with the equipment, and wor-ried that their documentation might not be adequate. Evenmy 11 years of experience in the emergency departmentrendered me a bit uneasy about this. So I decided to re-search the topic and develop a much-needed education
program for the ED staff. This led me to our hospital medi-cal library, the Internet, the Maternal-Child Health Educa-tor at our suburban hospital, and our local EMS ParamedicDirector. These combined resources played a vital role inthe creation and implementation of this program.
Problems Identified
I identified 3 main problem areas related to imminent de-liveries in the emergency department:
1. Accessible equipment2. Training in emergency deliveries3. Specialized documentation
First to be addressed was our equipment. The babywarmer and other delivery supplies were not located ina central location nor were they optimally organized. Imet with the Maternal-Child Health Educator and dis-cussed the issues concerning the equipment. A decisionwas made to assemble precipitous birth packs. These packscontain items essential only for the vaginal delivery and ini-tial care of the newborn and mother. They also contain thewrist bracelets with matching numbers for mother and in-fant. Before the creation of these packs, the unit did nothave the matching bracelets. The packs are bagged withan inventory list attached to the top. They are kept on thebaby warmer along with the episiotomy tray. Every time abirth pack is used, 2 RNs are assigned to replace it. The unitnow has multiple packs completed (Appendix A). The babywarmer was relocated to a more accessible location with itssupplies inventoried, updated, and reorganized.
Training needed to be addressed at several levels. Edu-cational updates needed to include the changes in equip-ment and in our documentation, as well as on the clinicalcare of a patient before, during, and after a vaginal delivery.The in-service program given to the ED staff began with apretest to assess existing knowledge about vaginal deliveries.After the test, I reviewed the sections in the newly created“Precipitous Vaginal Deliveries” binder. First, we reviewedthe section on equipment. It was explained that the precip-itous packs contained supplies used during an emergentvaginal delivery. We reviewed the use of each item in thepack and its location in the department. The entire in-servicewas very “hands on.” It is important for the nurses to feel
Linda Robinson, Member, Chapter 261, is Team Leader, Emergency Depart-ment, St. Elizabeth Medical Center, Covington, KY.
For correspondence, write: Linda Robinson, RN, BSN, CEN, CFN, SANE,Emergency Department, St Elizabeth Medical Center, 401 E 20th St,Covington, KY 41014; E-mail: [email protected].
J Emerg Nurs 2009;35:256-9.
0099-1767/$36.00
© 2009 EmergencyNurses Association. Published by Elsevier. All rights reserved.
doi: 10.1016/j.jen.2009.02.007
N U R S E E D U C A T O R
256 JOURNAL OF EMERGENCY NURSING 35:3 May 2009

comfortable with the equipment. A self-inflating breathingsystem bag (commonly known as a Mapleson) was a pieceof equipment that only a few of the nurses had used, so it wasimportant for everyone to become familiar with it.
Next, we reviewed the baby warmer and its con-tents and supplies. We then discussed the appropriate useof the newly created “Pyxis Baby Kits” that contain eryth-romycin eye ointment and the neonate vitamin K injec-tion that are now stored in our medication-dispensingmachine (Pyxis, Cardinal Health, Dublin, OH).
The childbirth section was reviewed, which coverednursing physical assessment, indications of an imminentdelivery, signs of hemorrhagic shock, and the importanceof obtaining a pertinent medical history. I facilitated dis-cussions of experiences and even “war stories” about pastED deliveries. I was then able to build upon and use theseas examples in teaching while still being able to acknowl-edge the experience level of the nursing staff.
The next section, normal vaginal delivery, covered areview of predelivery, delivery, potential complications, as-sessment and care of the infant, delivery of the placenta,assessment and care of the mother, patient identificationmeasures, and finally, disposition. Common complicationsdiscussed were prolapsed cord, amniotic sac covering theneonate’s face, and breech births.
The in-services were a big success with the help of avaginal delivery mannequin provided by our local EMS sys-tem. The mannequin simulated a vaginal delivery includingthe placenta and umbilical cord. The nurses were able tovisualize the neonate coming through the birth canal, usethe cord clamps to clamp the cord, and then deliver theplacenta. This stimulated much conversation regardingbirth presentations, additional complications, and personalexperiences. Collaborating with the EMS with the use ofthe mannequin also helped to improve relationships withEMS personnel. To organize this teaching informationand make it accessible to the staff to use as a reference,we made 2 identical notebooks that contained all the in-formation reviewed in the in-service including the laborand delivery record. The binders were clearly labeled “Pre-cipitous Vaginal Deliveries.” One binder was placed in thenursing station and the other one on the baby warmer.The staff was encouraged not to be afraid to reference thisbinder when a patient presented in the emergency depart-ment (… if all else fails, read the directions!).
The new labor and delivery record was reviewed beforethe post test. The need for specialized documentation onthe labor and delivery record was addressed. Most of ournurses wanted to know what was essential to documentversus what was nice to document. I met again with theMaternal-Child Health Educator and reviewed the inpa-
tient labor and delivery documentation. We used their re-cord as a prototype and, with revisions, turned their recordinto a usable ED document. We did this by deleting infor-mation that was not needed in an emergent situation andadding what was essential (Appendix B). The essential ad-ditions to the record included disposition identifiers andidentification bracelet numbers of the mother and new-born. These also included additional signatures of thoseinvolved with the delivery, Apgar scoring, and dispositionof the mother and newborn.
The disposition documentation is vital in the emer-gency department along with the bracelet placement andrecorded numbers. Because the Special Care Nursery atour sister hospital is a level 2 facility, the mother and thenewborn could possibly be transferred to 2 different facili-ties. Having this information documented on the newborn’sand mother’s chart along with the bracelet placement linksthem together, eliminating confusion and increasing pa-tient safety. The original labor and delivery record is placedon the mother’s ED chart, and a copy is placed on the new-born’s chart. The newborn also requires his or her own EDchart upon birth.
Because emergency nurses are not often involved withdeliveries, the new documentation enables them to give aconcise, pertinent report of the labor and delivery processto avoid omitting vital information. This allows the receiv-ing institution to prepare appropriately for the patient orpatients. The nurses were very receptive to the new record,stating that they often worried whether their documenta-tion was adequate. They believed that the new record wasa usable tool that would be a very effective focus during abusy delivery.
The pre–in-service test scores averaged 55%, and thepost–in-service test scores were 100%. Thirty-one RNscompleted the in-service and tests. There were no negativecomments on the course evaluations, and some of thepositive comments included the following: “we should dothis every year,” “a great review,” “very impressive,” “I lovedit,” and “I feel more prepared.”
We also made sure these classes included a lot oflaughter, information sharing, and a comfortable stress-free, hands-on learning environment. There was someinformal conversation between the staff so that these classeswere non-threatening and helpful. The entire in-servicelasted approximately 30 to 40 minutes.
In conclusion, our emergency department is now muchbetter prepared for precipitous vaginal deliveries. We willcontinue to revise our program as needed to best meet ourpatients’ and staff ’s needs. Although we do not want to pro-mote emergency deliveries in the emergency department,we certainly feel much more prepared to handle them now.
NURSE EDUCATOR/Robinson
May 2009 35:3 JOURNAL OF EMERGENCY NURSING 257
Acknowledgment
Special thanks to Gail Latham, former Maternal-Child Health Educator
at St Elizabeth Medical Center, Edgewood, KY; Karl Chalk, EMT/P,
EMS Director, City of Covington Fire Department, Covington, KY; and
Terry Foster, RN, MSN, CEN, CCRN, CCNS, Clinical Nurse Specialist,
St Elizabeth Medical Center, Edgewood, KY.
SUGGESTED READINGLimmer D, O’Keefe MF, Grant HD, Murray RH, Bergeron JD.Emergency care. 9th ed. Upper Saddle River (NJ): Prentice Hall; 2001.
Neonates in the emergency department. Primary midwife archives.2004. Available at: http://www.gentlebirth.org. Accessed Febru-ary 4, 2004.
PULSE emergency medical update video; obstetric emergencies; 1997.Available at: http://www.criticalinfonet.com.
Ralston M, Hazinski M, Zaritsky A, Schexnayder S, Kleinman M.Pediatric advanced life support; 2005.
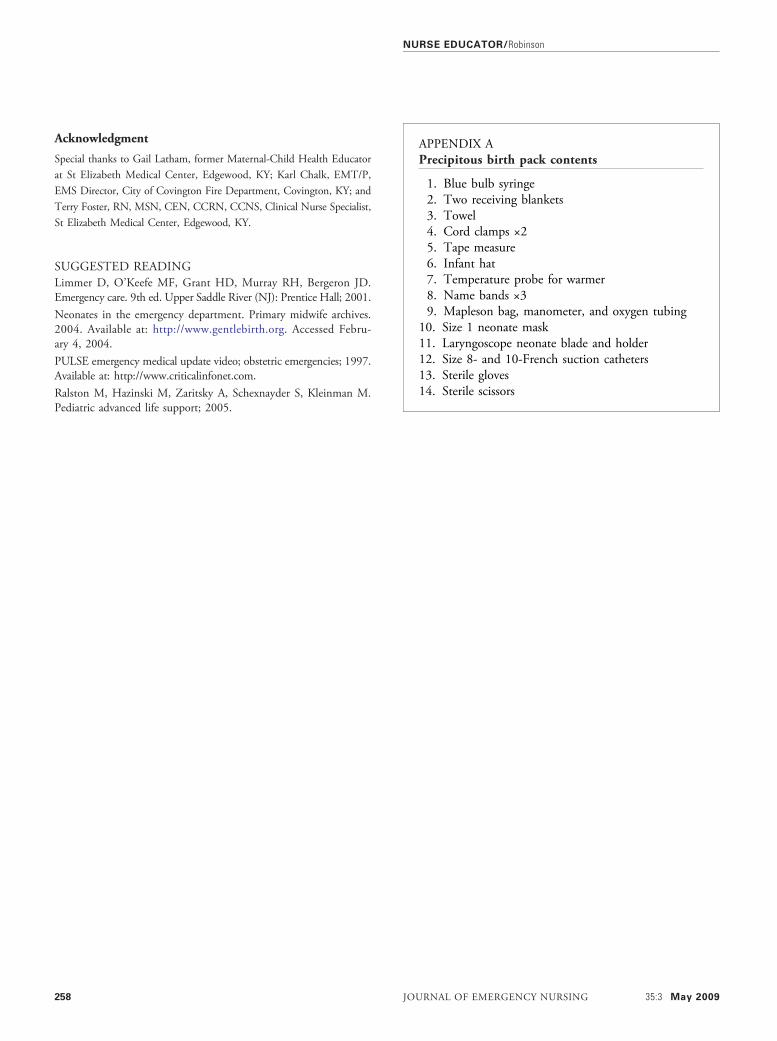
APPENDIX APrecipitous birth pack contents
1. Blue bulb syringe2. Two receiving blankets3. Towel4. Cord clamps ×25. Tape measure6. Infant hat7. Temperature probe for warmer8. Name bands ×39. Mapleson bag, manometer, and oxygen tubing
10. Size 1 neonate mask11. Laryngoscope neonate blade and holder12. Size 8- and 10-French suction catheters13. Sterile gloves14. Sterile scissors
NURSE EDUCATOR/Robinson
258 JOURNAL OF EMERGENCY NURSING 35:3 May 2009

APPENDIX BLabor and delivery summary record
Patient _____________________Date _______________________Time _______________________
LABOR AND DELIVERY SUMMARY RECORD
LABOR BP_____P_____RR_____TEMP_____ G_____ P_____ABS_____AB_____EDC____/____/____ FHT’S ______PMH____________________ ALLERGIES ________________
DELIVERY PRESENTATION: Cephalic ______________Breech _______________
METHOD OF DELIVERY: Vaginal with Forceps ______________Vaginal without Forceps ___________
PLACENTA: Contained and sent with Mother _________________
LABOR SUMMARY DATE TIMEMEMBRANES RUPTURED _____/_____/_____ __________ONSET OF LABOR _____/_____/_____ __________COMPLETION OF DILITATION _____/_____/_____ __________DELIVERY OF INFANT _____/_____/_____ __________DELIVERY OF PLACENTA _____/_____/_____ __________
DELIVERED BY ____________________________ RN _______________________________
INFANT
APGAR 0 1 2 1 min 5 min 10 min
COLOR Blue / pale Body pink ext. blue All pink
RESP EFFORT Absent Slow weak gasping Good strong cry
MUSCLE TONE Limp Flexion Active motion
HEART RATE Absent <100 > 100
REFLEX IRRITABILITY none Grimace cry
TOTALS:
ASSIGNED BY:_______________________WEIGHT ___________
RX: EYE OINTMENT ____________________ VITAMIN K _____________________
MOTHER DISPOSITION TO: ________________ MOTHER TRANSFER TIME: ______________
BABY DISPOSITION TO: _____________________ BABY TRANSFER TIME: _________________
INFANT ID BRACELET # _____________________MOTHER ID BRACELET # ____________________R.N.__________________________________
Copies 1- mother chart 1 – baby chart 1- ED chart
Form modified from SEMC inpatient Labor and Delivery Record
AB, abortion; ABS, abortion spontaneous; BP, blood pressure; EDC, estimated date of conception; FHT'S, fetal heart tones; G, gravida; P, para; P, pulse; PMH, previous medicalhistory; RR, respiratory rate; SEMC, St. Elizabeth Medical Center; TEMP, temperature.
NURSE EDUCATOR/Robinson
May 2009 35:3 JOURNAL OF EMERGENCY NURSING 259


















