Prenatal Tetanus, Diphtheria, Acellular Pertussis...
11
ARTICLE Prenatal Tetanus, Diphtheria, Acellular Pertussis Vaccination and Autism Spectrum Disorder Tracy A. Becerra-Culqui, PhD, MPH, OT/L, Darios Getahun, MD, PhD, MPH, Vicki Chiu, MS, Lina S. Sy, MPH, Hung Fu Tseng, PhD, MPH BACKGROUND: Increasing vaccination of pregnant women makes it important to assess safety events potentially linked to prenatal vaccination. This study investigates the association between prenatal tetanus, diphtheria, acellular pertussis (Tdap) vaccination and autism spectrum disorder (ASD) risk in offspring. METHODS: This is a retrospective cohort study of mother-child pairs with deliveries January 1, 2011 to December 31, 2014 at Kaiser Permanente Southern California hospitals. Maternal Tdap vaccination from pregnancy start to delivery date was obtained from electronic medical records. A diagnosis of ASD was obtained by using International Classification of Diseases, Ninth and Tenth Revision codes. Children were managed from birth to first ASD diagnosis, end of membership, or end of follow-up (June 30, 2017). Cox proportional hazards models estimated the unadjusted and adjusted hazard ratios (HRs) for the association between maternal Tdap vaccination and ASD, with inverse probability of treatment weighting to adjust for confounding. RESULTS: Women vaccinated were more likely to be Asian American or Pacific Islander, be nulliparous, have a higher education, receive influenza vaccination prenatally, and give birth at term. ASD was diagnosed in 1341 (1.6%) children, and the incidence rate was 3.78 per 1000 person years in the Tdap exposed and 4.05 per 1000 person years in the unexposed group (HR: 0.98, 95% confidence interval: 0.88–1.09). The inverse probability of treatment weighting–adjusted analyses revealed that prenatal Tdap vaccination was not associated with an increased ASD risk (HR: 0.85, 95% confidence interval: 0.77– 0.95). CONCLUSIONS: Prenatal Tdap vaccination was not associated with an increased ASD risk. We support recommendations to vaccinate pregnant women to protect infants, who are at highest risk of death after pertussis infection. abstract Department of Research and Evaluation, Kaiser Permanente Southern California, Pasadena, California Dr Becerra-Culqui conceptualized and designed the study, developed the analysis plan, coordinated the interpretation of the results, contributed expertise in epidemiologic methods and autism outcomes, and drafted and finalized the manuscript; Drs Tseng and Getahun contributed to the analysis plan and interpretation of results, critically reviewed the manuscript for important intellectual content within areas of expertise (such as epidemiologic methods, bias, vaccines, autism, and broad messaging of the manuscript), and revised; Ms Chiu provided statistical analysis consultation, feedback to the analysis plan, conducted the analyses, critically reviewed the manuscript for important statistical intellectual content, and revised; Ms Sy critically reviewed the manuscript for important intellectual content within vaccine area of expertise and broad messaging of the manuscript and revised; and all authors approved the final version of the manuscript as submitted and agree to be accountable for all aspects of the work. DOI: https://doi.org/10.1542/peds.2018-0120 PEDIATRICS Volume 142, number 3, September 2018:e20180120 WHAT’S KNOWN ON THIS SUBJECT: Few researchers have examined effects of prenatal tetanus, diphtheria, and acellular pertussis (Tdap) vaccination on maternal and child outcomes. No increased risk of preterm delivery or low birth weight has been found in infants born to women vaccinated prenatally. WHAT THIS STUDY ADDS: Prenatal Tdap vaccination was not associated with an increased risk of autism spectrum disorder (ASD) in children. No study to our knowledge has been published examining the risk of ASD after prenatal exposure to the Tdap vaccine. To cite: Becerra-Culqui TA, Getahun D, Chiu V, et al. Prenatal Tetanus, Diphtheria, Acellular Pertussis Vaccination and Autism Spectrum Disorder. Pediatrics. 2018;142(3): e20180120 by guest on March 5, 2019 www.aappublications.org/news Downloaded from
Transcript of Prenatal Tetanus, Diphtheria, Acellular Pertussis...

ARTICLE
Prenatal Tetanus, Diphtheria, Acellular Pertussis Vaccination and Autism Spectrum DisorderTracy A. Becerra-Culqui, PhD, MPH, OT/L, Darios Getahun, MD, PhD, MPH, Vicki Chiu, MS, Lina S. Sy, MPH, Hung Fu Tseng, PhD, MPH
BACKGROUND: Increasing vaccination of pregnant women makes it important to assess safety events potentially linked to prenatal vaccination. This study investigates the association between prenatal tetanus, diphtheria, acellular pertussis (Tdap) vaccination and autism spectrum disorder (ASD) risk in offspring.METHODS: This is a retrospective cohort study of mother-child pairs with deliveries January 1, 2011 to December 31, 2014 at Kaiser Permanente Southern California hospitals. Maternal Tdap vaccination from pregnancy start to delivery date was obtained from electronic medical records. A diagnosis of ASD was obtained by using International Classification of Diseases, Ninth and Tenth Revision codes. Children were managed from birth to first ASD diagnosis, end of membership, or end of follow-up (June 30, 2017). Cox proportional hazards models estimated the unadjusted and adjusted hazard ratios (HRs) for the association between maternal Tdap vaccination and ASD, with inverse probability of treatment weighting to adjust for confounding.RESULTS: Women vaccinated were more likely to be Asian American or Pacific Islander, be nulliparous, have a higher education, receive influenza vaccination prenatally, and give birth at term. ASD was diagnosed in 1341 (1.6%) children, and the incidence rate was 3.78 per 1000 person years in the Tdap exposed and 4.05 per 1000 person years in the unexposed group (HR: 0.98, 95% confidence interval: 0.88–1.09). The inverse probability of treatment weighting–adjusted analyses revealed that prenatal Tdap vaccination was not associated with an increased ASD risk (HR: 0.85, 95% confidence interval: 0.77–0.95).CONCLUSIONS: Prenatal Tdap vaccination was not associated with an increased ASD risk. We support recommendations to vaccinate pregnant women to protect infants, who are at highest risk of death after pertussis infection.
abstract
Department of Research and Evaluation, Kaiser Permanente Southern California, Pasadena, California
Dr Becerra-Culqui conceptualized and designed the study, developed the analysis plan, coordinated the interpretation of the results, contributed expertise in epidemiologic methods and autism outcomes, and drafted and finalized the manuscript; Drs Tseng and Getahun contributed to the analysis plan and interpretation of results, critically reviewed the manuscript for important intellectual content within areas of expertise (such as epidemiologic methods, bias, vaccines, autism, and broad messaging of the manuscript), and revised; Ms Chiu provided statistical analysis consultation, feedback to the analysis plan, conducted the analyses, critically reviewed the manuscript for important statistical intellectual content, and revised; Ms Sy critically reviewed the manuscript for important intellectual content within vaccine area of expertise and broad messaging of the manuscript and revised; and all authors approved the final version of the manuscript as submitted and agree to be accountable for all aspects of the work.
DOI: https:// doi. org/ 10. 1542/ peds. 2018- 0120
PEDIATRICS Volume 142, number 3, September 2018:e20180120
WHAT’S KNOWN ON THIS SUBJECT: Few researchers have examined effects of prenatal tetanus, diphtheria, and acellular pertussis (Tdap) vaccination on maternal and child outcomes. No increased risk of preterm delivery or low birth weight has been found in infants born to women vaccinated prenatally.
WHAT THIS STUDY ADDS: Prenatal Tdap vaccination was not associated with an increased risk of autism spectrum disorder (ASD) in children. No study to our knowledge has been published examining the risk of ASD after prenatal exposure to the Tdap vaccine.
To cite: Becerra-Culqui TA, Getahun D, Chiu V, et al. Prenatal Tetanus, Diphtheria, Acellular Pertussis Vaccination and Autism Spectrum Disorder. Pediatrics. 2018;142(3): e20180120
by guest on March 5, 2019www.aappublications.org/newsDownloaded from

Prenatal tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis, adsorbed (Tdap) vaccination has been shown to be effective in protecting vulnerable young infants from pertussis. Prompted by waning immunity, pertussis incidence has risen in the past decade in the United States, with peaks in 2010 and 2014.1, 2 Young infants are at the highest risk of hospitalization and death after pertussis infection, a highly contagious respiratory disease (whooping cough) caused by the bacterium Bordetella pertussis.3 In response, in October 2011 the Advisory Committee on Immunization Practices (ACIP) recommended that unvaccinated pregnant women receive the Tdap vaccine after 20 weeks’ gestation.4 Given the seriousness of the matter, this recommendation was amended in October 2012 to include all pregnant women regardless of previous vaccinations, and the optimal vaccination period was defined between 27 and 36 weeks’ gestation.5 Evidence revealed that antibodies are passed along to newborns, and the vaccine was 91.4% effective in providing some immunity until newborns reach 2 months of age, the age they are expected to receive their first dose of the diphtheria-tetanus-acellular pertussis vaccine.6, 7 Given the increasing practice to vaccinate pregnant women with Tdap, it is important to address the concern of a potential link between maternal vaccination and subsequent development of autism spectrum disorder (ASD) in children.
During a time when Tdap was not routinely recommended for pregnant women, spontaneous abortions were the most frequent pregnancy-specific adverse events (16.7%) reported in the Vaccine Adverse Event Reporting System, a national database used for monitoring the safety of vaccines in the population.8 However, the number
of pregnant women who received the vaccine was small (n = 132) and likely a selective group because the vaccine was not in routine use. Since the ACIP recommendations, researchers have examined the effects of the Tdap vaccine on maternal and child outcomes finding no associations between the vaccine and adverse events.9 – 11 A study based on data from 7 Vaccine Safety Datalink sites found that there was no increased risk of small for gestational age, preterm delivery, or low birth weight in infants born to women who received the vaccine while pregnant between 2007 and 2013.9
Researchers examining maternal and child outcomes after prenatal Tdap vaccination have not evaluated longer-term outcomes such as the risk of ASD, an outcome of significant public interest. ASD is a neurodevelopmental disorder typically diagnosed in early childhood and characterized by impairments in social-communication skills and restricted stereotyped behaviors.12 In the United States, ∼147 per 10 000 children are diagnosed with ASD by 8 years of age.13, 14 Although there is no consensus on timing of exposure, the prenatal period is strongly implicated in ASD etiology, 15 – 18 and both genetic and environmental causes are important.19 –21 Although there is consistent evidence supporting that vaccines administered in childhood and their preservatives do not cause ASD, 22 – 24 there is limited research on the safety of vaccines administered during pregnancy. In this study, we aimed to evaluate the association between the Tdap vaccine administered during pregnancy and ASD risk in a cohort of children born at Kaiser Permanente Southern California (KPSC) hospitals.
METHODS
Study Population and Design
In this retrospective cohort study, we observed the outcome of an
ASD diagnosis in children born at all KPSC hospitals between January 1, 2011, and December 31, 2014. KPSC is an integrated health care delivery organization that provides health care in 15 hospitals and ∼220 medical offices to ∼4.4 million members who are broadly representative of the Southern California population.25 KPSC uses electronic medical records (EMRs) to integrate medical information, such as diagnosis and immunizations. All recommended immunizations are free to members regardless of copayment status. This study was approved by the KPSC Institutional Review Board, which waived the requirement for informed consent.
Eligibility was restricted to pregnant women who did not have assisted conceptions (in vitro fertilization) and gave birth to live singleton infants at 22 to 45 weeks’ gestation. Childrens' medical records were linked longitudinally to biological mothers by using unique identifiers. Maternal and child pairs were included if pregnant women had continuous membership since the beginning of pregnancy (allowing for a ≤31-day gap) and infants were members for at least 90 continuous days after turning 1 year of age. Pairs were excluded if children were diagnosed with chromosomal or congenital anomalies.
Maternal Tdap Vaccination
Maternal vaccination captured in the EMR was defined as receipt of Tdap anytime during pregnancy (yes, no), from the pregnancy start date to the day before the delivery date. The pregnancy start date was calculated by subtracting the gestational age at birth from the child’s birth date. Adacel (Sanofi Pasteur, Swiftwater, PA) was the primary Tdap product used at KPSC facilities during the study period.26 The unvaccinated group was defined by women who were not vaccinated with
BECERRA-CULQUI et al2 by guest on March 5, 2019www.aappublications.org/newsDownloaded from

Tdap anytime during their entire pregnancy.
ASDs
ASD was defined by a clinical diagnosis any time after turning 1 year of age recorded in the EMR between January 1, 2012, and June 30, 2017 (International Classification of Diseases, Ninth Revision codes: 299.0, 299.8, 299.9; and International Classification of Diseases, 10th Revision codes: F84.0, F84.5, F84.8, F84.9). Although we consider children at risk for ASD from birth, we restricted the minimum diagnosis age on the basis of the 12-month minimum allowable evaluation age of the Autism Diagnostic Observation Schedule, the gold standard diagnostic instrument for identifying ASD.27
Covariates
Maternal and child characteristics were obtained from the EMR. Child data included sex (male or female), birth year (2011–2014), birth season (winter, spring, summer, fall), gestational age at birth (mean, SD; <37 or ≥37 weeks’ gestation), and birth weight (mean, SD). Maternal data at delivery included maternal age (≤25, 26–30, 31–34, ≥35 years), race and/or ethnicity (non-Hispanic white, non-Hispanic African American, Hispanic, non-Hispanic Asian American or Pacific Islander, other or multiracial, unknown), primary language (English, other), interpreter needed (yes, no), educational attainment (less than or equal to high school, some college, bachelor’s degree, greater than or equal to master’s degree, unknown), and medical center of delivery. Additional pregnancy information included Medicaid insurance (yes, no), parity (0, 1, ≥2), receipt of influenza vaccine during pregnancy (yes, no), start of prenatal care (≤3 months gestation, >3 months gestation, no care or missing), and medical and obstetrical
complications (pregestational hypertension, preeclampsia or eclampsia, pregestational and gestational diabetes, placenta previa, and placental abruption).
Statistical Analysis
The distributions of maternal and child characteristics by prenatal Tdap vaccination status and either χ2 test or Student’s t test for differences in characteristics were calculated. Follow-up characteristics, age of ASD diagnosis, and the incidence rate of ASD diagnosis by Tdap vaccination status were calculated. Children were followed from birth to first ASD diagnosis, end of membership in the health plan, or the end of the study follow-up period (June 30, 2017), whichever came first.
To assess the potential concern that ASD diagnoses were missed because of dual enrollment in another health care system and/or limited health care use within the KPSC system, we also calculated the proportion of children with no outpatient encounters after turning 1 year of age. Proportions were calculated by whether their mothers received the Tdap vaccine during pregnancy.
Cox proportional hazards regression was used to estimate the unadjusted and adjusted hazard ratios (HRs) and their 95% confidence intervals (CIs) to evaluate the magnitude of association between maternal Tdap vaccination and ASD diagnosis in children. To evaluate potential variations in results, we also conducted stratified analyses by child’s birth year and by assessing results among women giving birth to their first child (nulliparous). We used propensity score analyses with inverse probability of treatment weighting (IPTW) to adjust for potential confounding. First, we used a logistic regression model including variables associated with vaccination a priori, 28, 29 or variables from bivariate results (P < .05) that could reasonably affect Tdap receipt,
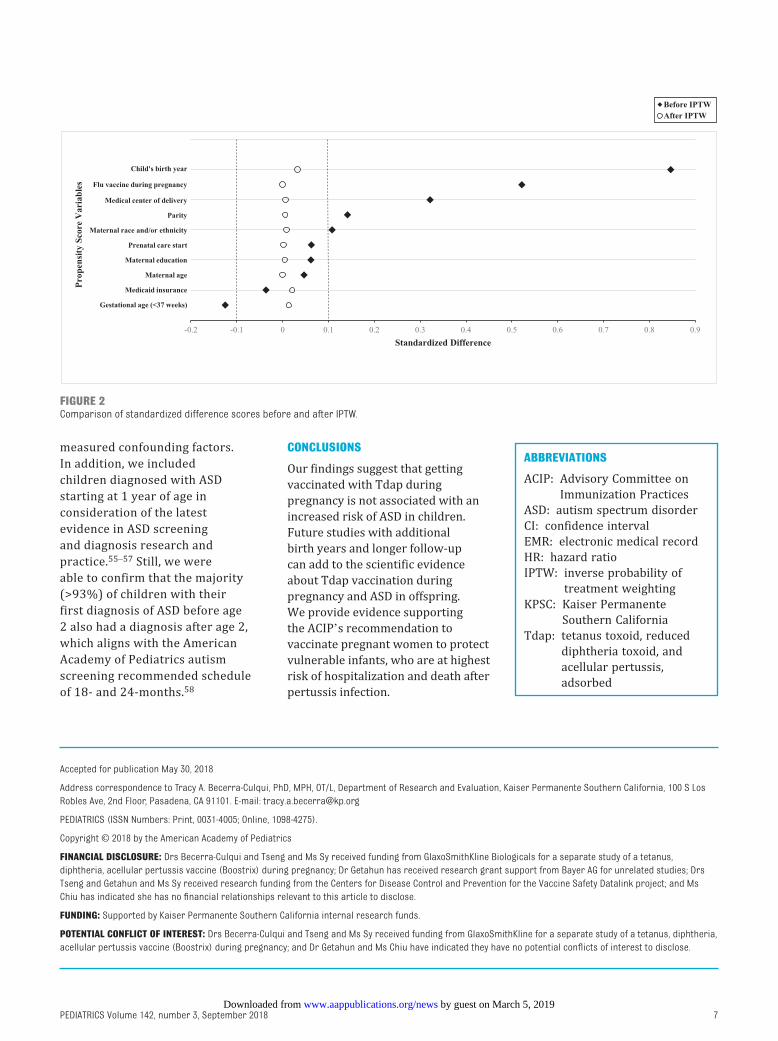
to estimate the probability of Tdap vaccination. The following variables were included: child’s birth year, gestational age at birth (<37 or ≥37 weeks’ gestation), maternal age, race and/or ethnicity, education, medical center of delivery, Medicaid insurance, parity, start of prenatal care, and influenza vaccination during pregnancy. Second, the weight for each mother was calculated as the inverse of her predicted probability of Tdap exposure and was normalized by dividing by the mean weight of each exposure group. Standardized difference scores were used to assess whether balance of covariates was achieved between the comparison groups. Unlike P values, for which the magnitude is highly related to the sample size, standardized difference is a unified approach to quantifying the magnitude of difference between groups regardless of sample size; an absolute value <0.10 is considered a negligible difference.30, 31
RESULTS
There were 109 536 women who had continuous enrollment since the beginning of pregnancy with nonassisted conceptions and gave birth to live singletons between January 1, 2011, and December 31, 2014. Of these, 94 400 (86.2%) children were enrolled by 1 year of age. After excluding an additional 9356 (8.5%) children with <90 days of continuous enrollment and 3051 (2.8%) diagnosed with chromosomal or congenital anomalies, the study included 81 993 children (Fig 1).
Prenatal Tdap vaccination coverage ranged from 26% (5407 of 20 553) for the 2012 birth cohort to 79% (16 882 of 21 433) for the 2014 birth cohort. The mean and median gestational age at vaccination was 28 weeks (SD: 7.4) and 29 weeks, respectively (interquartile range: 26–33 weeks). Women vaccinated during pregnancy were more likely to
PEDIATRICS Volume 142, number 3, September 2018 3 by guest on March 5, 2019www.aappublications.org/newsDownloaded from

be Asian American or Pacific Islander, have a bachelor’s degree or higher, be nulliparous, have received the influenza vaccine prenatally, and give birth at term (≥37 weeks’ gestation) compared with unvaccinated women (Table 1).
The follow-up time ranged between 1.2 and 6.5 years and was on average longer in the unvaccinated group (Table 2). There was an average difference of 6 months in follow-up time between both groups (unvaccinated, mean: 4.44 years [SD: 1.18]; vaccinated, mean: 3.85 years
[SD: 1.29]). Approximately 15% of children in the unvaccinated and 13% in the vaccinated group did not have complete follow-up through the end of the study because of termination of KPSC membership. ASD was diagnosed in 1341 children (1.6%). The proportion of children with ASD across birth years revealed a decline from 2.0% to 1.5% in the unvaccinated and 1.8% to 1.2% in the vaccinated group. Among children diagnosed with ASD, the first diagnosis commonly occurred at 2 years of age in either of the exposure
groups (44%) followed by diagnoses at ages 3 and 4 years. Among children diagnosed with ASD before age 2 (n = 213), 93.5% of children had a second confirmatory diagnosis after age 2 years. Among children of unvaccinated mothers and children of vaccinated mothers, there were 187 (0.44%) and 126 (0.32%) children, respectively, who did not have an outpatient encounter after 1 year of age.
The ASD incidence rate was 3.78 per 1000 person-years in the Tdap vaccinated and 4.05 per 1000 person-years in the unvaccinated group (Table 3). The unadjusted HR was 0.98 (95% CI: 0.88–1.09). After propensity score weighting, the standardized difference scores were <0.1 for all variables, suggesting a good balance of covariates (Fig 2). The IPTW-adjusted analyses showed that Tdap vaccination during pregnancy was not associated with increased ASD risk (HR: 0.85, 95% CI: 0.77–0.95). Results were consistent across study birth years and among nulliparous women.
DISCUSSION
In this large retrospective observational cohort study of 81 993 pairs of diverse pregnant women and their children, we found no evidence of increased risk for ASD diagnosis associated with Tdap vaccination during pregnancy. Subanalyses supported the overall results, revealing minimal variability by year of birth and parity. No study to our knowledge has been published with results examining the risk of ASD after maternal exposure to the Tdap vaccine.
Maternal immune activation during pregnancy is hypothesized to indirectly affect fetal neurodevelopment.32 – 35 Researchers have found infections during pregnancy (eg, rubella and influenza),
BECERRA-CULQUI et al4
FIGURE 1Inclusion flowchart. a Live births from nonassisted pregnancies and from mothers who were continuously enrolled during pregnancy.
by guest on March 5, 2019www.aappublications.org/newsDownloaded from

including prolonged episodes of fever to increase autism risk, hypothesizing that maternal infections, cytokine responses, and proinflammatory pathways are likely to alter fetal brain development.32, 36 – 41 Our results potentially indicate that the maternal Tdap vaccine affects immune trajectories protecting infants against infections that would otherwise lead to neurodevelopmental alterations. Alternatively, vaccinations during pregnancy can possibly activate the maternal immune system leading to neurodevelopmental insults. However, except for 1 study in which the association between the influenza vaccine during pregnancy and ASD was examined, 42 there is an insufficient number of studies that contain examinations of this hypothesis.
Only a handful of researchers have investigated adverse events potentially associated with Tdap receipt during pregnancy that may point to possible intermediate physiologic pathways to ASD. Two studies at sites participating in the Vaccine Safety Datalink project and a third study of >1 million pregnant women revealed a small but statistically significant increased risk of chorioamnionitis after maternal Tdap vaccination (6.1% in vaccinated, 5.5% in unvaccinated).43 – 46 Although Tdap increased the risk for chorioamnionitis, the investigators in the referenced studies found that the resulting chorioamnionitis was not associated with a preterm birth, a potential risk factor for ASD.47 Given that maternal Tdap vaccination alone or mediated by chorioamnionitis did not translate to a preterm birth or any clinically relevant adverse event in newborns, 9, 46 a direct or mediated relationship between maternal Tdap and ASD is not supported.
Our findings have some strengths and limitations. ASD was determined by recorded diagnoses in the EMR and was not validated by a study- specific standardized assessment.
PEDIATRICS Volume 142, number 3, September 2018 5
TABLE 1 Characteristics of Tdap-Unvaccinated and -Vaccinated Pregnant Women Who Delivered Children Born at KPSC, 2011–2014
Characteristics Unvaccinated Vaccinated Pa
n = 42 916 (%) n = 39 077 (%)
Maternal Age at delivery, y <.0001 ≤25 8237 (19.2) 6827 (17.5) 26–30 12 486 (29.1) 11 573 (29.6) 31–34 11 902 (27.7) 11 280 (28.9) ≥35 10 291 (24.0) 9397 (24.1) Race and/or ethnicity <.0001 Non-Hispanic white 11 127 (25.9) 10 322 (26.4) Non-Hispanic African American 3718 (8.7) 2474 (6.3) Hispanic 20 981 (48.9) 18 789 (48.1) Non-Hispanic Asian American or Pacific Islander 5947 (13.9) 6375 (16.3) Other or multiracial 1106 (2.6) 1061 (2.7) Unknown 37 (0.1) 56 (0.1) Primary language .6554 English 39 525 (92.1) 36 044 (92.2) Other 2936 (6.8) 2612 (6.7) Missing 455 (1.1) 421 (1.1) Needs interpreter 1608 (3.7) 1463 (3.7) <.0001 Education <.0001 Less than or equal to high school 11 410 (26.6) 9912 (25.3) Some college 13 329 (31.1) 11 402 (29.2) Bachelor’s degree 10 792 (25.1) 10 516 (26.9) Greater than or equal to master’s degree 6888 (16.0) 6744 (17.3) Unknown 497 (1.2) 523 (1.3)Prenatal Medicaid insurance 2489 (5.8) 1947 (5.0) <.0001 Parity <.0001 0 16 184 (37.7) 17 353 (44.4) 1 15 616 (36.4) 13 210 (33.8) ≥2 11 112 (25.9) 8512 (21.8) Start of prenatal care <.0001 ≤3 mo gestation 39 911 (93.0) 36 922 (94.5) >3 mo gestation 2733 (6.4) 1954 (5.0) No care or missing 272 (0.6) 201 (0.5) Received influenza vaccine 18 272 (42.6) 26 449 (67.7) <.0001 Pregestational hypertension 1583 (3.7) 1256 (3.2) .0002 Pregestational diabetes 829 (1.9) 683 (1.7) .0507 Gestational diabetes 6513 (15.2) 6238 (16.0) .0019 Placenta previa and/or placental abruption 2416 (5.6) 2232 (5.7) .6112 Preeclampsia or eclampsia 3514 (8.2) 3139 (8.0) .4162Child Sex .0147 Female 20 886 (48.7) 19 351 (49.5) Male 22 030 (51.3) 19 726 (50.5) Birth y <.0001 2011 11 202 (26.1) 8063 (20.6) 2012 15 146 (35.3) 5407 (13.8) 2013 12 017 (28.0) 8725 (22.3) 2014 4551 (10.6) 16 882 (43.2) Birth season <.0001 Winter (January to March) 10 191 (23.7) 9056 (23.2) Spring (April to June) 10 623 (24.8) 9184 (23.5) Summer (July to September) 11 688 (27.2) 10 076 (25.8) Fall (October to December) 10 414 (24.3) 10 761 (27.5) Gestational age, wk (mean, SD) 38.6 (1.98) 38.9 (1.50) <.0001 Preterm birth, <37 wk 3855 (9.0) 2235 (5.7) <.0001 Birth wt, g (mean, SD) 3328.0 (568.58) 3369.5 (500.04) <.0001
a P values were calculated by using χ2 or Student’s t test and do not include missing or unknown values.
by guest on March 5, 2019www.aappublications.org/newsDownloaded from

In addition, misclassification of ASD diagnosis could have occurred among children with dual insurance or limited health care use, if they sought care for ASD elsewhere. However, incident ASD diagnoses were likely captured consistently during most of the study years because of a California law enacted in 2012 (Senate Bill 946) requiring health plans to cover ASD-associated health costs, such as diagnostic and behavioral health treatment, 48 prompting the implementation of
systematic procedures for screening and diagnosing within the KPSC health care system. Thus, a diagnosis of ASD can only be made by qualified mental health professionals (child and/or adolescent psychiatrists, developmental and/or behavioral pediatricians, child psychologists, or neurologists). In addition, the combined prevalence of ASD in this study was 1.6%, comparable to the estimated 1.7% prevalence among 8-year-old children reported in the United States.49 In addition,
vaccinated and unvaccinated women may be different in aspects that may also be associated with ASD diagnosis. Because study follow-up time was dependent on the child’s birth year, children in this study had different opportunities for receiving an ASD diagnosis (ie, children born in 2011 had maximum follow-up potential of 5.5–6.5 years, whereas children born in 2014 had 2.5–3.5 years). Based on US representative data, 3 to 5 years of age is the period when most children with an ASD are diagnosed.50 Thus, we likely did not capture some children with ASD born in later study years considering that some children with milder ASD would not be diagnosed until they reach school age. Similarly, maternal Tdap vaccine uptake varied by birth year because of evolving ACIP recommendations and pertussis epidemics in California.2, 51, 52 However, because we identified minimal variability in study results when stratifying by birth year, these variations likely did not affect our results. In addition, although we controlled for major known confounding factors related to Tdap vaccination and ASD, our results could have been affected by residual confounding, such as behavioral or clinical factors not captured by the EMR. For example, we did not control for having an older sibling with ASD, although the sibling recurrence risk is between 10% and 20%, a 10- to 20-fold increase over the general population’s prevalence.53, 54 However, in our analysis restricted to mothers giving birth to their first child, the results were consistent with overall findings.
Our study has additional strengths. Maternal Tdap vaccination and ASD information was not subject to recall bias, and our weighting procedures enabled us to balance the Tdap exposed and unexposed groups to compare 2 populations that were comparable in important
BECERRA-CULQUI et al6
TABLE 2 Follow-up and ASD Diagnosis in Children Born Between 2011 and 2014 to Women Who Were Unvaccinated and Vaccinated With Tdap During Pregnancy
Unvaccinated n = 42 916 Vaccinated n = 39 077 Pa
Follow-up characteristics Total follow-up time (1000 person y) 190.74 150.56 —Length of follow-up, y Mean (SD) 4.44 (1.18) 3.85 (1.29) <.0001 Median 4.60 3.50 Q1, Q3 3.7, 5.3 2.9, 4.9 Range (1.2–6.5) (1.2–6.5)Reasons for ending follow-up Termination of KPSC membership,
n (%)6508 (15.2) 5242 (13.4) <.0001
End of study (June 30, 2017), n (%) 35 636 (83.0) 33 266 (85.1) <.0001 ASD diagnosis, n (%) 772 (1.8) 569 (1.5) .0008ASD diagnosis prevalence by birth y,
n (%) 2011 218 of 11 202 (1.9) 143 of 8063 (1.8) .3836 2012 282 of 15 146 (1.9) 80 of 5407 (1.5) .0666 2013 206 of 12 017 (1.7) 145 of 8725 (1.7) .7729 2014 66 of 4551 (1.5) 201 of 16 882 (1.2) .1611ASD diagnosis age, n (%), y 772 (100) 569 (100) <.0001 1 97 (12.6) 116 (20.4) 2 337 (43.7) 251 (44.1) 3 or 4 314 (40.7) 178 (31.3) 5 or 6 24 (3.1) 24 (4.2)
—, not applicable.a P values were calculated by using χ2 or Student’s t test.
TABLE 3 Rates and Associations Between Tdap Vaccination During Pregnancy and ASD Among Children Born Between 2011 and 2014
ASD Incidence Rate per 1000 Person y HR (95% CI)
Unvaccinated Vaccinated Unadjusted IPTW-Adjusteda
Overall 4.05 3.78 0.98 (0.88–1.09) 0.85 (0.77–0.95)Birth y 2011 3.57 3.22 0.91 (0.74–1.12) 0.86 (0.70–1.07) 2012 4.02 3.18 0.80 (0.62–1.02) 0.80 (0.63–1.03) 2013 4.48 4.46 1.00 (0.81–1.23) 0.99 (0.80–1.23) 2014 4.87 4.14 0.89 (0.68–1.18) 0.85 (0.65–1.12)Nulliparous 4.88 4.56 0.99 (0.85–1.15) 0.88 (0.75–1.02)
a Adjustments were made for child’s birth y, gestational age at birth (<37 or ≥37 wk); maternal age, race and/or ethnicity, and education; Medicaid insurance, medical center of delivery, parity, start of prenatal care, and influenza vaccination during pregnancy.
by guest on March 5, 2019www.aappublications.org/newsDownloaded from
measured confounding factors. In addition, we included children diagnosed with ASD starting at 1 year of age in consideration of the latest evidence in ASD screening and diagnosis research and practice.55 – 57 Still, we were able to confirm that the majority (>93%) of children with their first diagnosis of ASD before age 2 also had a diagnosis after age 2, which aligns with the American Academy of Pediatrics autism screening recommended schedule of 18- and 24-months.58
CONCLUSIONS
Our findings suggest that getting vaccinated with Tdap during pregnancy is not associated with an increased risk of ASD in children. Future studies with additional birth years and longer follow-up can add to the scientific evidence about Tdap vaccination during pregnancy and ASD in offspring. We provide evidence supporting the ACIP’s recommendation to vaccinate pregnant women to protect vulnerable infants, who are at highest risk of hospitalization and death after pertussis infection.
PEDIATRICS Volume 142, number 3, September 2018 7
Accepted for publication May 30, 2018
Address correspondence to Tracy A. Becerra-Culqui, PhD, MPH, OT/L, Department of Research and Evaluation, Kaiser Permanente Southern California, 100 S Los Robles Ave, 2nd Floor, Pasadena, CA 91101. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2018 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Drs Becerra-Culqui and Tseng and Ms Sy received funding from GlaxoSmithKline Biologicals for a separate study of a tetanus, diphtheria, acellular pertussis vaccine (Boostrix) during pregnancy; Dr Getahun has received research grant support from Bayer AG for unrelated studies; Drs Tseng and Getahun and Ms Sy received research funding from the Centers for Disease Control and Prevention for the Vaccine Safety Datalink project; and Ms Chiu has indicated she has no financial relationships relevant to this article to disclose.
FUNDING: Supported by Kaiser Permanente Southern California internal research funds.
POTENTIAL CONFLICT OF INTEREST: Drs Becerra-Culqui and Tseng and Ms Sy received funding from GlaxoSmithKline for a separate study of a tetanus, diphtheria, acellular pertussis vaccine (Boostrix) during pregnancy; and Dr Getahun and Ms Chiu have indicated they have no potential conflicts of interest to disclose.
ABBREVIATIONS
ACIP: Advisory Committee on Immunization Practices
ASD: autism spectrum disorderCI: confidence intervalEMR: electronic medical recordHR: hazard ratioIPTW: inverse probability of
treatment weightingKPSC: Kaiser Permanente
Southern CaliforniaTdap: tetanus toxoid, reduced
diphtheria toxoid, and acellular pertussis, adsorbed
FIGURE 2Comparison of standardized difference scores before and after IPTW.
by guest on March 5, 2019www.aappublications.org/newsDownloaded from

REFERENCES
1. Gambhir M, Clark TA, Cauchemez S, Tartof SY, Swerdlow DL, Ferguson NM. A change in vaccine efficacy and duration of protection explains recent rises in pertussis incidence in the United States. PLoS Comput Biol. 2015;11(4):e1004138
2. Winter K, Glaser C, Watt J, Harriman K; Centers for Disease Control and Prevention. Pertussis epidemic–California, 2014. MMWR Morb Mortal Wkly Rep. 2014;63(48):1129–1132
3. Centers for Disease Control and Prevention. Pertussis (whooping cough). 2017. Available at: https:// www. cdc. gov/ pertussis/ about/ signs- symptoms. html. Accessed June 6, 2017
4. Centers for Disease Control and Prevention. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months — Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60(41):1424–1426
5. Centers for Disease Control and Prevention. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine (Tdap) in pregnant women–Advisory Committee on Immunization Practices (ACIP), 2012. MMWR Morb Mortal Wkly Rep. 2013;62(7):131–135
6. Baxter R, Bartlett J, Fireman B, Lewis E, Klein NP. Effectiveness of vaccination during pregnancy to prevent infant pertussis. Pediatrics. 2017;139(5):e20164091
7. Centers for Disease Control and Prevention. Recommended immunization schedules for persons aged 0 through 18 years—United States, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(5):1–4
8. Zheteyeva YA, Moro PL, Tepper NK, et al. Adverse event reports after tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccines in pregnant women. Am J Obstet Gynecol. 2012;207(1):59.e1–59.e7
9. Sukumaran L, McCarthy NL, Kharbanda EO, et al. Association of Tdap vaccination with acute events and adverse birth outcomes among pregnant women with prior tetanus-containing immunizations. JAMA. 2015;314(15):1581–1587
10. DeSilva M, Vazquez-Benitez G, Nordin JD, et al. Tdap vaccination during pregnancy and microcephaly and other structural birth defects in offspring. JAMA. 2016;316(17):1823–1825
11. Moro PL, Cragan J, Tepper N, et al. Enhanced surveillance of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccines in pregnancy in the Vaccine Adverse Event Reporting System (VAERS), 2011-2015. Vaccine. 2016;34(20):2349–2353
12. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013
13. Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators; Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders–autism and developmental disabilities monitoring network, 14 sites, United States, 2008. MMWR Surveill Summ. 2012;61(3):1–19
14. Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators; Centers for Disease Control and Prevention. Prevalence of autism spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014;63(2):1–21
15. Courchesne E, Yeung-Courchesne R, Press GA, Hesselink JR, Jernigan TL. Hypoplasia of cerebellar vermal lobules VI and VII in autism. N Engl J Med. 1988;318(21):1349–1354
16. Gardener H, Spiegelman D, Buka SL. Prenatal risk factors for autism: comprehensive meta-analysis. Br J Psychiatry. 2009;195(1):7–14
17. Stoner R, Chow ML, Boyle MP, et al. Patches of disorganization in the neocortex of children with autism. N Engl J Med. 2014;370(13):1209–1219
18. Getahun D, Fassett MJ, Peltier MR, et al. Association of perinatal risk factors with autism spectrum disorder. Am J Perinatol. 2017;34(3):295–304
19. Hallmayer J, Cleveland S, Torres A, et al. Genetic heritability and shared environmental factors among twin pairs with autism. Arch Gen Psychiatry. 2011;68(11):1095–1102
20. Hertz-Picciotto I, Croen LA, Hansen R, Jones CR, van de Water J, Pessah IN. The CHARGE study: an epidemiologic investigation of genetic and environmental factors contributing to autism. Environ Health Perspect. 2006;114(7):1119–1125
21. Becerra TA, Wilhelm M, Olsen J, Cockburn M, Ritz B. Ambient air pollution and autism in Los Angeles county, California. Environ Health Perspect. 2013;121(3):380–386
22. American Academy of Pediatrics. Vaccine safety: examine the evidence. 2013. Available at: https:// www. aap. org/ en- us/ Documents/ immunization_ vaccine_ studies. pdf. Accessed November 16, 2017
23. Stratton K, Gable A, Shetty P, McCormick M, eds; Institute of Medicine Immunization Safety Review Committee. Immunization Safety Review: Measles-Mumps-Rubella Vaccine and Autism. Washington, DC: National Academies Press; 2001
24. Hviid A, Stellfeld M, Wohlfahrt J, Melbye M. Association between thimerosal-containing vaccine and autism. JAMA. 2003;290(13):1763–1766
25. Koebnick C, Langer-Gould AM, Gould MK, et al. Sociodemographic characteristics of members of a large, integrated health care system: comparison with US Census Bureau data. Perm J. 2012;16(3):37–41
26. Pasteur S. Adacel: prescribing information (tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine, adsorbed). 2017. Available at: https:// www. fda. gov/ downloads/ biologicsbloodvac cines/ vaccines/ approvedproducts/ ucm142764. pdf. Accessed January 8, 2018
27. Luyster R, Gotham K, Guthrie W, et al. The autism diagnostic observation schedule-toddler module: a new module
BECERRA-CULQUI et al8 by guest on March 5, 2019www.aappublications.org/newsDownloaded from

of a standardized diagnostic measure for autism spectrum disorders. J Autism Dev Disord. 2009;39(9):1305–1320
28. Butler AM, Layton JB, Li D, et al. Predictors of low uptake of prenatal tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis immunization in privately insured women in the United States. Obstet Gynecol. 2017;129(4):629–637
29. Goldfarb IT, Little S, Brown J, Riley LE. Use of the combined tetanus-diphtheria and pertussis vaccine during pregnancy. Am J Obstet Gynecol. 2014; 211(3):299.e1–299.e5
30. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424
31. Yang D, Dalton JE. A unified approach to measuring the effect size between two groups using SAS. In: Proceedings from the SAS Global Forum; April 22–25, 2012; Orlando, FL. Paper 335-2012
32. Patterson PH. Maternal infection and immune involvement in autism. Trends Mol Med. 2011;17(7):389–394
33. Smith SE, Li J, Garbett K, Mirnics K, Patterson PH. Maternal immune activation alters fetal brain development through interleukin-6. J Neurosci. 2007;27(40):10695–10702
34. Shi L, Tu N, Patterson PH. Maternal influenza infection is likely to alter fetal brain development indirectly: the virus is not detected in the fetus. Int J Dev Neurosci. 2005;23(2–3):299–305
35. Hagberg H, Gressens P, Mallard C. Inflammation during fetal and neonatal life: implications for neurologic and neuropsychiatric disease in children and adults. Ann Neurol. 2012;71(4):444–457
36. Atladóttir HO, Henriksen TB, Schendel DE, Parner ET. Autism after infection, febrile episodes, and antibiotic use during pregnancy: an exploratory study. Pediatrics. 2012;130(6). Available at: www. pediatrics. org/ cgi/ content/ full/ 130/ 6/ e1447
37. Chess S, Fernandez P, Korn S. Behavioral consequences of congenital rubella. J Pediatr. 1978;93(4):699–703
38. Patterson PH. Maternal infection: window on neuroimmune interactions in fetal brain development and mental illness. Curr Opin Neurobiol. 2002;12(1):115–118
39. Krakowiak P, Goines PE, Tancredi DJ, et al. Neonatal cytokine profiles associated with autism spectrum disorder. Biol Psychiatry. 2017;81(5):442–451
40. Masi A, Glozier N, Dale R, Guastella AJ. The immune system, cytokines, and biomarkers in autism spectrum disorder. Neurosci Bull. 2017;33(2):194–204
41. Zerbo O, Yoshida C, Grether JK, et al. Neonatal cytokines and chemokines and risk of autism spectrum disorder: the Early Markers for Autism (EMA) study: a case-control study. J Neuroinflammation. 2014;11:113
42. Zerbo O, Qian Y, Yoshida C, Fireman BH, Klein NP, Croen LA. Association between influenza infection and vaccination during pregnancy and risk of autism spectrum disorder. JAMA Pediatr. 2017;171(1):e163609
43. Kharbanda EO, Vazquez-Benitez G, Lipkind HS, et al. Evaluation of the association of maternal pertussis vaccination with obstetric events and birth outcomes. JAMA. 2014;312(18):1897–1904
44. Committee on Obstetric Practice. Committee opinion no. 712: intrapartum management of intraamniotic infection. Obstet Gynecol. 2017;130(2):e95–e101
45. DeSilva M, Vazquez-Benitez G, Nordin JD, et al. Maternal Tdap vaccination and risk of infant morbidity. Vaccine. 2017;35(29):3655–3660
46. Layton JB, Butler AM, Li D, et al. Prenatal Tdap immunization and risk of maternal and newborn adverse events. Vaccine. 2017;35(33):4072–4078
47. Wang C, Geng H, Liu W, Zhang G. Prenatal, perinatal, and postnatal factors associated with autism: a meta-analysis. Medicine (Baltimore). 2017;96(18):e6696
48. Steinberg N. Senate Bill 946, Chapter 650. 2011 California regular Session, Health care coverage: mental illness: pervasive developmental disorder or autism: public health. Available at http:// leginfo. legislature. ca. gov/ faces/ billNavClient. xhtml? bill_ id= 201120120SB946. Accessed July 2, 2018
49. Baio J, Wiggins L, Christensen DL, et al. Prevalence of autism spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveill Summ. 2018;67(6):1–23
50. Christensen DL, Baio J, Van Naarden Braun K, et al; Centers for Disease Control and Prevention. Prevalence and characteristics of autism spectrum disorder among children aged 8 years–autism and developmental disabilities monitoring network, 11 sites, United States, 2012. MMWR Surveill Summ. 2016;65(3):1–23
51. Winter K, Harriman K, Zipprich J, et al. California pertussis epidemic, 2010. J Pediatr. 2012;161(6):1091–1096
52. Winter K, Zipprich J, Harriman K. Pertussis in California: a tale of 2 epidemics. Pediatr Infect Dis J. 2018;37(4):324–328
53. Szatmari P, Chawarska K, Dawson G, et al. Prospective longitudinal studies of infant siblings of children with autism: lessons learned and future directions. J Am Acad Child Adolesc Psychiatry. 2016;55(3):179–187
54. Xie F, Peltier M, Getahun D. Is the risk of autism in younger siblings of affected children moderated by sex, race/ethnicity, or gestational age? J Dev Behav Pediatr. 2016;37(8):603–609
55. Sacrey LA, Bennett JA, Zwaigenbaum L. Early infant development and intervention for autism spectrum disorder. J Child Neurol. 2015;30(14):1921–1929
56. Zwaigenbaum L, Bauman ML, Stone WL, et al. Early identification of autism spectrum disorder: recommendations for practice and research. Pediatrics. 2015;136(suppl 1):S10–S40
57. Ozonoff S, Iosif AM, Baguio F, et al. A prospective study of the emergence of early behavioral signs of autism. J Am Acad Child Adolesc Psychiatry. 2010;49(3):256–266.e1–e2
58. American Academy of Pediatrics. Recommendations for preventive pediatric health care. 2017. Available at: https:// www. aap. org/ en- us/ Documents/ periodicity_ schedule. pdf. Accessed July 12, 2017
PEDIATRICS Volume 142, number 3, September 2018 9 by guest on March 5, 2019www.aappublications.org/newsDownloaded from

originally published online August 13, 2018; Pediatrics Tracy A. Becerra-Culqui, Darios Getahun, Vicki Chiu, Lina S. Sy and Hung Fu Tseng
Spectrum DisorderPrenatal Tetanus, Diphtheria, Acellular Pertussis Vaccination and Autism
ServicesUpdated Information &
018-0120http://pediatrics.aappublications.org/content/early/2018/08/09/peds.2including high resolution figures, can be found at:
References
018-0120#BIBLhttp://pediatrics.aappublications.org/content/early/2018/08/09/peds.2This article cites 50 articles, 4 of which you can access for free at:
Subspecialty Collections
_subhttp://www.aappublications.org/cgi/collection/vaccine:immunizationVaccine/Immunizationbhttp://www.aappublications.org/cgi/collection/infectious_diseases_suInfectious Diseasehttp://www.aappublications.org/cgi/collection/autism:asd_subAutism/ASDal_issues_subhttp://www.aappublications.org/cgi/collection/development:behaviorDevelopmental/Behavioral Pediatricsfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on March 5, 2019www.aappublications.org/newsDownloaded from

originally published online August 13, 2018; Pediatrics Tracy A. Becerra-Culqui, Darios Getahun, Vicki Chiu, Lina S. Sy and Hung Fu Tseng
Spectrum DisorderPrenatal Tetanus, Diphtheria, Acellular Pertussis Vaccination and Autism
http://pediatrics.aappublications.org/content/early/2018/08/09/peds.2018-0120located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2018 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on March 5, 2019www.aappublications.org/newsDownloaded from