Prenatal diagnosis of Partial Trisomy 2q. Case Report
3
, . 17:9: 874–876 (1997) SHORT COMMUNICATION PRENATAL DIAGNOSIS OF PARTIAL TRISOMY 2q. CASE REPORT 1 , 1 , ˜ 2 , ´ 3 , ´ 2,3 1 * 1 Department of Obstetrics and Gynaecology, Medical Faculty of Porto, Hospital S. Joa ˜o, Porto, Portugal 2 Unit of Genetics, IPATIMUP, Porto, Portugal 3 Department of Medical Genetics, Medical Faculty of Porto, Porto, Portugal Received 7 October 1996 Revised 12 January 1997 Accepted 2 February 1997 SUMMARY A case of partial trisomy 2(q21q33) detected by cordocentesis at 27 weeks’ gestation in a polymalformed fetus is described. This is the second case of a prenatally detected de novo duplication of 2q and the first involving the region referred to above. ? 1997 by John Wiley & Sons, Ltd. Prenat. Diagn. 17: 874–876, 1997 No. of Figures: 2. No. of Tables: 0. No. of References: 7. : prenatal diagnosis; chromosome 2; duplication; partial trisomy INTRODUCTION First reported by Ricci et al. (1968), partial trisomy 2q is a rare chromosomal aberration, with only eight cases reported in the literature (Schinzel, 1994). Of these, only one report con- cerns dup(2)(q21q33) (Schumacher et al., 1983). We report on a case of isolated partial trisomy of that region ascertained prenatally. CASE REPORT A 31-year-old Caucasian primigravida was referred to our hospital at 28 weeks’ gestation because of suspected fetal malformations on a routine ultrasound at 27 weeks. Her past history was unremarkable. There was no pregnancy exposure to drugs, smoking, alcohol, or known teratogenic agents. She had a brother who died in the neonatal period with no specified congenital malformations. The family history was otherwise irrelevant, with no other cases of congenital anomalies or mental retardation. Her husband, aged 31 years, was healthy and not consanguineous. His family history was unremarkable. Her pregnancy was uneventful and all screening analytical procedures during the first and second trimesters were normal, including serology for cytomegalovirus, toxoplasma, herpes, rubella, syphilis, and hepatitis B and C. An ultrasound scan, performed in our hospital at 28 weeks, revealed a male fetus with biometry consistent with the gestational age, Dandy– Walker syndrome, ventricular septal defect, club- feet, epispadias, and no visible left kidney. A fetal blood sample was obtained by cordocentesis for cytogenetic studies. A 46,XY,dup(2)(q21q33) chromosomal constitution was observed in all cells examined after conventional GTG banding (Fig. 1) and later confirmed by chromosome painting with a chromosome 2-specific library *Correspondence to: Professor Dr Nuno Montenegro, Department of Obstetrics and Gynaecology, Hospital S. Joa ˜o, P-4200 Porto, Portugal. CCC 0197–3851/97/090874–03 $17.50 ? 1997 by John Wiley & Sons, Ltd.
Transcript of Prenatal diagnosis of Partial Trisomy 2q. Case Report

, . 17:9: 874–876 (1997)
SHORT COMMUNICATION
PRENATAL DIAGNOSIS OF PARTIAL TRISOMY2q. CASE REPORT
1, 1, 2, 3, 2,3 1*
1Department of Obstetrics and Gynaecology, Medical Faculty of Porto, Hospital S. Joao, Porto, Portugal2Unit of Genetics, IPATIMUP, Porto, Portugal
3Department of Medical Genetics, Medical Faculty of Porto, Porto, Portugal
Received 7 October 1996Revised 12 January 1997Accepted 2 February 1997
SUMMARY
A case of partial trisomy 2(q21q33) detected by cordocentesis at 27 weeks’ gestation in a polymalformed fetus isdescribed. This is the second case of a prenatally detected de novo duplication of 2q and the first involving the regionreferred to above. ? 1997 by John Wiley & Sons, Ltd.
Prenat. Diagn. 17: 874–876, 1997No. of Figures: 2. No. of Tables: 0. No. of References: 7.
: prenatal diagnosis; chromosome 2; duplication; partial trisomy
INTRODUCTION
First reported by Ricci et al. (1968), partialtrisomy 2q is a rare chromosomal aberration,with only eight cases reported in the literature(Schinzel, 1994). Of these, only one report con-cerns dup(2)(q21q33) (Schumacher et al., 1983).We report on a case of isolated partial trisomy ofthat region ascertained prenatally.
CASE REPORT
A 31-year-old Caucasian primigravida wasreferred to our hospital at 28 weeks’ gestationbecause of suspected fetal malformations on aroutine ultrasound at 27 weeks.Her past history was unremarkable. There was
no pregnancy exposure to drugs, smoking, alcohol,or known teratogenic agents. She had a brother
who died in the neonatal period with no specifiedcongenital malformations. The family historywas otherwise irrelevant, with no other cases ofcongenital anomalies or mental retardation. Herhusband, aged 31 years, was healthy and notconsanguineous. His family history wasunremarkable.Her pregnancy was uneventful and all screening
analytical procedures during the first and secondtrimesters were normal, including serology forcytomegalovirus, toxoplasma, herpes, rubella,syphilis, and hepatitis B and C.An ultrasound scan, performed in our hospital
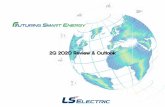
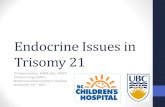
at 28 weeks, revealed a male fetus with biometryconsistent with the gestational age, Dandy–Walker syndrome, ventricular septal defect, club-feet, epispadias, and no visible left kidney. A fetalblood sample was obtained by cordocentesisfor cytogenetic studies. A 46,XY,dup(2)(q21q33)chromosomal constitution was observed in allcells examined after conventional GTG banding(Fig. 1) and later confirmed by chromosomepainting with a chromosome 2-specific library
*Correspondence to: Professor Dr Nuno Montenegro,Department of Obstetrics and Gynaecology, Hospital S. Joao,P-4200 Porto, Portugal.
CCC 0197–3851/97/090874–03 $17.50? 1997 by John Wiley & Sons, Ltd.

(Fig. 2). The karyotypes of the parents werenormal.At 33 weeks, she was admitted to our hospital
with pre-eclampsia. Premature rupture of themembranes occurred 3 days after admittance, and5 h later a male infant weighing 1650 g wasdelivered vaginally and died 5 min later.Phenotypic characteristics included a prominent
forehead, hypertelorism, a broad and flat nose,low-set posteriorly rotated ears, a short neck,sacrococcygeal fistula, hypospadias, bilateral pre-axial polydactyly in the hands (syndactyly betweenthe index finger and a supranumerary finger), andequinovarus feet.Autopsy findings included complex heart defects
(transposition of the great vessels, abnormal pul-monary venous drainage, a hypoplastic left heart,and pulmonary artery atresia), and urinary tractmalformation (including a pelvic left kidney).
DISCUSSION
To our knowledge, this is the second report ofa prenatally diagnosed case of isolated partialtrisomy 2q (Marchese et al., 1984) and the firstconcerning region 2q21q33. Most duplicationsinvolving 2q reported in the literature concernthe offspring of parents with balanced reciprocaltranslocations. Thus, the imbalances present inthese patients include, in addition to partial tri-somy 2q, duplications or deletions of parts ofother chromosomes. The phenotypic abnormali-ties present in these patients could thereforeresult from either the partial trisomy 2q or theother imbalances present. From the cases pre-viously reported with isolated partial trisomy of2q (Schinzel, 1994), only one involves segment2q21q33 (Schumacher et al., 1983), as observed inour case. Both the case described here and the
Fig. 1—Partial karyotype of GTG banding metaphase of chromosome 2
875 2q
? 1997 by John Wiley & Sons, Ltd. . ., . 17: 874–876 (1997)

case reported by Schumacher et al. (1983) hadin common craniofacial anomalies (prominentforehead, broad and flat nasal bridge, mal-formed ears, and short neck), cardiac defects(ventricular septal defect, left outflow tractanomalies, and pulmonary atresia), and renalectopia.Although the abnormalities described can be
found in a large number of chromosomal imbal-ances, it is interesting to note that no heart defectswere described in association with isolated trisomyof the segments distal to 2q31 (Romain et al.,1994). This suggests that the cardiac defects inour case, as well as in the patient described bySchumacher et al. (1983), are indeed related to 2q2duplication.As concerns the limb malformations, it is note-
worthy that the HOXD cluster, a family ofgenes supposed to play a role in the control oflimb morphogenesis (Johnson et al., 1994; Tickle,1995) and whose alterations have been implicatedin limb malformations (Akarsu et al., 1996),was recently mapped to 2q31 (Sarfarazi et al.,1995).Besides adding to the clinical characterization
of the partial trisomy 2q21q33, this case furtherillustrates the usefulness of fluorescence in situhybridization (FISH) studies in the elucidationof a prenatally detected de novo chromosomalrearrangement.
REFERENCES
Akarsu, A.N., Stoilov, I., Yilmaz, E., Sayli, B.S.,Sarjarazi, M. (1996). Genomic structure of HOXD8gene: a nine polyalanina duplication causes synpoly-dactyly in two unrelated families. Hum. Hol. Gen., 5,945–952.
Johnson, R.L., Riddle, R.D., Tabin, C.J. (1994). Mecha-nisms of limb patterning, Curr. Opin. Genet. Dev., 4,535–542.
Marchese, S., Diggans, G., Garver, K., Stadler, M.(1984). De novo 46,XX,dup(2)(q21]q31) ascertainedby prenatal cytogenetic analysis, Am. J. Hum. Genet.(Suppl.), 36, 1035.
Ricci, N., Dallapiccola, B., Cotti, G. (1968). Trans-location 2D familial, Ann. Genet., 11, 111–113.
Romain, D.R., Mackenzie, N.G., Moss, D.,Columbano-Green, L.M., Smyth, R.H., Parfitt, R.G.,Dixon, J.W. (1994). Partial trisomy for 29 in a patientwith diR dup(2)(9331q35). J. Med. Gen., 31, 652–653.
Sarfarazi, M., Akarsu, A.N., Sayli, B.S. (1995). Local-ization of the syndactyly type II (synpolydactyly)locus to 2q31 region and identification of tight linkageto HOXD8 intragenic marker, Hum. Mol. Genet., 4,1453–1458.
Schinzel, A. (1994). Human Cytogenetic Database,Oxford Medical Databases Series, Oxford: OxfordUniversity Press, Electronic Publishing.
Schumacher, R.E., Rocchini, A.P., Wilson, G.N. (1983).Partial trisomy 2q, Clin. Genet., 23, 191–194.
Tickle, C. (1995). Vertebrate limb development, Curr.Opin. Genet. Dev., 5, 478–484.
Fig. 2—Chromosome painting with a chromosome 2-specific library
876 . .
? 1997 by John Wiley & Sons, Ltd.. ., . 17: 874–876 (1997)










![Prenatal diagnosis of mosaic trisomy 2 and literature review...trisomy 2. For case 1, cytogentic analysis showed a karyotype of mos 47,XY,+2[8]/46,XY[19] as shown in Fig.1. Of 27 colonies](https://static.fdocuments.net/doc/165x107/60facf977ba85d6edf705492/prenatal-diagnosis-of-mosaic-trisomy-2-and-literature-review-trisomy-2-for.jpg)