PREMYX$OElig;DEMA AND CORONARY-ARTERY DISEASE
1
Click here to load reader
Transcript of PREMYX$OElig;DEMA AND CORONARY-ARTERY DISEASE

1328
PREMYXŒDEMA AND CORONARY-ARTERY
DISEASE
P. B. S. FOWLER
J. SWALE.Charing Cross Hospital,
London W.C.2.
SIR,-Dr. Burke, who wrote last week (p. 1274), is right touse the word " fanciful " in describing our concept of circulat-ing fats, thyroxine, cestrogens, antibodies, and clofibrate
competing for binding-sites like children playing musicalchairs.
If there is a note of stricture in Dr. Burke’s use of the wordfanciful we are not unduly perturbed. It seems to us that fancyis mainly to be deprecated when garnished with obscure jargonand dressed up as fact.
If Dr. Burke is offering to test our tentative musical-chairsconcept we should be pleased to have his help.
THYROID HORMONE AND CALCIUM
METABOLISM
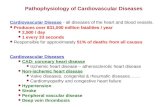
SIR,-Your leader (April 8, p. 766) drew attention to thedisturbances of calcium metabolism which often accompanythyrotoxicosis. This proved timely, because we were theninvestigating a female patient with an advanced thyrotoxicstate associated with both hypercalcasmia and hypercalcuria.Since she had presented with severe dysphagia and profoundmuscular weakness, the association of hyperparathyroidismwith thyrotoxicosis, as reported by Koenig et al.,1 seemed apossibility, despite a normal serum-phosphorus level. Periostealbone resorption was reported. Response of her abnormalcalcium metabolism to the treatment of her thyrotoxicosis wasawaited with interest. The fairly prompt fall of the raisedvalues of both serum and urinary calcium towards normallevels serves to illustrate the association which you note in
your leading article (see accompanying figure).Laboratory confirmation of severe thyrotoxicosis included
the following observations: (i) 1311 thyroidal uptake at 4
hours, 93% of tracer; (ii) ’Triosorb’ test (131 I-liothyronineuptake) 63%; (iii) serum-protein-bound-iodine, 20 g. per100 ml. The levels of serum and urinary calcium recordedin this patient are higher than those reported by Adams et1. Koenig, M. P., Scholz, D. A., Salassa, R. M. Minn. Med. 1957, 40, 782.
al. and Koenig et al.1 but similar to those reported byKleeman et al.3
In view of the unusual presentation and other special features ofthis case it is likely to be described in full at a later date.
J. N. HARRIS-JONESA. S. NAKADARA. L. WELLS.
Llanelli Hospital,Carmarthenshire.
Fall of serum and urinary calcium levels in patient with thyrotoxicosis in responseto carbimazole.
PREGNANCY TESTS AND PROTEINURIA
SiR,ŁThe letters from Dr. Kew and his colleagues (April 22,p. 902) and Dr. Warrack and Mr. Richards (April 29, p. 957),on misleading results when immunological pregnancy tests arecarried out on patients with proteinuria, call for comment.These misleading results have been known for a number ofyears. Indeed for about three years, in their leaflet of instruc-tions for the performance of their test, the manufacturers ofGravindex ’ (Ortho Pharmaceuticals Ltd.) have stated:" Urine specimens, shown by a standard protein test to con-tain excessive protein, should not be tested. In general, aprotein level of 100 mg. % is the maximum permissible levelfor consistently accurate results ".As a result of this, it was decided, about two years ago, to test
all urines for protein in cases with a positive gravindex test. Inrecent months, however, all urines have been screened for
protein as a routine in immunological tests. I agree with Dr.Warrack and Mr. Richards that it is " very little extra troubleto screen the urines ". Mere traces of proteinuria can beignored. Before doing a pregnancy test, protein is routinelyseparated from the urine, in cases where proteinuria is + + +or more by a standardised colour test, by precipitation with anequal volume of a saturated solution of ammonium sulphate,followed by filtration. Alternatively the urine is acidified with33% acetic acid, drop by drop, to a pH of around 5-5-i.e.,slightly acid to litmus-heated to about 70°C, and thenfiltered. (Even lengthy boiling or autoclaving of urine does notaffect human chorionic gonadotrophin [H.C.G.].) Traces ofblood in the urine can be ignored; larger amounts can befiltered. In hospital patients, especially if a large number ofabortions are dealt with, as in our hospital, when frank blood ispresent, catheter specimens of urine are used. It should benoted that hxmoglobin is a protein, and responds to all positive
tests for proteinuria.It is not surprising that proteinuria may give
a false pregnancy result when one considersthat H.C.G. is in fact a protein; but being aglycoprotein (molecular weight [M.w.] 100,000),it is of a different " type " from albumin(M.w. around 68,000). Egg albumin (M.w.
34,500), acidified and dissolved in 33% aceticacid, forms an albuminate and may change thereaction of known non-pregnancy urine to false
, positive. Moreover, an excessively alkalineurine may give a positive result in the absenceof protein. A standardised colour test for pro-tein changes from yellow to varying shades ofgreen when proteinuria is present, dependingon the type of protein and its concentration.If the proteins were identical, every pregnancyurine would give a positive reaction to thereagent strip for protein, owing to the presenceof this glycoprotein. It is true that, althoughthe urinary protein is mainly albumin, the pro-portion of other serum-proteins present in the
< urine varies considerably. In some patients, onlythe smaller nt.w. proteins are present on electro-phoresis of the urine; in others considerableamounts of larger M.w. proteins may be present.2. Adams, P. H., Jowsey, J., Kelly, P. J., Riggs, B. L.,
Kinney, V. R., Jones, J. D. Q. Jl Med. 1967, 36, 1.3. Kleeman, C. R., Tuttle, S., Basset, S. H., J. clin.
Endocr. Metab. 1958, 18, 447.