
TRACE 1300 and TRACE 1310 Preinstallation Requirements Guide
Upload
nguyenngocCategory
view
215download
3
Presented at 24th IFHE congress at 18-19 April 2016 in The Hague, The Netherlands
IFHE - International Federation of Hospital Engineering NVTG – Dutch Association for Technical Facility Professionals in the Healthcare Sector
PREINSTALLATION REQUIREMENTS FOR HIGHLY COMPLEX MEDICAL EQUIPMENT TO SUPPORT THE
PROCESSES OF DESIGN, PLANNING & MONITORING IN HOSPITAL CONSTRUCTION
Carolina Francisca Navarrete Guarda, Biomedical Engineer Ministry of Health, Chile

About the author 2
January - Practitioner of the Medical Equipment Unit belonging to the Investment Division
September - Biomedical Engineer of the Medical Equipment Unit belonging to the Investment Division
December - Biomedical Engineering graduate, Valparaiso University 2006 - 2012
2012 April – Biomedical Engineer of the Medical Equipment Unit belonging to the Investment Division
May - Biomedical Engineer, Specialist in Hospital Infrastructure of the oversight of construction belonging to the Investment Division
2014 Actually - Biomedical Engineer, Specialist in Hospital Infrastructure of the oversight of construction belonging to the Investment Division
2015 - 2016
• Biomedical Engineer, a specialist in Hospital Infrastructure since 2012 - Department of oversight of
construction belonging to the Investment Division of the Ministry of Health in Chile.
• Biomedical engineer, focused on Quality Management, Engineering and Construction Hospital.

Introduction/ Summary 3
This paper aims to create a methodological tool where the technical requirements of
installation and assembly of highly complex medical devices are explained through
tables with technical parameters and installation recommendations.
• Lack of standardized information for the design stage.
• Current rules and projects do not consider the medical and industrial
equipment as key crosscutting elements.
• General idea of the requirements.
CHILEAN PUBLIC
HEALTH AREA

Topics 4
Analysis of what we
have today
Methodology of Work
Requirements Design Implementation Validation Results

Analysis of what we have today ...
• Historical trend of management of infrastructure and technology in hospitals¹ in Latin America.
• Until 2009, 95% of health investments were in existing buildings².
5
Source: 1. “Medical Architectural Program Design for Safe Hospitals”. Bambarén, C. and Alatrista, S. 2008 2. “Investments Public Health Network in Chile 1998-2008”, Andres Bello University. Dr. Ignacio Astorga
Architectural design does not always have a file source containing the list of equipment with its installation requirements and parameters
Usually planning about installation and assembly requirements is not coordinated with the construction´s Gantt chart
Project bids are awarded under incomplete history
National Investment Plan Hospital Projects Period 2014-2018
20 Hospitals built by the end of the
period.
20 Hospitals under
construction by the end of the
period.
20 Hospitals in bidding processes or studies by the
end of the period.

This research is a practical aid to understand... 6
Weaknesses that exist at the national level, in public and private spheres, on the issue of buildings and hospital facilities. Lack of standardized information to make technical decisions about requirements of installation and assembly in the design stage, prior to bids
Find tangible solutions to solve these problems by increasing communication, understanding and knowledge of the time needed to build or reform hospital setting requirements.

Disadvantage v/s Advantages 7
Disadvantage • Poor Specialty Design. • Exchange value notes associated with the equipment. • Increased Deadlines. • Critical Path Modification. • Modification of deadlines in the implementation of
the project. • Lack of coordination with the technical teams of the
technical inspector of the construction site (ITO). • Delayed purchase of equipment. • The purchase programming, critical path modification
based on the time of acquisition. • Lack of human resources and equipment unit. • Market behavior affects shopping programming.
Advantages • Improve design considering the worst case scenario. • Decrease exchange value notes associated to
equipment. • Decrease of deadlines associated with equipment
modifications. • Slight modifications in the critical path. • Optimization the times associated with acquisition
and installation of equipment. • Continuous monitoring of the level of progress at
work, presenting alerts in case of errors in the execution.

Methodology of work
Model to use
Classical model with feedback considering also expert criteria
Data Collection Process
Build a Big Data Base, including data sheets, installation and assembly design criteria in relation to different services.
• Selection of the services to analyze.
• Data collected in order to know and understand the parameters that require such medical equipment.
Preparation of documents
Related to installation requirements.
Definition of Installation criteria.
Checklist for an in field review of hospitals.
8

Requirements
What are highly complex medical equipment?
Equipment that requires supply, anchor and specific infrastructure to be used, considering among others: o Large quantities and/or weight.
o Permanently connected to the facility.
o Attached to the physical infrastructure of the establishment.
9
Pathological anatomy - Dental Clinic - Ophthalmological Clinic - Otolaryngology Clinic - Food Nutrition Unit - Sterilization Unit - DAN (High Level Disinfection) – Dialysis – Pharmacy – Imaging - Clinical laboratory – Laundry - Physical Medicine and Rehabilitation - Hyperbaric Medicine - Surgical Pavilion – Radiotherapy - Milk Dietary Service - Critical Patient Unit - Flat washes and Macerators Services - ER (Resuscitation)
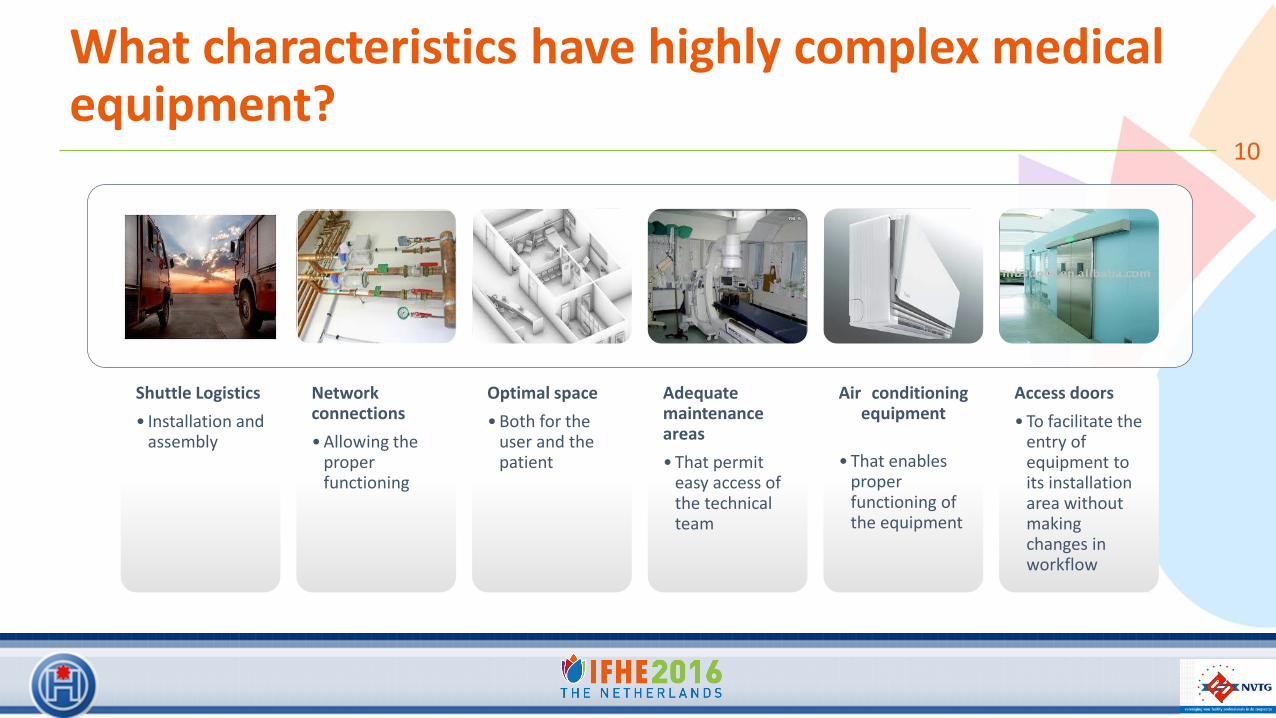
What characteristics have highly complex medical equipment?
10
Shuttle Logistics
• Installation and assembly
Network connections
• Allowing the proper functioning
Optimal space
• Both for the user and the patient
Adequate maintenance areas
• That permit easy access of the technical team
Air conditioning equipment
• That enables proper functioning of the equipment
Access doors
• To facilitate the entry of equipment to its installation area without making changes in workflow
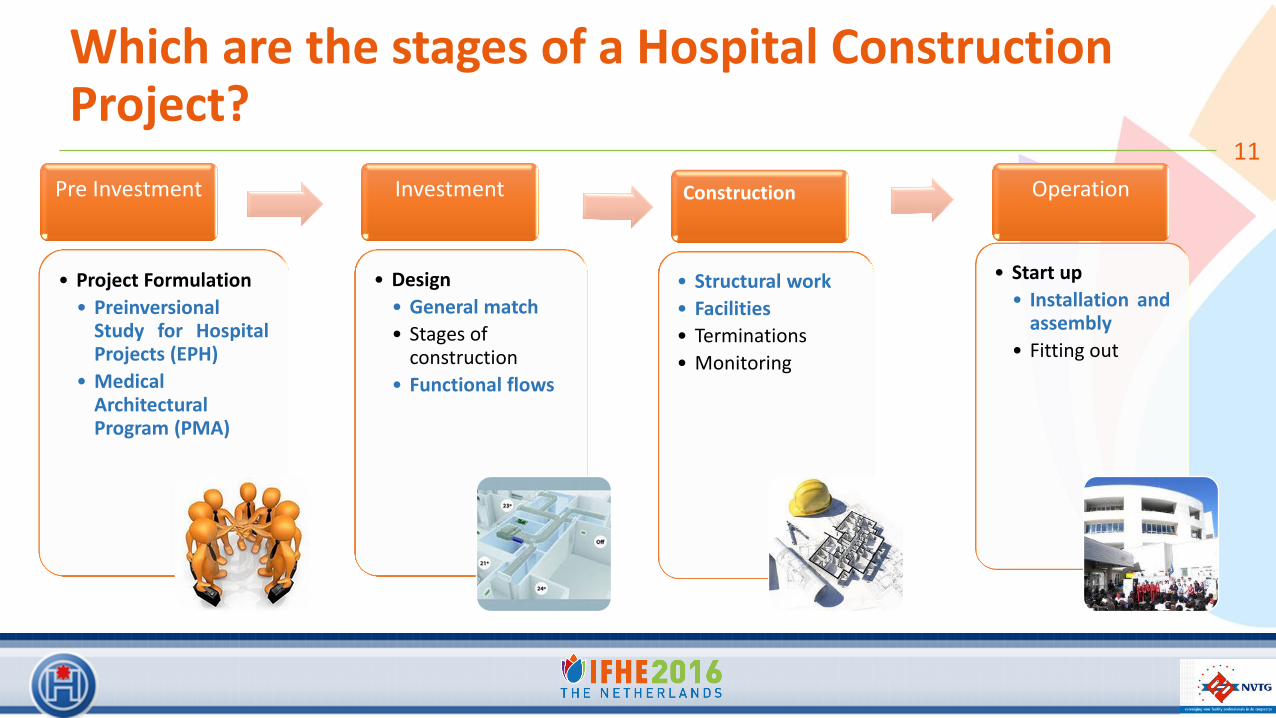
Which are the stages of a Hospital Construction Project?
11
Pre Investment
• Project Formulation
• Preinversional Study for Hospital Projects (EPH)
• Medical Architectural Program (PMA)
Investment
• Design
• General match
• Stages of construction
• Functional flows
Construction
• Structural work
• Facilities
• Terminations
• Monitoring
Operation
• Start up
• Installation and assembly
• Fitting out

Design
• Creating a technical tool considering:
o Architectural plans.
o Main workflows.
o Guidelines about technical requirements for installation and assembly.
o Recommendations and precautions.
o Guidelines or protocol for support of the Hospital Construction Process.
12
Alignment with the ministerial
vision
High standards thanks to the
support of medical
equipment companies
Referential basis for Hospital
Construction Projects
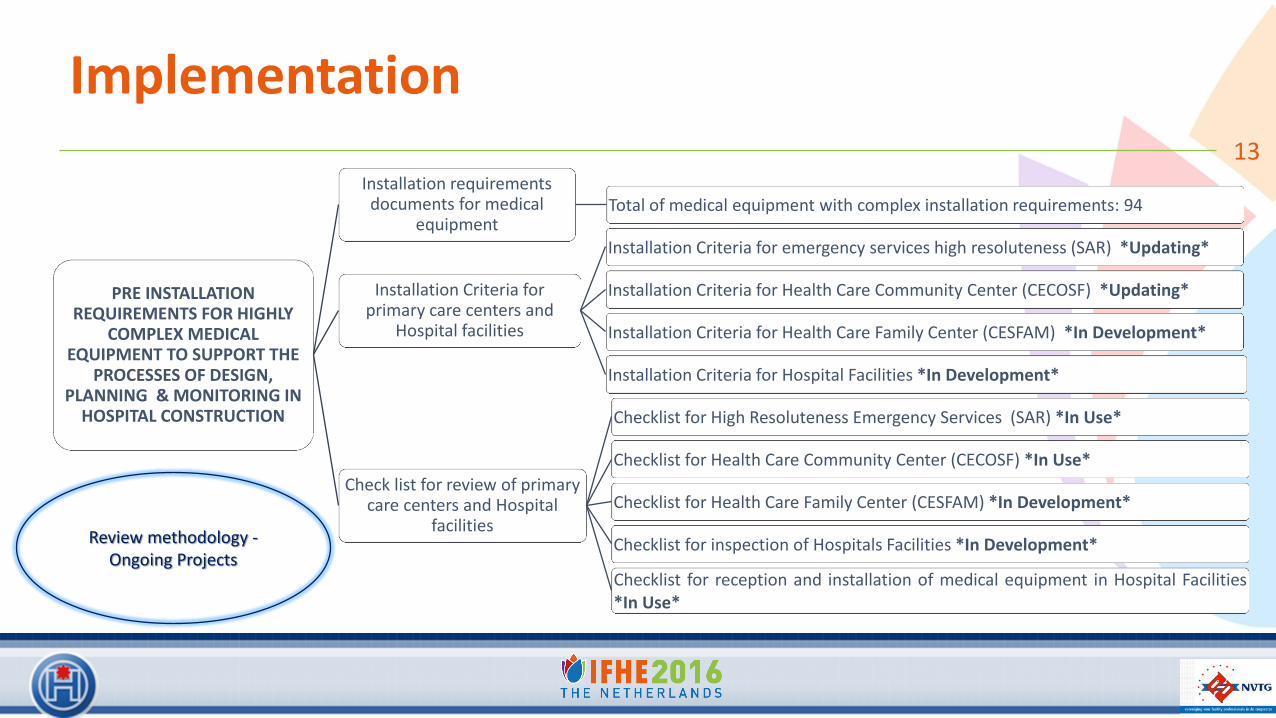
Implementation 13
PRE INSTALLATION REQUIREMENTS FOR HIGHLY
COMPLEX MEDICAL EQUIPMENT TO SUPPORT THE
PROCESSES OF DESIGN, PLANNING & MONITORING IN
HOSPITAL CONSTRUCTION
Installation requirements documents for medical
equipment Total of medical equipment with complex installation requirements: 94
Installation Criteria for primary care centers and
Hospital facilities
Installation Criteria for emergency services high resoluteness (SAR) *Updating*
Installation Criteria for Health Care Community Center (CECOSF) *Updating*
Installation Criteria for Health Care Family Center (CESFAM) *In Development*
Installation Criteria for Hospital Facilities *In Development*
Check list for review of primary care centers and Hospital
facilities
Checklist for High Resoluteness Emergency Services (SAR) *In Use*
Checklist for Health Care Community Center (CECOSF) *In Use*
Checklist for Health Care Family Center (CESFAM) *In Development*
Checklist for inspection of Hospitals Facilities *In Development*
Checklist for reception and installation of medical equipment in Hospital Facilities *In Use*
Review methodology - Ongoing Projects

Validation “Installation criteria for High Resoluteness Emergency Services (SAR) - Summary”
14
San
itar
y
Avoid past or sanitary discharges (sewage, drinking water) in the skies of rooms
If any, incorporate measures for containment and preventing failures
Ele
ctri
city
NCh 4/2003, connect emergency systems
HV
AC
Minimum outside air flow: 5 renovation/hr
Temperature Range: 20-22ºC
Estr
uct
ura
l
Rx BRS: 800-1000 Kg
Rx U Arc type: 324-600 Kg
Rad
iati
on
Always consider shielding the room, referring to this:
The study of ionizing radiation.
Comply with the basic technical standard (NTB).
Decree Nº 3/85 and 133/84 from CCHEN.
SEREMI and CCHEN certifications

Validation “Installation criteria for Health Care Community Center (CECOSF) - Summary”
15
San
itar
y
Avoid past or sanitary discharges (sewage, drinking water) in the skies of rooms, near of Intraoral X-ray and Dental Unit
If any, incorporate measures for containment and preventing failures
Dental unit: water connection (soft or household water); sanitary discharge. From floor, depending on the equipment, the connections may be head, center or foot.
Ele
ctri
city
NCh 4/2003, connect emergency systems
Clin
ical
gas
es
Air compressor, dry air and free of oil (Enable form approved project)
Connections from floor
Estr
uct
ura
l
Equipment load requirements, patients and staff (kg / m2).
In the case of Dental X Ray equipment, define wiring will be done by sky, wall or floor.
Rad
iati
on
Always consider shielding the room, referring to this:
The study of ionizing radiation.
Comply with the basic technical standard (NTB).
Decree Nº 3/85 and 133/84 from CCHEN.
SEREMI and CCHEN certifications.

Validation “Installation criteria for Health Care Family Center (CESFAM) - Summary”
16 St
eri
lizat
ion
Un
it
Distribution must be according to National normative.
It requires soft water and osmosis water for washing desinfectors and steam sterilizer.
Drying pistol requires: compressed air, dry air and free of oil.
It requires in the storage area, controlled temperature to prevent condensation moisture in the sterile package.
Sanitary downloads for Washer disinfectors and steam sterilizer equipment must be in copper material.
De
nta
l Bo
x
Used same criteria that CECOSF Facilities
X R
ay
Used same criteria that SAR facilities

Validation “Installation criteria for the Design Stage in the Hospital Facilities - Summary”
17 • Review of documents, analyze the medical equipment
with the installation requirements.
• Review of regulations associated with clinical services that have equipment with installation requirements.
• Review and compare to architecture blueprints and specialties, checking each clinical service that has equipment with installation requirement.
• Visit the construction in the execution stage.

Results 18
020406080
100120140160180
State of the reception and installation of medical equipment in Hospital Facilities
Installation of Equipment at WorkHospital - Remarks 17/06/2014
Installation of Equipment at WorkHospital - Remarks 21/10/2014
Documents of installation requirements for Medical Equipment
Checklist for Health Care Community Center (CECOSF)
Medical equipment parameters with complex installation
Sanitary Electrical Supply HVAC Shield
Dimensions Vahos evacuation Clinical Gases Space operation
Sound insulation (Noise)
Size of room Access door Equipment
Weight
Checklist for reception and installation of medical equipment in Hospital Facilities

Results
• The first year (2012) we only analyzed 6 clinical services 19
Total areas
analyzed 46%
Remaining areas 54%
High Complexity Hospital
Total areas
analyzed 13%
Remaining areas 87%
Medium Complexity Hospital
Structural work
Installations
Terminations
3 5
9
Hospitales
Historical Hospital Construction Projects - Increasing term
execution of the work
> 1 año
7 -11 meses
< 7 meses
> 1 Year
7 – 11 Month
< 7 Month
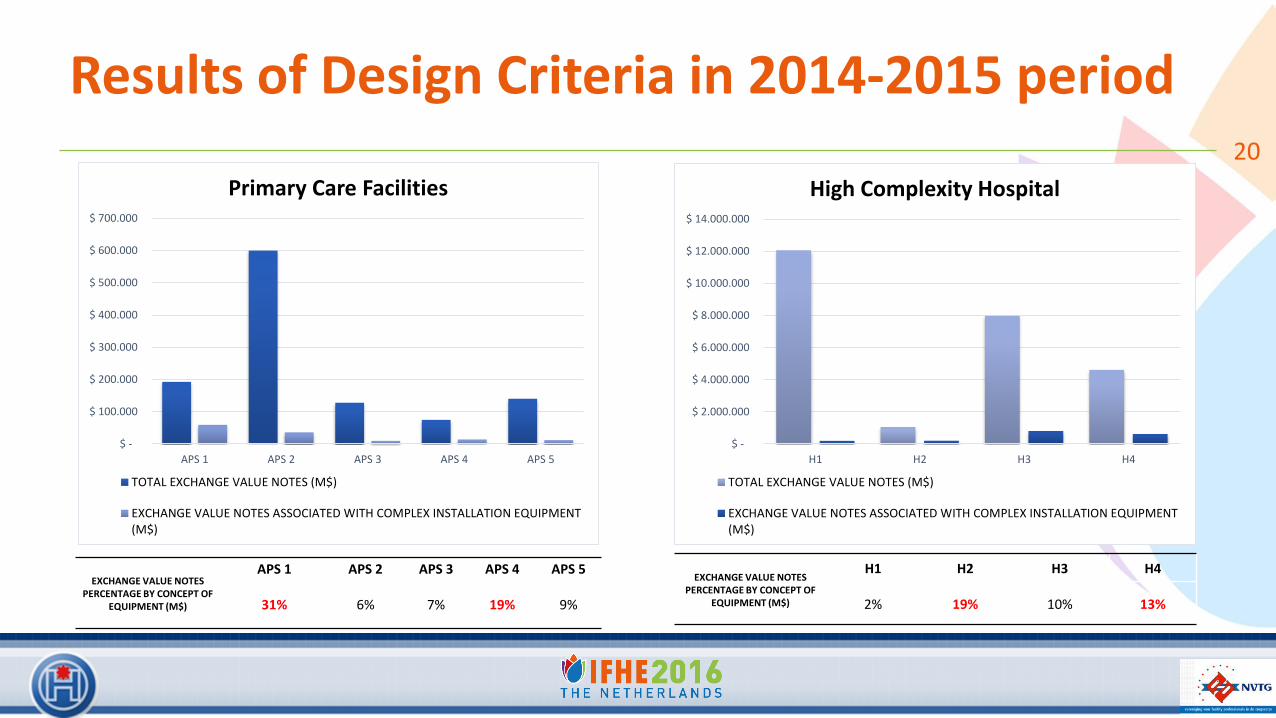
Results of Design Criteria in 2014-2015 period 20
$ -
$ 100.000
$ 200.000
$ 300.000
$ 400.000
$ 500.000
$ 600.000
$ 700.000
APS 1 APS 2 APS 3 APS 4 APS 5
Primary Care Facilities
TOTAL EXCHANGE VALUE NOTES (M$)
EXCHANGE VALUE NOTES ASSOCIATED WITH COMPLEX INSTALLATION EQUIPMENT(M$)
$ -
$ 2.000.000
$ 4.000.000
$ 6.000.000
$ 8.000.000
$ 10.000.000
$ 12.000.000
$ 14.000.000
H1 H2 H3 H4
High Complexity Hospital
TOTAL EXCHANGE VALUE NOTES (M$)
EXCHANGE VALUE NOTES ASSOCIATED WITH COMPLEX INSTALLATION EQUIPMENT(M$)
EXCHANGE VALUE NOTES PERCENTAGE BY CONCEPT OF
EQUIPMENT (M$)
APS 1 APS 2 APS 3 APS 4 APS 5
31% 6% 7% 19% 9%
EXCHANGE VALUE NOTES PERCENTAGE BY CONCEPT OF
EQUIPMENT (M$)
H1 H2 H3 H4
2% 19% 10% 13%

Results of Design Criteria
Among the commonly evidenced errors, we find the following:
• Errors in the installation of dental chairs, connections are not located on the defined area.
• Equipment material working at high temperatures, such as milk dietary services, sterilization, laundry and central feeding, made with PVC material.
• Vapor evacuation ducts for dryers, trouser or roller washers and washer desinfectors, are not considered in the project.
• The logistics of the implementation of anchoring rails and support slab imaging equipment doesn’t consider the details involved from the TDF connection to the control room.
• Hood enclosure gas for dialysis filters cleaning systems, among others.
21

Conclusions
• It is evident that there are issues that affect the design, therefore increasing the costs and time of execution.
• It can be seen that there is little knowledge of requirements when designing a hospital and, as a result of such a lack of knowledge, there is an increase of costs and work deadlines.
• This tool is meant to be a support program for architects, construction engineers, specialty designers and any professional who needs to modify infrastructure that includes highly complex equipment, or constructing a new area.
22

Summary of contributions ...
• As can be seen, the creation of this tool is useful in the following aspects:
o Allows project managers to understand the importance of pre-installation planning
and requirements of highly complex medical equipment.
o It helps to remind and consider the planning and execution of work space logistics
for the transport and fixing of equipment.
o In the case of an architectural redesign, it allows us to know the limitations and
possibilities for certain equipment installation.
23

My message ... Passion, Commitment and Vocation
• In my opinion, the infrastructure of a hospital should last at least 20 to 25 years, this of course, considers a
periodical equipment replacement program which depends on the lifecycle of each unit and its location, as well as
the provider’s recommendation.
• It is our responsibility to provide a work frame that contains all the necessary infrastructure and equipment for an
optimal performance and to create a better environment for the patients and staff who live and work in a Hospital
on a daily basis.
• We need to open our minds and put ourselves in the place of the other. Analyzing projects as if we were nurses,
doctors, maintenance and administrative staff, among others. Think about the details and consider all possible
domestic issues as elements that can cause problems in the project implementation.
24
References ...
• Informe Final consolidado Servicios de Salud, Marzo del 2009. Contraloría General de la República. División Auditoría Administrativa, Área Salud, Agricultura y Medio Ambiente. (DAA N° 62/2009)
• Bambarén, Celso; Alatrista, Socorro. “Programa Médico Arquitectónico para el Diseño de Hospitales Seguros”. Lima, Perú. 1° Edición, Diciembre de 2008. ISBN: 978-9972-2815-3-2.
• Dr. Ignacio Astorga Jorquera. Inversiones de la Red Pública de Salud En Chile PERIODO 1998-2008, Enero 2009. Escrito para el Instituto de políticas públicas y gestión salud y futuro, Universidad Andrés Bello. Resolución WHA60.29 de la Organización Mundial de la Salud (OMS) sobre Tecnologías sanitarias, 2007.
• Secretaría de Salud, Programa de Acción Específica. 1A edición, México 2008.
• Fiorentini, Domingo (Arq. y Dr.), Fiorentini Arquitetura de Hospitais. “Cuándo y Cómo Recuperar o Proyectar”, IV Congreso Infraestructura Hospitalaria. 2010.
• Ministerio de Salud, Gobierno de Chile. Guía Metodológica para estudios de Preinversión Hospitalaria. Chile, 2001.
• Monza, Luciano (Arq). “Futuro de los edificios para la salud: Tendencias”, IV Congreso Infraestructura Hospitalaria. 2010.
• Organización Panamericana de la Salud, Fundamentos para la mitigación de desastres en establecimientos de salud. Área de Preparativos para Situaciones de Emergencia y Socorro en Casos de Desastre, Washington, D.C., 2004.
• Rubén Boroschek Krauskopf y Rodrigo Retamales Saavedra. Guía para la reducción de la vulnerabilidad en el diseño de nuevos establecimientos de salud. Centro Colaborador OPS/OMS de Mitigación de Desastres en Establecimientos de Salud Universidad de Chile. Washington D.C., Enero 2004.
25

Presented at 24th IFHE congress at 18-19 April 2016 in The Hague, The Netherlands
IFHE - International Federation of Hospital Engineering NVTG – Dutch Association for Technical Facility Professionals in the Healthcare Sector
PREINSTALLATION REQUIREMENTS FOR HIGHLY COMPLEX MEDICAL EQUIPMENT TO SUPPORT THE PROCESSES OF DESIGN,
PLANNING & MONITORING IN HOSPITAL CONSTRUCTION
Carolina Navarrete Guarda, Biomedical Engineer Ministry of Health, Chile
Thank you for your attention…
Email: [email protected]


















