Prehabilitation for people awaiting bypass surgery:
21
Prehabilitation for people awaiting bypass surgery: A randomised controlled trial Gill Furze CARE AND EDUCATION RESEARCH GROUP
-
Upload
cardiacinfo -
Category
Documents
-
view
164 -
download
3
Transcript of Prehabilitation for people awaiting bypass surgery:
Prehabilitation for people awaiting bypass surgery:
A randomised controlled trial
Gill Furze
CARE AND EDUCATION RESEARCH GROUP

Prehab: what is it?
• Often found in the sports coaching field: “Prehab not rehab” – prevention of injury by identifying potential problems before they occur.
• In health care, prehabilitation is concerned with the prevention of functional decline, particularly prior to surgery or other inpatient stay.
• Term used in the USA to mean primary prevention for heart disease.

Why is it needed?• Patients have reported that waiting for heart surgery
is more disturbing than their chest pain.1
• Being on the waiting list can lead to greater disablement.
• Even with the proposed changes, time from seeing a GP to receiving bypass will still be up to 18 weeks.
• Study in Montreal: people who waited longer than 97 days became more physically and socially limited, compared to people with shorter waits.2
1. Bengtson et al. Heart 1996;75(3):257-260 2. Sampalis et al. Canadian Medical Association Journal 2001;165:429-33

Why are they more limited?
• Place life on hold
• Postpone stressful or exciting events until “after the op”
• Adopt a profoundly sedentary lifestyle
• Normal routines are lost
RESULT:
• Physical and mental decline

Previous studies of prehab
• Hospital-based exercise programme: reduced inpatient stay, post-op complications, time in ICU, and improved QoL.1
• Nurse-led education programme reduced smoking, BP and BMI.2
• Both of the above studies were compared to “no-treatment” control
1. Arthur et al. Annals of Internal Medicine 2000;133:253-62.
2. McHugh et al. Heart 2001;86:317-323

Our proposal• Develop a cognitive-behavioural, home-based,
preparation for bypass surgery programme, facilitated by a health professional.
• Include: exercise, risk factor management, psychological preparation for surgery (including education to dispel cardiac misconceptions).
• Test this in a randomised controlled trial
• Offer home-based, post-surgery exercise programme (Papworth Outreach) to all patients.
• Grant funding awarded by BHF

Development of the programme 1Information re:
– patient experience prior to surgery, – emotional impact of diagnosis and wait, – information needs, – family / carer needs
Derived from three sources:1. FAQs about CABS collected by patient support group2. (Anonymised) transcripts of focus groups about
patient / carer experience of CABS from Nottingham CR team
3. 12 semi-structured patient interviews post CABS

Development of the programme 2• Drafts of written materials reviewed by patient
interviewees
• Penultimate draft also reviewed by expert reference group consisting of:
–8 cardiac rehabilitation nurse specialists / managers, –4 cardiac surgeons, –3 cardiothoracic intensive care nurse specialists, –2 physiotherapists, –2 consultant cardiologists –1 each of the following: clinical psychologist, a researcher into diet in heart disease, a director of public health, a director of clinical governance and a CHD Collaborative project manager responsible for revascularisation
• The programme was piloted with 6 patients
The HeartOp Plan ProgrammeTwo patient-held booklets:
– Section 1 (practical ways to get ready for surgery):myths, questions and worries, staying active – getting fit, coping with stress
– Section 2 (information about):your heart and risk factors, the operation and after,other sources of information
Diary to record progress with goals
Relaxation programme on audiotape / CD
TheThe HeartOp Plan
HeartOp Plan
SECTION ONE
SECTION ONEOr how to get ready for your
Or how to get ready for your heart operation –
heart operation – and for the rest of your life
and for the rest of your life

Randomised controlled trial• Intervention: the HeartOp Plan Programme.
• Control programme: Nurse education programme explaining operation and targeting risk factors, using BHF booklets to provide written information.
• Remote randomisation by staff not involved in study
• Intervention delivered by nurse not otherwise involved in data collection
• Data entry blind to group
• Analysed by statistician not otherwise involved in study, blind to group

Interventions follow-up
Both interventions:• introduced to patients in 45-60 minute interview in
outpatients
• by cardiothoracic nurse who had undergone Angina Plan training,
• with phone follow up at weeks 1,3,6 and then monthly until operation

EndpointsPost-intervention (~8 wks) and post surgery (6,12, 26 wks)
Primary Endpoints1. Anxiety (State-Trait Anxiety Inventory)2. Smoking3. Obesity (BMI)4. Length of hospital stay
Secondary Endpoints1. Depression (Cardiac Depression Scale)2. Physical functioning (CLASP Mobility and Step Test)3. Misconceptions (Cardiac Beliefs Questionnaire) 4. Health Status (CLASP subscales)5. Pain Report (Visual Analogue Scale)

Participants Suggested sample size: 300 patientsInclusion:• All patients on the non-urgent waiting list for first time
CABS. Exclusion:• Exercise induced arrhythmias • Unstable angina • Canadian Angina Class 4 / NYHA class 4 • Life threatening co-morbidities.
• Concurrent participation in other research relating to coronary artery bypass grafting
• Previous experience of the Angina Plan• Recent MI awaiting cardiac rehabilitation• Operation date less than 6 weeks from entry to waiting list

Recruitment and follow-up Waiting list 604
Met inc / exc criteria: 370 – letter from consultant
HeartOp Plan Control Total
Not operated on 1- referral1- withdrawn surgeon1- withdrawn self
3 - referral 6 (3%)
Consent to participate 204
104 randomised to HeartOp Plan
100 randomised to control
84 (81%)Complete to 6 months
86 (86%) Complete to 6 months
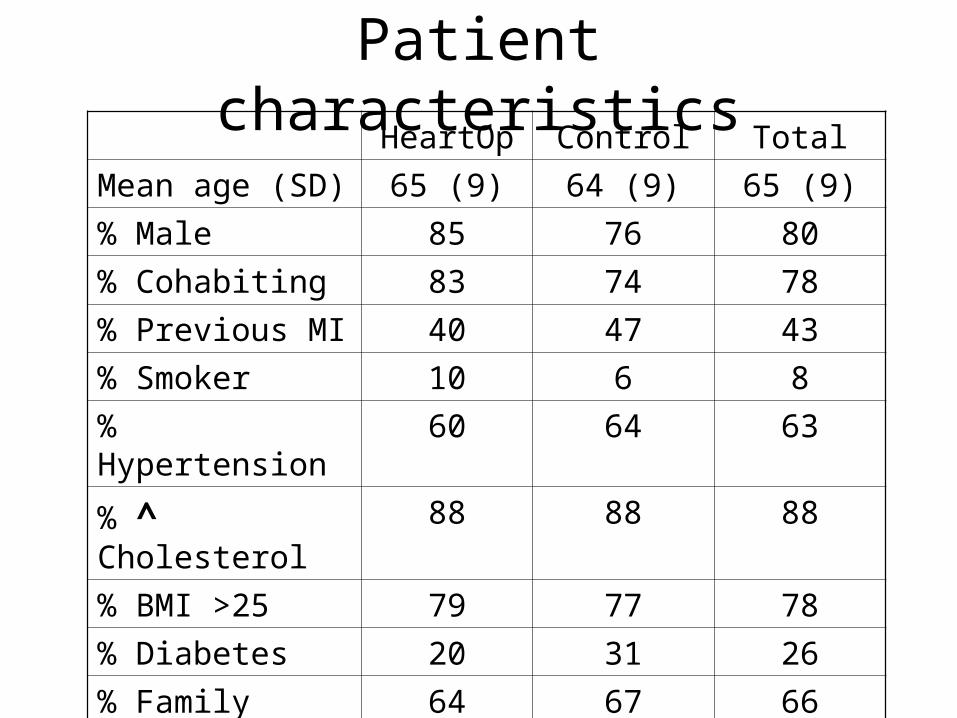
Patient characteristicsHeartOp Control Total
Mean age (SD) 65 (9) 64 (9) 65 (9)
% Male 85 76 80
% Cohabiting 83 74 78
% Previous MI 40 47 43
% Smoker 10 6 8
% Hypertension 60 64 63
% ^ Cholesterol 88 88 88
% BMI >25 79 77 78
% Diabetes 20 31 26
% Family history 64 67 66

Results – Primary EndpointsIntention-to-treat analysis using ANCOVA controlling
for surgeon and baseline variables: NYHA, CAC, BMI, systolic BP, smoking status, step-test time and T1 dependent variable.
• Primary endpoints: – (Anxiety, obesity, length of hospital stay) – No significant difference between the two
programmes at any of the follow-up time points.
• Smoking - too few to make a comparison.

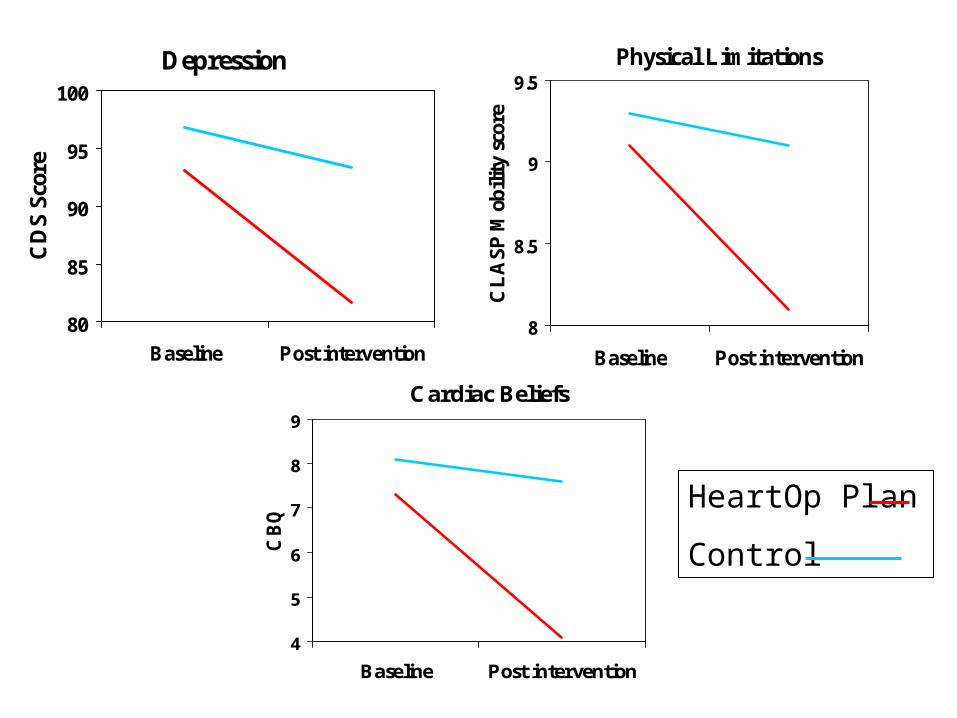
Results – Secondary endpoints
Post Intervention(pre-op)
Mean diff
95% CI Sig
Depression 7.79 2.04 - 13.54 .008
Physical Limitations 0.82 0.34 - 1.30 .001
Cardiac beliefs 2.56 1.64 - 3.48 <.001
Health Status Not significant
Post Operative
All variables Not significant except CBQ
Depression
80
85
90
95
100
Baseline Post intervention
CD
S Sc
ore
Physical Limitations
8
8.5
9
9.5
Baseline Post intervention
CL
ASP
Mob
ility
sco
re
Cardiac Beliefs
4
5
6
7
8
9
Baseline Post intervention
CB
Q
HeartOp Plan
Control

Risk factors over time: Total sampleBMI
28
28.5
29
29.5
T1 Preop T3
BMI
Cholesterol
3.5
4
4.5
5
T1 T3
Cho
lest
erol
Step-test
0.35
0.55
0.75
0.95
T1 T3 T4
Step
test
Anxiety
29
34
39
T1 T2 T3 T4 T5
Anx
iety
operation

Conclusion
• Use of the HeartOp Plan was significantly more successful at reducing depression, physical limitation and cardiac misconceptions preoperatively than a nurse education programme, but had no effect on risk factors, anxiety or length of stay.

AcknowledgementsThis study would not have been successful without the help of:
• Karen Irvine – Intervention facilitator
• Jenny Rumsby – Cardiothoracic nurse practitioner
• Outreach programme staff: Nicola Beaumont, Margaret Argent, Jo Wakefield, Heidi Teynan
• Carol Hargreaves - CHD Collaborative project manager for revascularisation
• Allan Fussey –Patient Choice Programme manager
• The staff of CTU Castle Hill Hospital, East Yorks
• The patients
• The BHF for grant funding the study