
Pregnant & Breastfeeding Women CAN-ADAPTT Guideline Webinar Series March 15, 2011 Guideline Section...
28
Pregnant & Breastfeeding Women CAN-ADAPTT Guideline Webinar Series March 15, 2011 Guideline Section Lead: Alice Ordean, MD, CCFP, MHSc
-
Upload
grace-hyden -
Category
Documents
-
view
219 -
download
0
Transcript of Pregnant & Breastfeeding Women CAN-ADAPTT Guideline Webinar Series March 15, 2011 Guideline Section...
Pregnant & Breastfeeding Women
CAN-ADAPTT Guideline Webinar Series March 15, 2011
Guideline Section Lead: Alice Ordean, MD, CCFP, MHSc
Bio and Disclosures
Alice Ordean is an Assistant Professor in the Department of Family & Community Medicine at the University of Toronto and Medical Director of the Toronto Centre for Substance Use in Pregnancy (T-CUP).
No disclosures.

Guideline Development Group
Peter Selby, MBBS, CCFP, MHSc, FASAM; Gerry Brosky, MD, MSc, CCFP; Charl Els, MBChB, FCPsych, MMed Psych (cum
laude), Cert. ASAM, MRO; Rosa Dragonetti, MSc; Sheila Cote-Meek, BScN, MBA, PhD; Jennifer O’Loughlin, PhD; Paul McDonald, PhD, FRSPH; Alice Ordean, MD, CCFP, MHSc; Robert Reid, PhD, MBA

CAN-ADAPTT
Guideline development, dissemination and engagement project
Integrates practice, policy and research in a collaborative smoking cessation network
Goal: To inform the development of a Pan-Canadian clinical practice guideline (CPG) for smoking cessation
Funded by the Drugs and Tobacco Initiative, Health Canada
Dissemination
& Engagement
National Network
Practice-informedResearch Agenda
Knowledge Translation
PRACTICERESEARCH Clinical Practice Guideline

Appraisal: AGREE4 independent reviewers (practicing physicians)All formally trained on AGREE instrument
HIGH QUALITY CLINICAL PRACTICE GUIDELINESU.S. Department of Health and Human Services Public Health Service: Treating Tobacco Use and Dependence (2008 Update),
New Zealand Smoking Cessation Guidelines (August 2007), Registered Nurses Association of Ontario: Integrating Smoking Cessation into Daily Nursing Practice (March 2007),
Registered Nurses Association of Ontario: Integrating Smoking Cessation into Daily Nursing Practice (October 2003), Institute for Clinical Systems Improvement. Tobacco use prevention and cessation for infants, children and adolescents (June 2004),
Institute for Clinical Systems Improvement Tobacco use prevention and cessation for adults and mature adolescents (June 2004).
The CAN-ADAPTT program engaged the Guidelines Advisory
Committee
COMPREHENSIVE LITERATURE SEARCH 87 Guidelines Found
87 Guidelines Found
Highest scoring CPG’s
included
6 Guidelines Included6 Guidelines Included
Appraisal: AGREE Plus8 Additional questions developed by CAN-ADAPTT to understand the applicability of the recommendations in the Canadian context
Initial LITERATURE REVIEW for existing Clinical Practice Guidelines
5 Guidelines Included
5 Guidelines Included
Version1.0
February 2009
Version1.0
February 2009
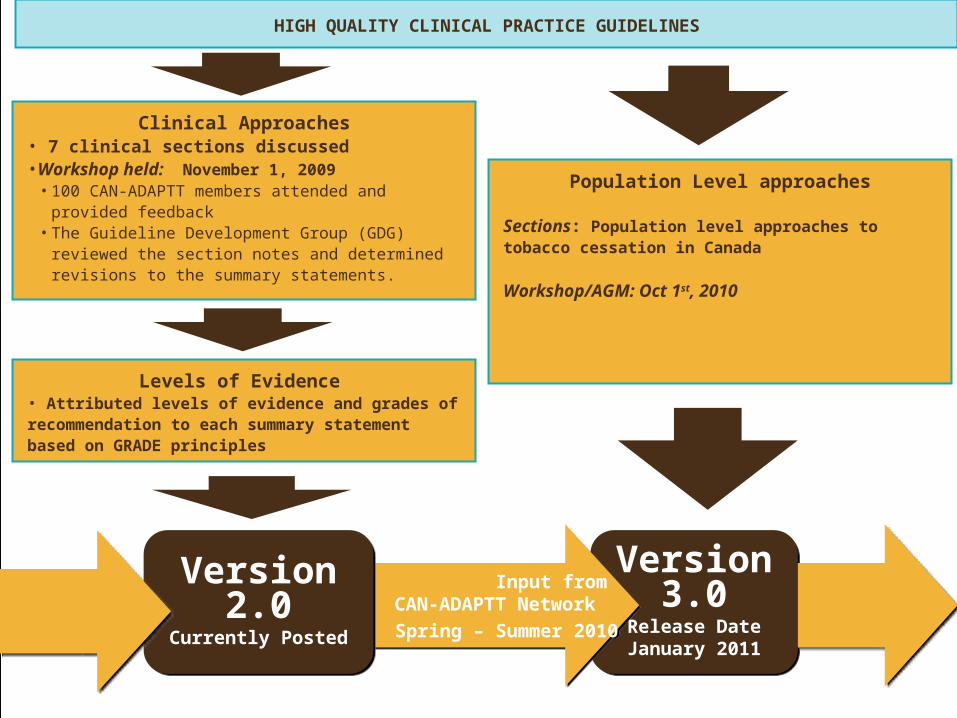
HIGH QUALITY CLINICAL PRACTICE GUIDELINES
Clinical Approaches• 7 clinical sections discussed•Workshop held: November 1, 2009
• 100 CAN-ADAPTT members attended and provided feedback
• The Guideline Development Group (GDG) reviewed the section notes and determined revisions to the summary statements.
Population Level approaches
Sections: Population level approaches to tobacco cessation in Canada
Workshop/AGM: Oct 1st, 2010
Version3.0
Release DateJanuary 2011
Version3.0
Release DateJanuary 2011
Input from CAN-ADAPTT Network
Spring – Summer 2010
Input from CAN-ADAPTT Network
Spring – Summer 2010
Version2.0
Currently Posted
Version2.0
Currently PostedNetwork input Network input Network Input Network Input
Levels of Evidence • Attributed levels of evidence and grades of recommendation to each summary statement based on GRADE principles
Background/Overview of Evidence
Existing evidence included CPGs from Canada, USA, New Zealand, France and UK
Literature review in this specific subpopulation has a limited number of high quality trials with contradictory results especially in area of pharmacotherapeutic options
Background/Overview of Evidence
U.S. Department of Health and Human Services Public Health Service (2008)
Because of the serious risks of smoking to the pregnant smoker and the fetus, whenever possible pregnant smokers should be offered person-to-person psychosocial interventions that exceed minimal advice to quit. (Strength of Evidence = A)
Although abstinence early in pregnancy will produce the greatest benefits to the fetus and expectant mother, quitting at any point in pregnancy can yield benefits. Therefore, clinicians should offer effective tobacco dependence interventions to pregnant smokers at the first prenatal visit as well as throughout the course of pregnancy. (Strength of Evidence = B)

Background/Overview of Evidence
New Zealand Ministry of Health (2007) Offer all pregnant and breastfeeding women who smoke
multi-session behavioural smoking cessation interventions from a specialist/dedicated cessation service. (Grade=A)
All health care workers should briefly advise pregnant and breastfeeding women who smoke to stop smoking. (Grade = A)
NRT can be used in pregnancy and during breastfeeding following a risk-benefit assessment. If NRT is used, oral NRT products (for example, gum, inhalers, microtabs and lozenges) are preferable to nicotine patches. (Grade=C)
Registered Nurses Association of Ontario (2007) Nurses implement, wherever possible, intensive intervention
with women who are pregnant and postpartum. (Strength of Evidence = A)

Gap in Practice and Barriers
Challenges in identification due to stigma associated with smoking during pregnancy
Pregnant & breastfeeding women frequently receive inaccurate advice from health care practitioners regarding the effects of smoking during pregnancy and the safety of smoking cessation interventions (e.g. NRT, bupropion)
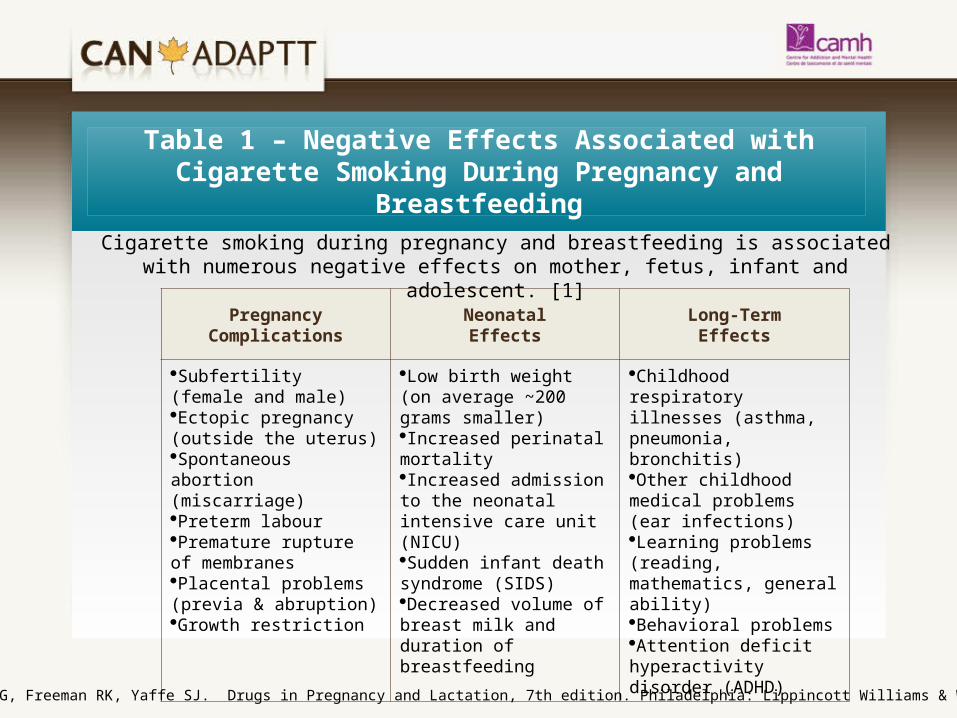
Table 1 – Negative Effects Associated with Cigarette Smoking During Pregnancy and Breastfeeding
Pregnancy ComplicationsNeonatalEffects
Long-TermEffects
Subfertility (female and male)Ectopic pregnancy (outside the uterus)Spontaneous abortion (miscarriage)Preterm labourPremature rupture of membranesPlacental problems (previa & abruption) Growth restriction
Low birth weight (on average ~200 grams smaller)Increased perinatal mortalityIncreased admission to the neonatal intensive care unit (NICU)Sudden infant death syndrome (SIDS) Decreased volume of breast milk and duration of breastfeeding
Childhood respiratory illnesses (asthma, pneumonia, bronchitis)Other childhood medical problems (ear infections)Learning problems (reading, mathematics, general ability)Behavioral problemsAttention deficit hyperactivity disorder (ADHD)
Cigarette smoking during pregnancy and breastfeeding is associated with numerous negative effects on mother, fetus, infant and adolescent. [1]
[1] Briggs GG, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation, 7th edition. Philadelphia: Lippincott Williams & Wilkins, 2005
Summary Statement #1
Smoking cessation should be encouraged forall pregnant, breastfeeding and postpartumwomen.
GRADE: 1A

Clinical Considerations
Smoking cessation interventions should be considered for the full spectrum of care from preconception visit to 1 year postpartum.
Smoking cessation counselling and care of pregnant smokers may be conducted by physicians, allied healthcare professionals (e.g. social worker, pharmacist, community health representatives), midwives, doulas, prenatal advisors, postpartum supports, family home visitors, and others.
Summary Statement #2
During pregnancy and breastfeeding,
counselling is recommended as first line of
treatment for smoking cessationGRADE: 1A
Summary Statement #3
If counselling is found ineffective, intermittentdosing nicotine replacement therapies (such as lozenges, gum) are preferred overcontinuous dosing of the patch after a risk-benefit analysis
GRADE: 1C
Clinical Considerations
There is limited evidence on harms associated with the use of nicotine replacement therapy (NRT) during pregnancy. Until further information is available, the risks and benefits of smoking versus the use of NRT during pregnancy must be considered when counselling about smoking cessation options
Clinical Considerations
NRT can be considered as a second line option for individuals who cannot quit after counselling interventions.
There is some evidence from RCTs that NRT may be efficacious in pregnancy in terms of decreasing tobacco use and improving pregnancy outcomes. No safety concerns identified in these trials. Therefore, benefits of NRT seems to outweigh potential risks; therefore, NRT should be considered when counselling has been ineffective.
• Depression during pregnancy is a common occurrence and the use of Zyban (bupropion) may be appropriate to treat both smoking and depression. There is limited evidence on the effectiveness of bupropion for smoking cessation during pregnancy. In addition, there is no evidence of harm related to the use of bupropion during pregnancy and therefore, it may be considered for use as an alternative to NRT for a subpopulation of pregnant smokers.
Clinical Considerations

Summary Statement #4
Partners, friends and family members should
also be offered smoking cessation
Interventions.GRADE: 2B

Clinical Considerations
Despite preliminary evidence that continued smoking and relapse are more likely among pregnant women who have a smoking partner, there is limited data regarding the benefits of partner involvement in smoking cessation interventions for pregnant smokers. In non-pregnant populations, interventions to increase support did not find increased quitting rates.
Summary Statement #5
A smoke-free home environment should be
encouraged for pregnant and breastfeeding women
to avoid exposure to second-hand smokeGRADE: 1B
• Evidence from a recent systematic review and meta-analysis demonstrated negative perinatal outcomes (e.g. trend towards lower birth weight, smaller head circumference and congenital anomalies) associated with second-hand smoke exposure. Therefore, pregnant and breastfeeding women should avoid this environmental risk.
Clinical Considerations

Research Gaps
Relationship between smoking and infertility remains uncertain
Lack of information regarding use of pharmacological agents such as Bupropion and Varenicline as a smoking cessation aid – need more research on the effectiveness and safety
Need more evidence of risk/benefit analysis of various smoking cessation aids

Research Gaps
Role of partners, family in smoking cessation interventions needs to be defined
Knowledge gaps of health care providers needs to be addressed
Have additional feedback?
1. Join the network
2. Review the current version of the guideline
3. Provide your feedback online• Clinical considerations; tools/resources
For more information
CAN-ADAPTT
Centre for Addiction and Mental Health
175 College St.
Toronto, ON M5T 1P7
T: 416-535-8501 ext. 7427
www.can-adaptt.net
Note: These presentation slides may be used or reproduced for educational purposes only. Please acknowledge authorship of this content to CAN-ADAPTT and CAMH.

Webinar Discussion: Suggested Resources
Medications and Mothers’ Milk by Dr. Thomas Hale (2010)
Drugs in Pregnancy and Lactation by GG Briggs, RK Freeman and SJ Yaffe (2009)
STARSS (Start Thinking About Reducing Second-hand Smoke) http:aware.on.ca/starss
TEACH course “Helping Pregnant Women Quit Smoking: A Woman-Centred Approach”
www.teachproject.ca/courses


















