
Pregnancy & The Liver - eventospr.com.br · Hyperemesis Gravidarum ... Clinical Presentation...
44
Pregnancy & The Liver Michael A. Heneghan MD, MMedSc, FRCPI. Institute of Liver Studies, King’s College Hospital, London.
Transcript of Pregnancy & The Liver - eventospr.com.br · Hyperemesis Gravidarum ... Clinical Presentation...
Pregnancy & The Liver
Michael A. Heneghan MD, MMedSc, FRCPI.
Institute of Liver Studies,
King’s College Hospital, London.
Normal Pregnancy
Palmar erythema
Spider naevi (60%)
Increased blood volume and cardiac ouput
Small oesophageal varices present in up to 50%
Compression of IVC and azygous flow
Decreased gallbladder motility
lithogenicity of bile ( cholesterol synthesis)
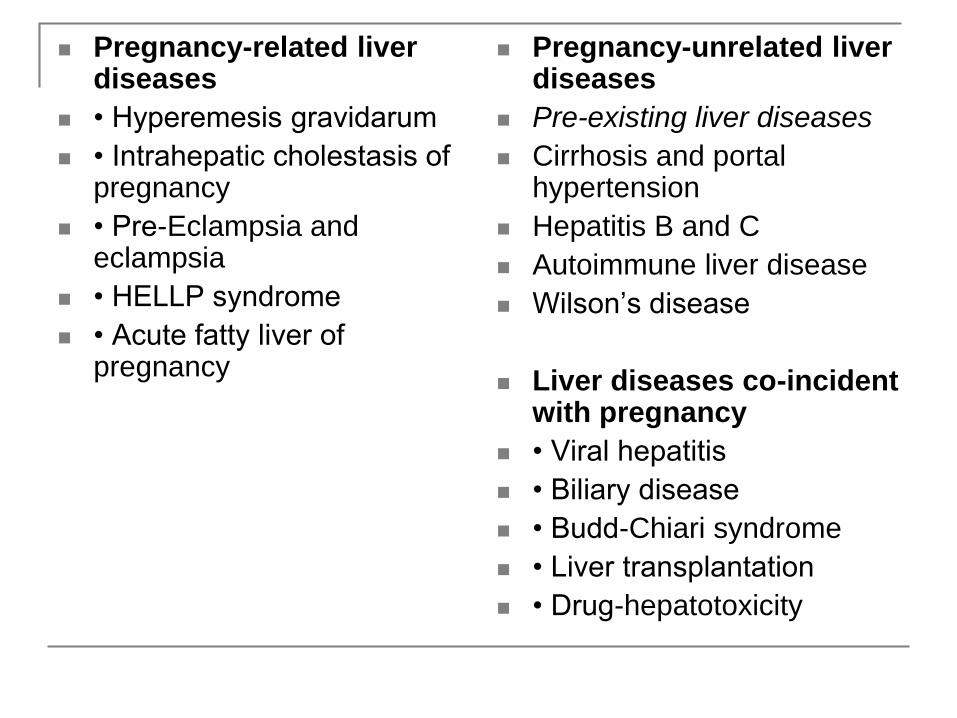
Pregnancy-related liver diseases
• Hyperemesis gravidarum
• Intrahepatic cholestasis of pregnancy
• Pre-Eclampsia and eclampsia
• HELLP syndrome
• Acute fatty liver of pregnancy
Pregnancy-unrelated liver diseases
Pre-existing liver diseases
Cirrhosis and portal hypertension
Hepatitis B and C
Autoimmune liver disease
Wilson’s disease
Liver diseases co-incident with pregnancy
• Viral hepatitis
• Biliary disease
• Budd-Chiari syndrome
• Liver transplantation
• Drug-hepatotoxicity
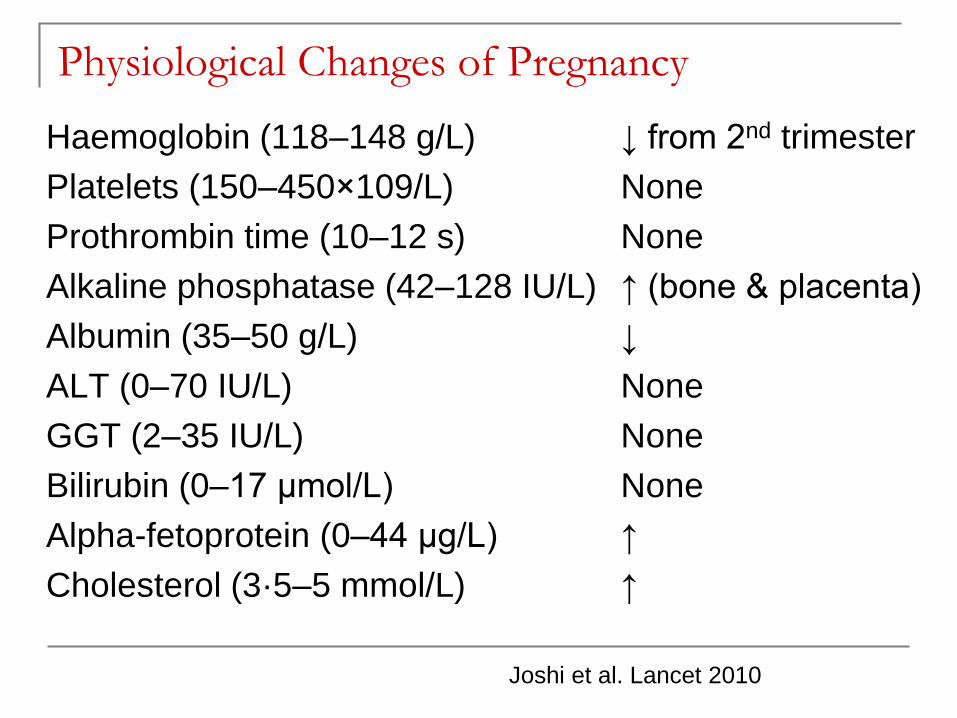
Physiological Changes of Pregnancy
Haemoglobin (118–148 g/L) ↓ from 2nd trimester
Platelets (150–450×109/L) None
Prothrombin time (10–12 s) None
Alkaline phosphatase (42–128 IU/L) ↑ (bone & placenta)
Albumin (35–50 g/L) ↓
ALT (0–70 IU/L) None
GGT (2–35 IU/L) None
Bilirubin (0–17 μmol/L) None
Alpha-fetoprotein (0–44 μg/L) ↑
Cholesterol (3·5–5 mmol/L) ↑
Joshi et al. Lancet 2010

Diagnoses in patients with abnormal LFTs
in Pregnancy
34%
15%
11%
2%
0%
5%
25%
8%
Pre-eclam
HELLP
OCP
AFLP
Infarct
Hyperem
Sepsis
Biliary
Ch’ng et al. Gut 2002
4377 Patients
15 months
142 with abnormal LFTs
206 possible diagnoses
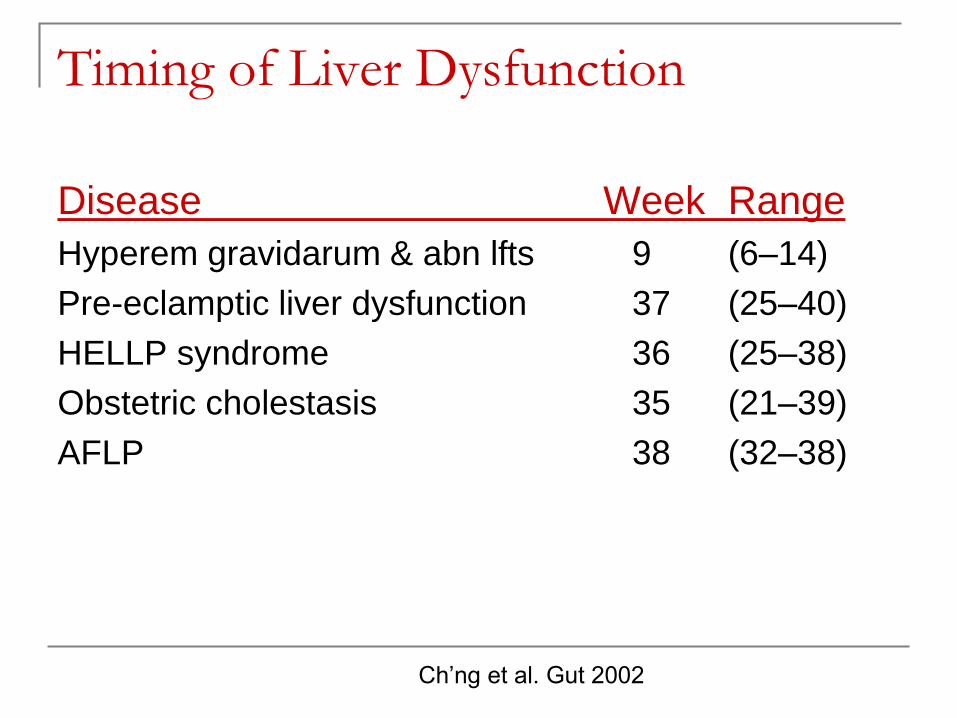
Timing of Liver Dysfunction
Disease Week Range
Hyperem gravidarum & abn lfts 9 (6–14)
Pre-eclamptic liver dysfunction 37 (25–40)
HELLP syndrome 36 (25–38)
Obstetric cholestasis 35 (21–39)
AFLP 38 (32–38)
Ch’ng et al. Gut 2002
Hyperemesis Gravidarum
Protracted vomiting resulting in
dehydration
ketosis
weight loss (>5% body weight)
Excessive salivation
Elevation in AST/ALT IN 50%
Rarely > 200 iu/l
Bilirubin up to 4 x normal
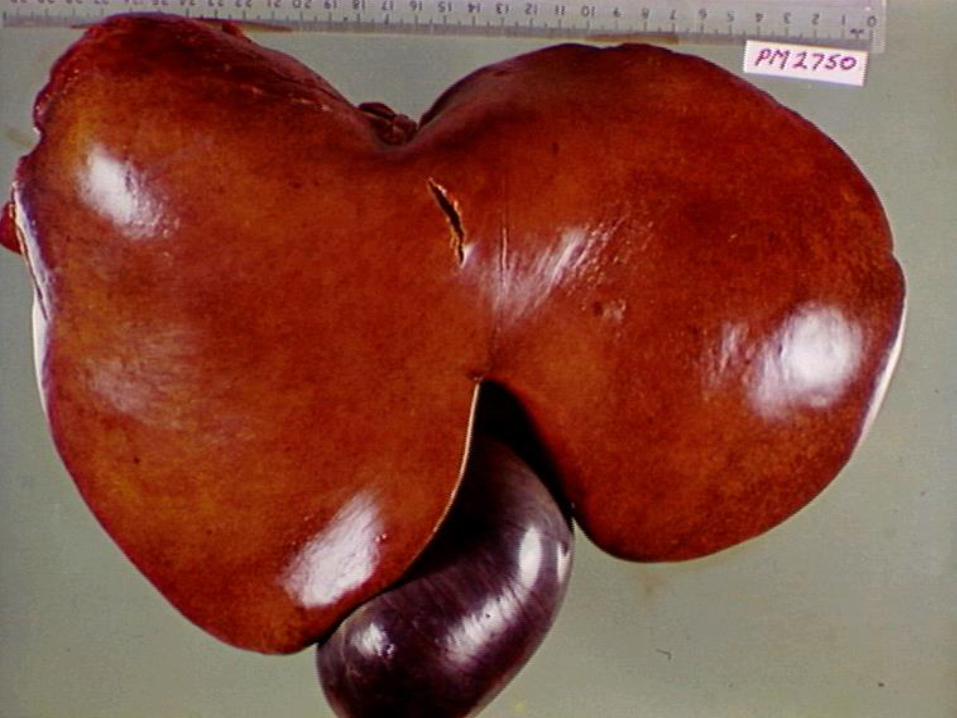
Acute Fatty Liver of Pregnancy
Incidence 5:100,000 maternities
Mitochondrial cytopathy
Similar pathology to
Reye’s Syndrome
Tetracycline toxicity
Valproic acid/Fialuridine
Mortality 10% for mother
10-20% for foetus
Knight et al. Gut 2008
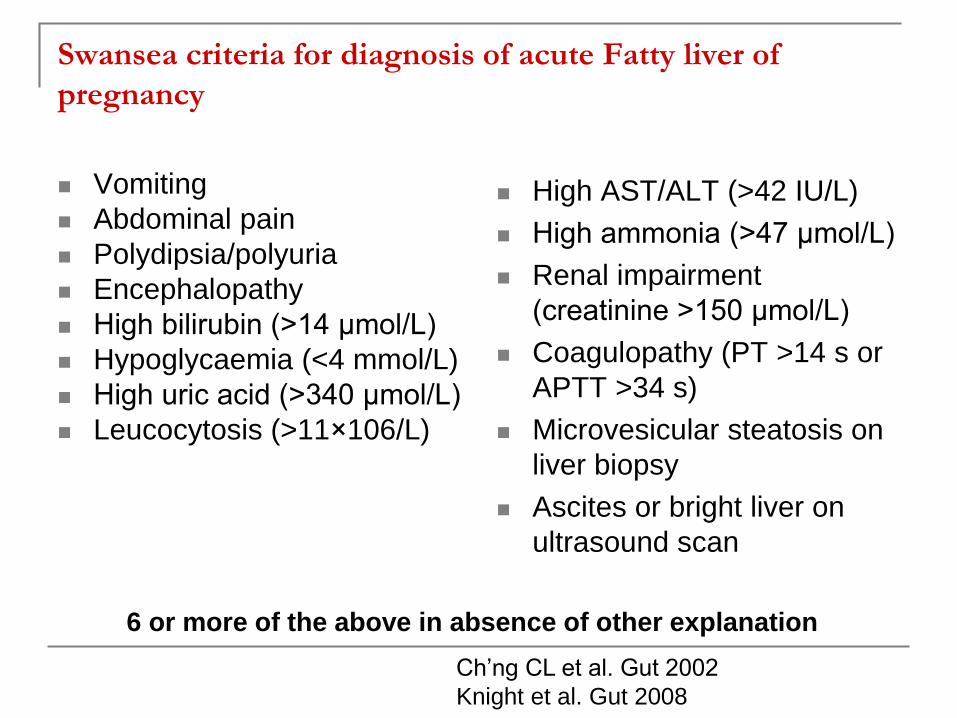
Swansea criteria for diagnosis of acute Fatty liver of
pregnancy
Vomiting
Abdominal pain
Polydipsia/polyuria
Encephalopathy
High bilirubin (>14 μmol/L)
Hypoglycaemia (<4 mmol/L)
High uric acid (>340 μmol/L)
Leucocytosis (>11×106/L)
High AST/ALT (>42 IU/L)
High ammonia (>47 μmol/L)
Renal impairment
(creatinine >150 μmol/L)
Coagulopathy (PT >14 s or
APTT >34 s)
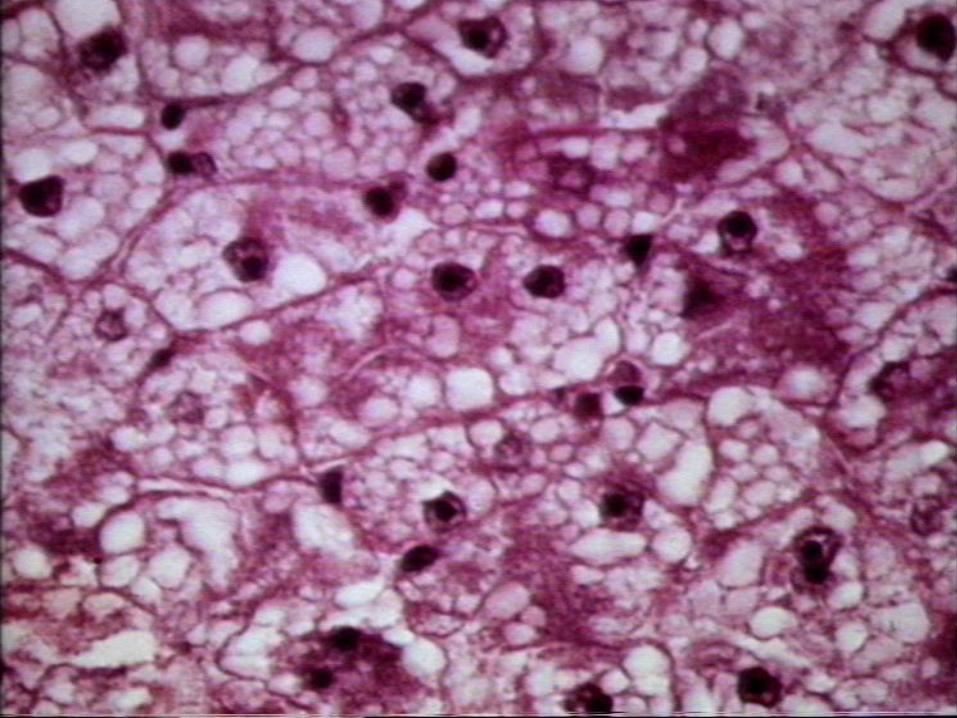
Microvesicular steatosis on
liver biopsy
Ascites or bright liver on
ultrasound scan
6 or more of the above in absence of other explanation
Ch’ng CL et al. Gut 2002
Knight et al. Gut 2008
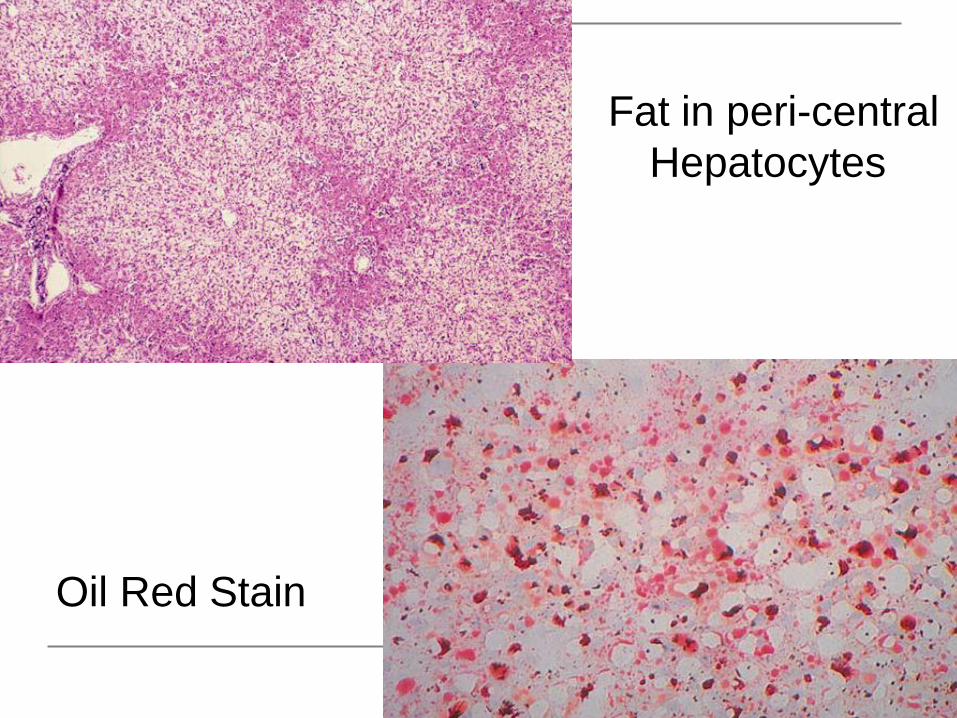
Oil Red Stain
Fat in peri-central
Hepatocytes
Clinical Presentation
Microvescicular fat in affected organs
Third trimester
More common in first or twin pregnancies
AST >10 x Normal
Up to 50% of patients pre-eclampsia
Uric acid may rise prior to symptoms
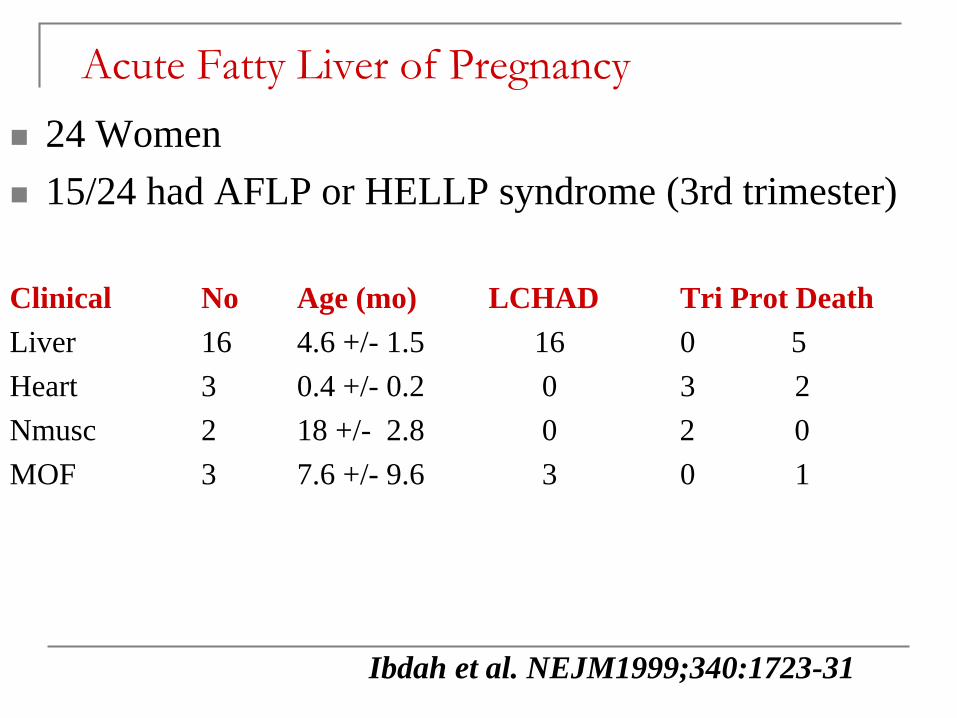
Acute Fatty Liver of Pregnancy
24 Women
15/24 had AFLP or HELLP syndrome (3rd trimester)
Clinical No Age (mo) LCHAD Tri Prot Death
Liver 16 4.6 +/- 1.5 16 0 5
Heart 3 0.4 +/- 0.2 0 3 2
Nmusc 2 18 +/- 2.8 0 2 0
MOF 3 7.6 +/- 9.6 3 0 1
Ibdah et al. NEJM1999;340:1723-31
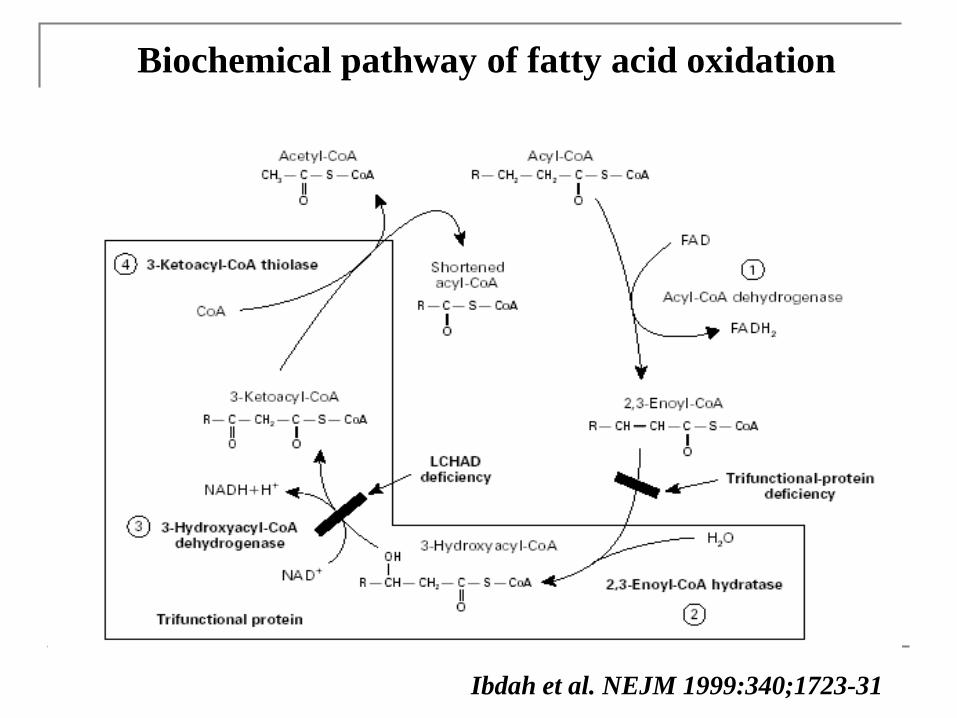
Ibdah et al. NEJM 1999:340;1723-31
Biochemical pathway of fatty acid oxidation
Management
Multi-disciplinary care
Imaging Ultrasound or CT
Biopsy can be postponed until after delivery
No resolution until delivery
If mild, may have time to observe
May rapidly progress to acute liver failure
Vaginal delivery versus Caesarian section
Liver abnormalities may persist 3-4 wks
Supplement with FFP/Plt/Cryoprecipitate

Hypertension Related liver disease of
Pregnancy Pre-eclampsia 5-10% of all pregnancies
Major cause of maternal death
Incorporates a spectrum of disease
Pre-eclampsia
Eclampsia
Hepatic Infarction
Liver Rupture
HELLP syndrome (Weinstein 1982)
Hypertension > 30mmHg (systolic)
>15 mmHg (diastolic)
or >140/90 mmHg
Proteinuria (> 300mg/24 hrs) after 20 wks gestation
Oedema (No longer necessary)
2nd and 3rd trimesters
Risks: Pre-existing hypertension
Extremes of child bearing age
First or twin pregnancies
Sibai BM, Obstet Gynaecol 2003
LFT abnormalities in BP in pregnancy
LFTs reflect severity of hypertension
24% of patients with mild hypertension
>80 of patients with severe hypertension
AST/ALT
Similar to levels in acute hepatitis
Bilirubin usually N unless haemolysis or liver rupture
ATIII correlates inversely with outcome
80% of deaths related to CNS
20% related to liver complications
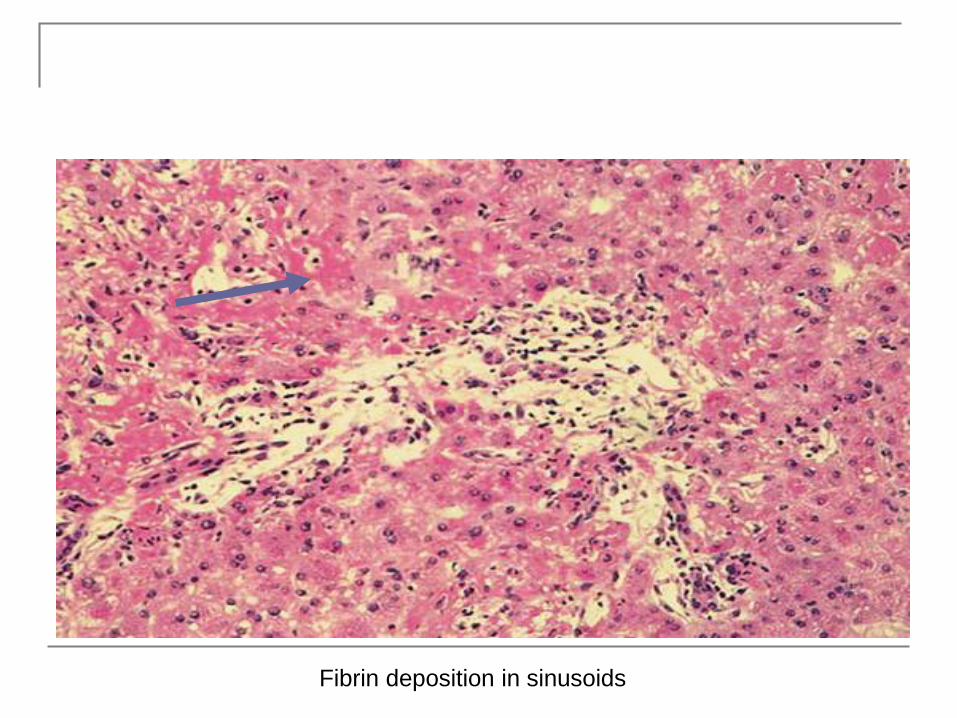
Fibrin deposition in sinusoids
HELLP Syndrome
Described by Pritchard in 1954
HELLP coined by Weinstein in 1982
Pathophysiology similar to pre-eclampsia
Hemolysis due to RBC damage in vascular intima
Caucasian
> 25 yo
< 36 weeks gestation
Hx of poor pregnancy outcome
HELLP Classification Tennessee system
• AST >70 IU/L
• LDH >600 IU/L
• Platelets <100×109/L
Mississippi system
AST >40 IU/L and LDH >600 IU/L and:
• Class I: platelets <50×109/L
• Class II: platelets 50–100×109/L
• Class III: platelets 100–150×109/L
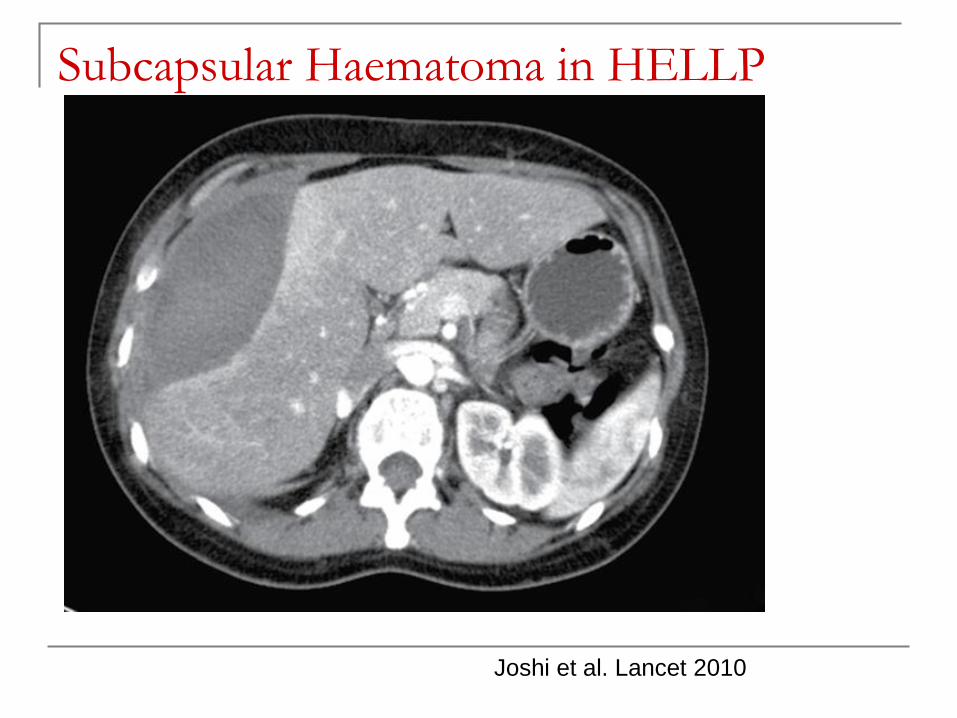
Subcapsular Haematoma in HELLP
Joshi et al. Lancet 2010
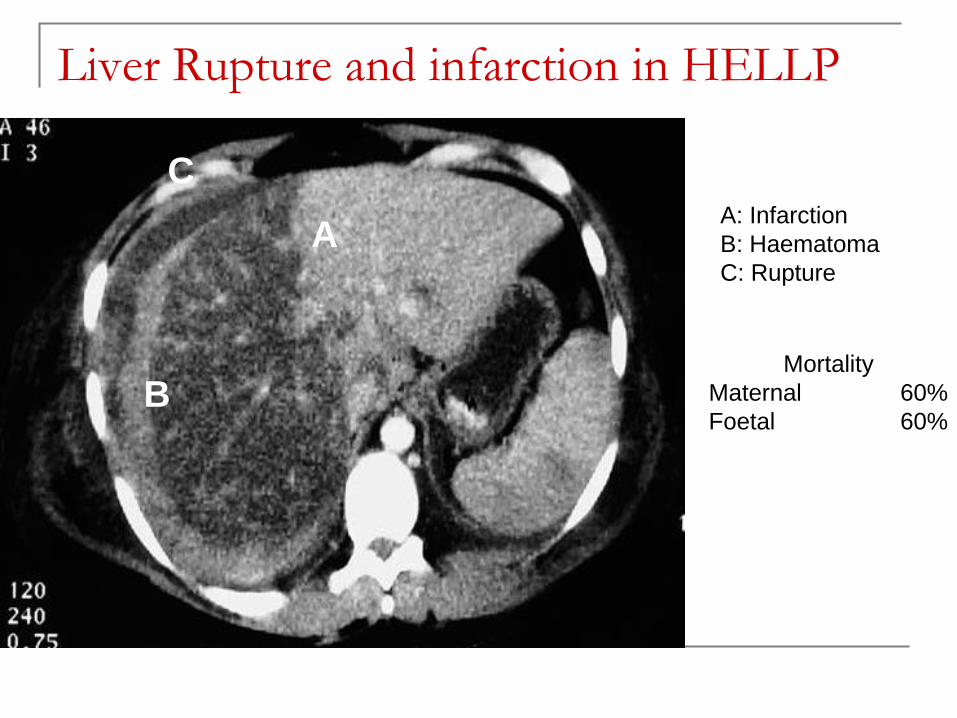
Liver Rupture and infarction in HELLP
A
B
CA: Infarction
B: Haematoma
C: Rupture
Mortality
Maternal 60%
Foetal 60%
Management
Course unpredictable
General management
Early delivery key to success
AST/ALT resolve like ischaemic hepatitis
GGT may rise for 10 days post partum

Management of HELLP
Treat as severe eclamptic
Early delivery if > 34 weeks
33% perinatal mortality in one series
19.3% still births
2-3% maternal death rate
Low dose aspirin and steroids prolonged gestation for
5.5 weeks, but perinatal mortality remained high
(28%)
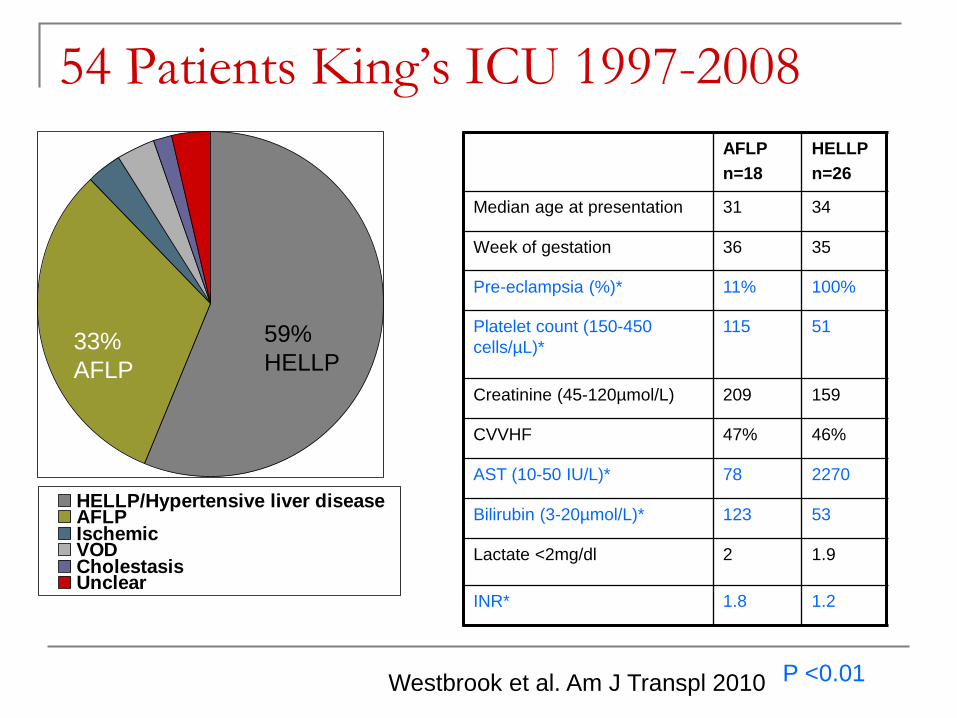
54 Patients King’s ICU 1997-2008
AFLP
n=18
HELLP
n=26
Median age at presentation 31 34
Week of gestation 36 35
Pre-eclampsia (%)* 11% 100%
Platelet count (150-450
cells/µL)*
115 51
Creatinine (45-120µmol/L) 209 159
CVVHF 47% 46%
AST (10-50 IU/L)* 78 2270
Bilirubin (3-20µmol/L)* 123 53
Lactate <2mg/dl 2 1.9
INR* 1.8 1.2
P <0.01
HELLP/Hypertensive liver diseaseAFLPIschemicVODCholestasisUnclear
33%
AFLP
59%
HELLP
Westbrook et al. Am J Transpl 2010
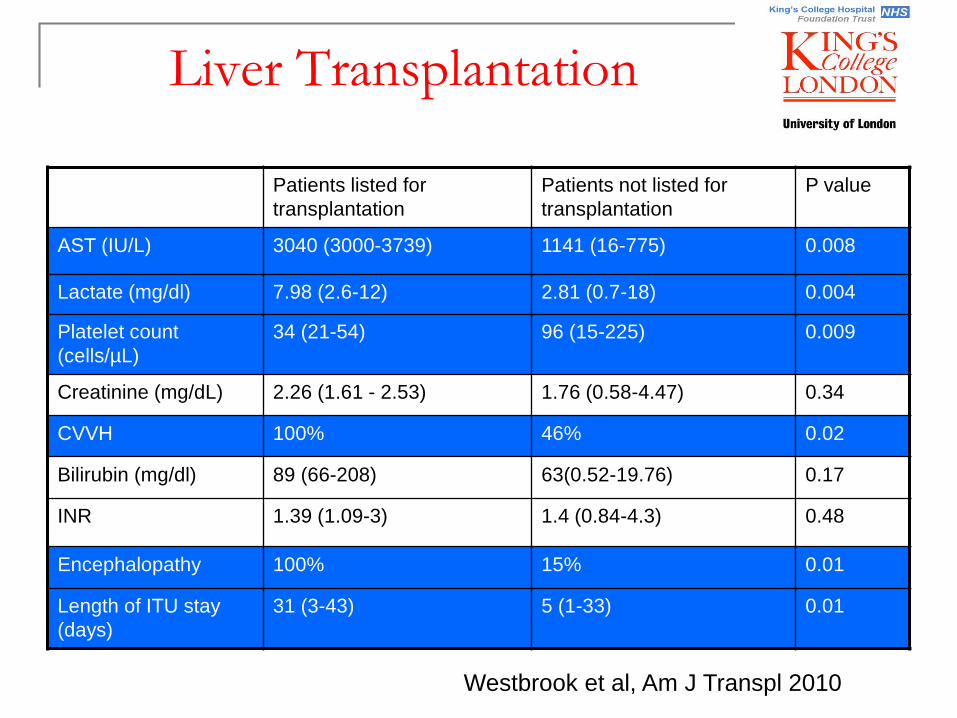
Liver Transplantation
Patients listed for
transplantation
Patients not listed for
transplantation
P value
AST (IU/L) 3040 (3000-3739) 1141 (16-775) 0.008
Lactate (mg/dl) 7.98 (2.6-12) 2.81 (0.7-18) 0.004
Platelet count
(cells/µL)
34 (21-54) 96 (15-225) 0.009
Creatinine (mg/dL) 2.26 (1.61 - 2.53) 1.76 (0.58-4.47) 0.34
CVVH 100% 46% 0.02
Bilirubin (mg/dl) 89 (66-208) 63(0.52-19.76) 0.17
INR 1.39 (1.09-3) 1.4 (0.84-4.3) 0.48
Encephalopathy 100% 15% 0.01
Length of ITU stay
(days)
31 (3-43) 5 (1-33) 0.01
Westbrook et al, Am J Transpl 2010
Intrahepatic Cholestasis of Pregnancy
Itch with elevated bile salts
20% of all jaundice in pregnancy
Up to 1% of all pregnancies in UK/USA
Scandinavia 1-1.5%
Araucanian Indians Chile 4.7-10%
Chilean twin pregnancies 20.9%
Rarely reported in black populations
50% of women with cholestasis on OCP develop cholestasis during pregnancy
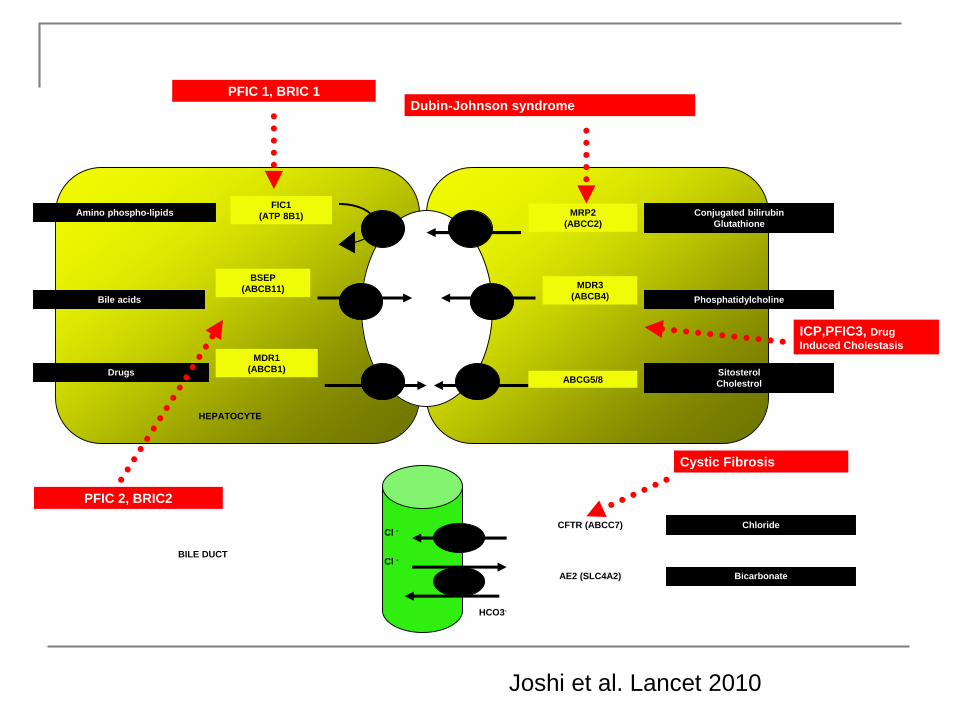
Amino phospho-lipids
Bile acids
Drugs
HEPATOCYTE
Conjugated bilirubin
Glutathione
Phosphatidylcholine
Sitosterol
Cholestrol
BILE DUCT
Cl -
Cl -
HCO3-
Bicarbonate
ChlorideCFTR (ABCC7)
AE2 (SLC4A2)
MRP2
(ABCC2)
MDR3
(ABCB4)
ABCG5/8
FIC1
(ATP 8B1)
BSEP
(ABCB11)
MDR1
(ABCB1)
PFIC 1, BRIC 1Dubin-Johnson syndrome
Cystic Fibrosis
ICP,PFIC3, Drug
Induced Cholestasis
PFIC 2, BRIC2
Joshi et al. Lancet 2010
Genetics of Intrahepatic Cholestasis
Progressive Familial Intrahepatic Cholestasis PFIC
Multiple subtypes (High & Low GGT)
Mutation in Human multidrug resistance 3 (MDR3) gene ABCB4
MDR3 P-glycoprotein a phospholipid translocator
Involved in adding phospholipid to bile
Heterozygosity associated with disease
Other factors may also be important (Oestrogens)
ABCB11 & ABCB4 represent most contributory mutn in large cohort Dixon et al. Am J Gastro 2014;109:76-84
Joshi et al. Lancet 2010
Presentation and Diagnosis
Commonest 2nd and 3rd trimesters
Itch precedes jaundice by 2 weeks
Pain rare (if present, suggests other dx)
Conjugated hyperbilirubinaemia (6 x normal)
Alk phos (5-10 x normal)
bile acids (cholic, deoxycholic, chenodeoxycholic)
AST/ALT usually normal (never more than 10 x)
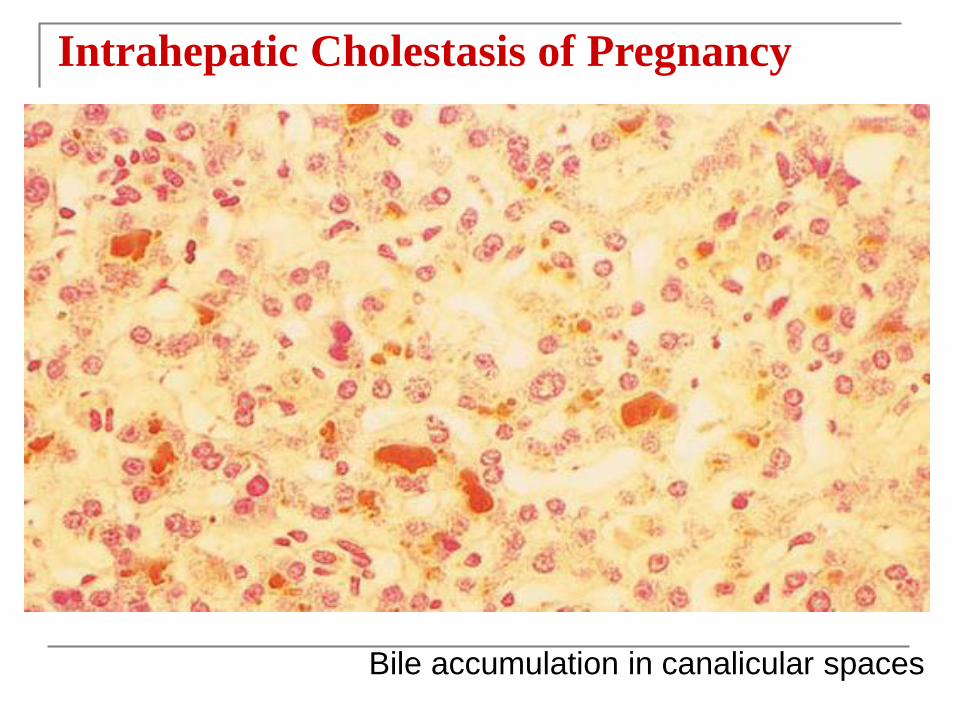
Intrahepatic Cholestasis of Pregnancy
Bile accumulation in canalicular spaces
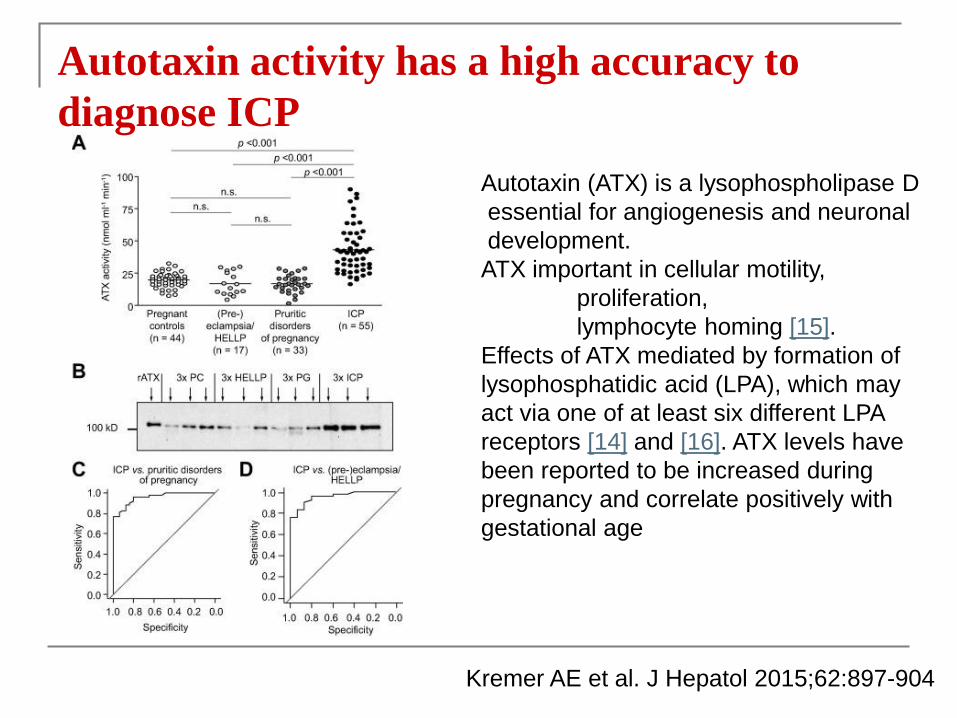
Kremer AE et al. J Hepatol 2015;62:897-904
Autotaxin activity has a high accuracy to
diagnose ICP
Autotaxin (ATX) is a lysophospholipase D
essential for angiogenesis and neuronal
development.
ATX important in cellular motility,
proliferation,
lymphocyte homing [15].
Effects of ATX mediated by formation of
lysophosphatidic acid (LPA), which may
act via one of at least six different LPA
receptors [14] and [16]. ATX levels have
been reported to be increased during
pregnancy and correlate positively with
gestational age
Management
Anti-histamines
Ursodeoxycholic acid (10-15 mg/kg/day)
Urso returns bile acids towards normal
Induces BSEP/MDR3 Transporters
Improves hepatic clearance of disulphated progesterone metabolites
Does not lithocholic acid in meconium
reduced serum taurocholic & taurodeoxycholic acid concentrations
(Prevents conjugation of Cholic Acid with Taurine & Glycine)
Dexamethasone 12mg/day for 7 days, then 3 day taper
Glantz A et al. Hepatol 2008
Tribe RM et al. Am J Gastro 2010
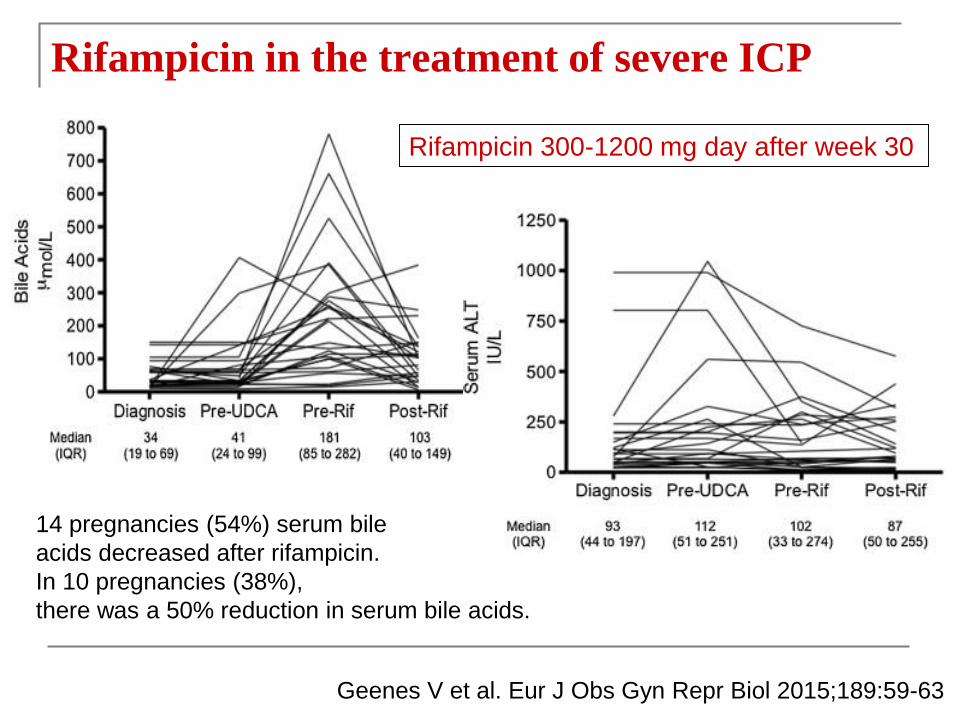
Geenes V et al. Eur J Obs Gyn Repr Biol 2015;189:59-63
Rifampicin in the treatment of severe ICP
14 pregnancies (54%) serum bile
acids decreased after rifampicin.
In 10 pregnancies (38%),
there was a 50% reduction in serum bile acids.
Rifampicin 300-1200 mg day after week 30
Premature birth rate up to 50%
Intra-partum foetal distress 22%
Perinatal mortality rate up to 35%
Risk of poor foetal outcome if serum bile acids
>40umol/L
Onset of Labour should not go beyond term
High risk of recurrence
Emerging data in humans and mice that increased
prevalence of metabolic phenotype in offspringGlantz et al. Hepatology 2004
Papaclevolou et al. JCI 2014
Pre-existing liver disease and Pregnancy
Pregnancy reported, but fertility low
Cirrhosis and risk of bleeding
Increased blood volume & azygous vein flow
Pressure from gravid uterus
Counterbalanced by vasodilation
Treat bleeding as in non-pregnant state
Primary prophyllaxis (banding verus beta-blockers)
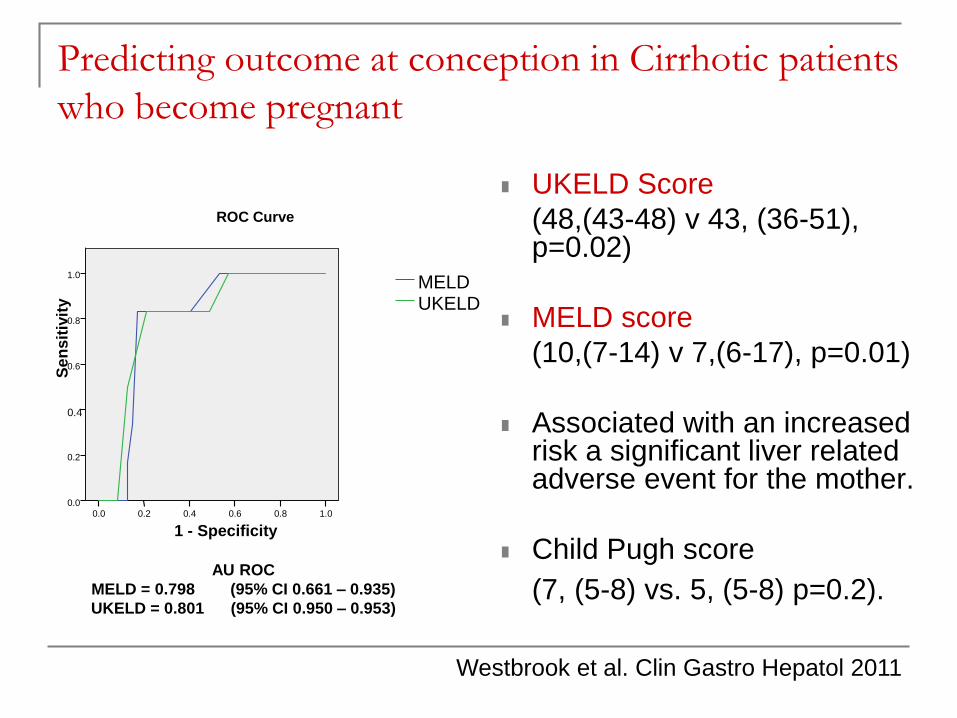
Predicting outcome at conception in Cirrhotic patients
who become pregnant
UKELD Score
(48,(43-48) v 43, (36-51), p=0.02)
MELD score
(10,(7-14) v 7,(6-17), p=0.01)
Associated with an increased risk a significant liver related adverse event for the mother.
Child Pugh score
(7, (5-8) vs. 5, (5-8) p=0.2).
1 - Specificity
1.00.80.60.40.20.0
Se
ns
itiv
ity
1.0
0.8
0.6
0.4
0.2
0.0
UKELDMELD
ROC Curve
AU ROC
MELD = 0.798 (95% CI 0.661 – 0.935)
UKELD = 0.801 (95% CI 0.950 – 0.953)
Westbrook et al. Clin Gastro Hepatol 2011
Acute Viral Hepatitis
Always consider Hepatitis A, B, C, E, HSV…..
Hepatitis B
Infection transmitted at time of delivery
If acute hepatitis B, 50% of infants affected
For chronic carriers in UK (Transmission rate <5%)
In endemic areas (China, Transmission rates > 80%)
Lamivudine/Entecavir FDA Class C
Tenofovir FDA Class B
Treat patients with DNA > 106 after 32 weeks
HCV and Pregnancy
Risk of transmission 0-2%
Increased risk in HIV co-infected and Geno 1 & 3
Antibodies in infant present for up to 6/12
Pregnancy not influenced by HCV
Interferon & ribavirin contra-indicated in
pregnancy but not breastfeeding
Hepatitis E Virus in Pregnancy
Water borne
Epidemic related
Increased prevalence and poor prognosis
Mortality 17.3% in pregnancy
2.1% in non-pregnancy
2.8% in men
No transmission to foetus

Conclusions: Rules of thumb regarding
jaundice in Pregnancy
Interpret LFT’s in light of physiological changes
Always consider co-existent diseases
Balance need for histology with clinical need
Delay biopsy to post-partum if possible
Ultrasound no risk
CT based on clinical need (shield foetus)
MRI (fine but avoid Gadolinium)
ERCP performed safely in pregnancy





![[PPT]Hyperemesis Gravidarum - Philadelphia University …philadelphia.edu.jo/academics/aalrazek/uploads... · Web viewHyperemesis Gravidarum Learning objective Identify Hyperemesis](https://static.fdocuments.net/doc/165x107/5af587257f8b9a190c8e7497/ppthyperemesis-gravidarum-philadelphia-university-viewhyperemesis-gravidarum.jpg)












