
PREDICTIVE VALUE OF THE ASTRAL SCORE, THE CHARLSON AND THE ELIXHAUSER COMORBIDITY INDEXES IN ACUTE...
5
PREDICTIVE VALUE OF THE ASTRAL SCORE, THE CHARLSON AND THE ELIXHAUSER COMORBIDITY INDEXES IN ACUTE ISCHEMIC STROKE Kakaletsis Nikolaos 1 , Papavasileiou Vasileios 1 , Lambrou Dimitrios 2 , Eskandari Ashraf 2 ,Ntaios George 2 , Michel Patrik 2 LARISSA 21 March 2015 1. Department of Clinical Neurosciences and Preventive Medicine, Danube University in Krems, Austria 2. Stroke Center, Neurology Service, Centre Hospitalier Universitaire Vaudois and University of Lausanne, Lausanne, Switzerland. Centre Cérébrovasculaire 1
-
Upload
warren-quinn -
Category
Documents
-
view
215 -
download
0
Transcript of PREDICTIVE VALUE OF THE ASTRAL SCORE, THE CHARLSON AND THE ELIXHAUSER COMORBIDITY INDEXES IN ACUTE...
PREDICTIVE VALUE OF THE ASTRAL SCORE, THE CHARLSON AND THE ELIXHAUSER COMORBIDITY INDEXES
IN ACUTE ISCHEMIC STROKE
Kakaletsis Nikolaos 1, Papavasileiou Vasileios 1, Lambrou Dimitrios 2, Eskandari Ashraf 2,Ntaios George 2, Michel Patrik 2
LARISSA 21 March 2015
1. Department of Clinical Neurosciences and Preventive Medicine, Danube University in Krems, Austria2. Stroke Center, Neurology Service, Centre Hospitalier Universitaire Vaudois and University of Lausanne, Lausanne, Switzerland.
CentreCérébrovasculaire
1
Introduction
Definitions: ComorbidityThe medical conditions that exist at the time of diagnosis of the index disease or later, but that are not a consequence of the index disease and it is likely to be a significant factor influencing mortality
and resource use in the hospital
• Comorbidity has been shown to be highly prevalent in stroke patients, especially in the older population.
• The phenomenon of comorbidity is relevant because it often has a negative impact on health outcomes, quality of life, and health care use.
• There is limited information on the prevalence and impact of comorbidities in stroke patients.
• Clinical prognostic models in acute stroke would be helpful in predicting outcome in future patients (informing them and their relatives of reasons for treatment and clinical decisions, creating clinical risk groups and stratifying patients by disease severity in clinical trials).
2
Guralnik JM. Assessing the impact of comorbidity in the older population. Ann Epidemiol. 1996;6(5):376-80. van den Akker et al. Multimorbidity in general practice: prevalence, incidence, and determinants of co-occurring chronic and recurrent diseases. J Clin Epidemiol. 1998;51(5):367-75. Gijsen R, eta al. Causes and consequences of comorbidity: a review. J Clin Epidemiol. 2001;54(7):661-74. Ording AG, et al. Concepts of comorbidities, multiple morbidities, complications, and their clinical epidemiologic analogs. Clin Epidemiol. 2013;5:199-203. Feinstein AR. The pre-therapeutic classification of co-morbidity in chronic disease. Journal of Chronic Diseases. 1970;23(7):455-68.

Aim - Methods
The aim was to evaluate the prognostic value of the Charlson/Deyo and Elixhauser comorbidity
indexes (CI) on functional outcome and mortality in patients with acute ischemic stroke (AIS) in short-, medium- and long-term and to test whether they can add further predictive
value in addition to the existing clinical predictive model (ASTRAL-score).
ASTRAL is the prospective registry of all consecutive patients admitted to the stroke unit or intensive care unit of the Central University Hospital of Vaud (CHUV) with acute ischemic stroke
within 24 hours after last proof of well-being.
We assessed 3,099 consecutive AIS patients from the Acute Stroke Registry and Analysis of
Lausanne (ASTRAL) regarding unfavorable functional outcome, (mRS>2) and mortality at 7
days, 3 and 12 months.
C-statistics (AUC: area under the receiver-operating-characteristic [ROC] curve) were calculated as measures of discrimination.
1 indicating perfect prediction and 0.5 indicating chance prediction. 0.7-0.8 can be considered as acceptable0.8-0.9 as excellent
3
4
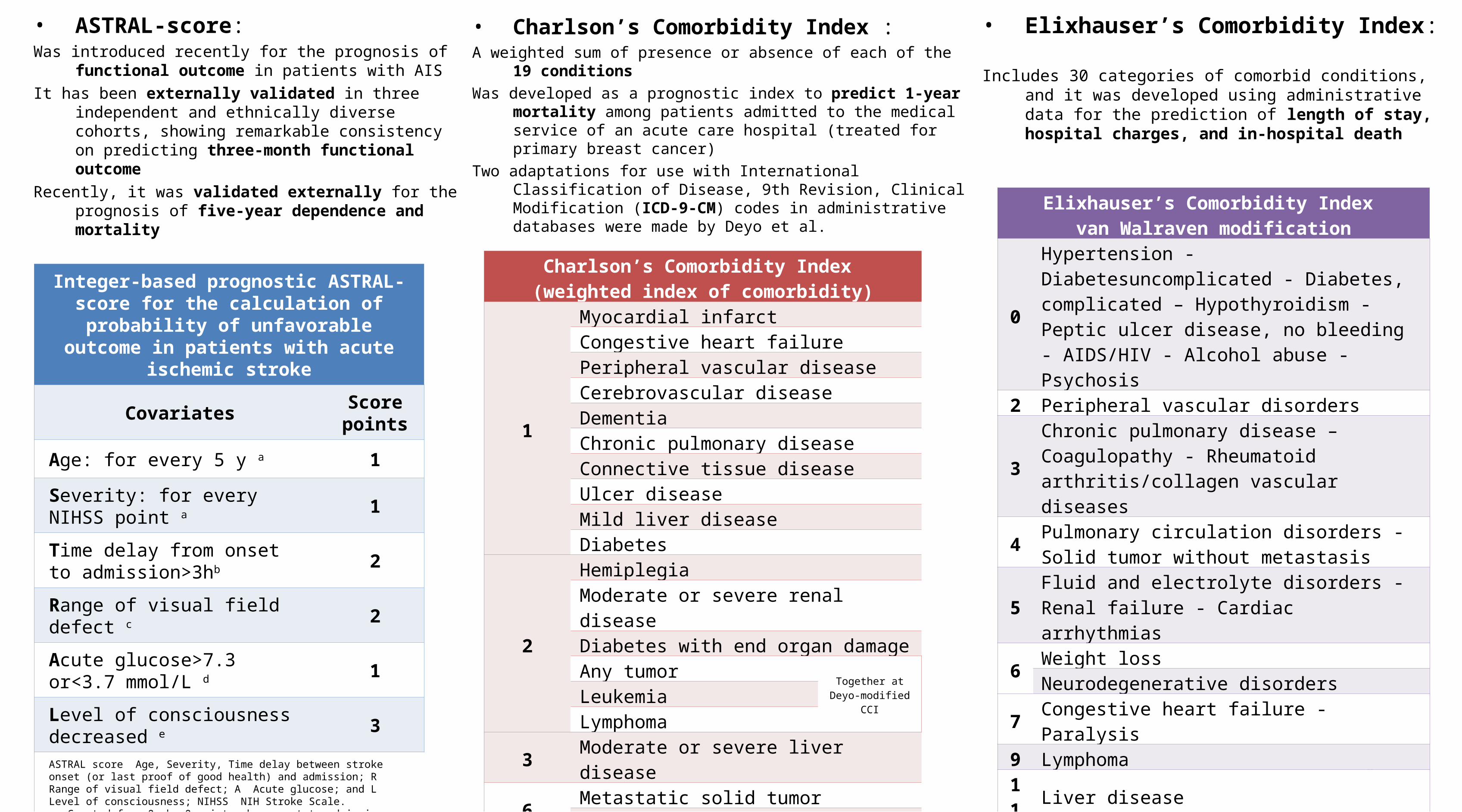
Integer-based prognostic ASTRAL-score for the calculation of probability of unfavorable
outcome in patients with acute ischemic stroke
Covariates Score points
Age: for every 5 y a 1
Severity: for every NIHSS point a 1
Time delay from onset to admission>3hb 2
Range of visual field defect c 2
Acute glucose>7.3 or<3.7 mmol/L d 1
Level of consciousness decreased e 3ASTRAL score Age, Severity, Time delay between stroke onset (or last proof of good health) and admission; R Range of visual field defect; A Acute glucose; and L Level of consciousness; NIHSS NIH Stroke Scale.a. Counted from 0, b. 0 points when onset-to-admission time was 3 hours, c. 2 points for any stroke-related visual field defect; 0 points in the absence of visual field defect, d. 0 points for glucose 3.7 and 7.3 mmol/L, e. 0 points for normal level of consciousness.
Charlson’s Comorbidity Index (weighted index of comorbidity)
1
Myocardial infarctCongestive heart failurePeripheral vascular diseaseCerebrovascular diseaseDementiaChronic pulmonary diseaseConnective tissue diseaseUlcer diseaseMild liver diseaseDiabetes
2
HemiplegiaModerate or severe renal diseaseDiabetes with end organ damageAny tumor
Together at Deyo-modified CCILeukemia
Lymphoma3 Moderate or severe liver disease
6Metastatic solid tumorAIDS
Elixhauser’s Comorbidity Index van Walraven modification
0
Hypertension - Diabetesuncomplicated - Diabetes, complicated – Hypothyroidism - Peptic ulcer disease, no bleeding - AIDS/HIV - Alcohol abuse - Psychosis
2 Peripheral vascular disorders
3Chronic pulmonary disease – Coagulopathy - Rheumatoid arthritis/collagen vascular diseases
4Pulmonary circulation disorders - Solid tumor without metastasis
5Fluid and electrolyte disorders - Renal failure - Cardiac arrhythmias
6Weight lossNeurodegenerative disorders
7 Congestive heart failure - Paralysis9 Lymphoma
11 Liver disease12 Metastatic cancer -1 Valvular disease-2 Blood loss anemia - Deficiency anemia-3 Depression-4 Obesity-7 Drug abuse
• ASTRAL-score:Was introduced recently for the prognosis of functional
outcome in patients with AISIt has been externally validated in three independent
and ethnically diverse cohorts, showing remarkable consistency on predicting three-month functional outcome
Recently, it was validated externally for the prognosis of five-year dependence and mortality
• Charlson’s Comorbidity Index :A weighted sum of presence or absence of each of the 19
conditionsWas developed as a prognostic index to predict 1-year mortality
among patients admitted to the medical service of an acute care hospital (treated for primary breast cancer)
Two adaptations for use with International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM) codes in administrative databases were made by Deyo et al.
• Elixhauser’s Comorbidity Index:
Includes 30 categories of comorbid conditions, and it was developed using administrative data for the prediction of length of stay, hospital charges, and in-hospital death

RESULTS
Conclusions• The ASTRAL-score is better predictor of AIS outcome
(functional outcome or death) than Charlson/Deyo and Elixhauser CIs in short-, medium- and long-term.
• It may be statistically improved with the addition of the Charlson/Deyo CI, but this addition is of limited clinically use because of its complex calculation.
















