Predicting self-harm and suicide: Have we progressed in...
33
Predicting self-harm and suicide: Have we progressed in the state-trait debate? Prof. Ella Arensman National Suicide Research Foundation, Department of Epidemiology and Public Health University College Cork, Ireland School of Applied Psychology UCC 16 th April 2014
Transcript of Predicting self-harm and suicide: Have we progressed in...

Predicting self-harm and suicide: Have we progressed in the
state-trait debate?
Prof. Ella Arensman
National Suicide Research Foundation,
Department of Epidemiology and Public Health
University College Cork, Ireland
School of Applied Psychology
UCC
16th April 2014

Overview
Background
Review 1: State – Trait factors associated with self-harm and suicide
Outcomes prospective study among self-harm patients in Ireland: stability of psychological outcomes over time
Review 2: Risk factors for repetition of self-harm
Evidence based recommendations & actions

Early discussions about state-trait and the relation with suicide
Vincent van Gogh (1853–1890) had an
eccentric personality and unstable moods,
suffered from recurrent psychotic episodes
during the last 2 years of his extraordinary
life, and died by suicide at the age of 37.
Despite limited evidence, well over 150
physicians have ventured a perplexing
variety of diagnoses of his illness.

Recognition of personal characteristics/ temperament associated with suicide
“Each victim of suicide gives his act a
personal stamp which expresses his
temperament, the special conditions in which
he is involved, and which, consequently,
cannot be explained by the social and general
causes of the phenomenon”
(Emile Durkheim, 1858-1917)

State or Trait? An old debate with on-going relevance
Enhance treatment interventions geared to subgroups of self-harm patients
Challenges in reducing repeated self-harm and suicide risk among self-harm patients with very frequent repetition
Challenges in understanding the occurrence of multiple cases of non-fatal and fatal suicidal behaviour within families

Identification of subgroups of frequently repeating self-harm patients presenting to
hospital Emergency Departments
Number of DSH acts in 2003-2012
Persons Presentations
Number (%) Number (%)
One 52,686 76.5% 52,686 47.2%
Two 8.913 12.9% 17,826 16%
Three 3,056 4.4% 9,168 8.2%
Four 1,421 2.1% 5,684 5.1%
Five 774 1.1% 3,870 3.5%
Six 559 0.8% 3,354 3.0%
Seven 337 0.5% 2,359 2.1%
Eight 237 0.3% 1,896 1.7%
Nine 163 0.2% 1,467 1.3%
10 or more 722 1.0% 13,372 12%
National Registry of Deliberate Self-Harm (2003-2012)

Consistent pattern regarding the number of previous acts of self-harm and risk of future repetition
Perry et al, 2012

Relevance of state-trait debate in early identification of self-harm, repeated self-harm
and suicide
Self-harm patients form a high-risk group – For suicide (e.g. Hawton et al, 2003)
– For future self-harm (e.g. Christiansen & Jensen, 2007)
→ Fortunately, not all those who present with self-harm will
self-harm fatally or non-fatally in the future
How can we identify at the earliest stage
those who will go on to repeat self-harm?

State – Trait Terminology and definition
Trait (temperament dimension/character/personality): Enduring characteristic of a patient related to the threshold for acting on suicidal/self-harm thoughts (Mann
et al, 1999).
State (frame of mind/situation): transient experience of mood that can change across situations and contexts (e.g. depression) (Terracciano et al, 2006).

Review 1
Reviews including studies addressing state and/or trait characteristics of people engaging in non-fatal and fatal suicidal behaviour (1980 >)
Individual studies addressing state and/or trait characteristics of people engaging in non-fatal suicidal behaviour not included in reviews

1980s – Identification of specific traits associated with suicidal behaviour
Review of 18 studies in patients with major depression - Asberg et al, (1986)
Comparing suicide attempters versus non-attempters:
Specific traits significantly associated with
suicide attempters:
-Lifetime aggression
-Lifetime impulsivity
-Comorbid borderline personality disorder
-Comorbid alcohol abuse
-Decreased serotonin function (att. suicide + suicide)
Indications for severity of depression as a state dependent factor
Fairly stable, variable time periods
1990s – Insight into neurobiological and psychological determined traits and states independent of type of psychiatric disorder
Reviews of clinical and post mortem studies among patients with depression and other types of psychiatric disorders – Mann & Arango, 1992; Soares & Mann, 1997; Mann et al, 1999
Further consolidation of identified traits: Lifetime aggression, lifetime impulsivity, comorbid borderline personality disorder, comorbid alcohol abuse, and comorbid substance abuse
Decreased serotonin function (attempted suicide + suicide) – Fairly stable, variable time periods
Similar patterns identified when comparing suicide attempters with non-attempters among patients diagnosed with other psychiatric diagnoses, such as schizophrenia and personality disorders

stressor
suicidal ideation
Sex, religion, childhood experiences, familial/genetic
factors, head injury, low cholesterol, etc.
diathesis
Suicid
al a
ct
Psychiatric disorder Psychiatric crisis
hopelessness
norepinephrine
impulsivity
serotonin
Development of a stress-diathesis model of suicidal behaviour – Mann et al, 1999

Further consolidation and elaboration in the 2000s: Towards a psychobiological model
Van Heeringen (2003) Review of biological and psychological studies of suicidal behaviour among people with different types of psychiatric disorders
-Sensitivity to stress
-Hopelessness
-Impulsivity
-Aggression
-Impaired problem-solving (no escape - entrapment)
Serotonine, Dopamine
Norepinephrine, Serotonine
Implication: Trait-dependent serotonergic dysfunction is not confined to depressive disorders, but is also involved in the development of suicidal behaviour in the context of other disorders, e.g. schizophrenia and substance abuse

Cry of Pain – Entrapment model of suicidal behaviour
Entrapment: Suicidal behaviour is the response to a stressful situation which has three components which act together to increase suicidal risk: (1) the presence of defeat, (2) perception of no escape and (3) perception of no rescue (Williams, 2001;2005; Rasmussen et al, 2010; O’Connor et al, 2013)

Stability of trait characteristics over time?

Prospective study among self-harm patients: Investigating stability and change of
psychological outcomes
Consecutive self-harm patients presenting to general hospitals in Cork and Limerick, who formed the control group (N=211) in a randomised controlled trial to test the effectiveness of a problem-solving intervention
Exclusion criteria: Severe alcohol abuse, current psychosis, having a learning disability
Prospective design: T1: Baseline interview after index self-harm act; T2: 6 weeks after T1; T3: 6 months after T2

Patient characteristics and outcome measures
Females: 65%; mean age total sample: 33.6 years (SD 12.1)
History of previous self-harm: 63%
Self-harm methods: Intentional drug overdose: 85%, self-cutting: 17%, attempted hanging: 4%, attempted drowning: 4%, other methods: 2%
Response rate at 6 months follow-up: 71%
Repetition rate during follow-up: 15.3%
Outcome measures and analysis
Evidence for trait
1. Impulsivity
2. Problem-Solving
3. Hopelessness
4. Self-Efficacy
Evidence for state
5. Suicidal intent
6. Depression
Within-person stability of the scores on the outcome measures over the 3 time points was calculated using the intraclass correlation coefficient.

0
10
20
30
40
50
60
70
80
90
Time 1 Time 2 Time 3
Impulsivity Mean
Problem Solving Mean
Male self-harm patients: Impulsivity and Problem Solving, mean scores at
T1, 2, 3
Impulsivity 95% CI Time 1: 68.19-75.69 Time 2: 67.06-74.76 Time 3: 65.03-73.14 Problem Solving 95% CI Time 1: 69.21-77.55 Time 2: 76.85-87.16 Time 3: 78.20-87.76

0
10
20
30
40
50
60
70
80
90
Time 1 Time 2 Time 3
Impulsivity Mean
Problem Solving Mean
Impulsivity 95% CI Time 1: 71.83-78.21 Time 2: 69.30-75.52 Time 3: 69.06-75.30 Problem Solving 95% CI Time 1: 67.83-73.75 Time 2: 72.64-79.79 Time 3: 73.64-81.11
Female self-harm patients: Impulsivity and Problem Solving, mean scores at
T1, 2, 3

0
5
10
15
20
25
30
35
40
Time 1 Time 2 Time 3
Hopelessness Mean
Depression Mean
Self Efficacy Mean
Suicide Intent Mean
Male Self-Harm patients: Hopelessness, Depression, Self Efficacy,
Suicide Intent, T1, T2, T3
Hopelessness 95% CI Time 1: 6.98-10.80 Time 2: 3.94-7.50 Time 3: 3.78-7.22 Depression 95% CI Time 1: 29.17-37.58 Time 2: 11.16-19.85 Time 3: 10.94-20.37 Self Efficacy 95% CI Time 1: 24.52-28.49 Time 2: 25.58-29.87 Time 3: 26.13-30.19 Suicide Intent 95% CI Time 1: 9.45-18.79 Time 2: 2.45-10.19 Time 3: 0.68-8.2
0
5
10
15
20
25
30
35
40
Time 1 Time 2 Time 3
Hopelessness Mean
Depression Mean
Self Efficacy Mean
Suicide Intent Mean
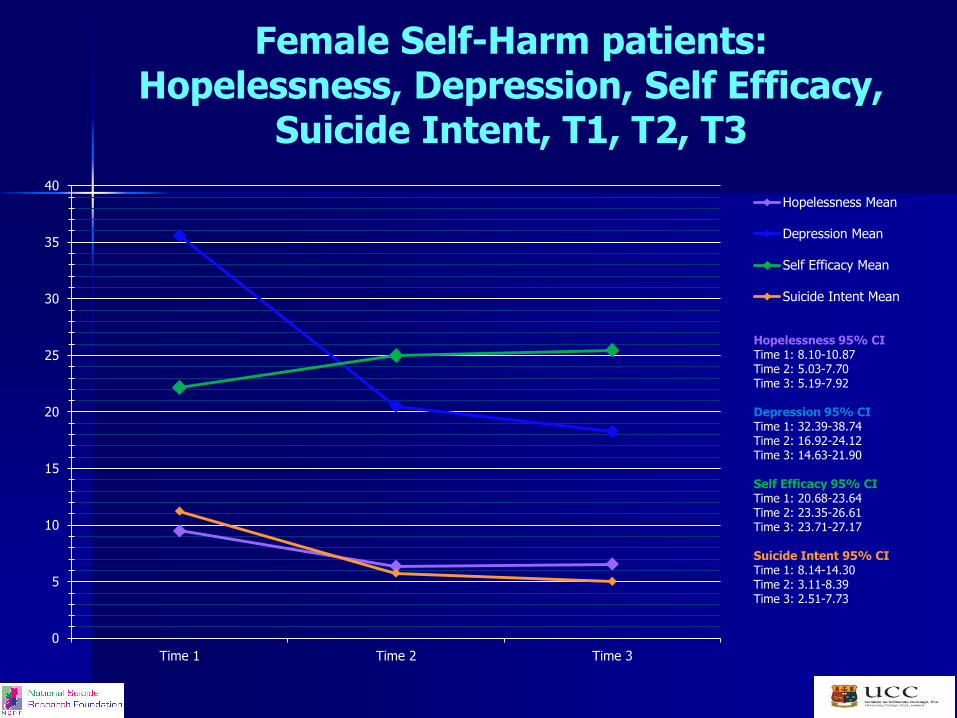
Hopelessness 95% CI Time 1: 8.10-10.87 Time 2: 5.03-7.70 Time 3: 5.19-7.92 Depression 95% CI Time 1: 32.39-38.74 Time 2: 16.92-24.12 Time 3: 14.63-21.90 Self Efficacy 95% CI Time 1: 20.68-23.64 Time 2: 23.35-26.61 Time 3: 23.71-27.17 Suicide Intent 95% CI Time 1: 8.14-14.30 Time 2: 3.11-8.39 Time 3: 2.51-7.73
Female Self-Harm patients: Hopelessness, Depression, Self Efficacy,
Suicide Intent, T1, T2, T3

History of previous Self-harm
Repeated self-harm -prospectively
ICC 95% CI
Impulsivity 0.58 0.40-0.73
Self Efficacy 0.42 0.17-0.67
Hopelessness 0.41 0.16-0.66
Suicide Intent 0.40 0.08-0.71
Depression 0.39 0.13-0.63
Problem Solving 0.38 0.10-0.65
Stability of outcomes over time by risk of repetition (subgroup ongoing repetition):
Intraclass Correlation Coefficients

No history of self-harm Repeated self-harm prospectively
ICC 95% CI
Self Efficacy 0.64 0.19-0.92
Depression 0.62 0.16-0.91
Hopelessness 0.61 0.19-0.89
Problem Solving 0.52 0.05-0.88
Impulsivity 0.52 0.04-0.88
Suicide Intent 0.20 -0.39-0.96
Stability of outcomes over time by risk of repetition (subgroup first repeat): Intraclass Correlation Coefficients

Review 2: Risk Factors for Repetition of Self-Harm
A Review of Prospective
Hospital-Based Studies (Larkin C, DiBlasi Z, Arensman E, 2014)

Psychological/neurological factors associated
with repeated self-harm
Number of studies Conclusion
Variable Hi-med
quality
significant
Hi-med
quality non-
significant
Low quality
significant
Low quality
non-
significant
Personality disorder 10(+) -- 2(+) -- Strong (+)
Hopelessness 9(+) 3 5(+) -- Strong(+)
Impulsivity 3(+) 3 1(+) 1 Emerging(+)
Problem-solving ability 2(-) -- 2(-) -- Emerging (-)
Sociopathy 1(+) -- 2(+) -- Emerging(+)
External hostility 1(+) -- 1(+) -- Little(+)
Internal hostility -- 1 1(+) -- Little (+)
Self-esteem 2(+) 2 2(-) 2 Mixed
(+) indicates that factor had significant direct association with repetition (-) indicates that factor had significant inverse association with repetition

Psychopathology factors associated with
repeated self-harm
Number of studies Conclusion
Variable Hi-med
quality
significant
Hi-med
quality
non-
significant
Low
quality
significant
Low quality
non-
significant
History of psychiatric treatment 18(+) 6 3(+) 1 Strong(+)
Alcohol misuse/dependence 14(+) 9 -- 2 Strong(+)
Drug misuse/dependence 10(+) 6 -- 1 Strong (+)
Current psychiatric treatment 6(+) -- -- -- Strong(+)
Schizophrenia history 3(+) -- 1(+) -- Emerging(+
)
History of major depression 2(+) 1 2(+) 1 Emerging(+
)
Substance misuse/dependence 2(+) 6 1(+) 3 Emerging(+
)

Self-harm related factors/suicidality associated
with repeated self-harm
Number of studies Conclusion
Variable Hi-med
quality
significant
Hi-med
quality non-
significant
Low
quality
significant
Low quality
non-
significant
Previous self-harm 31(+) 6 10(+) 4 Strong (+)
Negative attitude towards surviving episode 3(+) -- -- -- Emerging(+)
Suicidal plans at assessment 3(+) -- -- 1 Emerging(+)
Suicidal ideation 3(+) 1 -- 1 Emerging(+)
Major self-injury 2(+) -- -- -- Emerging(+)
Self-injury (comp self-poisoning) 1(+) 4 1(+) -- Little(+)
Steps to avoid discovery 1(+) 3 -- 1 Little(+)
Wish to die 1(+) 5 -- 2 Little(+)
Externally-directed motive -- 2 1(+) 2 Little(+)
Suicide note 2(+) 1(-) 3 2(-) 1 Mixed
Premeditation 2(+) 1(-) 3 -- 1 Mixed
Lethality 1(+) 1(-) 8 2(-) 4 Mixed

Evidence based Recommendations and Actions
There is a need for enhanced psychosocial and psychiatric assessment procedures taking into account the identified state and trait factors in order to identify people with high risk of frequent repetition at an early stage.
Research outcomes underline the need to provide a ‘menu’ of treatment interventions’ geared to different subgroups of self-harm patients, such as people with a pattern of multiple repeated self-harm acts and high levels of impulsivity and hopelessness (e.g. Dialectical Behaviour Therapy) and those with less frequent repetition and deficits in problem-solving (e.g. Cognitive Behaviour Therapy)
On-going assessment and monitoring of levels of suicidal intent is crucial as this may fluctuate rapidly over time (fluid rather than stable concept).

“People who attempt suicide never want to die, what they want is a different life”
(R. Wieg, 2003)

Acknowledgements
Dr Carmel McAuliffe Dr Tony Fitzgerald Dr Paul Corcoran Dr Celine Larkin
Ms Laura O’Connell Ms Caroline Daly
National Suicide Research Foundation Department of Epidemiology and Public Health, UCC
The National Suicide Research Foundation is in receipt of funding from the National Office for Suicide Prevention

Thank you!
Prof. Ella Arensman National Suicide Research Foundation
Department of Epidemiology and Public Health, University College Cork
Ireland E-mail: [email protected]
www.nsrf.ie